
Advances in Nanoparticles in the Prevention and Treatment of Myocardial Infarction

Abstract
:1. Introduction
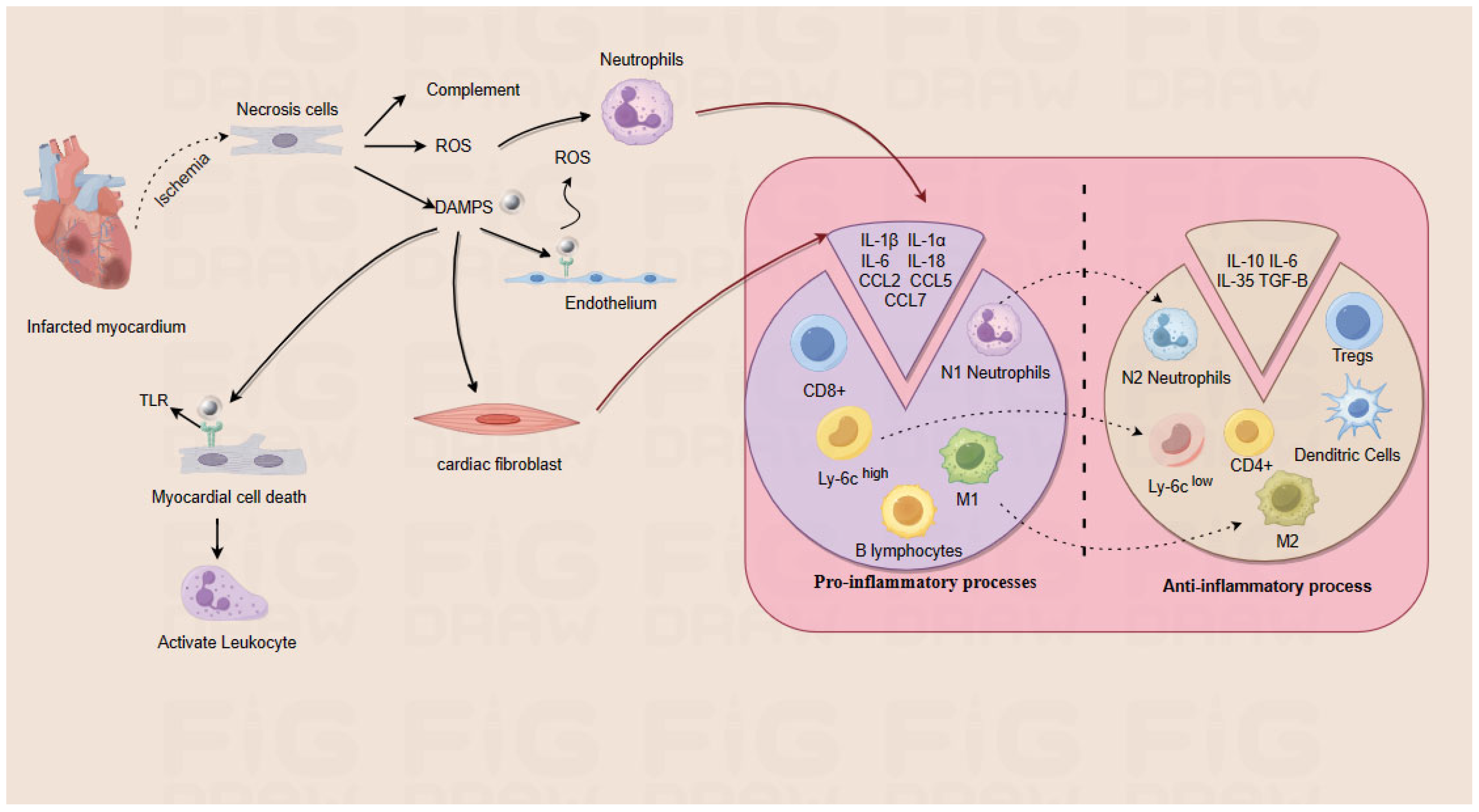
2. Pathologic Mechanisms of MI
2.1. Pathophysiology of MI
2.2. Heart Repair in MI
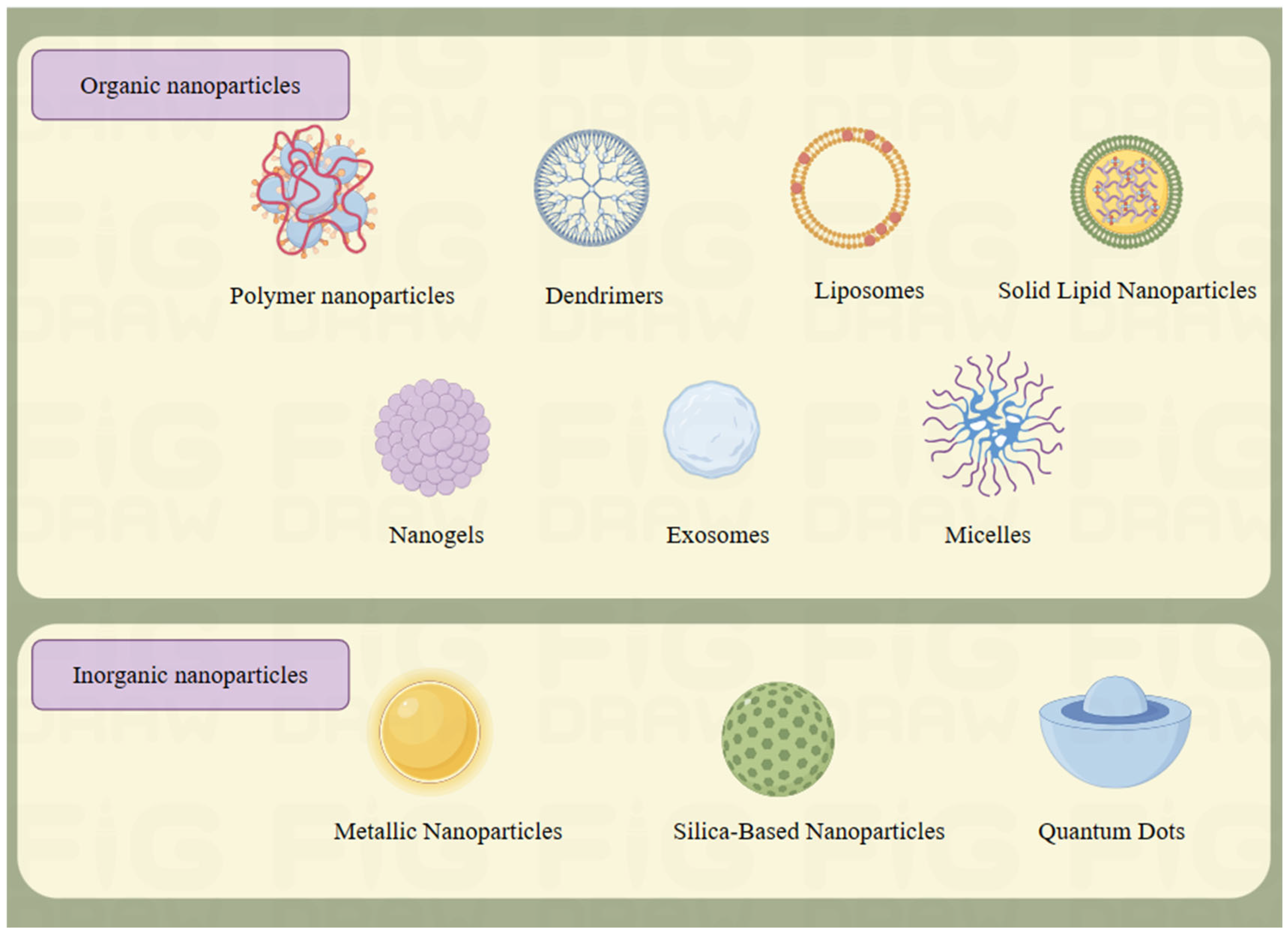
3. Types and Properties of Nanoparticles
3.1. Organic Nanoparticles
3.1.1. Polymer Nanoparticles
3.1.2. Dendrimers
3.1.3. Micelles
3.1.4. Nanogels
3.1.5. Liposomes
3.1.6. Solid Lipid Nanoparticles
3.1.7. Exosome
3.2. Inorganic Nanoparticles
3.2.1. Metal Nanoparticles
3.2.2. Silica Nanoparticle
3.2.3. Quantum Dots
4. Nanoparticles for MI Prevention

{kind=link}
{kind=link}
| Types of Nanoparticles | Payload | Target | Animal Model | Outcomes | Ref. |
|---|---|---|---|---|---|
| PLGA nanoparticles | siCamk2g | Macrophages | LDLR−/−mice | Necrotic core area decreased, fibrous cap thickness increased, and plaque stability increased | [95] |
| Macrophage membrane-coated PLGA nanoparticles | Rapamycin | AS plaque | ApoE−/−mice | Plaque lipids were reduced and necrotic core area was reduced | [96] |
| Macrophage membrane-coated nanoparticles | Atorvastatin | ROS | ApoE−/−mice | Plaque area and necrotic core area were significantly reduced | [97] |
| PLGA nanoparticles | Colchicine | AS plaque | ApoE−/−mice | Plaque lipid deposition was reduced and plaque area was reduced | [98] |
| Lipid nanoparticles | Apolipoprotein A-I | AS plaque | LDLR−/−mice | Inhibits the inflammatory response of macrophages, inhibits AS, and stabilizes AS plaques | [99] |
| Erythrocyte membrane-coated stellate polymers | Probucol | ROS | ApoE−/−mice | The formation of foam cells was inhibited and the plaque area was reduced | [100] |
| Mannose-modified dendritic nanoparticles | SR-A siRNA and LXR ligands | Macrophages | LDLR−/−mice | Plaque area was reduced and aortic cholesterol content was reduced | [101] |
| Hyaluronic acid-modified liposomes | Rosuvastatin | AS plaque | ApoE−/−mice | The levels of proinflammatory factors and foam cells were reduced, and plaque area was reduced | [102] |
| Micellar nanoparticles | microRNA-145 | Vascular smooth muscle cells | ApoE−/−mice | Plaque size and overall lesion area were reduced | [103] |
| Macrophage membrane-coated nanoparticles | Methotrexate | AS plaque | ApoE−/−mice | Plaque area and plaque lipid deposition were reduced | [104] |
5. Treatment of MI Nanoparticles
5.1. Nanoparticles for Regulating Cardiac Homeostasis
5.2. Nanoparticles to Promote the Regeneration of Damaged Hearts
6. Conclusions and Prospects
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Salari, N.; Morddarvanjoghi, F.; Abdolmaleki, A.; Rasoulpoor, S.; Khaleghi, A.A.; Hezarkhani, L.A.; Shohaimi, S.; Mohammadi, M. The global prevalence of myocardial infarction: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2023, 23, 206. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Liu, Y.; Yang, J.; Zhai, M.; Fan, Z.; Qiao, R.; Jin, P.; Yang, L. Effects of berbamine against myocardial ischemia/reperfusion injury: Activation of the 5′ adenosine monophosphate-activated protein kinase/nuclear factor erythroid 2-related factor pathway and changes in the mitochondrial state. Biofactors 2022, 48, 651–664. [Google Scholar] [CrossRef] [PubMed]
- George, T.A.; Hsu, C.C.; Meeson, A.; Lundy, D.J. Nanocarrier-Based Targeted Therapies for Myocardial Infarction. Pharmaceutics 2022, 14, 930. [Google Scholar] [CrossRef] [PubMed]
- Sagris, M.; Apostolos, A.; Theofilis, P.; Ktenopoulos, N.; Katsaros, O.; Tsalamandris, S.; Tsioufis, K.; Toutouzas, K.; Tousoulis, D. Myocardial Ischemia-Reperfusion Injury: Unraveling Pathophysiology, Clinical Manifestations, and Emerging Prevention Strategies. Biomedicines 2024, 12, 802. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G. Myocardial ischemia/reperfusion: Translational pathophysiology of ischemic heart disease. Med 2024, 5, 10–31. [Google Scholar] [CrossRef]
- Li, H.; Zheng, F.; Zhang, Y.; Sun, J.; Gao, F.; Shi, G. Resveratrol, novel application by preconditioning to attenuate myocardial ischemia/reperfusion injury in mice through regulate AMPK pathway and autophagy level. J. Cell. Mol. Med. 2022, 26, 4216–4229. [Google Scholar] [CrossRef]
- Li, S.; Li, F.; Wang, Y.; Li, W.; Wu, J.; Hu, X.; Tang, T.; Liu, X. Multiple delivery strategies of nanocarriers for myocardial ischemia-reperfusion injury: Current strategies and future prospective. Drug Deliv. 2024, 31, 2298514. [Google Scholar] [CrossRef] [PubMed]
- Stater, E.P.; Sonay, A.Y.; Hart, C.; Grimm, J. The ancillary effects of nanoparticles and their implications for nanomedicine. Nat. Nanotechnol. 2021, 16, 1180–1194. [Google Scholar] [CrossRef]
- Yuan, Z.; Yuan, Y.; Han, L.; Qiu, Y.; Huang, X.; Gao, F.; Fan, G.; Zhang, Y.; Tang, X.; He, X.; et al. Bufalin-loaded vitamin E succinate-grafted-chitosan oligosaccharide/RGD conjugated TPGS mixed micelles demonstrated improved antitumor activity against drug-resistant colon cancer. Int. J. Nanomed. 2018, 13, 7533–7548. [Google Scholar] [CrossRef]
- de Lemos, J.A.; Newby, L.K.; Mills, N.L. A Proposal for Modest Revision of the Definition of Type 1 and Type 2 Myocardial Infarction. Circulation 2019, 140, 1773–1775. [Google Scholar] [CrossRef]
- Fang, M.; Li, Y.; Wu, Y.; Ning, Z.; Wang, X.; Li, X. miR-185 silencing promotes the progression of atherosclerosis via targeting stromal interaction molecule 1. Cell Cycle 2019, 18, 682–695. [Google Scholar] [CrossRef]
- Kleinbongard, P.; Heusch, G. A fresh look at coronary microembolization. Nat. Rev. Cardiol. 2022, 19, 265–280. [Google Scholar] [CrossRef]
