
Significantly Elevated Levels of Plasma Nicotinamide, Pyridoxal, and Pyridoxamine Phosphate Levels in Obese Emirati Population: A Cross-Sectional Study


 , ,
, , 
 and
and 
Abstract
:1. Introduction
2. Results and Discussion
3. Materials and Methods
3.1. Materials
3.2. Preparation of Standard Solutions
3.3. Plasma Sample Extraction Method
3.4. Liquid Chromatography and Mass Spectrometry
3.5. Study Design and Sample Collection
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| PL | Pyridoxal |
| PLP | Pyridoxal 5′-phosphate |
| PM | Pyridoxamine |
| PMP | Pyridoxamine 5′-phosphate |
| PN | Pyridoxine; PN-d3: Pyridoxine - (methyl-d3) |
| TCA | Trichloroacetic acid |
| n.d. | Not detected |
| LC-MS/MS | Liquid Chromatography tandem Mass Spectrometry |
| CVD | Cardiovascular disease |
| BMI | Body Mass Index |
References
- Furdui, C.; Ragsdale, S.W. The role of pyruvate ferredoxin oxidoreductase in pyruvate synthesis during autotrophic growth by the Wood-Ljungdahl path-way. J. Biol. Chem. 2000, 275, 28494–28499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzetti, S.; Zhang, J.; Van Der Spoel, D. Thiamin function, metabolism, uptake, and transport. Biochemistry 2014, 53, 821–835. [Google Scholar] [PubMed]
- Kotloski, N.J.; Gralnick, J.A. Flavin electron shuttles dominate extracellular electron transfer by Shewanella oneidensis. mBio 2013, 4, e00553-12. [Google Scholar] [CrossRef] [Green Version]
- Velasquez-Orta, S.B.; Head, I.M.; Curtis, T.; Scott, K.; Lloyd, J.R.; Von Canstein, H. The effect of flavin electron shuttles in microbial fuel cells current production. Appl. Microbiol. Biotechnol. 2009, 85, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Selhub, J. Folate, vitamin B12 and vitamin B6 and one carbon metabolism. J. Nutr. Heal. Aging 2002, 6, 39–42. [Google Scholar]
- Clayton, P.T. B6-responsive disorders: A model of vitamin dependency. J. Inherit. Metab. Dis. 2006, 29, 317–326. [Google Scholar] [CrossRef]
- Wang, L.; Li, H.; Zhou, Y.; Jin, L.; Liu, J. Low-dose B vitamins supplementation ameliorates cardiovascular risk: A double-blind randomized controlled trial in healthy Chinese elderly. Eur. J. Nutr. 2014, 54, 455–464. [Google Scholar] [CrossRef]
- Selhub, J.; Morris, M.S.; Jacques, P.F.; Rosenberg, I.H. Folate-vitamin B-12 inter-action in relation to cognitive impairment, anemia, and biochemical indicators of vitamin B-12 deficiency. Am. J. Clin. Nutr. 2009, 89, 702S–706S. [Google Scholar] [CrossRef] [Green Version]
- Czeizel, A.E.; Dudás, I.; Vereczkey, A.; Bánhidy, F. Folate deficiency and folic acid supplementation: The prevention of neural-tube defects and congenital heart defects. Nutrients 2013, 5, 4760–4775. [Google Scholar] [CrossRef] [Green Version]
