
Advances in Management of Bladder Cancer—The Role of Photodynamic Therapy

 ,
,  ,
, 

Abstract
:1. Introduction
2. Photodynamic Therapy (PDT) in General
3. Photodynamic Therapy in Bladder Cancer
3.1. Using Different Synthetic Photosensitizers
3.1.1. 5-Aminolevulinic Acid (ALA or Levlan)
3.1.2. Hexaminolevulinic Acid (HAL)
3.2. Herbal Photosensitizers
3.2.1. Hypericin
3.2.2. Chlorophyllin
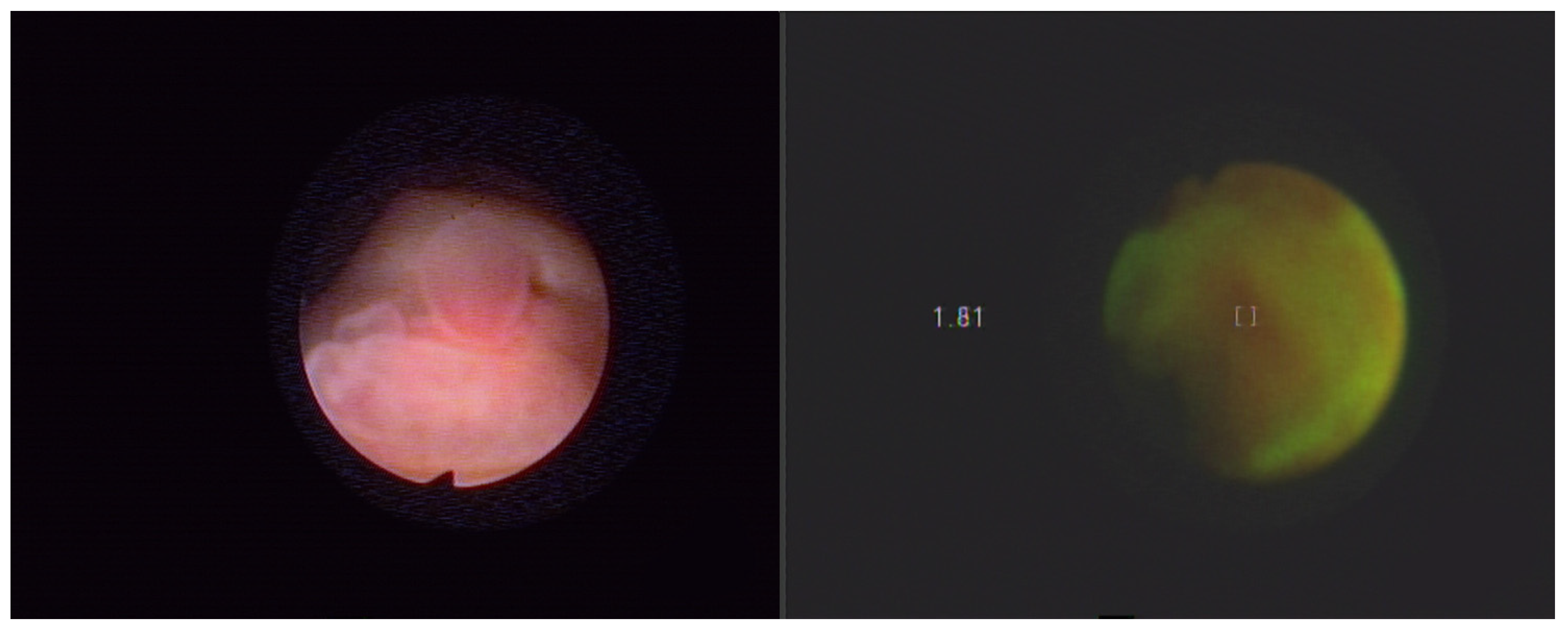
4. Autofluorescence Cystoscopy
- ALA [(1.5 g or 180 mM) in 50 mL of sodium carbonate buffer solution], which must be instilled and retained in the bladder for 2–3 h prior to cystoscopy,
- HAL [(8 mM) in 50 mL of phosphate buffer solution], instilled and retained in the bladder for 1 h before [73].