- Zeng, Z.; Xie, Y.; Li, L.; Wang, H.; Tan, J.; Li, X.; Bian, Q.; Zhang, Y.; Liu, T.; Weng, Y.; et al. Reducing Endogenous Labile Zn May Help to Reduce Smooth Muscle Cell Injury around Vascular Stents. Int. J. Mol. Sci. 2022, 23, 5139. [Google Scholar] [CrossRef]
- Layland, J.; Oldroyd, K.G.; Curzen, N.; Sood, A.; Balachandran, K.; Das, R.; Junejo, S.; Ahmed, N.; Lee, M.M.; Shaukat, A.; et al. Fractional flow reserve vs. angiography in guiding management to optimize outcomes in non-ST-segment elevation myocardial infarction: The British Heart Foundation FAMOUS-NSTEMI randomized trial. Eur. Heart J. 2015, 36, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, E.; Yonetsu, T.; Kakuta, T.; Soeda, T.; Saito, Y.; Yan, B.P.; Kurihara, O.; Takano, M.; Niccoli, G.; Higuma, T.; et al. Clinical and Laboratory Predictors for Plaque Erosion in Patients With Acute Coronary Syndromes. J. Am. Heart Assoc. 2019, 8, e012322. [Google Scholar] [CrossRef]
- Heusch, G. Myocardial ischaemia-reperfusion injury and cardioprotection in perspective. Nat. Rev. Cardiol. 2020, 17, 773–789. [Google Scholar] [CrossRef] [PubMed]
- Krasowska, D.; Gerkowicz, A.; Wroblewska-Luczka, P.; Grabarska, A.; Zaluska-Ogryzek, K.; Krasowska, D.; Luszczki, J.J. Anticancer Activity of Amantadine and Evaluation of Its Interactions with Selected Cytostatics in Relation to Human Melanoma Cells. Int. J. Mol. Sci. 2022, 23, 7653. [Google Scholar] [CrossRef]
- George, B.P.; Abrahamse, H. Increased Oxidative Stress Induced by Rubus Bioactive Compounds Induce Apoptotic Cell Death in Human Breast Cancer Cells. Oxid. Med. Cell. Longev. 2019, 2019, 6797921. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.D.; Yang, Y.J.; Liu, X.W.; Qin, Z.; Li, S.H.; Li, J.Y. The Protective Effect of Aspirin Eugenol Ester on Paraquat-Induced Acute Liver Injury Rats. Front. Med. 2020, 7, 589011. [Google Scholar] [CrossRef]
- Song, Z.; Song, H.; Liu, D.; Yan, B.; Wang, D.; Zhang, Y.; Zhao, X.; Tian, X.; Yan, C.; Han, Y. Overexpression of MFN2 alleviates sorafenib-induced cardiomyocyte necroptosis via the MAM-CaMKIIdelta pathway in vitro and in vivo. Theranostics 2022, 12, 1267–1285. [Google Scholar] [CrossRef]
- Wisowski, G.; Pudelko, A.; Olczyk, K.; Paul-Samojedny, M.; Kozma, E.M. Dermatan Sulfate Affects Breast Cancer Cell Function via the Induction of Necroptosis. Cells 2022, 11, 173. [Google Scholar] [CrossRef]
- Li, Z.; Jia, Y.; Feng, Y.; Cui, R.; Miao, R.; Zhang, X.; Qu, K.; Liu, C.; Zhang, J. Methane alleviates sepsis-induced injury by inhibiting pyroptosis and apoptosis: In vivo and in vitro experiments. Aging 2019, 11, 1226–1239. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Wang, X.; Hu, H.; Xu, Z.; Zhang, J.; An, G.; Su, G. Intracoronary application of nicorandil regulates the inflammatory response induced by percutaneous coronary intervention. J. Cell. Mol. Med. 2020, 24, 4863–4870. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Hu, S.; Jin, Q.; Shi, C.; Zhang, Y.; Zhu, P.; Ma, Q.; Tian, F.; Chen, Y. Mff-Dependent Mitochondrial Fission Contributes to the Pathogenesis of Cardiac Microvasculature Ischemia/Reperfusion Injury via Induction of mROS-Mediated Cardiolipin Oxidation and HK2/VDAC1 Disassociation-Involved mPTP Opening. J. Am. Heart Assoc. 2017, 6, e005328. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Xu, J.; Wu, M.; Kang, L.; Xu, B. The effector cells and cellular mediators of immune system involved in cardiac inflammation and fibrosis after myocardial infarction. J. Cell. Physiol. 2020, 235, 8996–9004. [Google Scholar] [CrossRef]
- Frangogiannis, N.G. The inflammatory response in myocardial injury, repair, and remodelling. Nat. Rev. Cardiol. 2014, 11, 255–265. [Google Scholar] [CrossRef]
- Prabhu, S.D.; Frangogiannis, N.G. The Biological Basis for Cardiac Repair After Myocardial Infarction: From Inflammation to Fibrosis. Circ. Res. 2016, 119, 91–112. [Google Scholar] [CrossRef]
- McElhinney, K.; Irnaten, M.; O’Brien, C. p53 and Myofibroblast Apoptosis in Organ Fibrosis. Int. J. Mol. Sci. 2023, 24, 6737. [Google Scholar] [CrossRef]
- Frangogiannis, N.G. Pathophysiology of Myocardial Infarction. Compr. Physiol. 2015, 5, 1841–1875. [Google Scholar] [CrossRef]
- Katsuki, S.; Matoba, T.; Nakashiro, S.; Sato, K.; Koga, J.; Nakano, K.; Nakano, Y.; Egusa, S.; Sunagawa, K.; Egashira, K. Nanoparticle-mediated delivery of pitavastatin inhibits atherosclerotic plaque destabilization/rupture in mice by regulating the recruitment of inflammatory monocytes. Circulation 2014, 129, 896–906. [Google Scholar] [CrossRef]
- Shastri, V.P. Non-degradable biocompatible polymers in medicine: Past, present and future. Curr. Pharm. Biotechnol. 2003, 4, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Liu, Y.; Weigmann, B. Biodegradable Polymeric Nanoparticles Loaded with Flavonoids: A Promising Therapy for Inflammatory Bowel Disease. Int. J. Mol. Sci. 2023, 24, 4454. [Google Scholar] [CrossRef]
- Kucuk, N.; Primozic, M.; Knez, Z.; Leitgeb, M. Sustainable Biodegradable Biopolymer-Based Nanoparticles for Healthcare Applications. Int. J. Mol. Sci. 2023, 24, 3188. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.H.; Lu, A.; Chen, X.; Yang, Z. Natural Ingredient-Based Polymeric Nanoparticles for Cancer Treatment. Molecules 2020, 25, 3620. [Google Scholar] [CrossRef]
