
Measurement of Urinary Gc-Globulin by a Fluorescence ELISA Technique: Method Validation and Clinical Evaluation in Septic Patients—A Pilot Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Optimization of Antigen Coating and Antibody Dilutions
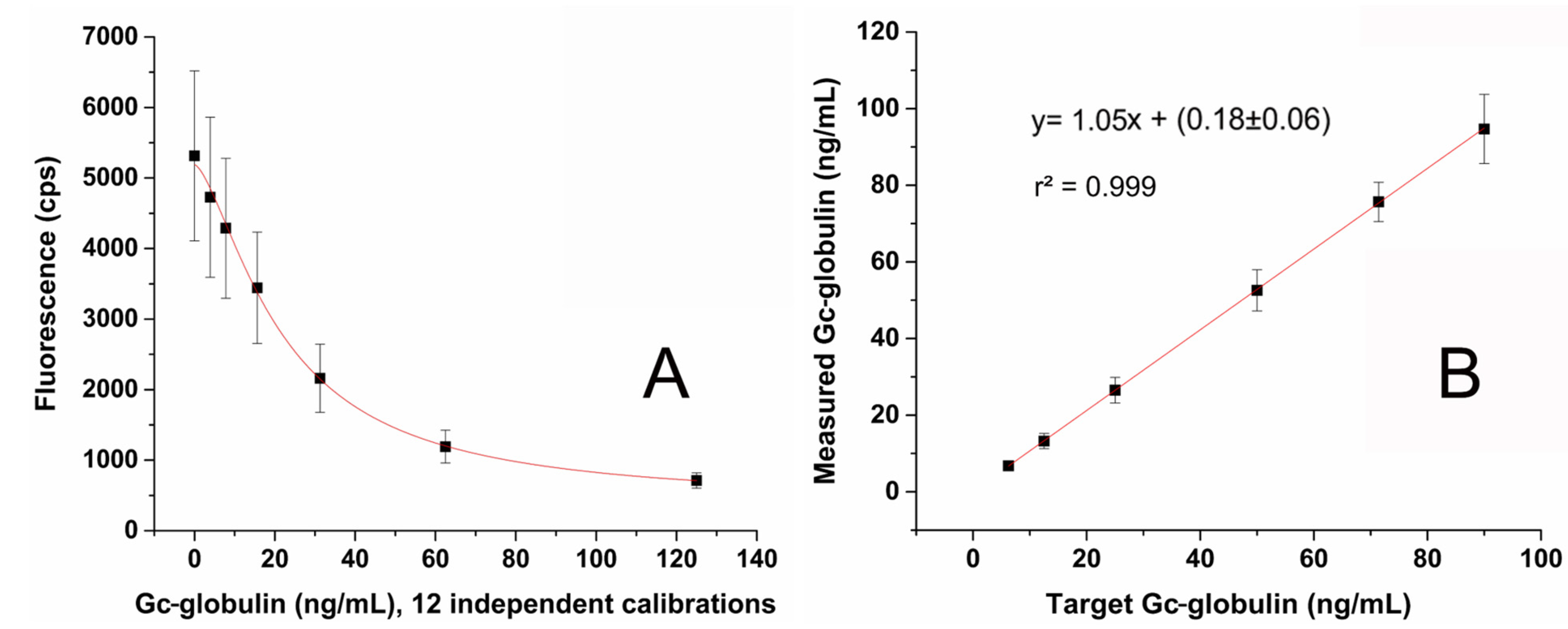
2.2. Validation of the Method
2.3. Patients’ Demographic and Laboratory Data
2.4. Septic Patients’ Clinical Data
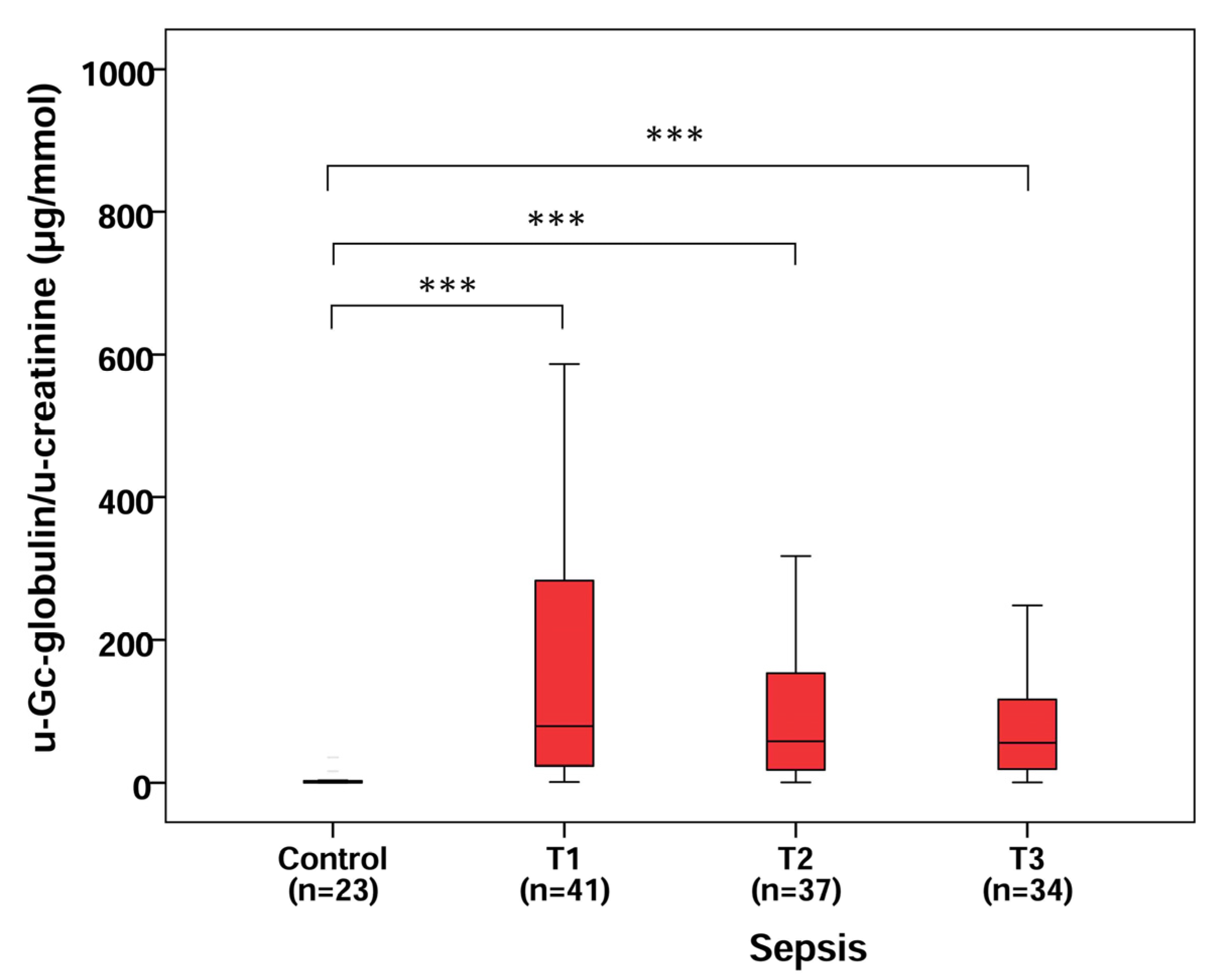
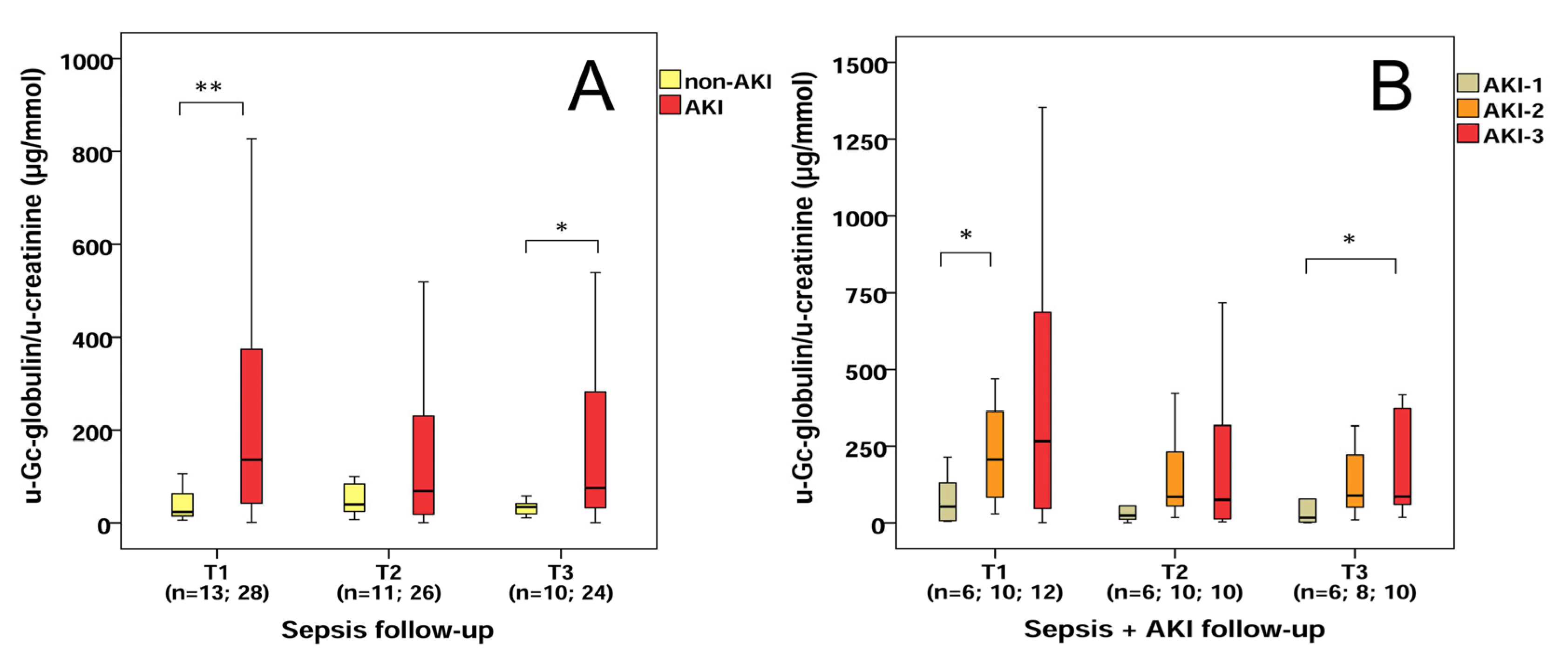
2.5. U-Gc/u-Creatinine Levels in Control, Septic and Sepsis-Related AKI Patients
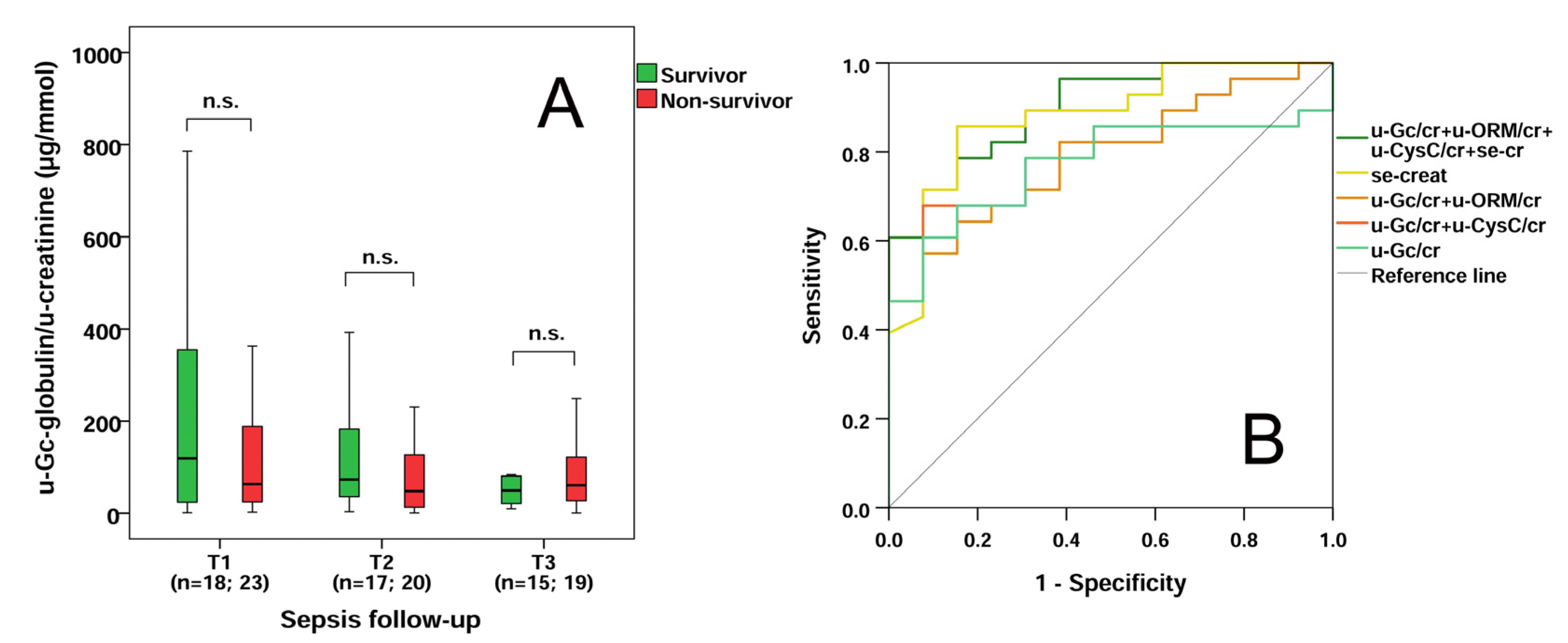
2.6. Survival Data and Distinctive Power of u-Gc Globulin/u-Creatinine Levels in Sepsis
2.7. Correlations
3. Discussion
4. Materials and Methods
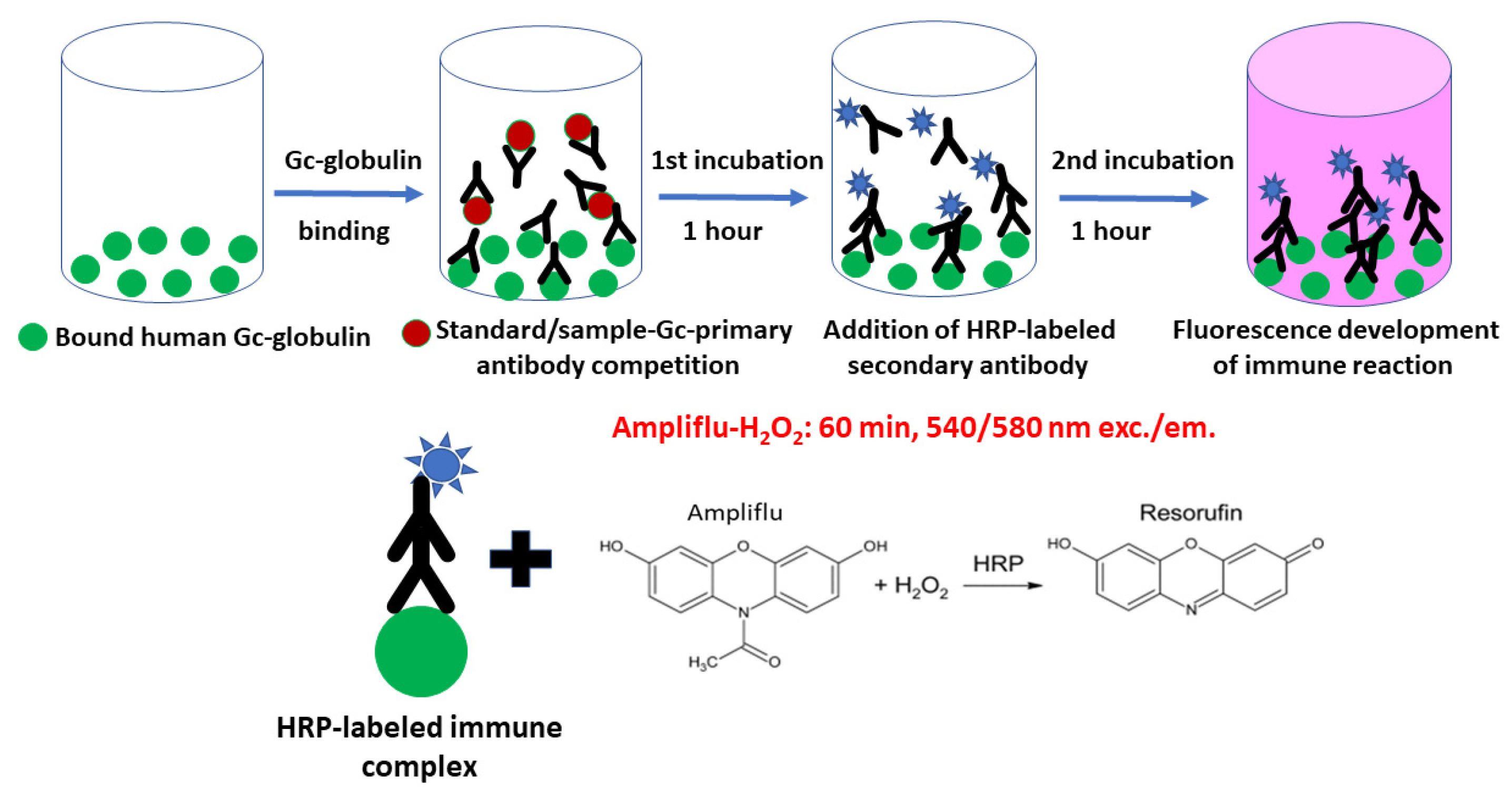
4.1. Development of a Competitive u-Gc Elisa Assay with Fluorescence Detection
Validation of the Method
4.2. Patient Enrollment and Study Design
Clinical Data and Laboratory Testing
4.3. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K.; International Forum of Acute Care Trialists. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Kumar, A.; Gangadharan, S. Biomarkers and newer laboratory investigations in the diagnosis of sepsis. J. R. Coll. Physicians Edinb. 2019, 49, 207–216. [Google Scholar] [CrossRef] [PubMed]
- László, I.; Trásy, D.; Molnár, Z.; Fazakas, J. Sepsis: From Pathophysiology to Individualized Patient Care. J. Immunol. Res. 2015, 2015, 510436. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Taeb, A.M. SIRS, qSOFA and new sepsis definition. J. Thorac. Dis. 2017, 9, 943–945. [Google Scholar] [CrossRef] [PubMed]
- Peerapornratana, S.; Manrique-Caballero, C.L.; Gómez, H.; Kellum, J.A. Acute kidney injury from sepsis: Current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019, 96, 1083–1099. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Zarbock, A.; Nadim, M.K.; Pickkers, P.; Gomez, H.; Bell, S.; Joannidis, M.; Kashani, K.; Koyner, J.L.; Pannu, N.; Meersch, M.; et al. Sepsis-associated acute kidney injury: Consensus report of the 28th Acute Disease Quality Initiative workgroup. Nat. Rev. Nephrol. 2023, 19, 401–417. [Google Scholar] [CrossRef]