5. Light Sources in Applications for PDD and PDT of Bladder Cancer
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farling, K.B. Bladder cancer: Risk factors, diagnosis, and management. Nurse Pract. 2017, 42, 26–33. [Google Scholar] [CrossRef]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Botteman, M.F.; Pashos, C.L.; Redaelli, A.; Laskin, B.; Hauser, R. The health economics of bladder cancer: A comprehensive review of the published literature. Pharmacoeconomics 2003, 21, 1315–1330. [Google Scholar] [CrossRef] [PubMed]
- Bochenek, K.; Aebisher, A.; Międzybrodzka, A.; Cieślar, G.; Kawczyk-Krupka, A. Methods for bladder cancer diagnosis—The role of autofluorescence and photodynamic diagnosis. Photodiagnosis Photodyn. Ther. 2019, 27, 141–148. [Google Scholar] [CrossRef]
- Supit, W.; Mochtar, C.A.; Santoso, R.B.; Umbas, R. Outcomes of radical cystectomy and bladder preservation treatment for muscle-invasive urothelial carcinoma of the bladder. Asian J. Surg. 2014, 37, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Knowles, M.A.; Hurst, C.D. Molecular biology of bladder cancer: New insights into pathogenesis and clinical diversity. Nat. Rev. Cancer 2015, 15, 25–41. [Google Scholar] [CrossRef]
- Lee, Y.H.; Lin, Y.C. Anti-EGFR Indocyanine Green-Mitomycin C-Loaded Perfluorocarbon Double Nanoemulsion: A Novel Nanostructure for Targeted Photochemotherapy of Bladder Cancer Cells. Nanomaterials 2018, 8, 283. [Google Scholar] [CrossRef] [Green Version]
- Kirkali, Z.; Chan, T.; Manoharna, M.; Algaba, T.; Busch, C.; Cheng, L.; Kiemeney, L.; Kriegmair, M.; Montironi, R.; Murphy, W.M.; et al. Bladder cancer: Epidemiology, staging and grading, and diagnosis. Urology 2005, 66 (Suppl. 1), 4–34. [Google Scholar] [CrossRef]
- Lipiński, M. Fluorescence diagnosis of bladder neoplasms. Przegląd Urologiczny 2013, 2, 78. [Google Scholar]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 2017, 198, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Svedsen, C.; James, A.; Matulewicz, R.S.; Moreton, E.; Sosnowski, R.; Sherman, S.; Jaspers, I.; Gordon, T.; Bjurlin, M.A. Carcinogenic biomarkers of exposure in the urine of heated tobacco product users associated with bladder cancer: A systematic review. Urol. Oncol. 2021, 1–12. [Google Scholar]
- Lam, T.; Nabi, G. Potential of urinary biomarkers in early bladder cancer diagnosis. Expert Rev. Anticancer Ther. 2007, 7, 1105–1115. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Stenzl, A.; Sharma, A.; Vasdev, N. Urinary biomarkers in bladder cancer: A review of the current landscape and future directions. Urol. Oncol. 2021, 39, 41–51. [Google Scholar] [CrossRef]
- Chueng, G.; Sahai, A.; Billia, M.; Dasgupta, P.; Khan, M.S. Recent advances in the diagnosis and treatment of bladder cancer. BMC Med. 2013, 11, 13. [Google Scholar] [CrossRef] [Green Version]
- Peng, M.; Xiao, D.; Bu, Y.; Long, J.; Yang, X.; Lv, S.; Yang, X. Novel Combination Therapies for the Treatment of Bladder Cancer. Front. Oncol. 2021, 27, 539527. [Google Scholar] [CrossRef]
- Fukuhara, H.; Yamamoto, S.; Karashima, T.; Inoue, K. Photodynamic diagnosis and therapy for urothelial carcinoma and prostate cancer: New imaging technology and therapy. Int. J. Clin. Oncol. 2021, 26, 18–25. [Google Scholar] [CrossRef]
- Prout, G.R., Jr.; Lin, C.W.; Benson, R., Jr.; Nseyo, U.O.; Daly, J.J.; Griffin, P.P.; Kinsey, J.; Tian, M.E.; Lao, Y.H.; Mian, Y.Z.; et al. Photodynamic therapy with hematoporphyrin derivative in the treatment of superficial transitional-cell carcinoma of the bladder. N. Engl. J. Med. 1987, 12, 1251–1255. [Google Scholar] [CrossRef]
- Zhao, X.; Liu, J.; Fan, J.; Chao, H.; Peng, X. Recent progress in photosensitizers for overcoming the challenges of photodynamic therapy: From molecular design to application. Chem. Soc. Rev. 2021, 50, 4185–4219. [Google Scholar] [CrossRef]