- George, A.; Shah, P.A.; Shrivastav, P.S. Natural biodegradable polymers based nano-formulations for drug delivery: A review. Int. J. Pharm. 2019, 561, 244–264. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, G.; Matoba, T.; Ishikita, A.; Nagaoka, K.; Nakano, K.; Koga, J.I.; Tsutsui, H.; Egashira, K. Nanoparticle-Mediated Simultaneous Targeting of Mitochondrial Injury and Inflammation Attenuates Myocardial Ischemia-Reperfusion Injury. J. Am. Heart Assoc. 2021, 10, e019521. [Google Scholar] [CrossRef] [PubMed]
- Janaszewska, A.; Lazniewska, J.; Trzepinski, P.; Marcinkowska, M.; Klajnert-Maculewicz, B. Cytotoxicity of Dendrimers. Biomolecules 2019, 9, 330. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.P.; da Silva Santos, S.; da Silva, J.V.; Parise-Filho, R.; Igne Ferreira, E.; Seoud, O.E.; Giarolla, J. Dendrimers in the context of nanomedicine. Int. J. Pharm. 2020, 573, 118814. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, A.S. Dendrimers for Drug Delivery. Molecules 2018, 23, 938. [Google Scholar] [CrossRef]
- Chis, A.A.; Dobrea, C.; Morgovan, C.; Arseniu, A.M.; Rus, L.L.; Butuca, A.; Juncan, A.M.; Totan, M.; Vonica-Tincu, A.L.; Cormos, G.; et al. Applications and Limitations of Dendrimers in Biomedicine. Molecules 2020, 25, 3982. [Google Scholar] [CrossRef]
- Zenze, M.; Daniels, A.; Singh, M. Dendrimers as Modifiers of Inorganic Nanoparticles for Therapeutic Delivery in Cancer. Pharmaceutics 2023, 15, 398. [Google Scholar] [CrossRef]
- Xue, X.; Shi, X.; Dong, H.; You, S.; Cao, H.; Wang, K.; Wen, Y.; Shi, D.; He, B.; Li, Y. Delivery of microRNA-1 inhibitor by dendrimer-based nanovector: An early targeting therapy for myocardial infarction in mice. Nanomedicine 2018, 14, 619–631. [Google Scholar] [CrossRef]
- Parra, A.; Jarak, I.; Santos, A.; Veiga, F.; Figueiras, A. Polymeric Micelles: A Promising Pathway for Dermal Drug Delivery. Materials 2021, 14, 7278. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Z.; Shah, A.; Siddiq, M.; Kraatz, H.-B. Polymeric micelles as drug delivery vehicles. RSC Adv. 2014, 4, 17028–17038. [Google Scholar] [CrossRef]
- Lu, Y.; Park, K. Polymeric micelles and alternative nanonized delivery vehicles for poorly soluble drugs. Int. J. Pharm. 2013, 453, 198–214. [Google Scholar] [CrossRef]
- Kotta, S.; Aldawsari, H.M.; Badr-Eldin, S.M.; Nair, A.B.; Yt, K. Progress in Polymeric Micelles for Drug Delivery Applications. Pharmaceutics 2022, 14, 1636. [Google Scholar] [CrossRef]
- Tesoro, L.; Hernandez, I.; Ramirez-Carracedo, R.; Diez-Mata, J.; Alcharani, N.; Jimenez-Guirado, B.; Ovejero-Paredes, K.; Filice, M.; Zamorano, J.L.; Saura, M.; et al. NIL10: A New IL10-Receptor Binding Nanoparticle That Induces Cardiac Protection in Mice and Pigs Subjected to Acute Myocardial Infarction through STAT3/NF-kappaB Activation. Pharmaceutics 2022, 14, 2044. [Google Scholar] [CrossRef]
- Kaewruethai, T.; Laomeephol, C.; Pan, Y.; Luckanagul, J.A. Multifunctional Polymeric Nanogels for Biomedical Applications. Gels 2021, 7, 228. [Google Scholar] [CrossRef]
- Manimaran, V.; Nivetha, R.P.; Tamilanban, T.; Narayanan, J.; Vetriselvan, S.; Fuloria, N.K.; Chinni, S.V.; Sekar, M.; Fuloria, S.; Wong, L.S.; et al. Nanogels as novel drug nanocarriers for CNS drug delivery. Front. Mol. Biosci. 2023, 10, 1232109. [Google Scholar] [CrossRef]
- Bhattarai, N.; Gunn, J.; Zhang, M. Chitosan-based hydrogels for controlled, localized drug delivery. Adv. Drug Deliv. Rev. 2010, 62, 83–99. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, W.; Zhao, X.; Xian, Y.; Wu, W.; Zhang, X.; Zhao, N.; Xu, F.J.; Wang, C. Natural Melanin/Alginate Hydrogels Achieve Cardiac Repair through ROS Scavenging and Macrophage Polarization. Adv. Sci. 2021, 8, e2100505. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Obireddy, S.R.; Lai, W.F. Preparation and use of nanogels as carriers of drugs. Drug Deliv. 2021, 28, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Chen, G.; Zhang, J. A Review of Liposomes as a Drug Delivery System: Current Status of Approved Products, Regulatory Environments, and Future Perspectives. Molecules 2022, 27, 1372. [Google Scholar] [CrossRef] [PubMed]
- Bozzuto, G.; Molinari, A. Liposomes as nanomedical devices. Int. J. Nanomed. 2015, 10, 975–999. [Google Scholar] [CrossRef] [PubMed]
- Patil, Y.P.; Jadhav, S. Novel methods for liposome preparation. Chem. Phys. Lipids 2014, 177, 8–18. [Google Scholar] [CrossRef]
- Xing, H.; Hwang, K.; Lu, Y. Recent Developments of Liposomes as Nanocarriers for Theranostic Applications. Theranostics 2016, 6, 1336–1352. [Google Scholar] [CrossRef] [PubMed]
- Scalzo, S.; Santos, A.K.; Ferreira, H.A.S.; Costa, P.A.; Prazeres, P.; da Silva, N.J.A.; Guimaraes, L.C.; e Silva, M.D.M.; Rodrigues Alves, M.T.R.; Viana, C.T.R.; et al. Ionizable Lipid Nanoparticle-Mediated Delivery of Plasmid DNA in Cardiomyocytes. Int. J. NanoMed. 2022, 17, 2865–2881. [Google Scholar] [CrossRef]
- Fulton, M.D.; Najahi-Missaoui, W. Liposomes in Cancer Therapy: How Did We Start and Where Are We Now. Int. J. Mol. Sci. 2023, 24, 6615. [Google Scholar] [CrossRef] [PubMed]
- Almeida, B.; Nag, O.K.; Rogers, K.E.; Delehanty, J.B. Recent Progress in Bioconjugation Strategies for Liposome-Mediated Drug Delivery. Molecules 2020, 25, 5672. [Google Scholar] [CrossRef]
- Subroto, E.; Andoyo, R.; Indiarto, R. Solid Lipid Nanoparticles: Review of the Current Research on Encapsulation and Delivery Systems for Active and Antioxidant Compounds. Antioxidants 2023, 12, 633. [Google Scholar] [CrossRef]
- Viegas, C.; Patricio, A.B.; Prata, J.M.; Nadhman, A.; Chintamaneni, P.K.; Fonte, P. Solid Lipid Nanoparticles vs. Nanostructured Lipid Carriers: A Comparative Review. Pharmaceutics 2023, 15, 1593. [Google Scholar] [CrossRef] [PubMed]