- Heseker, H. Folic acid and other potential measures in the prevention of neural tube defects. Ann. Nutr. Metab. 2011, 59, 41–45. [Google Scholar] [CrossRef]
- Bryan, J.; Calvaresi, E.; Hughes, D. Short-Term Folate, Vitamin B-12 or Vitamin B-6 supplementation slightly affects memory performance but not mood in women of various ages. J. Nutr. 2002, 132, 1345–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvaresi, E.; Bryan, J. B vitamins, cognition, and aging: A review. J. Gerontol. Ser. B 2001, 56, P327–P339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, R.H.; Fairfield, K.M. Vitamins for chronic disease prevention in adults, clinical applications. JAMA 2002, 287, 3127–3129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn-Lewis, C.; Kraemer, W.J.; Kupchak, B.R.; Kelly, N.A.; Creighton, B.A.; Luk, H.-Y.; Ballard, K.D.; Comstock, B.A.; Szivak, T.K.; Hooper, D.R.; et al. A multi-nutrient supplement reduced markers of inflammation and improved physical performance in active individuals of middle to older age: A randomized, double-blind, placebo-controlled study. Nutr. J. 2011, 10, 90. [Google Scholar] [CrossRef] [Green Version]
- Fairfield, K.M.; Fletcher, R.H. Vitamins for chronic disease prevention in adults. JAMA 2002, 287, 3116–3126. [Google Scholar] [CrossRef]
- Tully, D.B.; Allgood, V.E.; Cidlowski, J.A. Modulation of steroid receptor-mediated gene expression by vitamin B6. FASEB J. 1994, 8, 343–349. [Google Scholar] [CrossRef]
- Morris, M.S.; Picciano, M.F.; Jacques, P.F.; Selhub, J. Plasma pyridoxal 5′-phosphate in the US population: The National Health and Nutrition Examination Survey, 2003–2004. Am. J. Clin. Nutr. 2008, 87, 1446–1454. [Google Scholar] [CrossRef] [Green Version]
- Friso, S.; Girelli, D.; Martinelli, N.; Olivieri, O.; Lotto, V.; Bozzini, C.; Pizzolo, F.; Faccini, G.; Beltrame, F.; Corrocher, R. Low plasma vitamin B-6 concentrations and modulation of coronary artery disease risk. Am. J. Clin. Nutr. 2004, 79, 992–998. [Google Scholar] [CrossRef]
- Rimm, E.B.; Willett, W.C.; Hu, F.B.; Sampson, L.; Colditz, G.A.; E Manson, J.; Hennekens, C.; Stampfer, M.J. Folate and vitamin B6 from diet and supplements in relation to risk of coronary heart disease among women. JAMA 1998, 279, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Folsom, A.; Desvarieux, M.; Nieto, F.J.; Boland, L.L.; Ballantyne, C.M.; Chambless, L.E. B vitamin status and inflammatory markers. Atherosclerosis 2003, 169, 169–174. [Google Scholar] [CrossRef]
- Friso, S.; Jacques, P.F.; Wilson, P.W.; Rosenberg, I.H.; Selhub, J. Low circulating vitamin B(6) is associated with elevation of the inflammation marker C-reactive protein independently of plasma homocysteine levels. Circulation 2001, 103, 2788–2791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, S.; Vorster, H.H.; Venter, C.S.; Kruger, H.S.; Nell, T.A.; Veldman, F.J.; Ubbink, J.B. Nutritional status influences plasma fibrinogen concentration: Evidence from the THUSA survey. Thromb. Res. 2000, 98, 383–394. [Google Scholar] [CrossRef]
