

Cutaneous Melanoma: An Overview of Physiological and Therapeutic Aspects and Biotechnological Use of Serine Protease Inhibitors

 , , ,
, , ,  ,
,
Abstract
:
1. Introduction
2. Epidemiology
3. Melanoma Subtypes
3.1. Lentigo Maligna
3.2. Desmoplastic Melanoma
3.3. Acral Melanoma
3.4. Spitz Melanoma
3.5. Mucosal Melanoma
3.6. Melanoma Arising in a Congenital Nevus
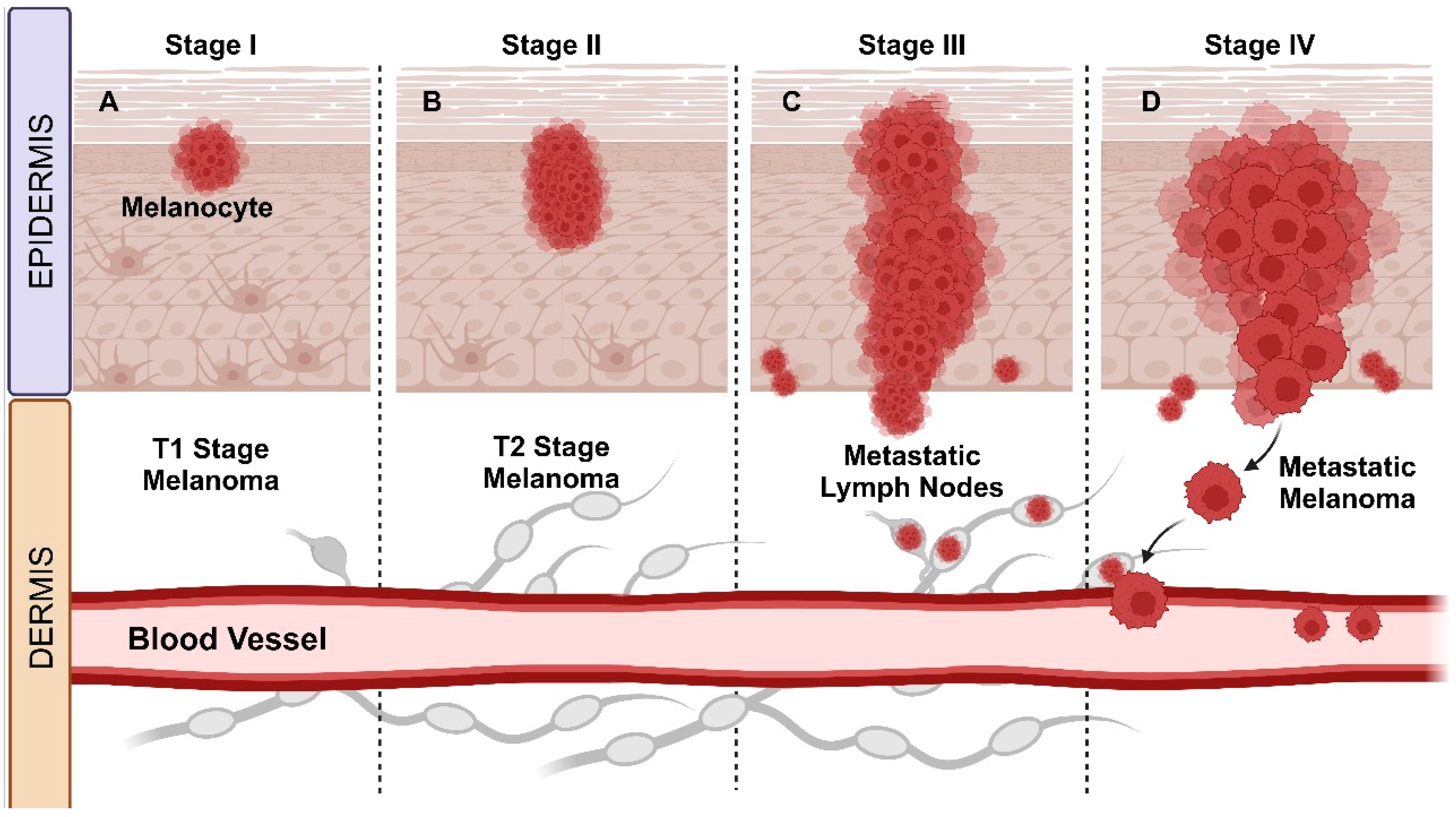
4. Melanoma Staging Phases
4.1. Primary Staging of Melanoma: Stages I and II
4.2. Melanoma Staging for Regional Lymph Nodes: Stage III
4.3. Metastatic Melanoma: Stage IV
5. Therapeutic Strategies and Medications Currently Used
5.1. Conventional Diagnosis and Therapy
5.1.1. Surgical Excision
5.1.2. Radiotherapy
5.1.3. Chemotherapy
5.2. Innovative Therapies
5.2.1. Topical Treatments
5.2.2. Targeted Anticancer Therapies: BRAF or MEK Mutation
5.2.3. Immunotherapy
5.2.4. Toll-like Receptor-9 (TLR-9) Agonists
5.2.5. Adoptive Cellular Therapy
5.2.6. Gene Therapy
6. Biotechnological Use of Serine Protease Inhibitors in the Anticancer Activity of Melanoma
7. Future Perspectives
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- O’Neill, C.H.; Scoggins, C.R. Melanoma. J. Surg. Oncol. 2019, 120, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Singh, D.; Laversanne, M.; Vignat, J.; Vaccarella, S.; Meheus, F.; Cust, A.E.; De Vries, E.; Whiteman, D.C.; Bray, F. Global Burden of Cutaneous Melanoma in 2020 and Projections to 2040. JAMA Dermatol. 2022, 158, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, G.C.; Falzone, L.; Salemi, R.; Zanghì, A.; Spandidos, D.A.; CMcubrey, J.A.; Candido, S.; Libra, M. Cutaneous Melanoma: From Pathogenesis to Therapy (Review). Int. J. Oncol. 2018, 52, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Slominski, R.M.; Sarna, T.; Płonka, P.M.; Raman, C.; Brożyna, A.A.; Slominski, A.T. Melanoma, Melanin, and Melanogenesis: The Yin and Yang Relationship. Front. Oncol. 2022, 12, 842496. [Google Scholar] [CrossRef] [PubMed]
- CMgovern, J.; Booth, J.C.; Clark, H.; Cochran, J.; Hicks, J.D.; Little, J.H.; Milton, G.W. The classification of malignant melanoma and its histologic reporting. Cancer 1973, 32, 1446–1457. [Google Scholar]
- Clark, W.H.; Braitman, L.E.; Trock, B.J.; Schultz, D.; Synnestvedt, M.; Halpern, A.C. Model Predicting Survival in Stage I Melanoma Based on Tumor Progression. J. Natl. Cancer Inst. 1989, 81, 1893–1904. [Google Scholar] [CrossRef] [PubMed]