- Algorri, J.F.; Ochoa, M.; Roldán-Varona, P.; Rodríguez-Cobo, L.; López-Higuera, J.M. Photodynamic Therapy: A Compendium of Latest Reviews. Cancers 2021, 13, 4447. [Google Scholar] [CrossRef]
- Baptista, M.S.; Cadet, J.; di Mascio, P.; Ghogare, A.A.; Greer, A.; Hamblin, M.R.; Lorente, C.; Nunez, S.C.; Ribeiro, M.S.; Thomas, A.H.; et al. Type I and Type II Photosensitized Oxidation Reactions: Guidelines and Mechanistic Pathways. Photochem. Photobiol. 2017, 93, 912–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, C.A.; Evans, D.H.; Abrahamse, H. Photodynamic therapy (PDT): A short review on cellular mechanisms and cancer research applications for PDT. J. Photochem. Photobiol. B 2009, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kędzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy—Mechanisms, photosensitizers and combinations. Biomed. Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Dima, V.F.; Ionescu, M.D.; Balotescu, C.; Dima, S.F. Photodynamic therapy and some clinical applications in oncology. Roum. Arch. Microbiol. Immunol. 2002, 61, 159–205. [Google Scholar]
- Vrouenraets, M.B.; Visser, G.W.; Snow, G.B.; van Dongen, G.A. Basic principles, applications in oncology and improved selectivity of photodynamic therapy. Anticancer Res. 2003, 23, 505–522. [Google Scholar]
- Brown, M.S.; Goldstein, J.L. A receptor-mediated pathway for cholesterol homeostasis. Science 1986, 232, 34–47. [Google Scholar] [CrossRef] [Green Version]
- Tatidis, L.; Masquelier, M.; Vitols, S. Elevated uptake of low density lipoprotein by drug resistant human leukemic cell lines. Biochem. Pharmacol. 2002, 63, 2169–2180. [Google Scholar] [CrossRef]
- Llaverias, G.; Danilo, C.; Mercier, I.; Daumer, K.; Capozza, F.; Williams, T.M.; Sotgia, F.; Lisanti, M.P.; Frank, P.G. Role of cholesterol in the development and progression of breast cancer. Am. J. Pathol. 2011, 178, 402–412. [Google Scholar] [CrossRef]
- Gorin, A.; Gabitova, L.; Astsaturov, I. Regulation of cholesterol biosynthesis and cancer signaling. Curr. Opin. Pharmacol. 2012, 12, 710–716. [Google Scholar] [CrossRef] [Green Version]
- Cruz, P.M.R.; Mo, H.; McConathy, W.J.; Sabnis, N.; Lacko, A.G. The role of cholesterol metabolism and cholesterol transport in carcinogenesis: A review of scientific findings, relevant to future cancer therapeutics. Front. Pharmacol. 2013, 4, 119. [Google Scholar] [CrossRef] [Green Version]
- Hamblin, M.R.; Newman, E.L. Photosensitizer targeting in photodynamic therapy. II. Conjugates of haematoporphyrin with serum lipoproteins. J. Photochem. Photobiol. B 1994, 26, 147–157. [Google Scholar] [CrossRef]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in photodynamic therapy: Part three—Photosensitizer pharmacokinetics, biodistribution, tumor localization and modes of tumor destruction. Photodiagnosis Photodyn. Ther. 2005, 2, 91–106. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Xu, H.; Meyers, A.D.; Musani, A.I.; Wang, L.; Tagg, R.; Barqawi, A.B.; Chen, Y.K. Photodynamic therapy for treatment of solid tumors—Potential and technical challenges. Technol. Cancer Res. Treat. 2008, 7, 309–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krammer, B. Vascular effects of photodynamic therapy. Anticancer Res. 2001, 21, 4271–4277. [Google Scholar]
- Dobson, J.; de Queiroz, G.F.; Golding, J.P. Photodynamic therapy and diagnosis: Principles and comparative aspects. Vet. J. 2018, 233, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Bozzini, G.; Colin, P.; Betrouni, N.; Nevoux, P.; Ouzzane, A.; Puech, P.; Villers, A.; Mordon, S. Photodynamic therapy in urology: What can we do now and where are we heading? Photodiagnosis Photodyn. Ther. 2012, 9, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Monro, S.; Colón, K.L.; Yin, H.; Roque, J., 3rd; Konda, P.; Gujar, S.; Thummel, R.P.; Lilge, L.; Cameron, C.G.; McFarland, S.A. Transition Metal Complexes and Photodynamic Therapy from a Tumor-Centered Approach: Challenges, Opportunities, and Highlights from the Development of TLD1433. Chem. Rev. 2019, 119, 797–828. [Google Scholar] [CrossRef]
