
Artificial Caries Lesion Characteristics after Secondary Demineralization with Theobromine-Containing Protocol



Abstract
1. Introduction
2. Results
3. Materials and Methods
3.1. Specimen Preparation and Initial Demineralization
3.2. Secondary Demineralization
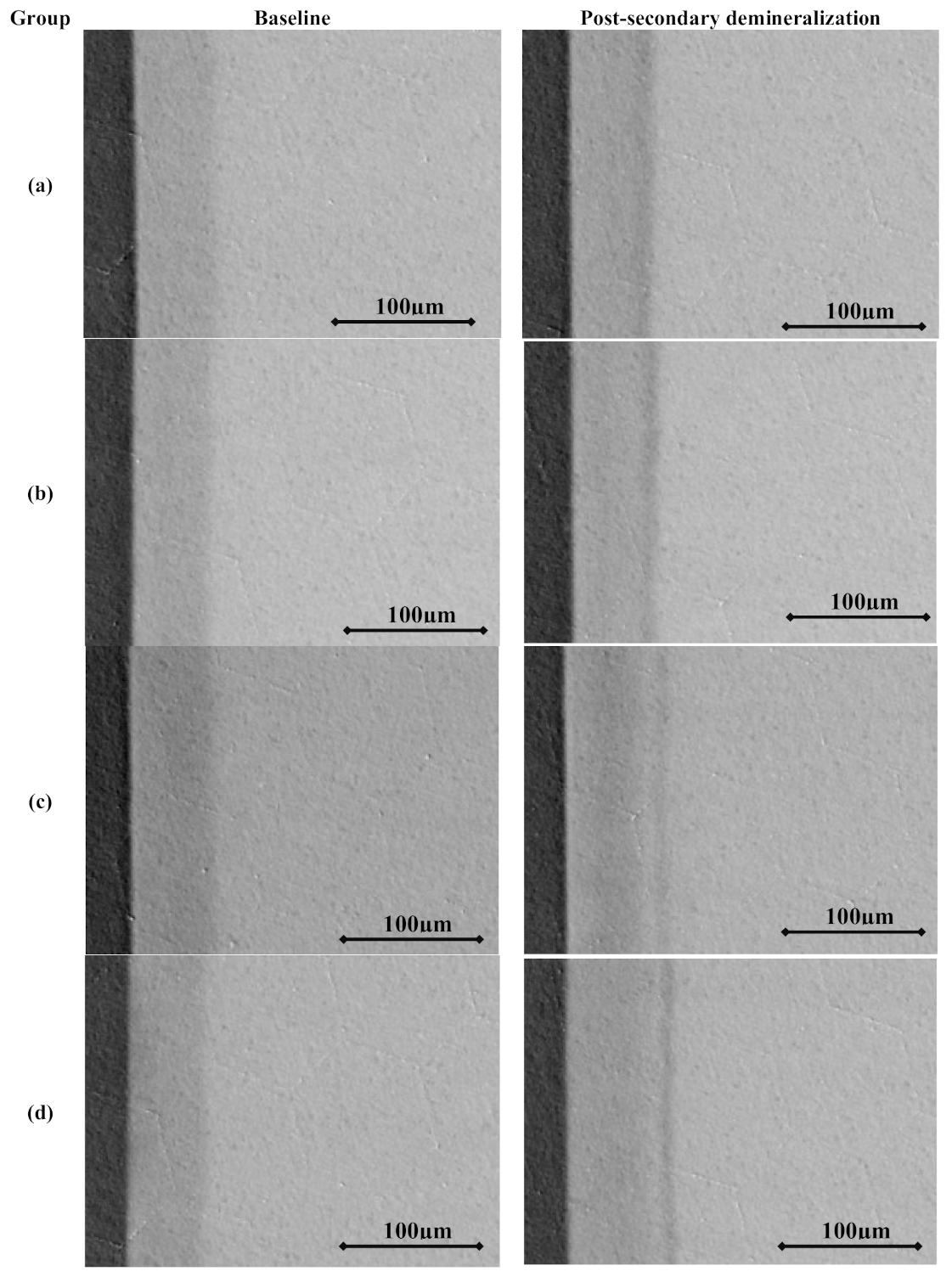
3.3. Transverse Microradiographic Analysis
3.4. Statistical Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TMR | Transverse microradiography |
| L | Lesion depth |
| ΔL | Changes in lesion depth |
| SZmax | Degree of surface layer mineralization |
| ΔSZmax | Changes in surface layer mineralization |
| ΔZ | Mineral content |
| ΔΔZ | Changes in mineral content |
References
- Jin, L.J.; Lamster, I.B.; Greenspan, J.S.; Pitts, N.B.; Scully, C.; Warnakulasuriya, S. Global burden of oral diseases: Emerging concepts, management and interplay with systemic health. Oral Dis. 2016, 22, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Young, D.A.; Featherstone, J.D.; Roth, J.R. Curing the silent epidemic: Caries management in the 21st century and beyond. J. Calif. Dent. Assoc. 2007, 35, 681–685. [Google Scholar] [PubMed]
- Featherstone, J.D. Dental caries: A dynamic disease process. Aust. Dent. J. 2008, 53, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Zero, D.T. Dental caries process. Dent. Clin. N. Am. 1999, 43, 635–664. [Google Scholar] [PubMed]
- Wiegand, A.; Buchalla, W.; Attin, T. Review on fluoride-releasing restorative materials—Fluoride release and uptake characteristics, antibacterial activity and influence on caries formation. Dent. Mater. 2007, 23, 343–362. [Google Scholar] [CrossRef] [PubMed]
- Adair, S.M. Evidence-based use of fluoride in contemporary pediatric dental practice. Pediatr. Dent. 2006, 28, 133–142; discussion 192–198. [Google Scholar] [PubMed]
- Ten Cate, J.M. In Vitro studies on the effects of fluoride on de- and remineralization. J. Dent. Res. 1990, 69, 614–619; discussion 634–636. [Google Scholar] [CrossRef]
- Nassar, H.M.; Lippert, F.; Eckert, G.J.; Hara, A.T. Dentifrice fluoride and abrasivity interplay on artificial caries lesions. Caries Res. 2014, 48, 557–565. [Google Scholar] [CrossRef]
- Nakamoto, T.; Simmons, W.B., Jr.; Falster, A.U. Products of apatite-forming-systems. U.S. Patent application number: US 5919426A, 6 July 1999. [Google Scholar]
- Nakamoto, T.; Simmons, W.B., Jr.; Falster, A.U. Apatite-forming-systems: Methods and products. U.S. Patent application number: US 6183711B1, 6 February 2001. [Google Scholar]