- Tsao, H.; Olazagasti, J.M.; Cordoro, K.M.; Brewer, J.D.; Taylor, S.C.; Bordeaux, J.S.; Chren, M.M.; Sober, A.J.; Tegeler, C.; Bhushan, R.; et al. Early Detection of Melanoma: Reviewing the ABCDEs American Academy of Dermatology Ad Hoc Task Force for the ABCDEs of Melanoma. J. Am. Acad. Dermatol. 2015, 72, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Elder, D.E.; Bastian, B.C.; Cree, I.A.; Massi, D.; Scolyer, R.A. The 2018 World Health Organization classification of cutaneous, mucosal, and uveal melanoma detailed analysis of 9 distinct subtypes defined by their evolutionary pathway. Arch. Pathol. Lab. Med. 2020, 144, 500–522. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.E.; Shalin, S.C.; Tackett, A.J. Current State of Melanoma Diagnosis and Treatment. Cancer Biol. Ther. 2019, 20, 1366–1379. [Google Scholar] [CrossRef]
- Hasan, N.; Nadaf, A.; Imran, M.; Jiba, U.; Sheikh, A.; Almalki, W.H.; Almujri, S.S.; Mohammed, Y.H.; Kesharwani, P.; Ahmad, F.J. Skin Cancer: Understanding the Journey of Transformation from Conventional to Advanced Treatment Approaches. Mol. Cancer 2023, 22, 168. [Google Scholar] [CrossRef]
- Tsao, H.; Chin, L.; Garraway, L.A.; Fisher, D.E. Melanoma: From Mutations to Medicine. Genes Dev. 2012, 26, 1131–1155. [Google Scholar] [CrossRef]
- Damsky, W.E.; Rosenbaum, L.E.; Bosenberg, M. Decoding Melanoma Metastasis. Cancers 2011, 3, 126–163. [Google Scholar] [CrossRef]
- Gamboa, A.C.; Lowe, M.; Yushak, M.L.; Delman, K.A. Surgical Considerations and Systemic Therapy of Melanoma. Surg. Clin. N. Am. 2020, 100, 141–159. [Google Scholar] [CrossRef]
- Weiss, S.A.; Wolchok, J.D.; Sznol, M. Immunotherapy of Melanoma: Facts and Hopes. Clin. Cancer Res. 2019, 25, 5191–5201. [Google Scholar] [CrossRef]
- Srikanth, S.; Chen, Z. Plant Protease Inhibitors in Therapeutics-Focus on Cancer Therapy. Front. Pharmacol. 2016, 7, 470. [Google Scholar] [CrossRef]
- Cid-Gallegos, M.S.; Corzo-Ríos, L.J.; Jiménez-Martínez, C.; Sánchez-Chino, X.M. Protease Inhibitors from Plants as Therapeutic Agents—A Review. Plant Foods Hum. Nutr. 2022, 77, 20–29. [Google Scholar] [CrossRef]
- Kimman, T.; Slomp, A.; Martens, A.; Grabherr, S.; Li, S.; Van Diest, E.; Meeldijk, J.; Kuball, J.; Minnema, C.M.; Eldering, E.; et al. Serpin B9 Controls Tumor Cell Killing by CAR T Cells. J. Immunother. Cancer 2023, 11, e006364. [Google Scholar] [CrossRef]
- Bulliard, J.L.; Cox, B.; Elwood, J.M. Latitude Gradients in Melanoma Incidence and Mortality in the Non-Maori Population of New Zealand. Cancer Causes Control 1994, 5, 234–240. [Google Scholar] [CrossRef]