- Filip, A.G.; Clichici, S.; Daicoviciu, D.; Olteanu, D.; Mureşan, A.; Dreve, S. Photodynamic therapy—Indications and limits in malignant tumors treatment. Rom. J. Intern. Med. 2008, 46, 285–293. [Google Scholar]
- Nseyo, U.O.; Lamm, D.L. Immunotherapy of bladder cancer. Semin. Surg. Oncol. 1997, 13, 342–349. [Google Scholar] [CrossRef]
- Simelane, N.W.N.; Kruger, C.A.; Abrahamse, H. Photodynamic diagnosis and photodynamic therapy of colorectal cancer in vitro and in vivo. RSC Adv. 2020, 10, 41560–41576. [Google Scholar] [CrossRef]
- Yavari, N.; Andersson-Engels, S.; Segersten, U.; Malmstrom, P.U. An overview on preclinical and clinical experiences with photodynamic therapy for bladder cancer. Can. J. Urol. 2011, 18, 5778–5786. [Google Scholar] [PubMed]
- Aboumarzouk, O.; Valentine, R.; Buist, R.; Ahmad, S.; Nabi, G.; Eljamel, S.; Moseley, H.; Kata, S.G. Laser-induced autofluorescence spectroscopy: Can it be of importance in detection of bladder lesions? Photodiagnosis Photodyn. Ther. 2015, 12, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Schenkman, E.; Lamm, D.L. Superficial bladder cancer therapy. Sci. World J. 2004, 28, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Adamek, M.; Kawczyk-Krupka, A.; Mostowy, A.; Czuba, Z.; Krol, W.; Kasperczyk, S.; Jakobisiak, M.; Golab, J.; Sieroń, A. Topical ALA—PDT modifies neutrophils’ chemiluminescence, lymphocytes’ interleukin-1beta secretion and serum level of transforming growth factor beta1 in patients with nonmelanoma skin malignancies—A clinical study. Photodiagnosis Photodyn. Ther. 2005, 2, 65–72. [Google Scholar] [CrossRef]
- Kawczyk-Krupka, A.; Ledwon, A.; Malyszek, J.; Sieron, A. Balanoposthitis with epithelial dysplasia treated by photodynamic therapy. Photodiagnosis Photodyn. Ther. 2007, 4, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Sieroń, A.; Sieroń-Stołtny, K.; Kawczyk-Krupka, A.; Latos, W.; Kwiatek, S.; Straszak, D.; Bugaj, A.M. The role of fluorescence diagnosis in clinical practice. OncoTargets Ther. 2013, 6, 977–982. [Google Scholar]
- Kawczyk-Krupka, A.; Waśkowska, J.; Raczkowska-Siostrzonek, A.; Kościarz-Grzesiok, A.; Kwiatek, S.; Straszak, D.; Latos, W.; Koszowski, R.; Sieroń, A. Comparison of cryotherapy and photodynamic therapy in treatment of oral leukoplakia. Potodiagnosis Photodyn. Ther. 2012, 9, 148–155. [Google Scholar] [CrossRef]
- Bachor, R.; Shea, C.R.; Gillies, R.; Hasan, T. Photosensitized destruction of human bladder carcinoma cells treated with chlorin e6-conjugated microspheres. Proc. Natl. Acad. Sci. USA 1991, 88, 1580–1584. [Google Scholar] [CrossRef] [Green Version]
- Bachor, R.; Reich, E.; Rück, A.; Hautmann, R. Aminolevulinic acid for photodynamic therapy of bladder carcinoma cells. Urol. Res. 1996, 24, 285–289. [Google Scholar] [CrossRef]
- Waidelich, R.; Beyer, W.; Knüchel, R.; Stepp, H.; Baumgartner, R.; Schröder, J.; Hofstetter, A.; Kriegmair, M. Whole bladder photodynamic therapy with 5-aminolevulinic acid using a white light source. Urology 2003, 61, 332–337. [Google Scholar] [CrossRef]
- Filonenko, E.V.; Kaprin, A.D.; Alekseev, B.Y.; Apolikhin, O.I.; Slovokhodov, E.K.; Ivanova-Radkevich, V.I.; Urlova, A.N. 5-Aminolevulinic acid in intraoperative photodynamic therapy of bladder cancer (results of multicenter trial). Photodiagnosis Photodyn. Ther. 2016, 16, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K. 5-Aminolevulinic acid-mediated photodynamic therapy for bladder cancer. Int. J. Urol. 2017, 24, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witjes, J.A.; Douglass, J. The role of hexaminolevulinate fluorescence cystoscopy in bladder