- Amaechi, B.T.; Porteous, N.; Ramalingam, K.; Mensinkai, P.K.; Ccahuana Vasquez, R.A.; Sadeghpour, A.; Nakamoto, T. Remineralization of artificial enamel lesions by theobromine. Caries Res. 2013, 47, 399–405. [Google Scholar] [CrossRef]
- Kargul, B.; Özcan, M.; Peker, S.; Nakamoto, T.; Simmons, W.B.; Falster, A.U. Evaluation of human enamel surfaces treated with theobromine: A pilot study. Oral Health Prev. Dent. 2012, 10, 275–282. [Google Scholar] [PubMed]
- Amaechi, B.T.; Mathews, S.M.; Mensinkai, P.K. Effect of theobromine-containing toothpaste on dentin tubule occlusion in situ. Clin. Oral Investig. 2015, 19, 109–116. [Google Scholar] [CrossRef]
- Herisa, H.; Noerdin, A.; Eriwati, Y.K. The effect of theobromine 200mg/l topical gel exposure duration against surface enamel hardness resistance from 1% citric acid. J. Phys. Conf. Ser. 2017, 884, 012009. [Google Scholar] [CrossRef]
- Premnath, P.; John, J.; Manchery, N.; Subbiah, G.K.; Nagappan, N.; Subramani, P. Effectiveness of Theobromine on Enamel Remineralization: A Comparative In Vitro Study. Cureus 2019, 11, e5686. [Google Scholar] [CrossRef] [PubMed]
- White, D.J. Use of synthetic polymer gels for artificial carious lesion preparation. Caries Res. 1987, 21, 228–242. [Google Scholar] [CrossRef]
- Lynch, R.J.; Ten Cate, J.M. The effect of lesion characteristics at baseline on subsequent de- and remineralisation behaviour. Caries Res. 2006, 40, 530–535. [Google Scholar] [CrossRef]
- De Jong, E.; Ten Bosch, J.; Noordmans, J. Optimised microcomputer-guided quantitative microradiography on dental mineralised tissue slices. Phys. Med. Biol. 1987, 32, 887. [Google Scholar] [CrossRef]
- Angmar, B.; Carlström, D.; Glas, J.-E. Studies on the ultrastructure of dental enamel: IV. The mineralization of normal human enamel. J. Ultrastruct. Res. 1963, 8, 12–23. [Google Scholar] [CrossRef]
- Lippert, F.; Lynch, R.J. Comparison of Knoop and Vickers surface microhardness and transverse microradiography for the study of early caries lesion formation in human and bovine enamel. Arch. Oral Biol. 2014, 59, 704–710. [Google Scholar] [CrossRef]
- Gantt, D.; Silverstone, L.; Featherstone, M.; Hicks, M. Structural comparison of sound and demineralized human and bovine enamel. J. Dent. Res. 1984, 63, 273. [Google Scholar]
