
Bone Dimensional Change Following Immediate Implant Placement in Posterior Teeth with CBCT: A 6-Month Prospective Clinical Study

 , and
, and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Subject Selection
4.2. Research Procedure
4.2.1. Pre-Operative Phase
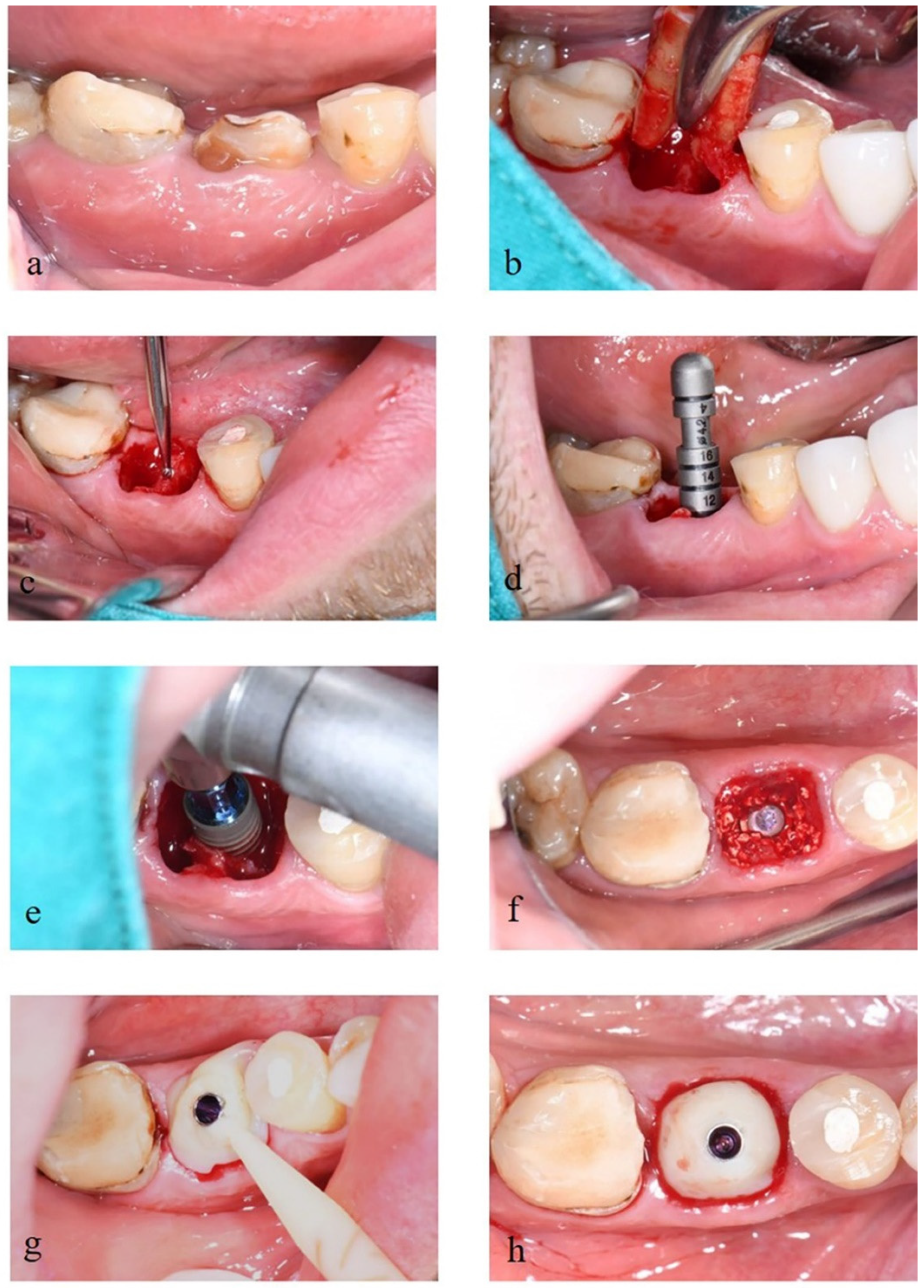
4.2.2. Operative Phase
4.2.3. Post-Operative Phase
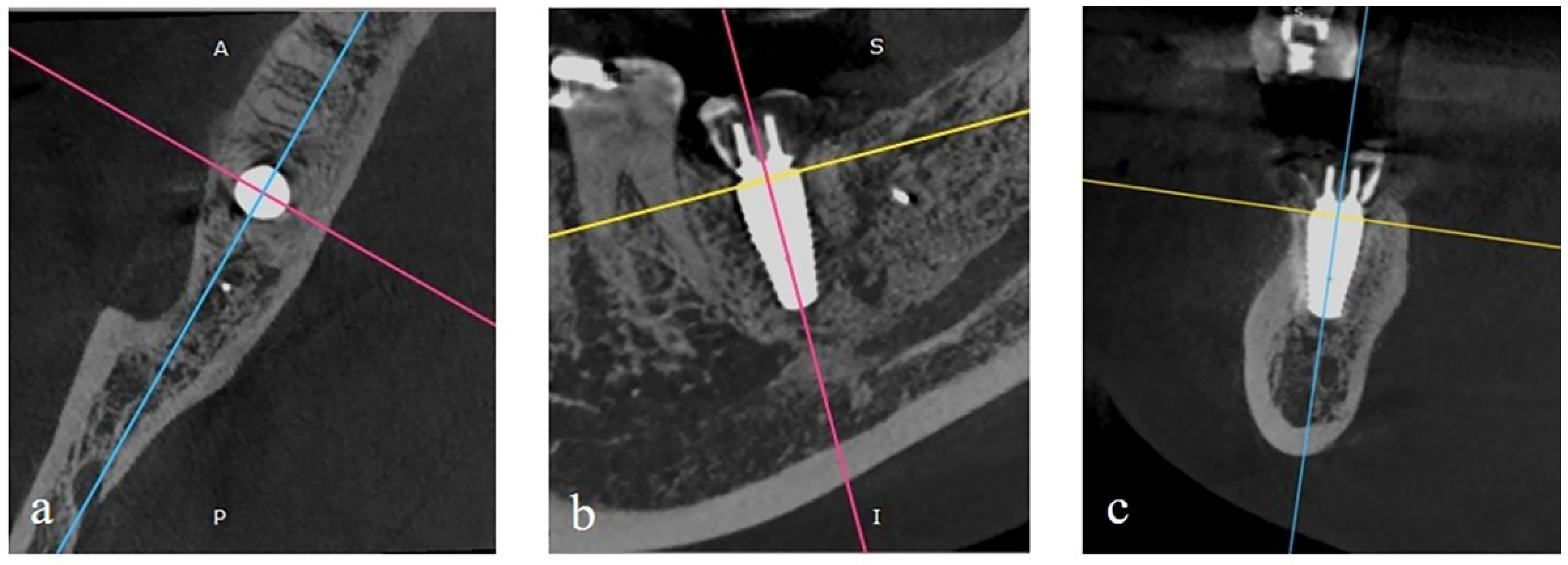
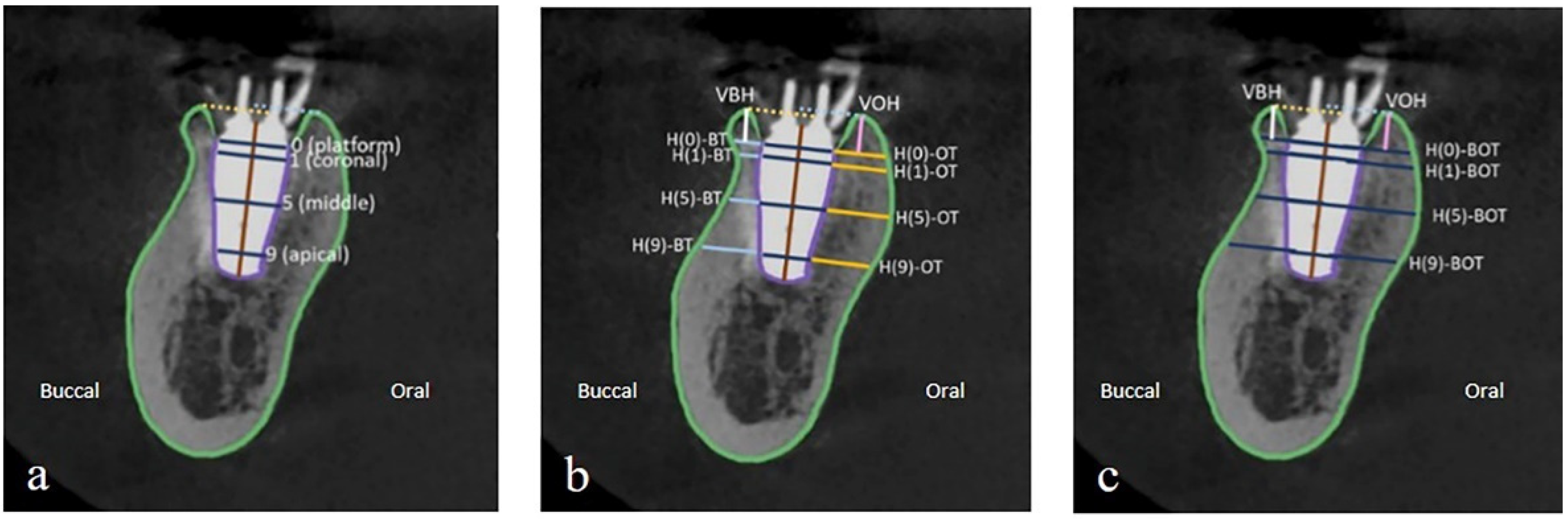
4.3. Outcome Measurement
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Pietrokovski, J.; Massler, M. Alveolar ridge resorption following tooth extraction. J. Prosthet. Dent. 1967, 17, 21–27. [Google Scholar] [CrossRef]
- Hattingh, A.; de Bruyn, H.; van Weehaeghe, M.; Hommez, G.; Vandeweghe, S. Contour changes following immediate placement of ultra-wide implants in molar extraction sockets without bone grafting. J. Clin. Med. 2020, 9, 2504. [Google Scholar] [CrossRef]
- Discepoli, N.; Vignoletti, F.; Laino, L.; de Sanctis, M.; Muñoz, F.; Sanz, M. Early healing of the alveolar process after tooth extraction: An experimental study in the beagle dog. J. Clin. Periodontol. 2013, 40, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Ridge alterations following implant placement in fresh extraction sockets: An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 645–652. [Google Scholar] [CrossRef]
- Hämmerle, C.H.; Chen, S.T.; Wilson, T.G., Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Botermans, A.; Lidén, A.; de Carvalho Machado, V.; Chrcanovic, B.R. Immediate implant placement in the maxillary aesthetic zone: A cone beam computed tomography study. J. Clin. Med. 2021, 10, 5853. [Google Scholar] [CrossRef]
- De Angelis, N.; Signore, A.; Alsayed, A.; Hai Hock, W.; Solimei, L.; Barberis, F.; Amaroli, A. Immediate implants in the aesthetic zone: Is socket shield technique a predictable treatment option? A narrative review. J. Clin. Med. 2021, 10, 4963. [Google Scholar] [CrossRef]