- Ostermann, M.; Zarbock, A.; Goldstein, S.; Kashani, K.; Macedo, E.; Murugan, R.; Bell, M.; Forni, L.; Guzzi, L.; Joannidis, M.; et al. Recommendations on Acute Kidney Injury Biomarkers from the Acute Disease Quality Initiative Consensus Conference: A Consensus Statement. JAMA Netw. Open 2020, 3, e2019209. [Google Scholar] [CrossRef]
- Ragán, D.; Horváth-Szalai, Z.; Szirmay, B.; Mühl, D. Novel Damage Biomarkers of Sepsis-Related Acute Kidney Injury. eJIFCC 2022, 33, 11–22. [Google Scholar]
- van Engelen, T.S.R.; Wiersinga, W.J.; Scicluna, B.P.; van der Poll, T. Biomarkers in Sepsis. Crit. Care Clin. 2018, 34, 139–152. [Google Scholar] [CrossRef]
- Póvoa, P.; Coelho, L.; Dal-Pizzol, F.; Ferrer, R.; Huttner, A.; Conway Morris, A.; Nobre, V.; Ramirez, P.; Rouze, A.; Salluh, J.; et al. How to use biomarkers of infection or sepsis at the bedside: Guide to clinicians. Intensive Care Med. 2023, 49, 142–153. [Google Scholar] [CrossRef]
- Kim, M.H.; Choi, J.H. An Update on Sepsis Biomarkers. Infect. Chemother. 2020, 52, 1–18. [Google Scholar] [CrossRef]
- Kustán, P.; Szirmay, B.; Horváth-Szalai, Z.; Ludány, A.; Lakatos, Á.; Mühl, D.; Christensen, P.H.; Miseta, A.; Kovács, G.L.; Kőszegi, T. Urinary orosomucoid: Validation of an automated immune turbidimetric test and its possible clinical use. Biochem. Med. 2016, 26, 421–430. [Google Scholar] [CrossRef]
- Kustán, P.; Szirmay, B.; Horváth-Szalai, Z.; Ludány, A.; Kovács, G.L.; Miseta, A.; Kőszegi, T.; Mühl, D. Urinary orosomucoid: A novel, early biomarker of sepsis with promising diagnostic performance. Clin. Chem. Lab. Med. 2017, 55, 299–307. [Google Scholar] [CrossRef]
- Horváth-Szalai, Z.; Kustán, P.; Mühl, D.; Ludány, A.; Bugyi, B.; Kőszegi, T. Antagonistic sepsis markers: Serum gelsolin and actin/gelsolin ratio. Clin. Biochem. 2017, 50, 127–133. [Google Scholar] [CrossRef]