- Okada, M.; Shibuya, M.; Yamamoto, E.; Murakami, Y. Effect of diabetes on vitamin B6 requirement in experimental animals. Diabetes Obes. Metab. 1999, 1, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Roubenoff, R.; Roubenoff, R.A.; Selhub, J.; Nadeau, M.R.; Cannon, J.G.; Freeman, L.M.; Dinarello, C.A.; Rosenberg, I.H. Abnormal vitamin b6status in rheumatoid cachexia association with spontaneous tumor necrosis factor α production and markers of inflammation. Arthritis Rheum. 1995, 38, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Saibeni, S.; Cattaneo, M.; Vecchi, M.; Zighetti, M.L.; Lecchi, A.; Lombardi, R.; Meucci, G.; Spina, L.; de Franchis, R. Low vitamin B(6) plasma levels, a risk factor for thrombosis, in inflammatory bowel disease: Role of inflammation and correlation with acute phase reactants. Am. J. Gastroenterol. 2003, 98, 112–117. [Google Scholar] [CrossRef]
- Shen, J.; Lai, C.-Q.; Mattei, J.; Ordovás, J.M.; Tucker, K.L. Association of vitamin B-6 status with inflammation, oxidative stress, and chronic inflammatory conditions: The Boston Puerto Rican Health Study. Am. J. Clin. Nutr. 2009, 91, 337–342. [Google Scholar] [CrossRef]
- Wan, P.; Moat, S.; Anstey, A. Pellagra: A review with emphasis on photosensitivity. Br. J. Dermatol. 2011, 164, 1188–1200. [Google Scholar] [CrossRef]
- Villines, T.C.; Kim, A.S.; Gore, R.S.; Taylor, A.J. Niacin: The evidence, clinical use, and future directions. Curr. Atheroscler. Rep. 2011, 14, 49–59. [Google Scholar] [CrossRef]
- Bruckert, E.; Labreuche, J.; Amarenco, P. Meta-analysis of the effect of nicotinic acid alone or in combination on cardiovascular events and atherosclerosis. Atherosclerosis 2010, 210, 353–361. [Google Scholar] [CrossRef]
- Taylor, A.J.; Lee, H.J.; Sullenberger, L.E. The effect of 24 months of combination statin and extended-release niacin on carotid intima-media thickness: ARBITER 3. Curr. Med. Res. Opin. 2006, 22, 2243–2250. [Google Scholar] [CrossRef]
- Taylor, A.J.; Villines, T.C.; Stanek, E.J.; Devine, P.J.; Griffen, L.; Miller, M.; Weissman, N.J.; Turco, M. Extended-release niacin or ezetimibe and carotid intima–media thickness. N. Engl. J. Med. 2009, 361, 2113–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukasova, M.; Hanson, J.; Tunaru, S.; Offermanns, S. Nicotinic acid (niacin): New lipid-independent mechanisms of action and therapeutic potentials. Trends Pharmacol. Sci. 2011, 32, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Roy, B.; Singh, B.; Rizal, A.; Malik, C.P. Bioanalytical method development and validation of niacin and nicotinuric acid in human plasma by LC-MS/MS. Int. J. Pharm. Clin. Res. 2014, 6, 206–213. [Google Scholar]