- Denissen, H.W.; Kalk, W.; Veldhuis, H.A.; van Waas, M.A. Anatomic consideration for preventive implantation. Int. J. Oral Maxillofac. Implant. 1993, 8, 191–196. [Google Scholar]
- Lee, D.-J.; Lee, J.-M.; Kim, E.-J.; Takata, T.; Abiko, Y.; Okano, T.; Green, D.W.; Shimono, M.; Jung, H.-S. Bio-implant as a novel restoration for tooth loss. Sci. Rep. 2017, 7, 7414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kan, J.Y.; Rungcharassaeng, K. Immediate placement and provisionalization of maxillary anterior single implants: A surgical and prosthodontic rationale. Pract. Periodontics Aesthetic. Dent. PPAD 2000, 12, 817–824, quiz 826. [Google Scholar]
- Blanco, J.; Nuñez, V.; Aracil, L.; Muñoz, F.; Ramos, I. Ridge alterations following immediate implant placement in the dog: Flap versus flapless surgery. J. Clin. Periodontol. 2008, 35, 640–648. [Google Scholar] [CrossRef]
- Botticelli, D.; Persson, L.G.; Lindhe, J.; Berglundh, T. Bone tissue formation adjacent to implants placed in fresh extraction sockets: An experimental study in dogs. Clin. Oral Implant. Res. 2006, 17, 351–358. [Google Scholar] [CrossRef]
- Caneva, M.; Botticelli, D.; Morelli, F.; Cesaretti, G.; Beolchini, M.; Lang, N.P. Alveolar process preservation at implants installed immediately into extraction sockets using deproteinized bovine bone mineral—An experimental study in dogs. Clin. Oral Implant. Res. 2012, 23, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Vignoletti, F.; de Sanctis, M.; Berglundh, T.; Abrahamsson, I.; Sanz, M. Early healing of implants placed into fresh extraction sockets: An experimental study in the beagle dog. Iii: Soft tissue findings. J. Clin. Periodontol. 2009, 36, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Vignoletti, F.; Discepoli, N.; Müller, A.; de Sanctis, M.; Muñoz, F.; Sanz, M. Bone modelling at fresh extraction sockets: Immediate implant placement versus spontaneous healing: An experimental study in the beagle dog. J. Clin. Periodontol. 2012, 39, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone grafts and substitutes in dentistry: A review of current trends and developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef]