cancer. Nat. Clin. Pract. Urol. 2007, 4, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Vaucher, L.; Jichlinski, P.; Lange, N.; Ritter-Schenk, C.; van den Bergh, H.; Kucera, P. Hexyl-aminolevulinate-mediated photodynamic therapy: How to spare normal urothelium. An in vitro approach. Lasers Surg. Med. 2007, 39, 67–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bader, M.J.; Stepp, H.; Beyer, W.; Pongratz, T.; Sroka, R.; Kriegmair, M.; Zaak, D.; Welschof, M.; Tilki, D.; Stief, C.G.; et al. Photodynamic therapy of bladder cancer—A phase I study using hexaminolevulinate (HAL). Urol. Oncol. 2013, 31, 1178–1183. [Google Scholar] [CrossRef]
- Kamuhabwa, A.R.; Agostinis, P.; D’Hallewin, M.A.; Kasran, A.; de Witte, P.A. Photodynamic activity of hypericin in human urinary bladder carcinoma cells. Anticancer Res. 2000, 20, 2579–2584. [Google Scholar]
- Saw, C.L.; Olivo, M.; Soo, K.C.; Heng, P.W. Delivery of hypericin for photodynamic applications. Cancer Lett. 2006, 8, 23–30. [Google Scholar] [CrossRef]
- Mühleisen, L.; Alev, M.; Unterweger, H.; Subatzus, D.; Pöttler, M.; Friedrich, R.P.; Alexiou, C.; Janko, C. Analysis of Hypericin-Mediated Effects and Implications for Targeted Photodynamic Therapy. Int. J. Mol. Sci. 2017, 18, 1388. [Google Scholar] [CrossRef] [Green Version]
- Du, L.; Jiang, N.; Wang, G.; Chu, Y.; Lin, W.; Qian, J.; Zhang, Y.; Zheng, J.; Chen, G. Autophagy inhibition sensitizes bladder cancer cells to the photodynamic effects of the novel photosensitizer chlorophyllin e4. J. Photochem. Photobiol. B 2014, 5, 1–10. [Google Scholar] [CrossRef]
- Li, B.; Wu, Z.; Li, W.; Jia, G.; Lu, J.; Fang, J.; Chen, G. Chlorophyllin e4 is a novel photosensitizer against human bladder cancer cells. Oncol. Rep. 2012, 27, 1455–1460. [Google Scholar]
- Gomaa, I.; Ali, S.E.; El-Tayeb, T.A.; Abdel-Kader, M.H. Chlorophyll derivative mediated PDT versus methotrexate: An in vitro study using MCF-7 cells. Photodiagnosis Photodyn. Ther. 2012, 9, 362–368. [Google Scholar] [CrossRef]
- Berger, A.P.; Steiner, H.; Stenzl, A.; Akkad, T.; Bartsch, G.; Holtl, L. Photodynamic therapy with intravesical instillation of 5-aminolevulinic acid for patients with recurrent superficial bladder cancer: A single-center study. Urology 2003, 61, 338–341. [Google Scholar] [CrossRef]
- Dhaneshar, S.; Patil, K.; Bulbule, M.; Kinjawadekar, V.; Joshi, D.; Joshi, V. Photodynamic therapy for cancer. Int. J. Pharm. Sci. Rev. Res. 2014, 27, 125–141. [Google Scholar]
- Szliszka, E.; Kawczyk-Krupka, A.; Czuba, Z.P.; Sieron, A.; Krol, W. Effect of ALA-mediated photodynamic therapy in combination with tumor necrosis factor-related apoptosis-inducing ligand (TRA IL) on bladder cancer cells. Cent. Eur. J. Urol. 2011, 64, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Szygula, M.; Wojciechowski, B.; Adamek, M.; Pietrusa, A.; Kawczyk-Krupka, A.; Cebula, W.; Zieleznik, W.; Biniszkiewicz, T.; Duda, W.; Sieroń, A. Fluorescent diagnosis of urinary bladder cancer-a comparison of two diagnostic modalities. Photodiagnosis Photodyn. Ther. 2004, 1, 23–26. [Google Scholar] [CrossRef]
- Kawczyk-Krupka, A.; Bugaj, A.M.; Latos, W.; Wawrzyniec, K.; Oleś, P.; Mertas, A.; Czuba, Z.; Król, W.; Sieroń-Stołtny, K.; Sieroń, A. ALA-mediated photodynamic effect onapoptosis induction and secretion of macrophage migration inhibitory factor(MIF) and of monocyte chemotactic protein(MCP-1) by colon cancer cells in normoxia and in hypoxia-like conditions in vitro. Photodiagnosis Photodyn. Ther. 2015, 12, 27–35. [Google Scholar] [CrossRef]
- Nakatani, S.; Ida, M.; Wang, X.; Naito, Y.; Kawaguchi, M. Oral 5-aminolevulinic acid administration prior to transurethral resection of bladder tumor causes intraoperative hypotension: Propensity score analysis. Photodiagnosis Photodyn. Ther. 2021, 34, 102342. [Google Scholar] [CrossRef]