- Cohen, K.; Gorecki, G.; Silverstein, S.; Ebersole, J.; Solomon, L. Effect of pyridoxine (vitamin B6) on diabetic patients with peripheral neuropathy. J. Am. Podiatr. Med. Assoc. 1984, 74, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J.M.; Folkers, K.; Minadeo, M.; VanBuskirk, R.; Xia, L.-J.; Tamagawa, H. A deficiency of vitamin B6 is a plausible molecular basis of the retinopathy of patients with diabetes mellitus. Biochem. Biophys. Res. Commun. 1991, 179, 615–619. [Google Scholar] [CrossRef]
- Hamaker, B.R.; Kirksey, A.; Borschel, M.W. Distribution of B-6 vitamers in human milk during a 24-h period after oral supplementation with different amounts of pyridoxine. Am. J. Clin. Nutr. 1990, 51, 1062–1066. [Google Scholar] [CrossRef]
- Taguchi, K.; Fukusaki, E.; Bamba, T. Determination of niacin and its metabolites using supercritical fluid chromatography coupled to tandem mass spectrometry. Mass Spectrom. 2014, 3, A0029. [Google Scholar] [CrossRef] [Green Version]
- Hamaker, B.; Kirksey, A.; Ekanayake, A.; Borschel, M. Analysis of B-6 vitamers in human milk by reverse-phase liquid chromatography. Am. J. Clin. Nutr. 1985, 42, 650–655. [Google Scholar] [CrossRef]
- Heydari, R.; Elyasi, N.S. Ion-pair cloud-point extraction: A new method for the determination of water-soluble vitamins in plasma and urine. J. Sep. Sci. 2014, 37, 2724–2731. [Google Scholar] [CrossRef]
- Hampel, D.; York, Y.R.; Allen, L.H. Ultra-performance liquid chromatography tandem mass-spectrometry (UPLC-MS/MS) for the rapid, simultaneous analysis of thiamin, riboflavin, flavin adenine dinucleotide, nicotinamide and pyridoxalin human milk. J. Chromatogr. B 2012, 903, 7–13. [Google Scholar] [CrossRef]
- Redeuil, K.M.; Redeuil, K.; Bénet, S.; Munari, C.; Giménez, E.C. Simultaneous quantification of 21 water soluble vitamin circulating forms in human plasma by liquid chromatography-mass spectrometry. J. Chromatogr. A 2015, 1422, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, J. Evaluation of the relative efficacy of various techniques for deprotenizing plasma samples prior to high performance liquid chromatographic analysis. J. Chromatogr. B 1981, 226, 455–460. [Google Scholar] [CrossRef]
- Polson, C.; Sarkar, P.; Incledon, B.; Raguvaran, V.; Grant, R. Optimization of protein precipitation based upon effectiveness of protein removal and ionization effect in liquid chromatography-tandem mass spectrometry. J. Chromatogr. B 2003, 785, 263–275. [Google Scholar] [CrossRef]