- Arnold, M.; de Vries, E.; Whiteman, D.C.; Jemal, A.; Bray, F.; Parkin, D.M.; Soerjomataram, I. Global Burden of Cutaneous Melanoma Attributable to Ultraviolet Radiation in 2012. Int. J. Cancer 2018, 143, 1305–1314. [Google Scholar] [CrossRef]
- Batta, N.; Shangraw, S.; Nicklawsky, A.; Yamauchi, T.; Zhai, Z.; Menon, D.R.; Gao, D.; Dellavalle, R.P.; Fujita, M. Global melanoma correlations with obesity, smoking, and alcohol consumption. JMIR Dermatol. 2021, 4, e31275. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Sera, F.; Cattaruzza, M.S.; Pasquini, P.; Zanetti, R.; Masini, C.; Boyle, P.; Melchi, C.F. Meta-Analysis of Risk Factors for Cutaneous Melanoma: III. Family History, Actinic Damage and Phenotypic Factors. Eur. J. Cancer 2005, 41, 2040–2059. [Google Scholar] [CrossRef]
- Conforti, C.; Zalaudek, I. Epidemiology and Risk Factors of Melanoma: A Review. Dermatol. Pract. Concept. 2021, 11, 2021161S. [Google Scholar] [CrossRef]
- Garbe, C.; Keim, U.; Gandini, S.; Amaral, T.; Katalinic, A.; Hollezcek, B.; Martus, P.; Flatz, L.; Leiter, U.; Whiteman, D. Epidemiology of cutaneous melanoma and keratinocyte cancer in white populations 1943–2036. Eur. J. Cancer 2021, 152, 18–25. [Google Scholar] [CrossRef]
- Buja, A.; Rugge, M.; Damiani, G.; Zorzi, M.; Toni, C.; Vecchiato, A.; Fiore, P.; Spina, R.; Baldo, V.; Brazzale, A.; et al. Sex Differences in Cutaneous Melanoma: Incidence, Clinicopathological Profile, Survival, and Costs. J. Women’s Health 2022, 31, 1012–1019. [Google Scholar] [CrossRef]
- de Castro e Souza, B.; Morais Silva, D.H.; Valente, N.Y.S.; Kakizaki, P.; Luce, M.C.A.; Bandeira, L.G. Cutaneous Melanoma: A Retrospective Study of 18 Years. Are There Gender Differences? An. Bras. Dermatol. 2021, 96, 619–623. [Google Scholar] [CrossRef]
- Bellenghi, M.; Puglisi, R.; Pontecorvi, G.; De Feo, A.; Carè, A.; Mattia, G. Sex and Gender Disparities in Melanoma. Cancers 2020, 12, 1819. [Google Scholar] [CrossRef]
- Sung, H.; Siegel, R.L.; Rosenberg, P.S.; Jemal, A. Emerging Cancer Trends among Young Adults in the USA: Analysis of a Population-Based Cancer Registry. Lancet Public Health 2019, 4, e137–e147. [Google Scholar] [CrossRef]
- Nader Marta, G.; Munhoz, R.R.; Teixeira, M.L.P.; Waldvogel, B.C.; Pires de Camargo, V.; Feher, O.; Sanches, J.A. Trends in Melanoma Mortality in Brazil: A Registry-Based Study. JCO Glob. Oncol. 2020, 6, 1766–1771. [Google Scholar] [CrossRef]