- Rytlewski, J.D.; Scalora, N.; Garcia, K.; Tanas, M.; Toor, F.; Miller, B.; Allen, B.; Milhem, M.; Monga, V. Photodynamic Therapy Using Hippo Pathway Inhibitor Verteporfin: A Potential Dual Mechanistic Approach in Treatment of Soft Tissue Sarcomas. Cancers 2021, 13, 675. [Google Scholar] [CrossRef]
- Kiesslich, T.; Berlanda, J.; Plaetzer, K.; Krammer, B.; Berr, F. Comparative characterization of the efficiency and cellular pharmacokinetics of Foscan- and Foslip-based photodynamic treatment in human biliary tract cancer cell lines. Photochem. Photobiol. Sci. 2007, 6, 619–627. [Google Scholar] [CrossRef]
- Josefsen, L.B.; Boyle, R.W. Photodynamic Therapy and the Development of Metal-Based Photosensitisers. Metal Based Drugs 2008, 2008, 276109. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.Y.; Diaz, R.R.; Cho, K.S.; Lim, M.S.; Chung, J.S.; Kim, W.T.; Ham, W.S.; Choi, Y.D. Efficacy and safety of photodynamic therapy for recurrent, high grade nonmuscle invasive bladder cancer refractory or intolerant to bacille Calmette-Guérin immunotherapy. J. Urol. 2013, 190, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Gándara, L.; Sandes, E.; di Venosa, G.; Prack Mc Cormick, B.; Rodriguez, L.; Mamone, L.; Batlle, A.; Eiján, A.M.; Casas, A. The natural flavonoid silybin improves the response to Photodynamic Therapy of bladder cancer cells. J. Photochem. Photobiol. B 2014, 133, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Kriegmair, M.; Baumgartner, R.; Knüchel, R.; Stepp, H.; Hofstädter, F.; Hofstetter, A. Detection of early bladder cancer by 5-aminolevulinic acid induced porphyrin fluorescence. J. Urol. 1996, 155, 105–109. [Google Scholar] [CrossRef]
- Waidelich, R.; Stepp, H.; Baumgartner, R.; Weninger, E.; Hofstetter, A.; Kriegmair, M. Clinical experience with 5-aminolevulinic acid and photodynamic therapy for refractory superficial bladder cancer. J. Urol. 2001, 165, 1904–1907. [Google Scholar] [CrossRef]
- Drăgoescu, O.; Tomescu, P.; Pănuş, A.; Enache, M.; Maria, C.; Stoica, L.; Pleşea, I.E. Photodynamic diagnosis of non-muscle invasive bladder cancer using hexaminolevulinic acid. Rom. J. Morphol. Embryol. 2011, 52, 123–127. [Google Scholar]
- Burgués, J.P.; Conde, G.; Oliva, J.; Abascal, J.M.; Iborra, I.; Puertas, M.; Ordoño, F.; Grupo BLUE (Blue Light Urologic Endoscopy). Diagnóstico fotodinámico con hexaminolevulinato en el cáncer vesical no músculo invasivo: Experiencia del grupo BLUE [Hexaminolevulinate photodynamic diagnosis in non-muscle invasive bladder cancer: Experience of the BLUE group]. Actas Urol. Esp. 2011, 35, 439–445. [Google Scholar] [CrossRef]
- Jichlinski, P.; Leisinger, H.J. Fluorescence cystoscopy in the management of bladder cancer: A help for the urologist! Urol. Int. 2005, 74, 97–101. [Google Scholar] [CrossRef]
- Colapaoli, L.; Thorsen, J.; Nopp, A.; Guttormsen, A.B. A case of anaphylactic shock possibly caused by intravesical Hexvix. Acta Anaesthesiol. Scand. 2006, 50, 1165–1167. [Google Scholar] [CrossRef]
- Sternberg, E.D.; Dolphin, D. Second Generation Photodynamic Agents: A Review. J. Clin. Laser Med. Surg. 1993, 11, 233–241. [Google Scholar] [CrossRef]
- Kataoka, H.; Nishie, H.; Hayashi, N.; Tanaka, M.; Nomoto, A.; Yano, S.; Joh, T. New Photodynamic Therapy with next-Generation Photosensitizers. Ann. Transl. Med. 2017, 5, 183. [Google Scholar] [CrossRef] [Green Version]
- Ormond, A.B.; Freeman, H.S. Dye Sensitizers for Photodynamic Therapy. Materials 2013, 6, 817–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frankenberg-Dinkel, N. Bacterial heme oxygenases. Antioxid. Redox Sign. 2004, 6, 825–834. [Google Scholar] [CrossRef]
- Guzman, L.-M.; Belin, D.; Carson, M.J.; Beckwith, J. Tight regulation, modulation, and high-level expression by vectors containing the arabinose pBAD promoter. J. Bacteriol. 1995, 177, 4121–4130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.Z.; Nikaido, H. Efflux-mediated drug resistance in bacteria. Drugs 2004, 64, 159–204. [Google Scholar] [CrossRef]