- Kustán, P.; Horváth-Szalai, Z.; Mühl, D. Nonconventional Markers of Sepsis. eJIFCC 2017, 28, 122–133. [Google Scholar]
- Horváth-Szalai, Z.; Kustán, P.; Szirmay, B.; Lakatos, Á.; Christensen, P.H.; Huber, T.; Bugyi, B.; Mühl, D.; Ludány, A.; Miseta, A.; et al. Validation of an automated immune turbidimetric assay for serum gelsolin and its possible clinical utility in sepsis. J. Clin. Lab. Anal. 2018, 32, e22321. [Google Scholar] [CrossRef]
- Szirmay, B.; Kustán, P.; Horváth-Szalai, Z.; Ludány, A.; Lakatos, Á.; Mühl, D.; Wittmann, I.; Miseta, A.; Kovács, G.L.; Kőszegi, T. Novel automated immune turbidimetric assay for routine urinary cystatin-C determinations. Bioanalysis 2018, 10, 377–384. [Google Scholar] [CrossRef]
- Horváth-Szalai, Z.; Kustán, P.; Szirmay, B.; Lakatos, Á.; Christensen, P.H.; Huber, T.; Bugyi, B.; Mühl, D.; Ludány, A.; Miseta, A.; et al. Predictive value of serum gelsolin and Gc globulin in sepsis—A pilot study. Clin. Chem. Lab. Med. 2018, 56, 1373–1382. [Google Scholar] [CrossRef]
- Ragán, D.; Kustán, P.; Horváth-Szalai, Z.; Szirmay, B.; Bugyi, B.; Ludány, A.; Miseta, A.; Nagy, B.; Mühl, D. Urinary actin, as a potential marker of sepsis-related acute kidney injury: A pilot study. PLoS ONE 2021, 16, e0255266. [Google Scholar] [CrossRef]
- Ragán, D.; Kustán, P.; Horváth-Szalai, Z.; Szirmay, B.; Miseta, A.; Woth, G.; Kőszegi, T.; Mühl, D. Presepsin: Gelsolin ratio, as a promising marker of sepsis-related organ dysfunction: A prospective observational study. Front. Med. 2023, 10, 1126982. [Google Scholar] [CrossRef]
- Haddad, J.G.; Harper, K.D.; Guoth, M.; Pietra, G.G.; Sanger, J.W. Angiopathic consequences of saturating the plasma scavenger system for actin. Proc. Natl. Acad. Sci. USA 1990, 87, 1381–1385. [Google Scholar] [CrossRef]
- Lind, S.E.; Smith, C.J. Actin is a noncompetitive plasmin inhibitor. J. Biol. Chem. 1991, 266, 5273–5278. [Google Scholar] [CrossRef]
- Janmey, P.A.; Lamb, J.A.; Ezzell, R.M.; Hvidt, S.; Lind, S.E. Effects of actin filaments on fibrin clot structure and lysis. Blood 1992, 80, 928–936. [Google Scholar] [CrossRef]