- Pena, S.D.J.; di Pietro, G.; Fuchshuber-Moraes, M.; Genro, J.P.; Hutz, M.H.; Kehdy, F.S.G.; Kohlrausch, F.; Magno, L.A.V.; Montenegro, R.C.; Moraes, M.O.; et al. The Genomic Ancestry of Individuals from Different Geographical Regions of Brazil Is More Uniform Than Expected. PLoS ONE 2011, 6, e17063. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, C.A.; Souza, D.L.B. Melanoma Mortality in Brazil: Trends and Projections (1998–2032). Cienc. E Saude Colet. 2019, 24, 1551–1561. [Google Scholar] [CrossRef]
- Faries, M.B.; Thompson, J.F.; Cochran, A.J.; Andtbacka, R.H.; Mozzillo, N.; Zager, J.S.; Jahkola, T.; Bowles, T.L.; Testori, A.; Beitsch, P.D.; et al. Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma. N. Engl. J. Med. 2017, 376, 2211–2222. [Google Scholar] [CrossRef]
- Rabbie, R.; Ferguson, P.; Molina-Aguilar, C.; Adams, D.J.; Robles-Espinoza, C.D. Melanoma Subtypes: Genomic Profiles, Prognostic Molecular Markers and Therapeutic Possibilities. J. Pathol. 2019, 247, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Carapeba, M.O.L.; Pineze, M.A.; Nai, G.A. Is Dermoscopy a Good Tool for the Diagnosis of Lentigo Maligna and Lentigo Maligna Melanoma? A Meta-Analysis. Clin. Cosmet. Investig. Dermatol. 2019, 12, 403–414. [Google Scholar] [CrossRef]
- Sharma, P.; Otto, M. Multifunctional nanocomposites modulating the tumor microenvironment for enhanced cancer im-munotherapy. Bioact Mater. 2024, 31, 440–462. [Google Scholar] [CrossRef] [PubMed]
- Menzies, S.W.; Liyanarachchi, S.; Coates, E.; Smith, A.; Cooke-Yarborough, C.; Lo, S.; Armstrong, B.; Scolyer, R.A.; Guitera, P. Estimated Risk of Progression of Lentigo Maligna to Lentigo Maligna Melanoma. Melanoma Res. 2020, 30, 193–197. [Google Scholar] [CrossRef]
- Navarrete-Dechent, C.; Cordova, M.; Liopyris, K.; Rishpon, A.; Aleissa, S.; Rossi, A.M.; Lee, E.; Chen, C.C.J.; Busam, K.J.; Marghoob, A.A.; et al. Reflectance confocal microscopy and dermoscopy aid in evaluating repigmentation within or adjacent to lentigo maligna melanoma surgical scars. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 74–81. [Google Scholar] [CrossRef]
- Sina, N.; Saeed-Kamil, Z.; Ghazarian, D. Pitfalls in the diagnosis of lentigo maligna and lentigo maligna melanoma, facts and an opinion. J. Clin. Pathol. 2021, 74, 7–9. [Google Scholar] [CrossRef]
- Cosgarea, I.; Ugurel, S.; Sucker, A.; Livingstone, E.; Zimmer, L.; Ziemer, M.; Utikal, J.; Mohr, P.; Pfeiffer, C.; Pföhler, C.; et al. Targeted next Generation Sequencing of Mucosal Melanomas Identifies Frequent NF1 and RAS Mutations. Oncotarget 2017, 8, 40683–40692. [Google Scholar] [CrossRef]