- Madkhali, O.A. Perspectives and Prospective on Solid Lipid Nanoparticles as Drug Delivery Systems. Molecules 2022, 27, 1543. [Google Scholar] [CrossRef] [PubMed]
- Mishra, V.; Bansal, K.K.; Verma, A.; Yadav, N.; Thakur, S.; Sudhakar, K.; Rosenholm, J.M. Solid Lipid Nanoparticles: Emerging Colloidal Nano Drug Delivery Systems. Pharmaceutics 2018, 10, 191. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Xing, X.; Lv, N.; Zhao, J.; Liu, Y.; Gong, H.; Du, Y.; Lu, Q.; Dong, Z. Therapy for myocardial infarction: In vitro and in vivo evaluation of puerarin-prodrug and tanshinone co-loaded lipid nanoparticulate system. Biomed. Pharmacother. 2019, 120, 109480. [Google Scholar] [CrossRef] [PubMed]
- German-Cortes, J.; Vilar-Hernandez, M.; Rafael, D.; Abasolo, I.; Andrade, F. Solid Lipid Nanoparticles: Multitasking Nano-Carriers for Cancer Treatment. Pharmaceutics 2023, 15, 831. [Google Scholar] [CrossRef] [PubMed]
- Kalluri, R.; LeBleu, V.S. The biology, function, and biomedical applications of exosomes. Science 2020, 367, eaau6977. [Google Scholar] [CrossRef]
- Wang, S.; Shi, Y. Exosomes Derived from Immune Cells: The New Role of Tumor Immune Microenvironment and Tumor Therapy. Int. J. Nanomed. 2022, 17, 6527–6550. [Google Scholar] [CrossRef] [PubMed]
- Kok, V.C.; Yu, C.C. Cancer-Derived Exosomes: Their Role in Cancer Biology and Biomarker Development. Int. J. Nanomed. 2020, 15, 8019–8036. [Google Scholar] [CrossRef]
- Song, J.; Chen, X.; Wang, M.; Xing, Y.; Zheng, Z.; Hu, S. Cardiac endothelial cell-derived exosomes induce specific regulatory B cells. Sci. Rep. 2014, 4, 7583. [Google Scholar] [CrossRef]
- Lou, G.; Chen, Z.; Zheng, M.; Liu, Y. Mesenchymal stem cell-derived exosomes as a new therapeutic strategy for liver diseases. Exp. Mol. Med. 2017, 49, e346. [Google Scholar] [CrossRef]
- He, C.; Zheng, S.; Luo, Y.; Wang, B. Exosome Theranostics: Biology and Translational Medicine. Theranostics 2018, 8, 237–255. [Google Scholar] [CrossRef] [PubMed]
- Amiri, A.; Bagherifar, R.; Ansari Dezfouli, E.; Kiaie, S.H.; Jafari, R.; Ramezani, R. Exosomes as bio-inspired nanocarriers for RNA delivery: Preparation and applications. J. Transl. Med. 2022, 20, 125. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.; Wang, Y.; Thomas, M.; McLaughlin, K.; Oguljahan, B.; Henderson, J.; Yang, Q.; Chen, Y.E.; Liu, D. Exosomes from adipose-derived stem cells alleviate myocardial infarction via microRNA-31/FIH1/HIF-1alpha pathway. J. Mol. Cell. Cardiol. 2022, 162, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Zhang, Y.; Chen, D.; Zheng, Y.; Jiang, J. Exosomes and Exosomal Cargos: A Promising World for Ventricular Remodeling Following Myocardial Infarction. Int. J. Nanomed. 2022, 17, 4699–4719. [Google Scholar] [CrossRef]
- Shi, Y.; Qiu, B.; Huang, L.; Li, Y.; Ze, Y.; Yao, Y. Exosomes in Liquid Biopsy: A Nanotool for Postradiotherapy Cancer Monitoring. Front. Biosci. 2022, 27, 205. [Google Scholar] [CrossRef]
- Batrakova, E.V.; Kim, M.S. Using exosomes, naturally-equipped nanocarriers, for drug delivery. J. Control. Release 2015, 219, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Alphandery, E. Natural Metallic Nanoparticles for Application in Nano-Oncology. Int. J. Mol. Sci. 2020, 21, 4412. [Google Scholar] [CrossRef] [PubMed]
- Abdal Dayem, A.; Hossain, M.K.; Lee, S.B.; Kim, K.; Saha, S.K.; Yang, G.M.; Choi, H.Y.; Cho, S.G. The Role of Reactive Oxygen Species (ROS) in the Biological Activities of Metallic Nanoparticles. Int. J. Mol. Sci. 2017, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Pavelic, K.; Kraljevic Pavelic, S.; Bulog, A.; Agaj, A.; Rojnic, B.; Colic, M.; Trivanovic, D. Nanoparticles in Medicine: Current Status in Cancer Treatment. Int. J. Mol. Sci. 2023, 24, 12827. [Google Scholar] [CrossRef]
- Arozal, W.; Monayo, E.R.; Barinda, A.J.; Perkasa, D.P.; Soetikno, V.; Nafrialdi, N.; Louisa, M. Protective effects of silver nanoparticles in isoproterenol-induced myocardial infarction in rats. Front. Med. 2022, 9, 867497. [Google Scholar] [CrossRef]
- Burlec, A.F.; Corciova, A.; Boev, M.; Batir-Marin, D.; Mircea, C.; Cioanca, O.; Danila, G.; Danila, M.; Bucur, A.F.; Hancianu, M. Current Overview of Metal Nanoparticles’ Synthesis, Characterization, and Biomedical Applications, with a Focus on Silver and Gold Nanoparticles. Pharmaceuticals 2023, 16, 1410. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, E.; Ansari, L.; Abnous, K.; Taghdisi, S.M.; Charbgoo, F.; Ramezani, M.; Alibolandi, M. Silica based hybrid materials for drug delivery and bioimaging. J. Control. Release 2018, 277, 57–76. [Google Scholar] [CrossRef] [PubMed]
- Nayl, A.A.; Abd-Elhamid, A.I.; Aly, A.A.; Brase, S. Recent progress in the applications of silica-based nanoparticles. RSC Adv. 2022, 12, 13706–13726. [Google Scholar] [CrossRef]
- Yu, H.; Li, Y.; Zhang, R.; Shen, M.; Zhu, Y.; Zhang, Q.; Liu, H.; Han, D.; Shi, X.; Zhang, J. Inhibition of cardiomyocyte apoptosis post-acute myocardial infarction through the efficient delivery of microRNA-24 by silica nanoparticles. Nanoscale Adv. 2021, 3, 6379–6385. [Google Scholar] [CrossRef] [PubMed]
- Tng, D.J.H.; Low, J.G.H. Current status of silica-based nanoparticles as therapeutics and its potential as therapies against viruses. Antiviral Res. 2023, 210, 105488. [Google Scholar] [CrossRef] [PubMed]
