

Quantitative Profiling of Serum Carnitines Facilitates the Etiology Diagnosis and Prognosis Prediction in Heart Failure

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinical Baseline Characteristics of Enrolled Patients in This Study
2.2. Levels of Serum Carnitines and Other Traditional Biomarkers at Baseline
2.3. Multivariate Logistic Analysis of the Impact of Carnitines on HF Diagnosis
2.4. Baseline Carnitines Discriminated DCM-HF from IHD-HF
2.5. Carnitines Added to Clinical Factors for DCM-HF Discrimination
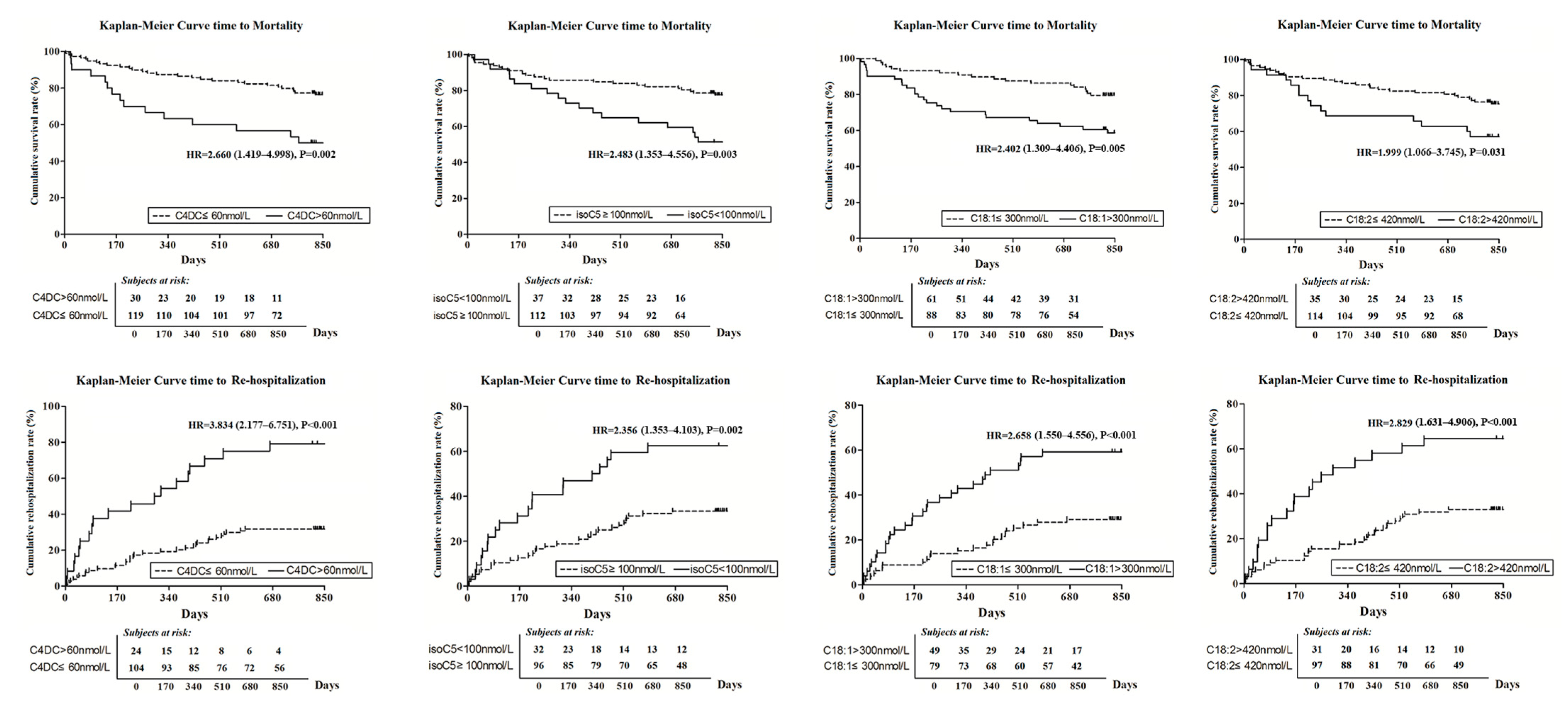
2.6. Baseline Carnitines and Primary Clinical Outcomes
2.6.1. All-Cause Mortality
2.6.2. HF Rehospitalization Rate
3. Methods
3.1. Patient Enrollment and Ethical Approval
3.2. Clinical Detection and Information Collection
3.2.1. Laboratory Measurements
3.2.2. Echocardiography and Electrocardiograph
3.2.3. Coronary Angiography
3.2.4. Etiology Diagnosis of HF and Treatment Strategy
3.3. Quantitative Measurements of Serum Carnitines
3.3.1. Reagents
3.3.2. Sample Preparation
3.3.3. Calibration Curves
3.3.4. Liquid Chromatography and Mass Spectrometry
3.3.5. Data Preprocessing
3.3.6. Quantitation of Carnitines without Commercial Standards
3.4. Follow-Up and Primary Outcomes
3.5. Statistical Analysis
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed] [Green Version]
- Vitale, C.; Wajngaten, M.; Sposato, B.; Gebara, O.; Rossini, P.; Fini, M.; Volterrani, M.; Rosano, G.M. Trimetazidine improves left ventricular function and quality of life in elderly patients with coronary artery disease. Eur. Heart J. 2004, 25, 1814–1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coats, C.J.; Pavlou, M.; Watkinson, O.T.; Protonotarios, A.; Moss, L.; Hyland, R.; Rantell, K.; Pantazis, A.A.; Tome, M.; McKenna, W.J.; et al. Effect of trimetazidine dihydrochloride therapy on exercise capacity in patients with nonobstructive hypertrophic cardiomyopathy: A randomized clinical trial. JAMA Cardiol. 2019, 4, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Dinicolantonio, J.J.; Lavie, C.J.; Fares, H.; Menezes, A.R.; O’Keefe, J.H. L-carnitine in the secondary prevention of cardiovascular disease: Systematic review and meta-analysis. Mayo Clin. Proc. 2013, 88, 544–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neubauer, S. The failing heart—An engine out of fuel. N. Engl. J. Med. 2007, 356, 1140–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, L.; Leone, T.C.; Keller, M.P.; Martin, O.J.; Broman, A.T.; Nigro, J.; Kapoor, K.; Koves, T.R.; Stevens, R.; Ilkayeva, O.R.; et al. Energy metabolic reprogramming in the hypertrophied and early stage failing heart: A multisystems approach. Circ. Heart Fail. 2014, 7, 1022–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, M.L.; Wang, C.H.; Shiao, M.S.; Liu, M.H.; Huang, Y.Y.; Huang, C.Y.; Mao, C.T.; Lin, J.F.; Ho, H.Y.; Yang, N.I. Metabolic disturbances identified in plasma are associated with outcomes in patients with heart failure: Diagnostic and prognostic value of metabolomics. J. Am. Coll. Cardiol. 2015, 65, 1509–1520. [Google Scholar] [CrossRef] [Green Version]