- Hamblin, M.R.; Viveiros, J.; Yang, C.; Ahmadi, A.; Ganz, R.A.; Tolkoff, M.J. Helicobacter pylori accumulates photoactive porphyrins and is killed by visible light. Antimicrob. Agents Chemother. 2005, 49, 2822–2827. [Google Scholar] [CrossRef] [Green Version]
- Schempp, C.M.; Winghofer, B.; Langheinrich, M.; Schöpf, E.; Simon, J.C. Hypericin levels in human serum and interstitial skin blister fluid after oral single-dose and steady-state administration of Hypericum perforatum extract (St. John’s wort). Skin Pharmacol. Appl. Skin Physiol. 1999, 12, 299–304. [Google Scholar] [CrossRef]
- Vantieghem, A.; Xu, Y.; Declercq, W.; Vandenabeele, P.; Denecker, G.; Vandenheede, J.R.; Merlevede, W.; de Witte, P.A.; Agostinis, P. Different pathways mediate cytochrome c release after photodynamic therapy with hypericin. Photochem. Photobiol. 2001, 74, 133–142. [Google Scholar] [CrossRef]
- Vantieghem, A.; Assefa, Z.; Vandenabeele, P.; Declercq, W.; Courtois, S.; Vandenheede, J.R.; Merlevede, W.; de Witte, P.; Agostinis, P. Hypericin-induced photosensitization of HeLa cells leads to apoptosis or necrosis. Involvement of cytochrome c and procaspase-3 activation in the mechanism of apoptosis. FEBS Lett. 1998, 27, 19–24. [Google Scholar] [CrossRef]
- Weller, M.; Trepel, M.; Grimmel, C.; Schabet, M.; Bremen, D.; Krajewski, S.; Reed, J.C. Hypericin-induced apoptosis of human malignant glioma cells is light-dependent, independent of bcl-2 expression, and does not require wild-type p53. Neurol. Res. 1997, 19, 459–470. [Google Scholar] [CrossRef]
- Zupkó, I.; Kamuhabwa, A.R.; D’Hallewin, M.A.; Baert, L.; de Witte, P.A. In vivo photodynamic activity of hypericin in transitional cell carcinoma bladder tumors. Int. J. Oncol. 2001, 18, 1099–1105. [Google Scholar] [CrossRef]
- Couldwell, W.T.; Hinton, D.R.; He, S.; Chen, T.C.; Sebat, I.; Weiss, M.H.; Law, R.E. Protein kinase C inhibitors induce apoptosis in human malignant glioma cell lines. FEBS Lett. 1994, 23, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Krammer, B.; Verwanger, T. Molecular response to hypericin-induced photodamage. Curr. Med. Chem. 2012, 19, 793–798. [Google Scholar] [CrossRef]
- Davids, L.M.; Kleemann, B.; Cooper, S.; Kidson, S.H. Melanomas display increased cytoprotection to hypericin-mediated cytotoxicity through the induction of autophagy. Cell Biol. Int. 2009, 33, 1065–1072. [Google Scholar] [CrossRef]
- Agostinis, P.; Vantieghem, A.; Merlevede, W.; de Witte, P.A. Hypericin in cancer treatment: More light on the way. Int. J. Biochem. Cell Biol. 2002, 34, 221–241. [Google Scholar] [CrossRef]
- Sim, H.G.; Lau, W.K.; Olivo, M.; Tan, P.H.; Cheng, C.W. Is photodynamic diagnosis using hypericin better than white-light cystoscopy for detecting superficial bladder carcinoma? BJU Int. 2005, 95, 1215–1218. [Google Scholar] [CrossRef] [PubMed]
- Kubin, A.; Meissner, P.; Wierrani, F.; Burner, U.; Bodenteich, A.; Pytel, A.; Schmeller, N. Fluorescence diagnosis of bladder cancer with new water soluble hypericin bound to polyvinylpyrrolidone: PVP-hypericin. Photochem. Photobiol. 2008, 84, 1560–1563. [Google Scholar] [CrossRef]
- Stavropoulos, N.E.; Kim, A.; Nseyo, U.U.; Tsimaris, I.; Chung, T.D.; Miller, T.A.; Redlak, M.; Nseyo, U.O.; Skalkos, D. Hypericum perforatum L. extract—Novel photosensitizer against human bladder cancer cells. J. Photochem. Photobiol. B 2006, 84, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Bhuvaneswari, R.; Gan, Y.Y.; Soo, K.C.; Olivo, M. Targeting EGFR with photodynamic therapy in combination with Erbitux enhances in vivo bladder tumor response. Mol. Cancer 2009, 8, 94. [Google Scholar] [CrossRef] [Green Version]