- Mattoussi, H.; Palui, G.; Na, H.B. Luminescent quantum dots as platforms for probing in vitro and in vivo biological processes. Adv. Drug Deliv. Rev. 2012, 64, 138–166. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.M.; Knipe, J.M.; Orive, G.; Peppas, N.A. Quantum dots in biomedical applications. Acta Biomater. 2019, 94, 44–63. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, T.; Bakhshi, R.; Petrova, D.; Pocock, R.; Imani, M.; Seifalian, A.M. Biological applications of quantum dots. Biomaterials 2007, 28, 4717–4732. [Google Scholar] [CrossRef] [PubMed]
- Dirheimer, L.; Pons, T.; Marchal, F.; Bezdetnaya, L. Quantum Dots Mediated Imaging and Phototherapy in Cancer Spheroid Models: State of the Art and Perspectives. Pharmaceutics 2022, 14, 2136. [Google Scholar] [CrossRef]
- Tabish, T.A.; Hayat, H.; Abbas, A.; Narayan, R.J. Graphene Quantum Dots-Based Electrochemical Biosensing Platform for Early Detection of Acute Myocardial Infarction. Biosensors 2022, 12, 77. [Google Scholar] [CrossRef]
- Bejarano, J.; Navarro-Marquez, M.; Morales-Zavala, F.; Morales, J.O.; Garcia-Carvajal, I.; Araya-Fuentes, E.; Flores, Y.; Verdejo, H.E.; Castro, P.F.; Lavandero, S.; et al. Nanoparticles for diagnosis and therapy of atherosclerosis and myocardial infarction: Evolution toward prospective theranostic approaches. Theranostics 2018, 8, 4710–4732. [Google Scholar] [CrossRef]
- Hetherington, I.; Totary-Jain, H. Anti-atherosclerotic therapies: Milestones, challenges, and emerging innovations. Mol. Ther. 2022, 30, 3106–3117. [Google Scholar] [CrossRef] [PubMed]
- Bai, Q.; Xiao, Y.; Hong, H.; Cao, X.; Zhang, L.; Han, R.; Lee, L.K.C.; Xue, E.Y.; Tian, X.Y.; Choi, C.H.J. Scavenger receptor-targeted plaque delivery of microRNA-coated nanoparticles for alleviating atherosclerosis. Proc. Natl. Acad. Sci. USA 2022, 119, e2201443119. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhang, W.; Zhou, X.; Xu, F.; Zou, J.; Zhang, Q.; Zhao, Y.; He, H.; Yang, H.; Liu, J. Reactive oxygen species (ROS)-responsive size-reducible nanoassemblies for deeper atherosclerotic plaque penetration and enhanced macrophage-targeted drug delivery. Bioact. Mater. 2023, 19, 115–126. [Google Scholar] [CrossRef]
- Tao, W.; Yurdagul, A., Jr.; Kong, N.; Li, W.; Wang, X.; Doran, A.C.; Feng, C.; Wang, J.; Islam, M.A.; Farokhzad, O.C.; et al. siRNA nanoparticles targeting CaMKIIgamma in lesional macrophages improve atherosclerotic plaque stability in mice. Sci. Transl. Med. 2020, 12, eaay1063. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, K.; Li, T.; Maruf, A.; Qin, X.; Luo, L.; Zhong, Y.; Qiu, J.; McGinty, S.; Pontrelli, G.; et al. Macrophage membrane functionalized biomimetic nanoparticles for targeted anti-atherosclerosis applications. Theranostics 2021, 11, 164–180. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Huang, Q.; Liu, C.; Kwong, C.H.T.; Yue, L.; Wan, J.B.; Lee, S.M.Y.; Wang, R. Treatment of atherosclerosis by macrophage-biomimetic nanoparticles via targeted pharmacotherapy and sequestration of proinflammatory cytokines. Nat. Commun. 2020, 11, 2622. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Li, T.; Xiong, X.; Yang, Q.; Su, Z.; Zheng, M.; Chen, Q. Colchicine delivered by a novel nanoparticle platform alleviates atherosclerosis by targeted inhibition of NF-kappaB/NLRP3 pathways in inflammatory endothelial cells. J. Nanobiotechnol. 2023, 21, 460. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Guo, Y.; Wang, H.; Yu, M.; Hong, K.; Li, D.; Li, R.; Wen, B.; Hu, D.; Chang, L.; et al. Phospholipid nanoparticles: Therapeutic potentials against atherosclerosis via reducing cholesterol crystals and inhibiting inflammation. eBioMedicine 2021, 74, 103725. [Google Scholar] [CrossRef]
- Liang, X.; Li, H.; Zhang, A.; Tian, X.; Guo, H.; Zhang, H.; Yang, J.; Zeng, Y. Red blood cell biomimetic nanoparticle with anti-inflammatory, anti-oxidative and hypolipidemia effect ameliorated atherosclerosis therapy. Nanomedicine 2022, 41, 102519. [Google Scholar] [CrossRef]
- He, H.; Wang, J.; Yannie, P.J.; Korzun, W.J.; Yang, H.; Ghosh, S. Nanoparticle-based “Two-pronged” approach to regress atherosclerosis by simultaneous modulation of cholesterol influx and efflux. Biomaterials 2020, 260, 120333. [Google Scholar] [CrossRef]
- Ma, Q.; Wu, S.; Yang, L.; Wei, Y.; He, C.; Wang, W.; Zhao, Y.; Wang, Z.; Yang, S.; Shi, D.; et al. Hyaluronic Acid-Guided Cerasome Nano-Agents for Simultaneous Imaging and Treatment of Advanced Atherosclerosis. Adv. Sci. 2023, 10, e2202416. [Google Scholar] [CrossRef]
- Chin, D.D.; Patel, N.; Lee, W.; Kanaya, S.; Cook, J.; Chung, E.J. Long-term, in vivo therapeutic effects of a single dose of miR-145 micelles for atherosclerosis. Bioact. Mater. 2023, 27, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Li, H.; Li, J.; Zhong, Y.; Wu, S.; Yan, M.; Ni, S.; Zhang, K.; Wang, G.; Qu, K.; et al. Biomimetic nanoparticles to enhance the reverse cholesterol transport for selectively inhibiting development into foam cell in atherosclerosis. J. Nanobiotechnol. 2023, 21, 307. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.B.; Hernandez-Resendiz, S.; Crespo-Avilan, G.E.; Mukhametshina, R.T.; Kwek, X.Y.; Cabrera-Fuentes, H.A.; Hausenloy, D.J. Inflammation following acute myocardial infarction: Multiple players, dynamic roles, and novel therapeutic opportunities. Pharmacol. Ther. 2018, 186, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Li, Y.Y.; Jin, J. A double-edged sword of immuno-microenvironment in cardiac homeostasis and injury repair. Signal Transduct. Target. Ther. 2021, 6, 79. [Google Scholar] [CrossRef] [PubMed]
- Ai, W.; Bae, S.; Ke, Q.; Su, S.; Li, R.; Chen, Y.; Yoo, D.; Lee, E.; Jon, S.; Kang, P.M. Bilirubin Nanoparticles Protect Against Cardiac Ischemia/Reperfusion Injury in Mice. J. Am. Heart Assoc. 2021, 10, e021212. [Google Scholar] [CrossRef] [PubMed]