- Pauly, D.F.; Pepine, C.J. The role of carnitine in myocardial dysfunction. Am. J. Kidney Dis. 2003, 41, S35–S43. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Granger, C.B.; Craig, D.; Haynes, C.; Bain, J.; Stevens, R.D.; Hauser, E.R.; Newgard, C.B.; Kraus, W.E.; Newby, L.K.; et al. Validation of the association between a branched chain amino acid metabolite profile and extremes of coronary artery disease in patients referred for cardiac catheterization. Atherosclerosis 2014, 232, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Zhang, Z.; Kolwicz, S.C.; Abell, L.; Roe, N.D.; Kim, M.; Zhou, B.; Cao, Y.; Ritterhoff, J.; Gu, H.; et al. Defective branched-chain amino acid catabolism disrupts glucose metabolism and sensitizes the heart to ischemia-reperfusion injury. Cell Metab. 2017, 25, 374–385. [Google Scholar] [CrossRef] [Green Version]
- Felker, G.M.; Thompson, R.E.; Hare, J.M.; Hruban, R.H.; Clemetson, D.E.; Howard, D.L.; Baughman, K.L.; Kasper, E.K. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. N. Engl. J. Med. 2000, 342, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Felker, G.M.; Shaw, L.K.; O’Connor, C.M. A standardized definition of ischemic cardiomyopathy for use in clinical research. J. Am. Coll. Cardiol. 2002, 39, 210–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, Y.M.; Elliott, P.M.; Arbustini, E.; Adler, Y.; Anastasakis, A.; Böhm, M.; Duboc, D.; Gimeno, J.; De Groote, P.; Imazio, M.; et al. Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: A position statement of the ESC working group on myocardial and pericardial diseases. Eur. Heart J. 2016, 37, 1850–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollenberg, S.M.; Warner Stevenson, L.; Ahmad, T.; Amin, V.J.; Bozkurt, B.; Butler, J.; Davis, L.L.; Drazner, M.H.; Kirkpatrick, J.N.; Peterson, P.N.; et al. 2019 ACC expert consensus decision pathway on risk assessment, management, and clinical trajectory of patients hospitalized with heart failure: A report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2019, 74, 1966–2011. [Google Scholar] [CrossRef]
- van Vark, L.C.; Lesman-Leegte, I.; Baart, S.J.; Postmus, D.; Pinto, Y.M.; Orsel, J.G.; Westenbrink, B.D.; Rocca, H.P.B.-L.; van Miltenburg, A.J.; Boersma, E.; et al. Prognostic Value of Serial ST2 Measurements in Patients with Acute Heart Failure. J. Am. Coll. Cardiol. 2017, 70, 2378–2388. [Google Scholar] [CrossRef]