- Yassen, G.H.; Platt, J.A.; Hara, A.T. Bovine teeth as substitute for human teeth in dental research: A review of literature. J. Oral Sci. 2011, 53, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Lippert, F. The effects of fluoride, strontium, theobromine and their combinations on caries lesion rehardening and fluoridation. Arch. Oral Biol. 2017, 80, 217–221. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Fluoride (ppm) | Theo-bromine (ppm) | n | Mineral Loss – ΔZ (vol.%) | Lesion Depth – L (µm) | Surface Zone Mineralization –SZmax (vol.%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | ΔΔZ | p-Value for Paired t-Test 1 | Pre | Post | ΔL | p-Value for Paired t-Test 1 | Pre | Post | ΔSZmax | p-Value for Paired t-Test 1 | ||||
| A | 0 | 50 | 11 | 1607.3 (253.6)A/a | 1995.5 (331.6) | −388.2 (306.1)B/a | 0.002 | 65.4 (8.5)A/a | 72.3 (9.9) | −6.9 (6.7)B/a | 0.006 | 63.2 (4.4)A/a | 63.8 (4.2) | −0.6 (4.3)A/a | 0.677 |
| B | 0 | 200 | 14 | 1667.9 (280.2)A/a | 2236.4 (477.3) | −568.6 (343.3)B/a | < 0.001 | 66.7 (9.3)A/a | 80.2 (13.7) | −13.5 (7.8)B/a,b | < 0.001 | 64.3 (5.6)A/a | 64.0 (6.9) | 0.3 (6.4)A/a | 0.857 |
| C | 1 | 50 | 15 | 1674.0 (318.5)A/a | 2045.3 (244.6) | −371.3 (376.7)B/a | < 0.001 | 66.1 (8.8)A/a | 85.4 (8.1) | −19.3 (9.7)B/b | < 0.001 | 64.9 (4.2)A/a | 66.9 (4.5) | −2.0 (4.5)A/a | 0.114 |
| D | 1 | 200 | 14 | 1506.4 (435.8)A/a | 1875.7 (391.4) | −369.3 (271.1)B/a | < 0.001 | 63.7 (13.5)A/a | 81.1 (13.0) | −17.3 (7.3)B/b | < 0.001 | 63.9 (6.9)A/a | 65.5 (5.6) | −1.7 (5.1)A/a | 0.242 |
| p-value for ANOVA 2 | 0.516 | - | 0.319 | - | 0.882 | - | 0.002 | - | 0.875 | - | 0.629 | - | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nassar, H.M.; Lippert, F. Artificial Caries Lesion Characteristics after Secondary Demineralization with Theobromine-Containing Protocol. Molecules 2021, 26, 300. https://doi.org/10.3390/molecules26020300
Nassar HM, Lippert F. Artificial Caries Lesion Characteristics after Secondary Demineralization with Theobromine-Containing Protocol. Molecules. 2021; 26(2):300. https://doi.org/10.3390/molecules26020300
Chicago/Turabian StyleNassar, Hani M., and Frank Lippert. 2021. "Artificial Caries Lesion Characteristics after Secondary Demineralization with Theobromine-Containing Protocol" Molecules 26, no. 2: 300. https://doi.org/10.3390/molecules26020300
APA StyleNassar, H. M., & Lippert, F. (2021). Artificial Caries Lesion Characteristics after Secondary Demineralization with Theobromine-Containing Protocol. Molecules, 26(2), 300. https://doi.org/10.3390/molecules26020300