- Ubbink, J.B.; Serfontein, W.J.; de Villiers, L.S. Analytical Recovery of protein-bound pyridoxal-5′-phosphate in plasma analysis. J. Chromatogr. B 1986, 375, 399–404. [Google Scholar] [CrossRef]
- Lumeng, L.; Brashear, R.E.; Li, T.K. Pyridoxal 5′-phosphate in plasma: Source, protein-binding, and cellular transport. J. Lab. Clin. Med. 1974, 84, 334–343. [Google Scholar]
- Bates, C.J.; Pentieva, K.D.; Matthews, N.; Macdonald, A. A simple, sensitive and reproducible assay for pyridoxal 5′-phospate and 4-pyridoxic acid in human plasma. Clin. Chem. Acta 1999, 280, 101–111. [Google Scholar] [CrossRef]
- Zhou, S.-S.; Li, D.; Chen, N.-N.; Zhou, Y. Vitamin paradox in obesity: Deficiency or excess? World J. Diabetes 2015, 6, 1158–1167. [Google Scholar] [CrossRef]
- Midttun, Ø.; Hustad, S.; Solheim, E.; Schneede, J.; Ueland, P.M. Multianalyte Quantification of Vitamin B6 and B2 Species in the nanomolar range in human plasma by liquid chromatography–tandem mass spectrometry. Clin. Chem. 2005, 51, 1206–1216. [Google Scholar] [CrossRef] [Green Version]
Sample Availability: Samples and compounds mentioned in the manuscript are available from the authors. |



{kind=link}
{kind=link}
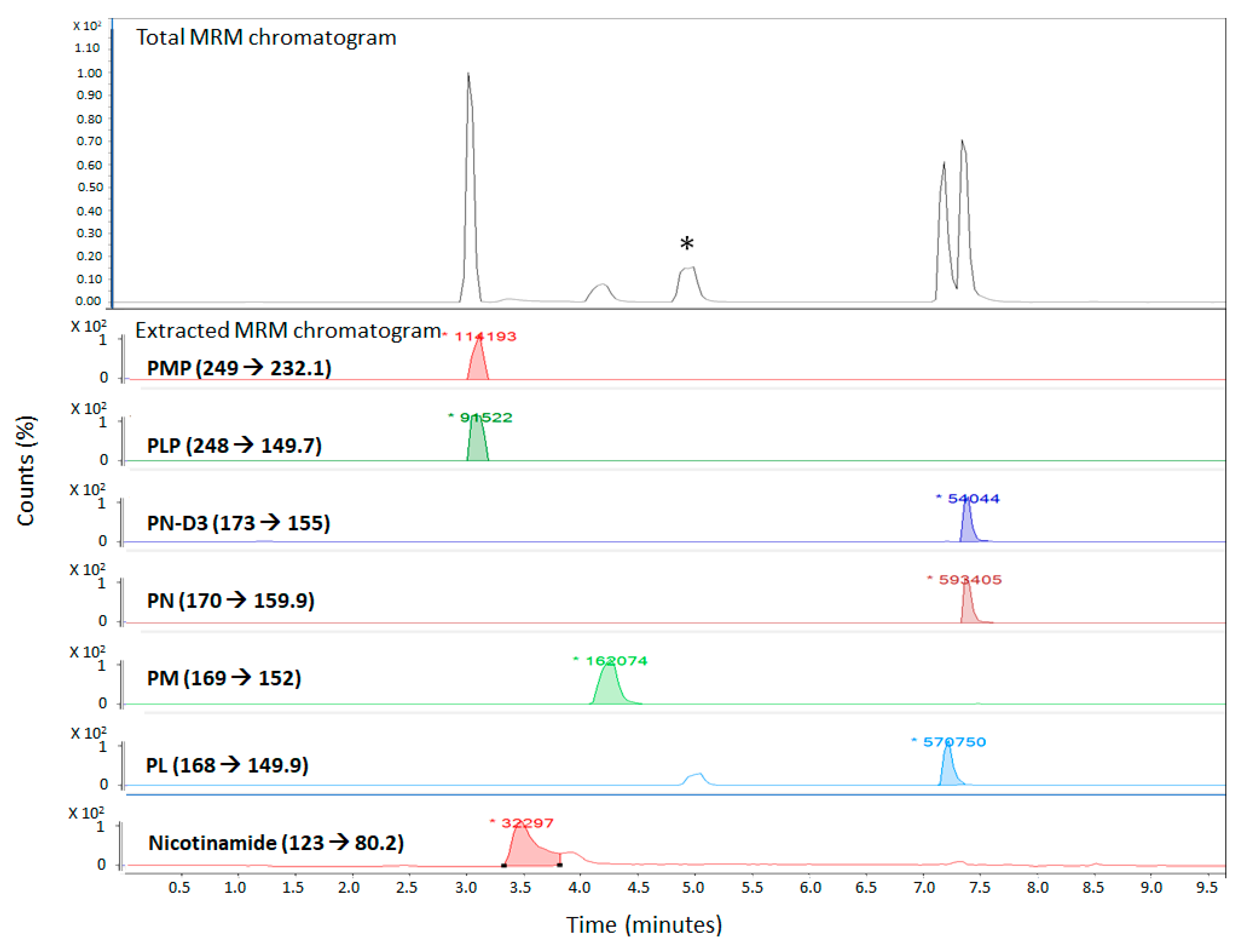
| Name | Vitamer Structure | Mass (g/mol) | Precursor Ion [M + H]+ (m/z) | Product Ion [M + H]+ (m/z) | Fragmentor Voltage (V) | Collision Energy (eV) |
|---|---|---|---|---|---|---|
| Pyridoxal-5′-phosphate (PLP) |  C8H10NO6P | 247 | 248 | 149.7 | 45 | 15 |
| Pyridoxal hydrochloride (PL) |  C8H9NO3 · HCl | 203.63 167.06 (-HCl) | 168 | 149.9 | 94 | 10 |
| Pyridoxamine dihydrochloride (PM) |  C8H12N2O2 · 2HCl | 241.11 168.09 (-2HCl) | 169 | 152 | 45 | 10 |
| Pyridoxamine-5′-phosphate (PMP) |  C8H13N2O5P | 248 | 249 | 232.1 | 94 | 10 |
| Pyridoxine hydrochloride (PN) |  C8H11NO3 · HCl | 205.64 169.07 (-HCl) | 170 | 151.9 | 94 | 10 |
| Nicotinamide |  C6H6N2O | 122.12 | 123 | 80.2 | 94 | 20 |
| Pyridoxine-(methyl-d3) hydrochloride |  C8D3H8NO3·HCl | 208.6 | 173 | 155 | 94 | 10 |
| Analyte | Recovery (%) | Standard Deviation |
|---|---|---|
| PLP | 121.3 | 19.2 |
| PM | 82.5 | 1.8 |
| PL | 118.0 | 25.6 |
| PN | 102.8 | 2.6 |
| PMP | 100.8 | 34.1 |
| Nicotinamide | 83.6 | 9.2 |
| PN-D3 | 95.2 | 2.6 |
| Analyte | LLOD (pg) | LLOQ (pg) |
|---|---|---|
| PLP | 0.66 | 56.0 |
| PL | 6.0 | 18.4 |
| PMP | 6.0 | 18.4 |
| PM | 18.0 | 56.0 |
| PN | 2.0 | 6.0 |
| Nicotinamide | 4400 | 4400 |
| PMP | PLP | PN | PM | PL | Nicotinamide | |
|---|---|---|---|---|---|---|
| Sample | Concentration (nM) | |||||
| 1 | 42.9 | n.d. * | 25.6 | n.d. | 20.3 | 1365.0 |
| 2 | 36.5 | 35.3 | 25.0 | n.d. | 84.3 | 544.9 |
| 3 | 21.0 | n.d. | 18.1 | n.d. | 66.8 | 2600.6 |
| 4 | 35.9 | 30.6 | 13.3 | n.d. | 53.8 | 1035.9 |
| 5 | 29.7 | n.d. | 19.2 | n.d. | 24.5 | 2492.7 |
| 6 | 21.4 | 23.5 | 14.9 | n.d. | 33.6 | 1338.1 |