- Minkler, P.E.; Stoll, M.S.K.; Ingalls, S.T.; Yang, S.; Kerner, J.; Hoppel, C.L. Quantification of carnitine and acylcarnitines in biological matrices by HPLC electrospray ionization-mass spectrometry. Clin. Chem. 2008, 54, 1451–1462. [Google Scholar] [CrossRef] [Green Version]
- Minkler, P.E.; Stoll, M.S.K.; Ingalls, S.T.; Kerner, J.; Hoppel, C.L. Quantitative acylcarnitine determination by UHPLC-MS/MS—Going beyond tandem MS acylcarnitine “profiles”. Mol. Genet. Metab. 2015, 116, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Song, J.P.; Chen, L.; Chen, X.; Ren, J.; Zhang, N.N.; Tirasawasdichai, T.; Hu, Z.L.; Hua, W.; Hu, Y.R.; Tang, H.-R.; et al. Elevated plasma β-hydroxybutyrate predicts adverse outcomes and disease progression in patients with arrhythmogenic cardiomyopathy. Sci. Transl. Med. Am. Assoc. Adv. Sci. 2020, 12, e8329. [Google Scholar] [CrossRef]
- Taegtmeyer, H.; Young, M.E.; Lopaschuk, G.D.; Abel, E.D.; Brunengraber, H.; Darley-Usmar, V.; Des Rosiers, C.; Gerszten, R.; Glatz, J.F.; Griffin, J.L.; et al. Assessing Cardiac Metabolism: A Scientific Statement from the American Heart Association. Circ. Res. 2016, 118, 1659–1701. [Google Scholar] [CrossRef]
- Abdel-aleem, S.; Sayed-Ahmed, M.; Nada, M.A.; Hendrickson, S.C.; St Louis, J.; Lowe, J.E. Stimulation of non-oxidative glucose utilization by L-carnitine in isolated myocytes. J. Mol. Cell. Cardiol. 1995, 27, 2465–2472. [Google Scholar] [CrossRef] [Green Version]
- Vescovo, G.; Ravara, B.; Gobbo, V.; Dalla Libera, L. Inflammation and perturbation of the l-carnitine system in heart failure. Eur. J. Heart Fail. 2005, 7, 997–1002. [Google Scholar] [CrossRef] [Green Version]
- Rizza, S.; Copetti, M.; Rossi, C.; Cianfarani, M.; Zucchelli, M.; Luzi, A.; Pecchioli, C.; Porzio, O.; Di Cola, G.; Urbani, A.; et al. Metabolomics signature improves the prediction of cardiovascular events in elderly subjects. Atherosclerosis 2014, 232, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Ueland, T.; Svardal, A.; Øie, E.; Askevold, E.T.; Nymoen, S.H.; Bjørndal, B.; Dahl, C.P.; Gullestad, L.; Berge, R.K.; Aukrust, P. Disturbed carnitine regulation in chronic heart failure–increased plasma levels of palmitoyl-carnitine are associated with poor prognosis. Int. J. Cardiol. 2013, 167, 1892–1899. [Google Scholar] [CrossRef] [PubMed]