- Belsky, J.B.; Morris, D.C.; Bouchebl, R.; Filbin, M.R.; Bobbitt, K.R.; Jaehne, A.K.; Rivers, E.P. Plasma levels of F-actin and F:G-actin ratio as potential new biomarkers in patients with septic shock. Biomarkers 2016, 21, 180–185. [Google Scholar] [CrossRef]
- Gu, X.; Yao, Y.; Wu, G.; Lv, T.; Luo, L.; Song, Y. The plasma mitochondrial DNA is an independent predictor for post-traumatic systemic inflammatory response syndrome. PLoS ONE 2013, 8, e72834. [Google Scholar] [CrossRef]
- Hazeldine, J.; Dinsdale, R.J.; Naumann, D.N.; Acharjee, A.; Bishop, J.R.B.; Lord, J.M.; Harrison, P. Traumatic injury is associated with reduced deoxyribonuclease activity and dysregulation of the actin scavenging system. Burn. Trauma 2021, 9, tkab001. [Google Scholar] [CrossRef]
- Lee, P.S.; Sampath, K.; Karumanchi, S.A.; Tamez, H.; Bhan, I.; Isakova, T.; Gutierrez, O.M.; Wolf, M.; Chang, Y.; Stossel, T.P.; et al. Plasma gelsolin and circulating actin correlate with hemodialysis mortality. J. Am. Soc. Nephrol. 2009, 20, 1140–1148. [Google Scholar] [CrossRef]
- Suhler, E.; Lin, W.; Yin, H.L.; Lee, W.M. Decreased plasma gelsolin concentrations in acute liver failure, myocardial infarction, septic shock, and myonecrosis. Crit. Care Med. 1997, 25, 594–598. [Google Scholar] [CrossRef]
- Meier, U.; Gressner, O.; Lammert, F.; Gressner, A.M. Gc-globulin: Roles in response to injury. Clin. Chem. 2006, 52, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Delanghe, J.R.; Speeckaert, R.; Speeckaert, M.M. Behind the scenes of vitamin D binding protein: More than vitamin D binding. Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 773–786. [Google Scholar] [CrossRef] [PubMed]
- Ciriello, V.; Gudipati, S.; Stavrou, P.Z.; Kanakaris, N.K.; Bellamy, M.C.; Giannoudis, P.V. Biomarkers predicting sepsis in polytrauma patients: Current evidence. Injury 2013, 44, 1680–1692. [Google Scholar] [CrossRef]