- Maranhao, R.C.; Guido, M.C.; de Lima, A.D.; Tavares, E.R.; Marques, A.F.; Tavares de Melo, M.D.; Nicolau, J.C.; Salemi, V.M.; Kalil-Filho, R. Methotrexate carried in lipid core nanoparticles reduces myocardial infarction size and improves cardiac function in rats. Int. J. Nanomed. 2017, 12, 3767–3784. [Google Scholar] [CrossRef] [PubMed]
- Asanuma, H.; Sanada, S.; Yoshitomi, T.; Sasaki, H.; Takahama, H.; Ihara, M.; Takahama, H.; Shinozaki, Y.; Mori, H.; Asakura, M.; et al. Novel Synthesized Radical-Containing Nanoparticles Limit Infarct Size Following Ischemia and Reperfusion in Canine Hearts. Cardiovasc. Drugs Ther. 2017, 31, 501–510. [Google Scholar] [CrossRef]
- Shao, M.; Yang, W.; Han, G. Protective effects on myocardial infarction model: Delivery of schisandrin B using matrix metalloproteinase-sensitive peptide-modified, PEGylated lipid nanoparticles. Int. J. Nanomed. 2017, 12, 7121–7130. [Google Scholar] [CrossRef]
- Rostamzadeh, F.; Jafarinejad-Farsangi, S.; Ansari-Asl, Z.; Farrokhi, M.S.; Jafari, E. Treatment for Myocardial Infarction: In Vivo Evaluation of Curcumin-Loaded PEGylated-GQD Nanoparticles. J. Cardiovasc. Pharmacol. 2023, 81, 361–372. [Google Scholar] [CrossRef]
- Kwon, S.P.; Hwang, B.H.; Park, E.H.; Kim, H.Y.; Lee, J.R.; Kang, M.; Song, S.Y.; Jung, M.; Sohn, H.S.; Kim, E.; et al. Nanoparticle-Mediated Blocking of Excessive Inflammation for Prevention of Heart Failure Following Myocardial Infarction. Small 2021, 17, e2101207. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhu, J.; Xu, Y.W.; Mou, F.F.; Shan, X.L.; Wang, Q.L.; Liu, B.N.; Ning, K.; Liu, J.J.; Wang, Y.C.; et al. Notoginsenoside R1-loaded mesoporous silica nanoparticles targeting the site of injury through inflammatory cells improves heart repair after myocardial infarction. Redox Biol. 2022, 54, 102384. [Google Scholar] [CrossRef]
- Fu, H.; Li, X.; Tan, J. NIPAAm-MMA nanoparticle-encapsulated visnagin ameliorates myocardial ischemia/reperfusion injury through the promotion of autophagy and the inhibition of apoptosis. Oncol. Lett. 2018, 15, 4827–4836. [Google Scholar] [CrossRef]
- Lyu, Y.; Xie, J.; Liu, Y.; Xiao, M.; Li, Y.; Yang, J.; Yang, J.; Liu, W. Injectable Hyaluronic Acid Hydrogel Loaded with Functionalized Human Mesenchymal Stem Cell Aggregates for Repairing Infarcted Myocardium. ACS Biomater. Sci. Eng. 2020, 6, 6926–6937. [Google Scholar] [CrossRef]
- Waters, R.; Alam, P.; Pacelli, S.; Chakravarti, A.R.; Ahmed, R.P.H.; Paul, A. Stem cell-inspired secretome-rich injectable hydrogel to repair injured cardiac tissue. Acta Biomater. 2018, 69, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Zhao, E.R.; Hableel, G.; Hu, T.; Kim, T.; Li, J.; Gonzalez-Pech, N.I.; Cheng, D.J.; Lemaster, J.E.; Xie, Y.; et al. Increasing the Efficacy of Stem Cell Therapy via Triple-Function Inorganic Nanoparticles. ACS Nano 2019, 13, 6605–6617. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.; Tang, Y.; Zhao, M.; Lou, X.; Pretorius, D.; Menasche, P.; Zhu, W.; Zhang, J. CHIR99021 and fibroblast growth factor 1 enhance the regenerative potency of human cardiac muscle patch after myocardial infarction in mice. J. Mol. Cell. Cardiol. 2020, 141, 1–10. [Google Scholar] [CrossRef]
- Qi, Q.; Lu, L.; Li, H.; Yuan, Z.; Chen, G.; Lin, M.; Ruan, Z.; Ye, X.; Xiao, Z.; Zhao, Q. Spatiotemporal delivery of nanoformulated liraglutide for cardiac regeneration after myocardial infarction. Int. J. Nanomed. 2017, 12, 4835–4848. [Google Scholar] [CrossRef]
- Wu, T.; Zhang, X.; Liu, Y.; Cui, C.; Sun, Y.; Liu, W. Wet adhesive hydrogel cardiac patch loaded with anti-oxidative, autophagy-regulating molecule capsules and MSCs for restoring infarcted myocardium. Bioact. Mater. 2023, 21, 20–31. [Google Scholar] [CrossRef]
- Gu, J.; You, J.; Liang, H.; Zhan, J.; Gu, X.; Zhu, Y. Engineered bone marrow mesenchymal stem cell-derived exosomes loaded with miR302 through the cardiomyocyte specific peptide can reduce myocardial ischemia and reperfusion (I/R) injury. J. Transl. Med. 2024, 22, 168. [Google Scholar] [CrossRef] [PubMed]
- Shilo, M.; Oved, H.; Wertheim, L.; Gal, I.; Noor, N.; Green, O.; Baruch, E.S.; Shabat, D.; Shapira, A.; Dvir, T. Injectable Nanocomposite Implants Reduce ROS Accumulation and Improve Heart Function after Infarction. Adv. Sci. 2021, 8, e2102919. [Google Scholar] [CrossRef] [PubMed]
- Awada, H.K.; Long, D.W.; Wang, Z.; Hwang, M.P.; Kim, K.; Wang, Y. A single injection of protein-loaded coacervate-gel significantly improves cardiac function post infarction. Biomaterials 2017, 125, 65–80. [Google Scholar] [CrossRef]
- Zhu, D.; Liu, S.; Huang, K.; Li, J.; Mei, X.; Li, Z.; Cheng, K. Intrapericardial long non-coding RNA-Tcf21 antisense RNA inducing demethylation administration promotes cardiac repair. Eur. Heart J. 2023, 44, 1748–1760. [Google Scholar] [CrossRef]
- Jan, N.; Madni, A.; Khan, S.; Shah, H.; Akram, F.; Khan, A.; Ertas, D.; Bostanudin, M.F.; Contag, C.H.; Ashammakhi, N.; et al. Biomimetic cell membrane-coated poly(lactic-co-glycolic acid) nanoparticles for biomedical applications. Bioeng. Transl. Med. 2023, 8, e10441. [Google Scholar] [CrossRef]
- Zhang, C.X.; Cheng, Y.; Liu, D.Z.; Liu, M.; Cui, H.; Zhang, B.L.; Mei, Q.B.; Zhou, S.Y. Mitochondria-targeted cyclosporin A delivery system to treat myocardial ischemia reperfusion injury of rats. J. Nanobiotechnol. 2019, 17, 18. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wang, Y.; Guo, R.; Li, S.; Ni, J.; Gao, S.; Gao, X.; Mao, J.; Zhu, Y.; Wu, P.; et al. Ginsenoside Rg3-loaded, reactive oxygen species-responsive polymeric nanoparticles for alleviating myocardial ischemia-reperfusion injury. J. Control. Release 2020, 317, 259–272. [Google Scholar] [CrossRef]