- Kiuru, M.; Busam, K.J. The NF1 Gene in Tumor Syndromes and Melanoma. Lab. Investig. 2017, 97, 146–157. [Google Scholar] [CrossRef]
- Florent, L.; Saby, C.; Slimano, F.; Morjani, H. BRAF V600-Mutated Metastatic Melanoma and Targeted Therapy Resistance: An Update of the Current Knowledge. Cancers 2023, 15, 2607. [Google Scholar] [CrossRef]
- Ochoa, C.E.; Joseph, R.W. Desmoplastic Melanoma: A Brief Review and the Efficacy of Immunotherapy. Expert Rev. Anticancer Ther. 2019, 19, 205–207. [Google Scholar] [CrossRef]
- Fernandez-Flores, A.; Singh, R.; Cassarino, D.S. Top 10 Differential Diagnoses for Desmoplastic Melanoma. Head Neck Pathol. 2023, 17, 143–153. [Google Scholar] [CrossRef]
- Howard, M.; Xie, C.; Wee, E.; Wolfe, R.; McLean, C.; Kelly, J.W.; Pan, Y. Acral lentiginous melanoma: Clinicopathologic and survival differences according to tumour location. Aust. J. Dermatol. 2020, 61, 312–317. [Google Scholar] [CrossRef]
- Rawson, R.V.; Vergara, I.A.; Stretch, J.R.; Saw, R.P.M.; Thompson, J.F.; Lo, S.N.; Scolyer, R.A.; Busam, K.J. Representa-tiveness of initial skin biopsies showing pure desmoplastic melanoma: Implications for management. Pathology 2023, 55, 214–222. [Google Scholar] [CrossRef]
- Shi, P.; Xu, Z.; Lei, X.; Yibulayin, F.; Wushou, A. Desmoplastic melanoma: Demographic and clinicopathological features and disease-specific prognostic factors. Oncol. Lett. 2019, 17, 5619–5627. [Google Scholar] [CrossRef]
- Hadfield, M.J.; Helsing, R.; Grant-Kels, J.M. Desmoplastic melanoma: An updated clinical review and the emerging role of genetic markers and immunotherapies. Melanoma Res. 2020, 30, 429–432. [Google Scholar] [CrossRef]
- Boada Garcia, A.; Quer Pi-Sunyer, A.; Richarz, N.; Jaka-Moreno, A. Update on the Diagnosis and Management of Desmoplastic Melanoma. Actas Dermosifiliogr. 2022, 113, 47–57. [Google Scholar] [CrossRef]
- Wiesner, T.; Kiuru, M.; Scott, S.N.; Arcila, M.; Halpern, A.C.; Hollmann, T.; Berger, M.F.; Busam, K.J. NF1 Mutations Are Common in Desmoplastic Melanoma. Am. J. Surg. Pathol. 2015, 39, 1357–1362. [Google Scholar] [CrossRef]
- Kadokura, A.; Frydenlund, N.; Leone, D.A.; Yang, S.; Hoang, M.P.; Deng, A.; Hernandez-Perez, M.; Biswas, A.; Singh, R.; Yaar, R.; et al. Neurofibromin protein loss in desmoplastic melanoma subtypes: Implicating NF1 allelic loss as a distinct genetic driver? Hum. Pathol. 2016, 53, 82–90. [Google Scholar] [CrossRef]