- Chaykovska, L.; Heunisch, F.; von Einem, G.; Alter, M.L.; Hocher, C.F.; Tsuprykov, O.; Dschietzig, T.; Kretschmer, A.; Hocher, B. Urinary Vitamin D Binding Protein and KIM-1 Are Potent New Biomarkers of Major Adverse Renal Events in Patients Undergoing Coronary Angiography. PLoS ONE 2016, 11, e0145723. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Riera, E.; García-Arguinzonis, M.; López, L.; Garcia-Moll, X.; Badimon, L.; Padró, T. Vitamin D Binding Protein and Renal Injury in Acute Decompensated Heart Failure. Front. Cardiovasc. Med. 2022, 9, 829490. [Google Scholar] [CrossRef]
- Thrailkill, K.M.; Jo, C.H.; Cockrell, G.E.; Moreau, C.S.; Fowlkes, J.L. Enhanced excretion of vitamin D binding protein in type 1 diabetes: A role in vitamin D deficiency? J. Clin. Endocrinol. Metab. 2011, 96, 142–149. [Google Scholar] [CrossRef]
- Tian, X.Q.; Zhao, L.M.; Ge, J.P.; Zhang, Y.; Xu, Y.C. Elevated urinary level of vitamin D-binding protein as a novel biomarker for diabetic nephropathy. Exp. Ther. Med. 2014, 7, 411–416. [Google Scholar] [CrossRef]
- Abdella, N.A.; Mojiminiyi, O.A. Vitamin D-Binding Protein Clearance Ratio Is Significantly Associated with Glycemic Status and Diabetes Complications in a Predominantly Vitamin D-Deficient Population. J. Diabetes Res. 2018, 2018, 6239158. [Google Scholar] [CrossRef]
- Bai, X.; Luo, Q.; Tan, K.; Guo, L. Diagnostic value of VDBP and miR-155-5p in diabetic nephropathy and the correlation with urinary microalbumin. Exp. Ther. Med. 2020, 20, 86. [Google Scholar] [CrossRef]
- Brunner, H.I.; Bennett, M.R.; Gulati, G.; Abulaban, K.; Klein-Gitelman, M.S.; Ardoin, S.P.; Tucker, L.B.; Rouster-Stevens, K.A.; Witte, D.; Ying, J.; et al. Urine Biomarkers to Predict Response to Lupus Nephritis Therapy in Children and Young Adults. J. Rheumatol. 2017, 44, 1239–1248. [Google Scholar] [CrossRef]
- Liu, L.; Wang, R.; Ding, H.; Tian, L.; Gao, T.; Bao, C. The utility of urinary biomarker panel in predicting renal pathology and treatment response in Chinese lupus nephritis patients. PLoS ONE 2020, 15, e0240942. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.R.; Pordal, A.; Haffner, C.; Pleasant, L.; Ma, Q.; Devarajan, P. Urinary Vitamin D-Binding Protein as a Biomarker of Steroid-Resistant Nephrotic Syndrome. Biomark Insights 2016, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.R.; Pleasant, L.; Haffner, C.; Ma, Q.; Haffey, W.D.; Ying, J.; Wagner, M.; Greis, K.D.; Devarajan, P. A Novel Biomarker Panel to Identify Steroid Resistance in Childhood Idiopathic Nephrotic Syndrome. Biomark Insights 2017, 12, 1177271917695832. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, A.; Mohanraj, P.S.; Krishnamurthy, S.; Rajappa, M. Association of Urinary Vitamin D Binding Protein and Neutrophil Gelatinase-Associated Lipocalin with Steroid Responsiveness in Idiopathic Nephrotic Syndrome of Childhood. Saudi J. Kidney Dis. Transpl. 2020, 31, 946–956. [Google Scholar] [CrossRef]
- Kalousova, M.; Dusilova-Sulkova, S.; Zakiyanov, O.; Kostirova, M.; Safranek, R.; Tesar, V.; Zima, T. Vitamin D Binding Protein Is Not Involved in Vitamin D Deficiency in Patients with Chronic Kidney Disease. BioMed Res. Int. 2015, 2015, 492365. [Google Scholar] [CrossRef]
- Gaipov, A.; Makhammajanov, Z.; Dauyey, Z.; Markhametova, Z.; Mussina, K.; Nogaibayeva, A.; Kozina, L.; Auganova, D.; Tarlykov, P.; Bukasov, R.; et al. Urinary Protein Profiling for Potential Biomarkers of Chronic Kidney Disease: A Pilot Study. Diagnostics 2022, 12, 2583. [Google Scholar] [CrossRef]
- Albejante, M.C.; Kunz, T.C.M.; Ferreira, M.F.C.; Júnior, J.H.Z.R.; de Almeida, R.J.; Bacigalupo, L.D.S.; Matheus, L.H.G.; Dalboni, M.A.; Camacho, C.P.; Dellê, H. Proteinuria is Associated with Urinary Loss of Cubilin and Vitamin D-Binding Protein in Patients with Preeclampsia. Sci. Rep. 2020, 10, 3956. [Google Scholar] [CrossRef]
- Chen, W.C.; Cheng, C.M.; Liao, W.T.; Chang, T.C. Urinary Biomarkers for Detection of Clinical Endometriosis or Adenomyosis. Biomedicines 2022, 10, 833. [Google Scholar] [CrossRef]
- Human Vitamin D BP Quanitikine (rndsystems.com). Available online: https://www.rndsystems.com/products/human-vitamin-d-bp-quantikine-elisa-kit_dvdbp0b (accessed on 22 August 2023).