- Rokaya, D.; Srimaneepong, V.; Wisitrasameewon, W.; Humagain, M.; Thunyakitpisal, P. Peri-implantitis update: Risk indicators, diagnosis, and treatment. Eur. J. Dent. 2020, 14, 672–682. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Ku, J.-K. Extraction socket preservation. J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 435–439. [Google Scholar] [CrossRef]
- Stumbras, A.; Kuliesius, P.; Januzis, G.; Juodzbalys, G. Alveolar ridge preservation after tooth extraction using different bone graft materials and autologous platelet concentrates: A systematic review. J. Oral Maxillofac. Res. 2019, 10, e2. [Google Scholar] [CrossRef]
- Lekovic, V.; Kenney, E.B.; Weinlaender, M.; Han, T.; Klokkevold, P.; Nedic, M.; Orsini, M. A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. J. Periodontol. 1997, 68, 563–570. [Google Scholar] [CrossRef]
- Vance, G.S.; Greenwell, H.; Miller, R.L.; Hill, M.; Johnston, H.; Scheetz, J.P. Comparison of an allograft in an experimental putty carrier and a bovine-derived xenograft used in ridge preservation: A clinical and histologic study in humans. Int. J. Oral Maxillofac. Implant. 2004, 19, 491–497. [Google Scholar]
- Shi, B.; Zhou, Y.; Wang, Y.N.; Cheng, X.R. Alveolar ridge preservation prior to implant placement with surgical-grade calcium sulfate and platelet-rich plasma: A pilot study in a canine model. Int. J. Oral Maxillofac. Implant. 2007, 22, 656–665. [Google Scholar]
- Matarasso, S.; Salvi, G.E.; Iorio Siciliano, V.; Cafiero, C.; Blasi, A.; Lang, N.P. Dimensional ridge alterations following immediate implant placement in molar extraction sites: A six-month prospective cohort study with surgical re-entry. Clin. Oral Implant. Res. 2009, 20, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Loubele, M.; van Assche, N.; Carpentier, K.; Maes, F.; Jacobs, R.; van Steenberghe, D.; Suetens, P. Comparative localized linear accuracy of small-field cone-beam ct and multislice ct for alveolar bone measurements. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 512–518. [Google Scholar] [CrossRef]