- Martín, M.A.; Gómez, M.A.; Guillén, F.; Börnstein, B.; Campos, Y.; Rubio, J.; de la Calzada, C.S.; Arenas, J. Myocardial carnitine and carnitine palmitoyltransferase deficiencies in patients with severe heart failure. Biochim. Biophys. Acta 2000, 1502, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter, S.E.; Evans, A.M.; Chace, D.H.; Fornasini, G. Determination of the reference range of endogenous plasma carnitines in healthy adults. Ann. Clin. Biochem. 2008, 45, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Zaugg, C.E.; Spaniol, M.; Kaufmann, P.; Bellahcene, M.; Barbosa, V.; Tolnay, M.; Buser, P.T. Myocardial function and energy metabolism in carnitine-deficient rats. Cell Mol. Life Sci. 2003, 60, 767–775. [Google Scholar] [CrossRef]
- Bergmann, S.R.; Herrero, P.; Sciacca, R.; Hartman, J.J.; Rubin, P.J.; Hickey, K.T.; Epstein, S.; Kelly, D.P. Characterization of altered myocardial fatty acid metabolism in patients with inherited cardiomyopathy. J. Inherit. Metab. Dis. 2001, 24, 657–674. [Google Scholar] [CrossRef]
- Choong, K.; Clarke, J.T.; Cutz, E.; Pollit, R.J.; Olpin, S.E. Lethal cardiac tachyarrhythmia in a patient with neonatal carnitine-acylcarnitine translocase deficiency. Pediatr. Dev. Pathol. 2001, 4, 573–579. [Google Scholar] [CrossRef]
- Lysiak, W.; Toth, P.P.; Suelter, C.H.; Bieber, L.L. Quantitation of the efflux of acylcarnitines from rat heart, brain, and liver mitochondria. J. Biol. Chem. 1986, 261, 13698–13703. [Google Scholar] [CrossRef]
- Yamada, K.A.; Kanter, E.M.; Newatia, A. Long-chain acylcarnitine induces Ca2+ efflux from the sarcoplasmic reticulum. J. Cardiovasc. Pharmacol. 2000, 36, 14–21. [Google Scholar] [CrossRef]
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef] [Green Version]
- Beiert, T.; Straesser, S.; Malotki, R.; Stöckigt, F.; Schrickel, J.W.; Andrié, R.P. Increased mortality and ICD therapies in ischemic versus non-ischemic dilated cardiomyopathy patients with cardiac resynchronization having survived until first device replacement. Arch. Med. Sci. 2019, 15, 845–856. [Google Scholar] [CrossRef]
- Deidda, M.; Piras, C.; Dessalvi, C.C.; Locci, E.; Barberini, L.; Torri, F.; Ascedu, F.; Atzori, L.; Mercuro, G. Metabolomic approach to profile functional and metabolic changes in heart failure. J. Transl. Med. 2015, 13, 297–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, W.G.; Kelly, J.P.; McGarrah, R.W.; Khouri, M.G.; Craig, D.; Haynes, C.; Ilkayeva, O.; Stevens, R.D.; Bain, J.R.; Muehlbauer, M.J.; et al. Metabolomic Profiling Identifies Novel Circulating Biomarkers of Mitochondrial Dysfunction Differentially Elevated in Heart Failure with Preserved versus Reduced Ejection Fraction: Evidence for Shared Metabolic Impairments in Clinical Heart Failure. J. Am. Heart Assoc. 2016, 5, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierpont, M.E.; Judd, D.; Goldenberg, I.F.; Ring, W.S.; Olivari, M.T.; Pierpont, G.L. Myocardial carnitine in end-stage congestive heart failure. Am. J. Cardiol. 1989, 64, 56–60. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 48) | IHD-HF Group (n = 63) | DCM Group (n = 98) | |