- Prytuła, A.; Wells, D.; McLean, T.; Balona, F.; Gullett, A.; Knott, C.; Cantwell, M.; Hassen, K.; Ledermann, S.; Rees, L.; et al. Urinary and dialysate losses of vitamin D-binding protein in children on chronic peritoneal dialysis. Pediatr. Nephrol. 2012, 27, 643–649. [Google Scholar] [CrossRef]
- Sauriasari, R.; Safitri, D.D.; Azmi, N.U. Current updates on protein as biomarkers for diabetic kidney disease: A systematic review. Ther. Adv. Endocrinol. Metab. 2021, 12, 20420188211049612. [Google Scholar] [CrossRef]
- Nielsen, R.; Christensen, E.I.; Birn, H. Megalin and cubilin in proximal tubule protein reabsorption: From experimental models to human disease. Kidney Int. 2016, 89, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Lögdberg, L.; Wester, L. Immunocalins: A lipocalin subfamily that modulates immune and inflammatory responses. Biochim. Biophys. Acta 2000, 1482, 284–297. [Google Scholar] [CrossRef] [PubMed]
- Herget-Rosenthal, S.; van Wijk, J.A.; Bröcker-Preuss, M.; Bökenkamp, A. Increased urinary cystatin C reflects structural and functional renal tubular impairment independent of glomerular filtration rate. Clin. Biochem. 2007, 40, 946–951. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Evaluation of the Linearity of Quantitative Measurement Procedures: A Statistical Approach; Approved Guideline; CLSI document EP06-A; CLSI: Wayne, PA, USA, 2003. [Google Scholar]
- CLSI. Evaluation of Detection Capability for Clinical Laboratory Measurement Procedures; Approved Guideline—Second Edition; CLSI document EP17-A2; CLSI: Wayne, PA, USA, 2012. [Google Scholar]
- CLSI. Preliminary Evaluation of Quantitative Clinical Laboratory Measurement Procedures; Approved Guideline—Third Edition; CLSI document EP10-A3-AMD; CLSI: Wayne, PA, USA, 2014. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imprecision Data for the u-Gc Method | |||
|---|---|---|---|
| u-Gc Intra-assay Imprecision | |||
| u-Gc target ng/mL (n = 25) | u-Gc obtained ng/mL (n = 25) | SD | CV% |
| 7.81 | 8.08 | 1.08 | 13.33 |
| 31.25 | 31.16 | 2.55 | 8.20 |
| u-Gc Inter-assay Imprecision | |||
| u-Gc target ng/mL (n = 80) | u-Gc obtained ng/mL (n = 80) | SD | CV% |
| 7.81 | 7.60 | 1.54 | 20.30 |
| 31.25 | 31.29 | 3.82 | 12.21 |
| Control (n = 23) | Sepsis (n = 13) | Sepsis + AKI (n = 28) | p Value | |
|---|---|---|---|---|
| Age (years) | 52 (48–56) | 72 (58–80) | 67 (59–70) | <0.05 a,b |
| Males, n (%) | 13 (56.5) | 7 (53.8) | 20 (71.4) | n.s. |
| Major Comorbidities, n (%) | ||||
| Cardiovascular disease | 10 (43.5) | 12 (92.3) | 21 (75.0) | <0.05 a,b |
| Type-2 diabetes mellitus | 5 (21.7) | 3 (23.1) | 8 (28.6) | n.s. |
| Chronic kidney disease | 0 | 3 (23.1) | 4 (14.3) | <0.05 a |
| Pulmonary disease | 2 (8.7) | 1 (7.7) | 6 (21.4) | n.s. |
| Immunological disease | 1 (4.3) | 1 (7.7) | 1 (3.6) | n.s. |
| Malignancy | 0 | 3 (23.1) | 10 (35.7) | <0.05 a,b |
| Admission Laboratory Data | ||||
| se-TP (g/L) | 76.1 (72.2–77.7) | 41.6 (38.6–46.9) | 48.7 (42.5–51.1) | <0.05 a,b,c |
| se-albumin (g/L) | 49.2 (46.9–51.1) | 22.2 (18.9–26.4) | 23.6 (19.6–28.4) | <0.05 a,b |
| se-creatinine (µmol/L) | 76 (70–86) | 87 (64–136) | 181 (146–297) | <0.05 b,c |
| WBC (G/L) | 7.2 (6.4–7.9) | 13.8 (9.8–20.5) | 17.1 (12.6–20.6) | <0.05 a,b |
| PLT (G/L) | 262 (249–300) | 223 (133–306) | 218 (140–321) | n.s. |
| hs-CRP (mg/L) | 1.3 (0.6–2.5) | 295.4 (189–367) | 281.3 (167–390) | <0.05 a,b |
| PCT (ng/mL) | - | 7.9 (2.4–23.4) | 11.6 (6.2–60.4) | n.s. |
| se-GSN (mg/L) | 78.5 (75.1–89.1) | 11.2 (6.5–25.2) | 14.5 (6.1–21.1) | <0.05 a,b |
| se-Gc (mg/L) | 403.2 (369–418) | 221.2 (205–251) | 239.6 (178–279) | <0.05 a,b |
| u-TP (mg/L) | 60 (50–80) | 120 (40–425) | 270 (145–478) | <0.05 b |
| u-albumin (mg/L) | 4.7 (2.0–7.1) | 8.1 (1.9–21.2) | 38.8 (26.3–87.6) | <0.05 b,c |