- Roe, P.; Kan, J.Y.; Rungcharassaeng, K.; Caruso, J.M.; Zimmerman, G.; Mesquida, J. Horizontal and vertical dimensional changes of peri-implant facial bone following immediate placement and provisionalization of maxillary anterior single implants: A 1-year cone beam computed tomography study. Int. J. Oral Maxillofac. Implant. 2012, 27, 393–400. [Google Scholar]
- Amornvit, P.; Rokaya, D.; Bajracharya, S.; Keawcharoen, K.; Supavanich, W. Management of obstructive sleep apnea with implant retained mandibular advancement device. World J. Dent. 2014, 5, 184–189. [Google Scholar] [CrossRef]
- Amornvit, P.; Rokaya, D.; Keawcharoen, K.; Raucharernporn, S.; Thongpulsawasdi, N. One- vs two stage surgery technique for implant placement in finger prosthesis. J. Clin. Diagn. Res. 2013, 7, 1956–1968. [Google Scholar]
- Lacarbonara, M.; Cazzolla, A.P.; Lacarbonara, V.; Lo Muzio, L.; Ciavarella, D.; Testa, N.F.; Crincoli, V.; Di Venere, D.; de Franco, A.; Tripodi, D.; et al. Prosthetic rehabilitation of maxillary lateral incisors agenesis using dental mini-implants: A multicenter 10-year follow-up. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Selvido, D.I.; Bhattarai, B.P.; Rokaya, D.; Niyomtham, N.; Wongsirichat, N. Pain in oral and maxillofacial surgery and implant dentistry: Types and management. Eur. J. Dent. 2021, 15, 588–598. [Google Scholar] [CrossRef]
- Arora, H.; Ivanovski, S. Immediate and early implant placement in single-tooth gaps in the anterior maxilla: A prospective study on ridge dimensional, clinical, and aesthetic changes. Clin. Oral Implant. Res. 2018, 29, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Barone, A.; Aldini, N.N.; Fini, M.; Giardino, R.; Calvo Guirado, J.L.; Covani, U. Xenograft versus extraction alone for ridge preservation after tooth removal: A clinical and histomorphometric study. J. Periodontol. 2008, 79, 1370–1377. [Google Scholar] [CrossRef]