|---|---|---|---|
| Age (years) | 47 ± 16 | 65 ± 9 * | 61 ± 14 *# |
| Male (%) | 21 (43.8) | 58 (92.1) * | 83 (84.7) * |
| Heart rate (beats/min) | 77 ± 11 | 77 ± 15 | 76 ± 14 |
| Hypertension (%) | 1 (2.1) | 35 (55.6) * | 40 (40.8) * |
| Diabetes (%) | 1 (2.1) | 18 (28.6) * | 23 (23.5) * |
| History of PCI/CABG (%) | 0 (0) | 30 (47.6) | 0 (0) |
| History of MI | 0 (0) | 26 (41.3) | 0 (0) |
| Systolic BP (mmHg) | 121 ± 13 | 127 ± 21 | 118 ± 25 # |
| Diastolic BP (mmHg) | 77 ± 9 | 79 ± 12 | 76 ± 13 |
| Blood glucose (mmol/L) | 4.91 ± 0.58 | 6.95 ± 3.45 * | 6.16 ± 2.31 * |
| HbA1c (%) | 5.44 ± 0.41 | 6.45 ± 1.34 * | 6.27 ± 0.99 * |
| D-dimer (mg/L) | 0.27 ± 0.23 | 0.73 ± 1.19 * | 0.80 ± 1.11 * |
| Hemoglobin (g/L) | 135 ± 17 | 136 ± 18 | 137 ± 20 |
| Serum creatinine (μmol/L) | 69.3 ± 16.7 | 100.8 ± 29.7 * | 107.2 ± 46.6 * |
| Serum Uric acid (μmol/L) | 308.9 ± 77.9 | 437.7 ± 123.8* | 480.1 ± 137.9 *# |
| Total cholesterol (mmol/L) | 4.39 ± 0.94 | 3.67 ± 1.03 * | 3.93 ± 1.04 * |
| Triglyceride (mmol/L) | 1.39 ± 0.82 | 1.81 ± 1.31 * | 1.56 ± 0.98 |
| HDL-C (mmol/L) | 1.22 ± 0.31 | 0.97 ± 0.22 * | 1.11 ± 0.58 |
| LDL-C (mmol/L) | 2.56 ± 0.82 | 1.94 ± 0.82 * | 2.22 ± 0.88 *# |
| NYHA (grade): | |||
| I–II | 48 (100.0) | 54 (85.7) * | 54 (55.1) *# |
| III–IV | 0 (0) | 9 (12.3) * | 44 (44.9) *# |
| CRP (mg/L) | 0.86 ± 1.01 | 8.89 ± 13.83 * | 8.91 ± 16.10 * |
| Troponin T (ng/mL) | 0.005 ± 0.006 | 0.093 ± 0.147 * | 0.042 ± 0.041 *# |
| NT-pro-BNP (pg/mL) | 66.5 ± 78.1 | 3402.4 ± 4170.6 * | 4635.0 ± 5561.2 * |
| stenosis ≥ 75% & vessels ≥ 2 | -- | 34 (54.0) | 0 (0) |
| LM stenosis ≥ 75% | -- | 7 (11.1) | 0 (0) |
| LAD stenosis ≥ 75% | -- | 26 (41.3) | 0 (0) |
| Medication, n (%) | |||
| ACEI/ARB | -- | 57 (90.5) | 93 (94.9) |
| Beta-blocker | -- | 59 (93.7) | 92 (93.9) |
| MRA | -- | 38 (60.3) | 66 (67.3) |
| statins | -- | 58 (92.1) | 23 (23.5) # |
| Carnitines | Abbreviation | Control Group (n = 48) | All HF Patients (n = 161) | IHD-HF Group (n = 63) | DCM-HF Group (n = 98) |
|---|---|---|---|---|---|
| L-Carnitine | C0 | 6468.6 ± 1294.1 | 7154.0 ± 1990.8 * | 6799.9 ± 1891.6 | 7381.6 ± 2028.95 * |
| O-Acetyl-L-carnitine | C2 | 6157.3 ± 1920.3 | 10,595.1 ± 6154.2 * | 9140.4 ± 4862.7 * | 11530.3 ± 6715.7 *# |
| Propionyl-L-carnitine | C3 | 437.6 ± 218.8 | 698.0 ± 450.8 * | 564.1 ± 205.3 | 783.0 ± 537.7 *# |
| Butyryl-L-carnitine | C4 | 114.4 ± 43.6 | 184.8 ± 98.1 * | 163.7 ± 84.8 * | 198.4 ± 103.9 *# |
| Isobutyryl-L-carnitine | isoC4 | 142.9 ± 110.3 | 314.5 ± 252.2 * | 252.5 ± 177.1 * | 354.4 ± 284.2 *# |
| Isovaleryl-L-carnitine | isoC5 | 106.3 ± 35.5 | 142.4 ± 64.1 * | 131.9 ± 58.5 * | 149.2 ± 66.8 * |