| 7 | 30.7 | 17.6 | 12.7 | n.d. | 34.3 | 776.9 |
| 8 | 20.0 | n.d. | 12.3 | n.d. | 32.6 | 949.6 |
| 9 | 18.6 | 18.8 | 13.3 | n.d. | 23.8 | 2881.2 |
| 10 | 36.3 | n.d. | 11.3 | n.d. | 27.5 | 1138.4 |
| 11 | 21.6 | n.d. | 9.9 | n.d. | 31.1 | 3032.2 |
| 12 | 21.4 | n.d. | 15.7 | n.d. | 21.6 | 588.1 |
| 13 | 13.8 | n.d. | 17.0 | n.d. | 22.6 | 1143.8 |
| 14 | 17.1 | 38.4 | 9.5 | n.d. | 44.5 | 393.9 |
| 15 | 18.1 | n.d. | 22.4 | n.d. | 13.8 | 884.8 |
| 16 | 28.2 | n.d. | 23.2 | n.d. | 51.4 | 491.0 |
| 17 | 23.7 | n.d. | 18.4 | n.d. | 53.3 | 841.7 |
| 18 | 34.2 | n.d. | 22.7 | n.d. | 50.2 | 286.0 |
| 19 | 33.6 | n.d. | 16.3 | n.d. | 44.6 | 701.4 |
| 20 | 35.0 | 20.0 | 20.9 | n.d. | 58.6 | 1251.7 |
| 21 | 23.3 | n.d. | 30.8 | n.d. | 57.7 | 458.6 |
| 22 | 30.7 | 90.5 | 28.7 | n.d. | 130.1 | n.d. |
| 23 | 30.9 | n.d. | 21.6 | n.d. | 46.7 | 669.0 |
| 24 | 27.2 | 30.6 | 21.6 | n.d. | 53.6 | 1381.2 |
| 25 | 38.3 | n.d. | 19.8 | n.d. | 42.7 | 415.4 |
| 26 | 29.3 | n.d. | 19.4 | n.d. | 43.9 | 577.3 |
| 27 | 45.1 | n.d. | 19.9 | n.d. | 44.0 | 863.3 |
| 28 | 19.0 | n.d. | 21.9 | n.d. | 11.3 | 604.3 |
| 29 | 52.2 | n.d. | 18.3 | n.d. | 53.0 | 750.0 |
| 30 | 56.9 | n.d. | 13.1 | n.d. | 32.7 | 1084.5 |
| 31 | 82.3 | 38.0 | 17.5 | n.d. | 60.1 | 825.5 |
| 32 | 47.4 | n.d. | 21.0 | n.d. | 38.5 | 1165.4 |
| 33 | 51.7 | n.d. | 19.5 | n.d. | 32.2 | 1764.3 |
| 34 | 21.4 | n.d. | 22.0 | n.d. | 46.5 | 2390.2 |
| 35 | 26.6 | 18.8 | 19.4 | n.d. | 37.7 | 6005.1 |
| 36 | 35.9 | 68.9 | 19.1 | n.d. | 95.9 | 3620.3 |
| 37 | 41.2 | n.d. | 19.1 | n.d. | 32.5 | 830.9 |
| 38 | 27.4 | n.d. | 22.2 | n.d. | 42.0 | 965.8 |
| 39 | 13.8 | n.d. | 19.9 | n.d. | 42.0 | 1705.0 |
| 40 | 11.3 | n.d. | 22.8 | n.d. | 39.7 | 690.6 |
| 41 | 13.8 | n.d. | 20.3 | n.d. | 41.2 | 572.7 |
| 42 | 10.9 | n.d. | 21.7 | n.d. | 47.9 | 793.1 |
| 43 | 20.2 | n.d. | 21.0 | n.d. | 32.9 | 2303.8 |
| 44 | 26.6 | n.d. | 17.5 | n.d. | 48.9 | n.d. |
| 45 | 14.6 | n.d. | 19.3 | n.d. | 50.7 | 566.5 |
| 46 | 19.2 | n.d. | 22.1 | n.d. | 52.1 | 1348.9 |
| 47 | 35.9 | 37.6 | 24.3 | n.d. | 88.8 | 1980.1 |
| 48 | 15.9 | n.d. | 26.6 | n.d. | 43.3 | n.d. |
| 49 | 63.3 | n.d. | 27.1 | n.d. | 41.2 | 588.1 |
| 50 | 16.7 | n.d. | 28.2 | n.d. | 52.3 | 372.3 |
| 51 | 28.4 | n.d. | 26.0 | n.d. | 49.5 | 755.4 |
| 52 | 22.7 | n.d. | 30.1 | n.d. | 52.2 | 1429.8 |
| 53 | 21.4 | n.d. | 31.8 | n.d. | 49.0 | 302.1 |
| 54 | 55.9 | 35.6 | 32.4 | n.d. | 58.2 | 388.5 |
| 55 | 29.9 | n.d. | 33.2 | n.d. | 48.4 | 275.2 |
| 56 | 43.1 | n.d. | 28.5 | n.d. | 36.0 | 825.5 |
| 40 | 11.3 | n.d. | 22.8 | n.d. | 39.7 | 690.6 |
| Average | 30.2 | 36.0 | 21.0 | n.d | 45.8 | 1206.5 |
| Max | 82.3 | 90.5 | 33.2 | n.d | 130.1 | 6005.1 |
| Min | 10.9 | n.d. | 9.5 | n.d | 11.3 | 275.2 |
| PMP | PLP | PN | PM | PL | Nicotinamide | |