- Li, Y.; Chen, X.; Jin, R.; Chen, L.; Dang, M.; Cao, H.; Dong, Y.; Cai, B.; Bai, G.; Gooding, J.J.; et al. Injectable hydrogel with MSNs/microRNA-21-5p delivery enables both immunomodification and enhanced angiogenesis for myocardial infarction therapy in pigs. Sci. Adv. 2021, 7, eabd6740. [Google Scholar] [CrossRef]
- Yaman, S.; Chintapula, U.; Rodriguez, E.; Ramachandramoorthy, H.; Nguyen, K.T. Cell-mediated and cell membrane-coated nanoparticles for drug delivery and cancer therapy. Cancer Drug Resist. 2020, 3, 879–911. [Google Scholar] [CrossRef]
- Jin, J.; Krishnamachary, B.; Barnett, J.D.; Chatterjee, S.; Chang, D.; Mironchik, Y.; Wildes, F.; Jaffee, E.M.; Nimmagadda, S.; Bhujwalla, Z.M. Human Cancer Cell Membrane-Coated Biomimetic Nanoparticles Reduce Fibroblast-Mediated Invasion and Metastasis and Induce T-Cells. ACS Appl. Mater. Interfaces 2019, 11, 7850–7861. [Google Scholar] [CrossRef]
- Liu, H.; Su, Y.Y.; Jiang, X.C.; Gao, J.Q. Cell membrane-coated nanoparticles: A novel multifunctional biomimetic drug delivery system. Drug Deliv. Transl. Res. 2023, 13, 716–737. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Jiang, L.H. Extracellular vesicles: Targeting the heart. Front. Cardiovasc. Med. 2022, 9, 1041481. [Google Scholar] [CrossRef] [PubMed]
- Phumsuay, R.; Muangnoi, C.; Dasuni Wasana, P.W.; Hasriadi; Vajragupta, O.; Rojsitthisak, P.; Towiwat, P. Molecular Insight into the Anti-Inflammatory Effects of the Curcumin Ester Prodrug Curcumin Diglutaric Acid In Vitro and In Vivo. Int. J. Mol. Sci. 2020, 21, 5700. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.Y.; Kim, H.; Mun, D.; Yun, N.; Joung, B. Co-delivery of curcumin and miRNA-144-3p using heart-targeted extracellular vesicles enhances the therapeutic efficacy for myocardial infarction. J. Control. Release 2021, 331, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Ma, J.; Ji, Z.; Shen, J.; Wang, Q. Recent Advances of Cell Membrane Coated Nanoparticles in Treating Cardiovascular Disorders. Molecules 2021, 26, 3428. [Google Scholar] [CrossRef]
- Li, F.; Liu, D.; Liu, M.; Ji, Q.; Zhang, B.; Mei, Q.; Cheng, Y.; Zhou, S. Tregs biomimetic nanoparticle to reprogram inflammatory and redox microenvironment in infarct tissue to treat myocardial ischemia reperfusion injury in mice. J. Nanobiotechnol. 2022, 20, 251. [Google Scholar] [CrossRef]
- Madigan, M.; Atoui, R. Therapeutic Use of Stem Cells for Myocardial Infarction. Bioengineering 2018, 5, 28. [Google Scholar] [CrossRef] [PubMed]
- Saffari, S.; Saffari, T.M.; Ulrich, D.J.O.; Hovius, S.E.R.; Shin, A.Y. The interaction of stem cells and vascularity in peripheral nerve regeneration. Neural Regen. Res. 2021, 16, 1510–1517. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Jiang, D.; Wang, K.; Zheng, D.; Zhu, Z.; Shao, F.; Qian, R.; Lan, X.; Qin, C. Conductive nanocomposite hydrogel and mesenchymal stem cells for the treatment of myocardial infarction and non-invasive monitoring via PET/CT. J. Nanobiotechnol. 2022, 20, 211. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Yang, Z.; Wang, L.; Xing, D.; Lin, J. Global research trends in extracellular vesicles based on stem cells from 1991 to 2021: A bibliometric and visualized study. Front. Bioeng. Biotechnol. 2022, 10, 956058. [Google Scholar] [CrossRef]
- Yang, H.; Qin, X.; Wang, H.; Zhao, X.; Liu, Y.; Wo, H.T.; Liu, C.; Nishiga, M.; Chen, H.; Ge, J.; et al. An in Vivo miRNA Delivery System for Restoring Infarcted Myocardium. ACS Nano 2019, 13, 9880–9894. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Xue, S.; Du, M.; Lian, F. Highly Efficient MicroRNA Delivery Using Functionalized Carbon Dots for Enhanced Conversion of Fibroblasts to Cardiomyocytes. Int. J. Nanomed. 2021, 16, 3741–3754. [Google Scholar] [CrossRef] [PubMed]
- Najahi-Missaoui, W.; Arnold, R.D.; Cummings, B.S. Safe Nanoparticles: Are We There Yet? Int. J. Mol. Sci. 2020, 22, 385. [Google Scholar] [CrossRef] [PubMed]
- Kreyling, W.G.; Semmler-Behnke, M.; Seitz, J.; Scymczak, W.; Wenk, A.; Mayer, P.; Takenaka, S.; Oberdorster, G. Size dependence of the translocation of inhaled iridium and carbon nanoparticle aggregates from the lung of rats to the blood and secondary target organs. Inhal. Toxicol. 2009, 21 (Suppl. S1), 55–60. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Hu, Z.; Ma, J.; Wang, X.; Zhang, Y.; Wang, W.; Yuan, Z. The systematic evaluation of size-dependent toxicity and multi-time biodistribution of gold nanoparticles. Colloids Surf. B Biointerfaces 2018, 167, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, D.; Santra, C.R.; Ghosh, A.N.; Karmakar, P. Differential toxicity of rod and spherical zinc oxide nanoparticles on human peripheral blood mononuclear cells. J. Biomed. Nanotechnol. 2014, 10, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Peng, S.Y.; Tsao, H.H.; Huang, H.T.; Lai, X.Y.; Hsu, H.J.; Jiang, S.J. A Multitarget Therapeutic Peptide Derived From Cytokine Receptors Based on in Silico Analysis Alleviates Cytokine-Stimulated Inflammation. Front. Pharmacol. 2022, 13, 853818. [Google Scholar] [CrossRef] [PubMed]
- Nel, A.E.; Madler, L.; Velegol, D.; Xia, T.; Hoek, E.M.; Somasundaran, P.; Klaessig, F.; Castranova, V.; Thompson, M. Understanding biophysicochemical interactions at the nano-bio interface. Nat. Mater. 2009, 8, 543–557. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.R.; Ullrey, D.E. The pig as a model for human nutrition. Annu. Rev. Nutr. 1987, 7, 361–382. [Google Scholar] [CrossRef] [PubMed]