| 2-Methylbutyryl-L-Carnitine | MC4 | 43.1 ± 17.8 | 76.2 ± 47.2 * | 69.0 ± 37.5 * | 80.9 ± 52.5 * |
| Methylmalonyl DL-Carnitine | MM | b.LOD | b.LOD | b.LOD | b.LOD |
| Valeryl-L-carnitine | C5 | 2.03 ± 2.06 | 4.56 ± 4.08 * | 3.75 ± 2.35 * | 5.08 ± 4.82 *# |
| 3-Hydroxybutyrylcarnitine | C4OH | 28.8 ± 21.4 | 100.1 ± 117.2 * | 78.5 ± 101.0 * | 114.0 ± 125.0 * |
| Hexanoyl-L-carnitine | C6 | 49.2 ± 29.5 | 105.7 ± 75.5 * | 86.6 ± 63.4 * | 117.9 ± 80.4 *# |
| Succinyl Carnitine | C4DC | 20.8 ± 7.6 | 46.2 ± 23.5 * | 42.0 ± 22.7 * | 49.0 ± 23.7 * |
| (2R)-3-Hydroxyisovaleroyl Carnitine | C5OH | 18.1 ± 5.1 | 35.4 ± 30.1 * | 30.2 ± 17.5 * | 38.7 ± 35.6 * |
| L-Glutaryl Carnitine | C5DC | 316.0 ± 141.6 | 503.9 ± 397.4 * | 492.1 ± 346.4 * | 511.4 ± 428.6 * |
| Octanoyl-L-carnitine | C8 | 97.7 ± 85.3 | 159.8 ± 101.3 * | 147.1 ± 100.7 * | 168.0 ± 101.3 * |
| Adipoyl-L-carnitine | C6DC | 12.6 ± 8.2 | 41.5 ± 52.7 * | 35.5 ± 43.5 * | 45.3 ± 57.8 * |
| Decanoyl-L-carnitine | C10 | 127.9 ± 136.1 | 198.6 ± 131.5 * | 184.8 ± 139.2 * | 207.5 ± 126.2 * |
| Lauroyl-L-carnitine | C12 | 18.4 ± 16.9 | 37.0 ± 32.4 * | 35.1 ± 37.2 * | 38.2 ± 29.0 * |
| 5-cis-Tetradecenoyl Carnitine | C14:1 | 41.5 ± 30.1 | 98.5 ± 105.8 * | 88.6 ± 122.2 * | 104.9 ± 94.0 * |
| Myristoyl-L-carnitine | C14 | 1.75 ± 4.33 | 11.88 ± 15.38 * | 10.00 ± 17.8 * | 13.1 ± 13.6 * |
| Palmitoyl-L-carnitine | C16 | 95.8 ± 24.1 | 146.2 ± 55.62 * | 129.7 ± 45.0 * | 156.8 ± 59.3 *# |
| 3-Hydroxyhexadecanoyl-Carnitine | C16OH | b.LOD | b.LOD | b.LOD | b.LOD |
| Linoleoyl-L-carnitine | C18:2 | 169.0 ± 54.8 | 332.4 ± 156.3 * | 278.3 ± 105.3 * | 367.2 ± 173.4 *# |
| Oleoyl L-carnitine | C18:1 | 154.1 ± 44.9 | 297.5 ± 140.9 * | 246.2 ± 93.3 * | 330.6 ± 156.1 *# |
| Stearoyl-L-carnitine | C18 | 45.5 ± 9.0 | 63.0 ± 22.9 * | 54.5 ± 16.9 * | 68.5 ± 24.5 *# |
| 3-Hydroxyoleylcarnitine | C18:1OH | 1.12 ± 0.85 | 2.43 ± 2.13 * | 2.10 ± 1.90 * | 2.64 ± 2.25 * |
| Arachidonoyl-L-carnitine | C20:4 | 32.1 ± 14.2 | 74.0 ± 46.2 * | 64.0 ± 31.8 * | 80.4 ± 52.7 *# |
| ROC | Unadjusted | Adjusted by ACGH | ||||||
|---|---|---|---|---|---|---|---|---|
| C Value | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| NT-pro-BNP | 0.995 | <0.01 | 1.019 | 1.010–1.028 | <0.01 | 1.020 | 1.008–1.033 | <0.01 |
| C0 | 0.614 | 0.017 | 1.000 | 1.000–1.000 | 0.027 | 1.000 | 1.000–1.001 | <0.01 |
| C2 | 0.794 | <0.01 | 1.000 | 1.000–1.001 | <0.01 | 1.000 | 1.000–1.001 | <0.01 |
| C3 | 0.776 | <0.01 | 1.005 | 1.003–1.007 | <0.01 | 1.004 | 1.001–1.007 | <0.01 |
| C4 | 0.769 | <0.01 | 1.021 | 1.012–1.031 | <0.01 | 1.021 | 1.008–1.033 | <0.01 |
| isoC4 | 0.805 | <0.01 | 1.009 | 1.005–1.014 | <0.01 | 1.006 | 1.002–1.010 | <0.01 |
| isoC5 | 0.670 | <0.01 | 1.013 | 1.006–1.021 | <0.01 | 1.011 | 1.001–1.021 | 0.031 |