- Cosyn, J.; Hooghe, N.; de Bruyn, H. A systematic review on the frequency of advanced recession following single immediate implant treatment. J. Clin. Periodontol. 2012, 39, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Job, S.; Bhat, V.; Naidu, E.M. In vivo evaluation of crestal bone heights following implant placement with ‘flapless’ and ‘with-flap’ techniques in sites of immediately loaded implants. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2008, 19, 320–325. [Google Scholar] [CrossRef]
- Wu, D.T.; Munguia-Lopez, J.G.; Cho, Y.W.; Ma, X.; Song, V.; Zhu, Z.; Tran, S.D. Polymeric scaffolds for dental, oral, and craniofacial regenerative medicine. Molecules 2021, 26, 7043. [Google Scholar] [CrossRef] [PubMed]
- Rokaya, D.; Srimaneepong, V.; Sapkota, J.; Qin, J.; Siraleartmukul, K.; Siriwongrungson, V. Polymeric materials and films in dentistry: An overview. J. Adv. Res. 2018, 14, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Spreda, M.; Hauptmann, N.; Lehner, V.; Biehl, C.; Liefeith, K.; Lips, K.S. Porous 3d scaffolds enhance msc vitality and reduce osteoclast activity. Molecules 2021, 26, 6258. [Google Scholar] [CrossRef]
- Ngah, N.A.; Ratnayake, J.; Cooper, P.R.; Dias, G.J.; Tong, D.C.; Mohd Noor, S.N.F.; Hussaini, H.M. Potential of lyophilized platelet concentrates for craniofacial tissue regenerative therapies. Molecules 2021, 26, 517. [Google Scholar] [CrossRef]
- Asa’ad, F.; Pelanyte, G.; Philip, J.; Dahlin, C.; Larsson, L. The role of epigenetic functionalization of implants and biomaterials in osseointegration and bone regeneration—A review. Molecules 2020, 25, 5879. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | Bone Dimension (mm) | Dimensional Change (mm) (T-2) − (T-1) | p Value | |
|---|---|---|---|---|
| T-1 (Mean ± SD) | T-2 (Mean ± SD) | |||
| Vertical bone height: | ||||
| VBH | 1.58 ± 0.48 | 0.89 ± 0.42 | −0.69 ± 0.46 | <0.001 * |
| VOH | 1.47 ± 1.23 | 1.08 ± 1.12 | −0.39 ± 0.30 | 0.001 * |
| Horizontal buccal bone thickness: | ||||