- De Villiers, C.; Riley, P.R. Mouse models of myocardial infarction: Comparing permanent ligation and ischaemia-reperfusion. Dis. Model. Mech. 2020, 13, dmm046565. [Google Scholar] [CrossRef]
- Park, J.H.; Dehaini, D.; Zhou, J.; Holay, M.; Fang, R.H.; Zhang, L. Biomimetic nanoparticle technology for cardiovascular disease detection and treatment. Nanoscale Horiz. 2020, 5, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Qi, J.; Wang, J.; Hu, W.; Zhou, W.; Wang, Y.; Li, T. Nanoparticle technology for mRNA: Delivery strategy, clinical application and developmental landscape. Theranostics 2024, 14, 738–760. [Google Scholar] [CrossRef] [PubMed]
| Types of Nanoparticles | Payload | Target | Animal Model | Outcomes | Ref. |
|---|---|---|---|---|---|
| Polyethylene glycol nanoparticles | Bilirubin | Infarcted myocardium | Myocardial infarction (ischemia-reperfusion, mice) | Inhibition of cell apoptosis and reduction of myocardial infarction size | [107] |
| Liposome nanoparticles | Methotrexate | Infarcted myocardium | Myocardial infarction (permanent occlusion, mice) | Reduced infarct size and promoted a significant improvement in left ventricular systolic function | [108] |
| Micellar nanoparticles | 2,2,6,6-tetramethylpiperidine-1-oxyl | Infarcted myocardium | Myocardial infarction (ischemia-reperfusion, dog) | Reduced myocardial infarct size and myocardial apoptosis | [109] |
| PEG modification of solid lipid nanoparticles | Schisandrin B | SOD/GSH-Px | Myocardial infarction (permanent occlusion, rat) | Reduction in infarct size | [110] |
| PEG-graphene quantum dot nanoparticles | Curcumin | Infarcted myocardium | Myocardial infarction (permanent occlusion, rat) | Reduction of myocardial infarct size and fibrosis | [111] |
| Liposome nanoparticles | MI antigen and rapamycin | T cell | Myocardial infarction (permanent occlusion, mice) | Infarct size and fibrosis area were reduced | [112] |
| MSN conjugated to CD11b anti-body | Panax notoginseng saponins R1 | Monocytes and neutrophils | Myocardial infarction (permanent occlusion, mice) | Improves local inflammation of injured myocardium and reduces myocardial infarction area | [113] |
| Methacrylic acid, N-isopropyl acrylamide hydrogel | Visnagin | Infarcted myocardium | Myocardial infarction (ischemia-reperfusion, rat) | Reduce myocardial infarction area and improve cardiac dysfunction | [114] |
| Types of Nanoparticles | Payload | Animal Model | Outcomes | Ref. |
|---|---|---|---|---|
| Hyaluronic acid hydrogel | Mesenchymal stem cells | Myocardial infarction (permanent occlusion, rat) | Promotion of angiogenesis, improvement of the microenvironment of MI, and reduced ventricular remodeling | [115] |
| Laponite/gelatin hydrogel | Stem cell-derived secretome | Myocardial infarction (permanent occlusion, rat) | Ejection fraction and cardiac output were improved and cardiac remodeling was reduced | [116] |
| Mesoporous silica-iron oxide nanoparticles | Insulin-like growth factor | Myocardial infarction (ischemia-reperfusion, mice) | Cardiac function indexes such as left ventricular ejection fraction were improved and ventricular remodeling was reduced | [117] |
| PLGA human cardiomyocytes patch | Fibroblast factor 1 and CHIR99021 | Myocardial infarction (permanent occlusion, mice) | Reduced cell apoptosis and improved ventricular remodeling | [118] |
| PLGA-PEG nanoparticles | Liraglutide | Myocardial infarction (permanent occlusion, rat) | Reduced scar thickness and cardiac dilatation, reduced myocardial cell apoptosis, and improved ventricular remodeling apoptosis | [119] |
| Wet tissue adheres to the hydrogel | Resveratrol and mesenchymal stem cells | Myocardial infarction (permanent occlusion, rat) | Improved cardiac microenvironment, reduced myocardial cell apoptosis, and improved ventricular remodeling | [120] |
| Exosomes derived from bone mesenchymal stem cells | Peptide specific for cardiomyocytes | Myocardial infarction (ischemia-reperfusion, mice) | Ejection fraction and other indicators were improved and ventricular remodeling was reduced | [121] |
| Extracellular matrix composite hydrogel | Gold nanoparticles | Myocardial infarction (ischemia-reperfusion, mice) | Improved the ejection fraction, improved ventricular remodeling, and reduced the content of ROS | [122] |
| Composite hydrogel | TIMP-3, FGF-2, SDF-1α | Myocardial infarction (permanent occlusion, rat) | Reduced ventricular dilatation, improved ventricular remodeling and increased cardiomyocyte survival rate | [123] |
| Mesenchymal stem cell-derived extracellular vesicles | – | Myocardial infarction (ischemia reperfusion, mice) | Reduced myocardial cell apoptosis, improved myocardial fibrosis, and reduced ventricular remodeling | [124] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, Q.; Xiao, Y.; Du, L.; Li, Y. Advances in Nanoparticles in the Prevention and Treatment of Myocardial Infarction. Molecules 2024, 29, 2415. https://doi.org/10.3390/molecules29112415
Wei Q, Xiao Y, Du L, Li Y. Advances in Nanoparticles in the Prevention and Treatment of Myocardial Infarction. Molecules. 2024; 29(11):2415. https://doi.org/10.3390/molecules29112415
Chicago/Turabian StyleWei, Qidong, Yifei Xiao, Lixin Du, and Ya Li. 2024. "Advances in Nanoparticles in the Prevention and Treatment of Myocardial Infarction" Molecules 29, no. 11: 2415. https://doi.org/10.3390/molecules29112415