| MC4 | 0.806 | <0.01 | 1.059 | 1.034–1.085 | <0.01 | 1.038 | 1.008–1.068 | 0.012 |
| C5 | 0.768 | <0.01 | 1.575 | 1.290–1.294 | <0.01 | 1.455 | 1.090–1.944 | 0.011 |
| C4OH | 0.820 | <0.01 | 1.048 | 1.026–1.071 | <0.01 | 1.041 | 1.011–1.071 | <0.01 |
| C6 | 0.829 | <0.01 | 1.042 | 1.025–1.059 | <0.01 | 1.032 | 1.013–1.052 | <0.01 |
| C4DC | 0.915 | <0.01 | 1.224 | 1.145–1.308 | <0.01 | 1.211 | 1.105–1.328 | <0.01 |
| C5OH | 0.835 | <0.01 | 1.218 | 1.133–1.311 | <0.01 | 1.236 | 1.115–1.369 | <0.01 |
| C5DC | 0.695 | <0.01 | 1.004 | 1.002–1.007 | <0.01 | -- | -- | NS |
| C8 | 0.762 | <0.01 | 1.012 | 1.005–1.018 | <0.01 | -- | -- | NS |
| C6DC | 0.848 | <0.01 | 1.149 | 1.088–1.213 | <0.01 | 1.121 | 1.045–1.203 | <0.01 |
| C10 | 0.746 | <0.01 | 1.007 | 1.002–1.011 | <0.01 | -- | -- | NS |
| C12 | 0.766 | <0.01 | 1.059 | 1.029–1.090 | <0.01 | -- | -- | NS |
| C14:1 | 0.785 | <0.01 | 1.032 | 1.017–1.047 | <0.01 | 1.018 | 1.002–1.034 | 0.027 |
| C14 | 0.763 | <0.01 | 1.189 | 1.108–1.276 | <0.01 | 1.155 | 1.051–1.269 | <0.01 |
| C16 | 0.812 | <0.01 | 1.040 | 1.025–1.055 | <0.01 | 1.045 | 1.021–1.069 | <0.01 |
| C18:2 | 0.868 | <0.01 | 1.020 | 1.013–1.027 | <0.01 | 1.020 | 1.010–1.030 | <0.01 |
| C18:1 | 0.870 | <0.01 | 1.023 | 1.015–1.032 | <0.01 | 1.022 | 1.011–1.033 | <0.01 |
| C18 | 0.753 | <0.01 | 1.073 | 1.041–1.105 | <0.01 | 1.084 | 1.029–1.142 | <0.01 |
| C18:1OH | 0.742 | <0.01 | 2.329 | 1.596–3.397 | <0.01 | -- | -- | NS |
| C20:4 | 0.871 | <0.01 | 1.087 | 1.057–1.118 | <0.01 | 1.079 | 1.039–1.121 | <0.01 |
| ROC | Unadjusted | Adjusted by ALU | Adjusted by ALU and LVEF | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| C Value | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| BNP | 0.587 | 0.064 | -- | -- | NS | -- | -- | NS | -- | -- | NS |
| Troponin T | 0.478 | 0.645 | 0.002 | 0.000–0.209 | <0.01 | 0.001 | 0.000–0.136 | <0.01 | 0.000 | 0.000–0091 | <0.01 |
| C2 | 0.627 | <0.01 | 1.000 | 1.000–1.000 | 0.021 | 1.000 | 1.000–1.000 | 0.020 | 1.000 | 1.000–1.000 | 0.039 |
| C3 | 0.642 | <0.01 | 1.002 | 1.001–1.003 | <0.01 | 1.002 | 1.001–1.003 | <0.01 | 1.002 | 1.001–1.004 | <0.01 |
| C4 | 0.615 | 0.014 | 1.004 | 1.000–1.008 | 0.034 | -- | -- | NS | -- | -- | NS |
| isoC4 | 0.610 | 0.019 | 1.002 | 1.000–1.004 | 0.016 | 1.004 | 1.001–1.006 | <0.01 | 1.004 | 1.001–1.007 | <0.01 |
| C5 | 0.565 | 0.163 | 1.116 | 1.000–1.246 | 0.050 | -- | -- | NS | -- | -- | NS |
| C6 | 0.625 | <0.01 | 1.006 | 1.001–1.013 | 0.014 | 1.010 | 1.002–1.018 | 0.011 | 1.009 | 1.001–1.017 | 0.019 |
| C16 | 0.642 | <0.01 | 1.011 | 1.003–1.018 | <0.01 | 1.010 | 1.002–1.019 | 0.016 | -- | -- | NS |
| C18:2 | 0.645 | <0.01 | 1.004 | 1.002–1.007 | <0.01 | 1.005 | 1.002–1.008 | <0.01 | 1.004 | 1.001–1.007 | 0.010 |