- Lihuan, D.; Jingcun, Z.; Ning, J.; Guozeng, W.; Yiwei, C.; Wei, L.; Jing, Q.; Yuanfang, Z.; Gang, C. Photodynamic therapy with the novel photosensitizer chlorophyllin f induces apoptosis and autophagy in human bladder cancer cells. Lasers Surg. Med. 2014, 46, 319–334. [Google Scholar] [CrossRef]
- Zhuo, Z.; Song, Z.; Ma, Z.; Zhang, Y.; Xu, G.; Chen, G. Chlorophyllin e6-mediated photodynamic therapy inhibits proliferation and induces apoptosis in human bladder cancer cells. Oncol. Rep. 2019, 41, 2181–2193. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.M.; Darafsheh, A. Light sources and dosimetry techniques for photodynamic therapy. Photochem. Photobiol. 2020, 96, 280–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beigzadeh, A.M.; Rashidian Vaziri, M.R.; Ziaie, F.; Sharif, S. A new optical method for online monitoring of the light dose and dose profile in Photodynamic Therapy. Lasers Surg. Med. 2020, 52, 659–670. [Google Scholar] [CrossRef]
- Kamuhabwa, A.; Agostinis, P.; Ahmed, B.; Landuyt, W.; van Cleynenbreugel, B.; van Poppel, H.; de Witte, P. Hypericin as a potential phototherapeutic agent in superficial transitional cell carcinoma of the bladder. Photochem. Photobiol. Sci. 2004, 3, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Kamuhabwa, A.A.; Roskams, T.; D’Hallewin, M.A.; Baert, L.; van Poppel, H.; de Witte, P.A. Whole bladder wall photodynamic therapy of transitional cell carcinoma rat bladder tumors using intravesically administered hypericin. Int. J. Cancer 2003, 107, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Kamuhabwa, A.A.; Cosserat-Gerardin, I.; Didelon, J.; Notter, D.; Guillemin, F.; Roskams, T.; D’Hallewin, M.A.; Baert, L.; de Witte, P.A. Biodistribution of hypericin in orthotopic transitional cell carcinoma bladder tumors: Implication for whole bladder wall photodynamic therapy. Int. J. Cancer 2002, 97, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Van Staveren, H.J.; Keijzer, M.; Keesmaat, T.; Jansen, H.; Kirkel, W.J.; Beek, J.F.; Star, W.M. Integrating sphere effect in whole-bladder wall photodynamic therapy: III. Fluence multiplication, optical penetration and light distribution with an eccentric source for human bladder optical properties. Phys. Med. Biol. 1996, 41, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Stewart, F.A.; Oussoren, Y.; te Poele, J.A.; Horenblas, S.; Mooi, W.J. Functional and histological damage in the mouse bladder after photodynamic therapy. Br. J. Cancer 1992, 65, 884–890. [Google Scholar] [CrossRef] [Green Version]
- Marynissen, J.P.; Jansen, H.; Star, W.M. Treatment system for whole bladder wall photodynamic therapy with in vivo monitoring and control of light dose rate and dose. J. Urol. 1989, 142, 1351–1355. [Google Scholar] [CrossRef]
- Misaki, T.; Hisazumi, H.; Hirata, A.; Kunimi, K.; Yamamoto, H.; Amano, T.; Kumaki, O.; Koshida, K.; Nishino, A.; Nakazima, K. Photodynamic therapy of superficial bladder tumors. Hinyokika Kiyo 1986, 32, 1941–1948. [Google Scholar]
- Hisazumi, H.; Naito, K.; Uchibayashi, T.; Hirata, A.; Komatsu, K. Integral photodynamic therapy of superficial bladder tumors with special reference to carcinoma in situ. Scand. J. Urol. Nephrol. Suppl. 1991, 138, 161–165. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubrak, T.; Karakuła, M.; Czop, M.; Kawczyk-Krupka, A.; Aebisher, D. Advances in Management of Bladder Cancer—The Role of Photodynamic Therapy. Molecules 2022, 27, 731. https://doi.org/10.3390/molecules27030731
Kubrak T, Karakuła M, Czop M, Kawczyk-Krupka A, Aebisher D. Advances in Management of Bladder Cancer—The Role of Photodynamic Therapy. Molecules. 2022; 27(3):731. https://doi.org/10.3390/molecules27030731
Chicago/Turabian StyleKubrak, Tomasz, Michał Karakuła, Marcin Czop, Aleksandra Kawczyk-Krupka, and David Aebisher. 2022. "Advances in Management of Bladder Cancer—The Role of Photodynamic Therapy" Molecules 27, no. 3: 731. https://doi.org/10.3390/molecules27030731