| H(0)-BT | 2.60 ± 1.04 | 2.14 ± 1.00 | −0.46 ± 0.32 | <0.001 * |
| H(1)-BT | 3.04 ± 1.12 | 2.5 ± 1.17 | −0.54 ± 0.47 | 0.001 * |
| H(5)-BT | 3.57 ± 1.38 | 3.27 ± 1.32 | −0.30 ± 0.18 | <0.001 * |
| H(9)-BT | 4.14 ± 1.98 | 3.96 ± 2.07 | −0.18 ± 0.28 | 0.014 * |
| Horizontal oral bone thickness: | ||||
| H(0)-OT | 3.01 ± 1.79 | 2.82 ± 1.83 | −0.20 ± 0.22 | 0.009 * |
| H(1)-OT | 3.15 ± 1.90 | 2.94 ± 1.87 | −0.21 ± 0.16 | 0.001 * |
| H(5)-OT | 4.40 ± 1.78 | 4.28 ± 1.80 | −0.12 ± 0.08 | <0.001 * |
| H(9)-OT | 4.78 ± 1.82 | 4.66 ± 1.82 | −0.12 ± 0.08 | <0.001 * |
| Total horizontal bone thickness: | ||||
| H(0)-BOT | 10.10 ± 1.54 | 9.49 ± 1.59 | −0.62 ± 0.43 | <0.001 * |
| H(1)-BOT | 11.07 ± 1.73 | 10.37 ± 1.73 | −0.70 ± 0.49 | <0.001 * |
| H(5)-BOT | 12.34 ± 1.55 | 12.10 ± 1.66 | −0.24 ± 0.21 | 0.003 * |
| H(9)-BOT | 12.10 ± 1.55 | 11.88 ± 1.54 | −0.22 ± 0.33 | 0.007 * |
| Measurement Level | p Value (T2 − T1) |
|---|---|
| Vertical height | 0.056 |
| Horizontal thickness | |
| H(0) | 0.024 * |
| H(1) | 0.029 * |
| H(5) | <0.001 * |
| H(9) | 0.795 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bungthong, W.; Amornsettachai, P.; Luangchana, P.; Chuenjitkuntaworn, B.; Suphangul, S. Bone Dimensional Change Following Immediate Implant Placement in Posterior Teeth with CBCT: A 6-Month Prospective Clinical Study. Molecules 2022, 27, 608. https://doi.org/10.3390/molecules27030608
Bungthong W, Amornsettachai P, Luangchana P, Chuenjitkuntaworn B, Suphangul S. Bone Dimensional Change Following Immediate Implant Placement in Posterior Teeth with CBCT: A 6-Month Prospective Clinical Study. Molecules. 2022; 27(3):608. https://doi.org/10.3390/molecules27030608
Chicago/Turabian StyleBungthong, Witchayani, Parinya Amornsettachai, Penporn Luangchana, Boontharika Chuenjitkuntaworn, and Suphachai Suphangul. 2022. "Bone Dimensional Change Following Immediate Implant Placement in Posterior Teeth with CBCT: A 6-Month Prospective Clinical Study" Molecules 27, no. 3: 608. https://doi.org/10.3390/molecules27030608