|---|---|---|---|---|---|---|
| Sample | Concentration (nM) | |||||
| 1 | 12.0 | n.d. * | 24.7 | n.d. | 51.5 | 5471.0 |
| 2 | 34.4 | n.d. | 20.8 | n.d. | n.d. | 1823.7 |
| 3 | 13.6 | n.d. | 21.7 | n.d. | 48.4 | 1348.9 |
| 4 | n.d. | n.d. | 39.5 | n.d. | n.d. | n.d. |
| 5 | 64.3 | 26.2 | 20.9 | n.d. | 114.9 | 2314.6 |
| 6 | 27.8 | n.d. | 20.1 | n.d. | 58.3 | 1246.3 |
| 7 | 69.1 | n.d. | 21.0 | n.d. | 46.4 | 3118.6 |
| 8 | 14.2 | n.d. | 26.3 | n.d. | 62.2 | 1516.1 |
| 9 | 79.2 | 29.8 | 25.8 | n.d. | 74.7 | 2514.3 |
| 10 | 37.1 | n.d. | 23.8 | n.d. | 57.0 | n.d. |
| 11 | 36.1 | 30.2 | 27.2 | n.d. | 41.7 | n.d. |
| 12 | 28.7 | n.d. | 24.5 | n.d. | 45.4 | n.d. |
| 13 | 46.4 | n.d. | 23.4 | n.d. | 57.9 | n.d. |
| 14 | 15.0 | n.d. | 23.6 | n.d. | n.d. | 2044.9 |
| 15 | 14.4 | n.d. | 30.8 | n.d. | n.d. | 2217.5 |
| 16 | 24.1 | n.d. | 25.8 | n.d. | n.d. | 2854.2 |
| 17 | 31.3 | 36.8 | 21.2 | n.d. | 70.0 | 3177.9 |
| 18 | 77.9 | n.d. | 35.3 | n.d. | 63.1 | 2082.6 |
| 19 | 15.9 | 69.3 | 28.7 | n.d. | 95.1 | 3679.7 |
| 20 | 33.2 | n.d. | 24.4 | n.d. | 41.2 | 3323.6 |
| 21 | 20.6 | n.d. | 26.1 | n.d. | 57.6 | n.d. |
| 22 | 24.3 | 61.5 | 21.3 | n.d. | 97.3 | 1818.3 |
| 23 | 22.5 | n.d. | 20.3 | n.d. | 41.4 | 5956.5 |
| 24 | 18.6 | n.d. | 21.1 | n.d. | 41.1 | 6167.0 |
| 25 | 59.8 | n.d. | 28.0 | n.d. | 40.7 | 2271.5 |
| 26 | 42.9 | n.d. | 29.1 | n.d. | 86.2 | 1645.6 |
| 27 | 18.3 | n.d. | 22.4 | n.d. | 41.5 | 4526.8 |
| 28 | 33.2 | n.d. | 25.0 | n.d. | 40.0 | 3275.0 |
| 29 | 21.2 | n.d. | 23.4 | n.d. | 70.1 | 4402.7 |
| 30 | 16.1 | n.d. | 20.6 | n.d. | 54.3 | 3258.8 |
| 31 | 77.3 | n.d. | 12.6 | n.d. | 56.7 | 5287.5 |
| 32 | 32.4 | 22.7 | 11.8 | n.d. | 62.6 | 8810.7 |
| 33 | 94.8 | n.d. | 14.3 | n.d. | 59.0 | 2401.0 |
| 34 | 86.0 | n.d. | 14.8 | n.d. | 35.8 | 1494.5 |
| 35 | 38.8 | n.d. | 24.3 | n.d. | 93.9 | 5406.2 |
| 36 | 243.9 | n.d. | 18.0 | n.d. | 63.6 | 9625.4 |
| 37 | 138.3 | n.d. | 20.7 | n.d. | 65.3 | 11,303.4 |
| 38 | 44.3 | n.d. | 12.1 | n.d. | 76.3 | 5109.5 |
| 39 | 100.6 | n.d. | 12.0 | n.d. | 58.3 | 4337.9 |
| 40 | 95.4 | n.d. | 6.7 | n.d. | 75.6 | 3345.2 |
| 41 | 101.0 | n.d. | n.d. | n.d. | 58.3 | 4105.9 |
| 42 | 47.8 | n.d. | 20.7 | n.d. | n.d. | n.d. |
| 43 | 25.6 | n.d. | 17.6 | n.d. | n.d. | 3998.0 |
| 44 | 34.8 | n.d. | 21.8 | n.d. | n.d. | 3064.6 |
| 45 | 90.9 | n.d. | 16.4 | n.d. | n.d. | 3933.3 |
| 46 | 168.2 | 27.8 | 21.3 | n.d. | 60.6 | 1386.6 |
| 47 | 17.5 | n.d. | 19.2 | n.d. | n.d. | 7181.3 |
| 48 | 27.2 | n.d. | 12.7 | n.d. | 25.2 | 10,693.7 |
| 49 | 191.9 | n.d. | 7.7 | n.d. | n.d. | 372.3 |
| 50 | 65.3 | n.d. | 13.5 | n.d. | n.d. | 2832.6 |
| 51 | 53.8 | n.d. | 15.4 | n.d. | n.d. | 2498.1 |
| 52 | 19.8 | n.d. | 14.0 | n.d. | n.d. | 3884.7 |
| 53 | 39.0 | n.d. | 7.8 | n.d. | n.d. | 3965.6 |