| C18:1 | 0.668 | <0.01 | 1.006 | 1.002–1.009 | <0.01 | 1.006 | 1.002–1.010 | <0.01 | 1.005 | 1.001–1.009 | <0.01 |
| C18 | 0.676 | <0.01 | 1.034 | 1.015–1.053 | <0.01 | 1.032 | 1.011–1.053 | <0.01 | 1.028 | 1.007–1.050 | <0.01 |
| C20:4 | 0.560 | 0.200 | 1.009 | 1.001–1.017 | 0.033 | -- | -- | NS | -- | -- | NS |
| Univariate COX Regression | For Mortality | For HF Rehospitalization | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| age > 65 | 1.978 (1.056–3.704) | 0.033 | 1.793 (1.037–3.099) | 0.037 |
| serum creatinine > 2 mg/dL | 7.687 (3.191–18.518) | <0.01 | 3.572 (1.415–9.016) | <0.01 |
| NT-pro-BNP > 4000 pg/mL | 3.184 (1.705–5.947) | <0.01 | 2.659 (1.556–4.543) | <0.01 |
| left atrial diameter > 55 mm | 2.847 (1.482–5.467) | <0.01 | 2.410 (1.325–4.382) | <0.01 |
| LVEF < 35% | 1.106 (0.607–2.014) | 0.742 | 3.380 (1.836–6.221) | <0.01 |
| diagnosis of DCM | 0.822 (0.449–1.507) | 0.527 | 1.900 (1.033–3.495) | 0.039 |
| Multivariate COX regression | Unadjusted | Adjusted | ||
| HR (95% CI) | p value | HR (95% CI) | p value | |
| For all-cause mortality † | ||||
| C18:1 > 300 nmol/L | 2.402 (1.309–4.406) | <0.01 | 2.363 (1.122–4.976) | 0.024 |
| isoC5 < 100 nmol/L | 2.483 (1.353–4.556) | <0.01 | 2.108 (1.091–4.074) | 0.026 |
| For HF rehospitalization ‡ | ||||
| C18:2 > 420 nmol/L | 2.783 (1.607–4.822) | <0.01 | 2.088 (1.071–4.067) | 0.031 |
| C4DC > 60 nmol/L | 2.964 (1.691–5.193) | <0.01 | 2.121 (1.002–4.490) | 0.049 |
| isoC5 < 100 nmol/L | 2.277 (1.308–3.964) | <0.01 | 2.302 (1.282–4.132) | 0.010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Lu, D.; Qi, B.; Wu, Y.; Xia, Y.; Chen, A.; Li, S.; Tang, H.; Qian, J.; Ge, J. Quantitative Profiling of Serum Carnitines Facilitates the Etiology Diagnosis and Prognosis Prediction in Heart Failure. Molecules 2023, 28, 5345. https://doi.org/10.3390/molecules28145345
Chen Z, Lu D, Qi B, Wu Y, Xia Y, Chen A, Li S, Tang H, Qian J, Ge J. Quantitative Profiling of Serum Carnitines Facilitates the Etiology Diagnosis and Prognosis Prediction in Heart Failure. Molecules. 2023; 28(14):5345. https://doi.org/10.3390/molecules28145345
Chicago/Turabian StyleChen, Zhangwei, Danbo Lu, Baoling Qi, Yuan Wu, Yan Xia, Ao Chen, Su Li, Huiru Tang, Juying Qian, and Junbo Ge. 2023. "Quantitative Profiling of Serum Carnitines Facilitates the Etiology Diagnosis and Prognosis Prediction in Heart Failure" Molecules 28, no. 14: 5345. https://doi.org/10.3390/molecules28145345
APA StyleChen, Z., Lu, D., Qi, B., Wu, Y., Xia, Y., Chen, A., Li, S., Tang, H., Qian, J., & Ge, J. (2023). Quantitative Profiling of Serum Carnitines Facilitates the Etiology Diagnosis and Prognosis Prediction in Heart Failure. Molecules, 28(14), 5345. https://doi.org/10.3390/molecules28145345