| u-ORM (mg/L) | 0.9 (0.5–2.1) | 31.9 (13.5–62.7) | 31.5 (21.6–84.4) | <0.05 a,b |
| u-ORM/u-creatinine (mg/mmol) | 0.1 (0.05–0.17) | 15.1 (10.9–22.2) | 16.7 (11.3–24.2) | <0.05 a,b |
| u-Cystatin C (mg/L) | 0.06 (0.05–0.1) | 0.53 (0.1–1.1) | 1.17 (0.2–5.5) | <0.05 a,b |
| u-Cystatin C/u-creatinine (mg/mmol) | 0.006 (0.005–0.01) | 0.19 (0.04–0.43) | 0.39 (0.09–3.17) | <0.05 a,b |
| u-Gc (ng/mL) | 4.7 (0.1–32.5) | 61.3 (22–257) | 349.8 (106–1041) | <0.05 a,b,c |
| u-Gc/u-creatinine (µg/mmol) | 0.5 (0.1–2.8) | 23.6 (14.4–63.1) | 136.5 (39.9–379.1) | <0.05 a,b,c |
| Sepsis (n = 13) | Sepsis + AKI (n = 28) | p Value | |
|---|---|---|---|
| Age (years) | 72 (58–80) | 67 (59–70) | n.s. |
| Males, n (%) | 7 (53.8) | 20 (71.4) | n.s. |
| Cause of Admission | |||
| Internal medicine origin, n (%) | 2 (15.4) | 12 (42.9) | n.s. |
| Surgical origin, n (%) | 11 (84.6) | 16 (57.1) | n.s. |
| ICU treatment days | 9 (3–17) | 11 (4–17) | n.s. |
| 14-day mortality, death (%) | 5 (38.5) | 13 (46.4) | n.s. |
| AKI requiring RRT, n (%) | - | 12 (42.9) | - |
| Organ Dysfunctions, n (%) | |||
| 1 | 4 (30.7) | 3 (10.7) | n.s. |
| 2 | 3 (23.1) | 7 (25.0) | n.s. |
| ≥3 | 6 (46.2) | 18 (64.3) | n.s. |
| Clinical Prognostic Scores | |||
| APACHE II score | 15 (11–19) | 23 (18–27) | <0.05 |
| SAPS II score | 42 (35–46) | 53 (40–59) | <0.05 |
| SOFA score | 9 (7–11) | 11 (9–13) | n.s. |
| Identified Pathogens, n (%) | |||
| Unidentified | 4 (30.7) | 9 (32.1) | n.s. |
| Gram-positive bacteria | 1 (7.7) | 4 (14.3) | n.s. |
| Gram-negative bacteria | 3 (23.2) | 5 (17.9) | n.s. |
| Fungi | 1 (7.7) | 2 (7.1) | n.s. |
| Mixed | 4 (30.7) | 8 (28.6) | n.s. |
| U-Gc/u-Creatinine (µg/mmol)—Correlations (Spearman) | |
|---|---|
| Parameter | Correlation Coefficient |
| u-Gc-globulin (ng/mL) | 0.923 (p < 0.001) |
| se-creatinine (µmol/L) | 0.466 (p < 0.001) |
| se-urea (mmol/L) | 0.399 (p < 0.001) |
| se-hs-CRP (mg/L) | 0.407 (p < 0.001) |
| White Blood Cell count (G/L) | 0.376 (p < 0.001) |
| se-total protein (g/L) | −0.402 (p < 0.001) |
| se-albumin (g/L) | −0.427 (p < 0.001) |
| se-gelsolin (mg/L) | −0.390 (p < 0.001) |
| se-Gc-globulin (mg/L) | −0.250 (p < 0.01) |
| u-total protein (mg/L) | 0.563 (p < 0.001) |
| u-albumin (mg/L) | 0.696 (p < 0.001) |
| u-ORM (mg/L) | 0.415 (p < 0.001) |
| u-ORM/u-creatinine (mg/mmol) | 0.608 (p < 0.001) |
| u-Cystatin C (mg/L) | 0.624 (p < 0.001) |
| u-Cystatin C/u-creatinine (mg/mmol) | 0.722 (p < 0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kőszegi, T.; Horváth-Szalai, Z.; Ragán, D.; Kósa, B.; Szirmay, B.; Kurdi, C.; Kovács, G.L.; Mühl, D. Measurement of Urinary Gc-Globulin by a Fluorescence ELISA Technique: Method Validation and Clinical Evaluation in Septic Patients—A Pilot Study. Molecules 2023, 28, 6864. https://doi.org/10.3390/molecules28196864
Kőszegi T, Horváth-Szalai Z, Ragán D, Kósa B, Szirmay B, Kurdi C, Kovács GL, Mühl D. Measurement of Urinary Gc-Globulin by a Fluorescence ELISA Technique: Method Validation and Clinical Evaluation in Septic Patients—A Pilot Study. Molecules. 2023; 28(19):6864. https://doi.org/10.3390/molecules28196864
Chicago/Turabian StyleKőszegi, Tamás, Zoltán Horváth-Szalai, Dániel Ragán, Brigitta Kósa, Balázs Szirmay, Csilla Kurdi, Gábor L. Kovács, and Diána Mühl. 2023. "Measurement of Urinary Gc-Globulin by a Fluorescence ELISA Technique: Method Validation and Clinical Evaluation in Septic Patients—A Pilot Study" Molecules 28, no. 19: 6864. https://doi.org/10.3390/molecules28196864
APA StyleKőszegi, T., Horváth-Szalai, Z., Ragán, D., Kósa, B., Szirmay, B., Kurdi, C., Kovács, G. L., & Mühl, D. (2023). Measurement of Urinary Gc-Globulin by a Fluorescence ELISA Technique: Method Validation and Clinical Evaluation in Septic Patients—A Pilot Study. Molecules, 28(19), 6864. https://doi.org/10.3390/molecules28196864