| 54 | 87.2 | n.d. | 12.9 | n.d. | n.d. | 933.4 |
| 55 | 26.8 | n.d. | 9.5 | n.d. | n.d. | 2476.5 |
| 56 | 54.6 | n.d. | 11.4 | n.d. | n.d. | 2633.0 |
| 57 | 23.7 | n.d. | 8.8 | n.d. | n.d. | 3539.4 |
| Average | 53.2 | 38.0 | 20.1 | n.d. | 60.2 | 3733.5 |
| Max | 243.9 | 69.3 | 39.5 | n.d. | 114.9 | 11,303.4 |
| Min | 12.0 | n.d. | 6.7 | n.d. | n.d | 372.3 |
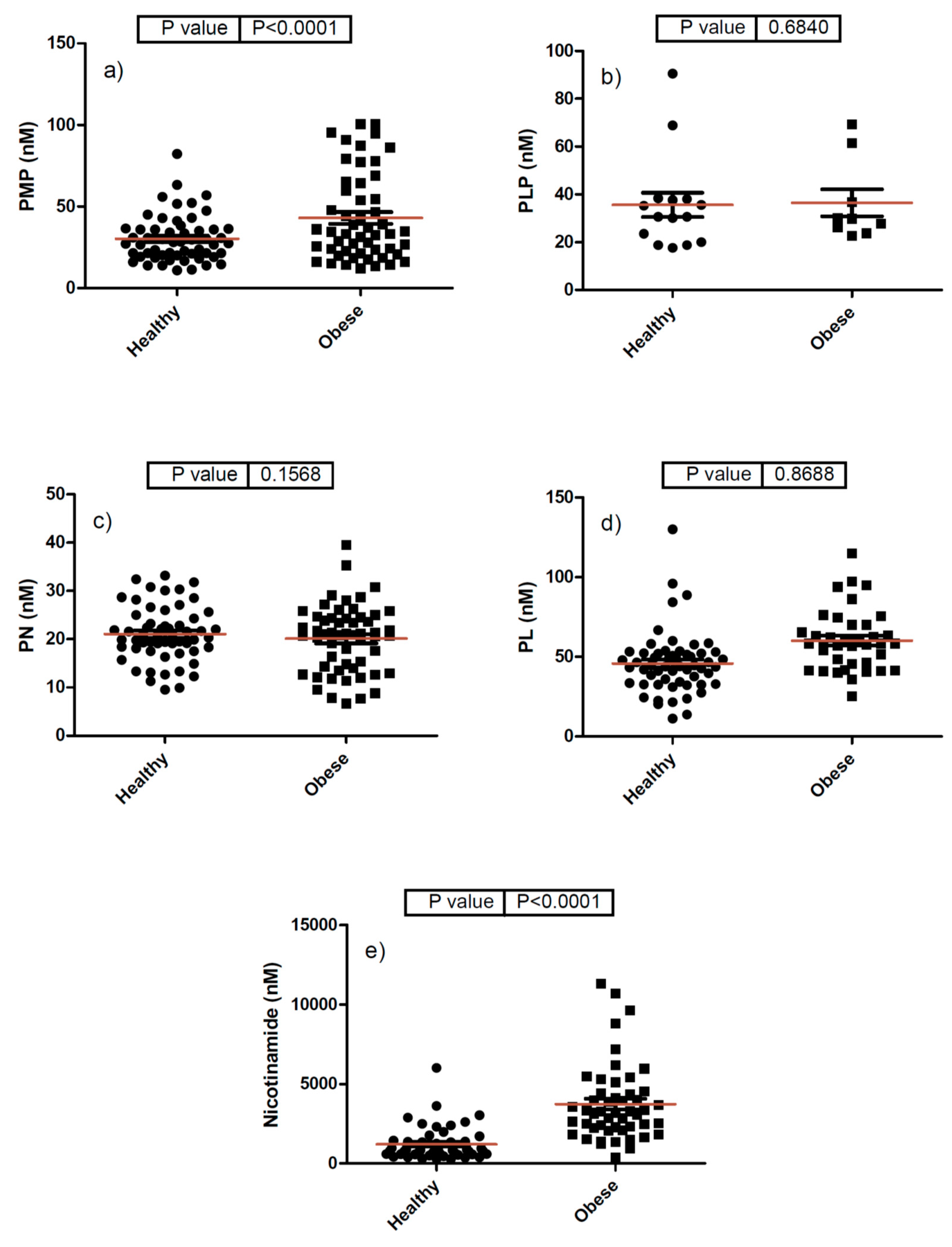
| Analyte (nM) | Healthy Plasma | Obese Plasma | ||||
|---|---|---|---|---|---|---|
| Average | Max | Min | Average | Max | Min | |
| PMP | 30.2 | 82.3 | 10.9 | 53.2 | 243.9 | 12.0 |
| PLP | 36.0 | 90.5 | n.d. * | 38.0 | 69.3 | n.d. |
| PN | 21.0 | 33.2 | 9.5 | 20.1 | 39.5 | 6.7 |
| PM | n.d. | |||||
| PL | 45.8 | 130.1 | 11.3 | 60.2 | 114.9 | n.d. |
| Nicotinamide | 1206.5 | 6005.1 | 275.2 | 3733.5 | 11303.4 | 372.3 |
| Analyte (nM) | Healthy Emirati Plasma | US Population [41] | European Population [48] | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Average | Max | Min | Average | Max | Min | Average | Max | Min | |
| PMP | 30.2 | 82.3 | 10.9 | 4.9 | 7.6 | 2.1 | Not detected | ||
| PLP | 36.0 | 90.5 | n.d. | 92.1 | 163.3 | 20.9 | 34.4 | 102.3 | 17.0 |
| PN | 21.0 | 33.2 | 9.5 | 142.8 | 285.4 | 0.2 | Not detected | ||
| PM | Not detected | 4.1 | 7.7 | 0.4 | Not detected | ||||
| PL | 45.8 | 130.1 | 11.3 | 118.4 | 233.5 | 3.2 | 9.9 | 28.2 | 5.7 |
| Nicotinamide | 1206.5 | 6005.1 | 275.2 | 274.4 | 479.6 | 69.1 | Not included | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, G.R.; Shah, I.; Gariballa, S.; Yasin, J.; Barker, J.; Salman Ashraf, S. Significantly Elevated Levels of Plasma Nicotinamide, Pyridoxal, and Pyridoxamine Phosphate Levels in Obese Emirati Population: A Cross-Sectional Study. Molecules 2020, 25, 3932. https://doi.org/10.3390/molecules25173932
Ibrahim GR, Shah I, Gariballa S, Yasin J, Barker J, Salman Ashraf S. Significantly Elevated Levels of Plasma Nicotinamide, Pyridoxal, and Pyridoxamine Phosphate Levels in Obese Emirati Population: A Cross-Sectional Study. Molecules. 2020; 25(17):3932. https://doi.org/10.3390/molecules25173932
Chicago/Turabian StyleIbrahim, Ghada Rashad, Iltaf Shah, Salah Gariballa, Javed Yasin, James Barker, and Syed Salman Ashraf. 2020. "Significantly Elevated Levels of Plasma Nicotinamide, Pyridoxal, and Pyridoxamine Phosphate Levels in Obese Emirati Population: A Cross-Sectional Study" Molecules 25, no. 17: 3932. https://doi.org/10.3390/molecules25173932
APA StyleIbrahim, G. R., Shah, I., Gariballa, S., Yasin, J., Barker, J., & Salman Ashraf, S. (2020). Significantly Elevated Levels of Plasma Nicotinamide, Pyridoxal, and Pyridoxamine Phosphate Levels in Obese Emirati Population: A Cross-Sectional Study. Molecules, 25(17), 3932. https://doi.org/10.3390/molecules25173932