- Zob, D.L.; Augustin, I.; Caba, L.; Panzaru, M.C.; Popa, S.; Popa, A.D.; Florea, L.; Gorduza, E.V. Genomics and Epigenomics in the Molecular Biology of Melanoma—A Prerequisite for Biomarkers Studies. Int. J. Mol. Sci. 2023, 24, 716. [Google Scholar] [CrossRef]
- Nakamura, Y.; Namikawa, K.; Yoshino, K.; Yoshikawa, S.; Uchi, H.; Goto, K.; Fukushima, S.; Kiniwa, Y.; Takenouchi, T.; Uhara, H.; et al. Anti-PD1 Checkpoint Inhibitor Therapy in Acral Melanoma: A Multicenter Study of 193 Japanese Patients. Ann. Oncol. 2020, 31, 1198–1206. [Google Scholar] [CrossRef]
- Tod, B.M.; Schneider, J.W.; Bowcock, A.M.; Visser, W.I.; Kotze, M.J. The Tumor Genetics of Acral Melanoma: What Should a Dermatologist Know? JAAD Int. 2020, 1, 135–147. [Google Scholar] [CrossRef]
- Zheng, Q.; Li, J.; Zhang, H.; Wang, Y.; Zhang, S. Immune Checkpoint Inhibitors in Advanced Acral Melanoma: A Systematic Review. Front. Oncol. 2020, 10, 602705. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, S.S.; Ferreira, I.; Elder, D.E.; Nobre, A.B.; Martínez-Said, H.; Adams, D.J.; Robles-Espinoza, C.D.; Possik, P.A. More than Just Acral Melanoma: The Controversies of Defining the Disease. J. Pathol. Clin. Res. 2021, 7, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Darmawan, C.C.; Jo, G.; Montenegro, S.E.; Kwak, Y.; Cheol, L.; Cho, K.H.; Mun, J.H. Early Detection of Acral Melanoma: A Review of Clinical, Dermoscopic, Histopathologic, and Molecular Characteristics. J. Am. Acad. Dermatol. 2019, 81, 805–812. [Google Scholar] [CrossRef]
- Basurto-Lozada, P.; Molina-Aguilar, C.; Castaneda-Garcia, C.; Vázquez-Cruz, M.E.; Garcia-Salinas, O.I.; Álvarez-Cano, A.; Martínez-Said, H.; Roldán-Marín, R.; Adams, D.J.; Possik, P.A.; et al. Acral Lentiginous Melanoma: Basic Facts, Biological Characteristics and Research Perspectives of an Understudied Disease. Pigment Cell Melanoma Res. 2021, 34, 59–71. [Google Scholar] [CrossRef]
- Raghavan, S.S.; Peternel, S.; Mully, T.W.; North, J.P.; Pincus, L.B.; LeBoit, P.E.; McCalmont, T.H.; Bastian, B.C.; Yeh, I. Spitz Melanoma is a Distinct Subset of Spitzoid Melanoma. Mod. Pathol. 2020, 33, 1122–1134. [Google Scholar] [CrossRef]
- Bastian, B.C.; LeBoit, P.E.; Pinkel, D. Mutations and Copy Number Increase of HRAS in Spitz Nevi with Distinctive Histo-pathological Features. Am. J. Pathol. 2000, 157, 967–972. [Google Scholar] [CrossRef]
- Wiesner, T.; He, J.; Yelensky, R.; Esteve-Puig, R.; Botton, T.; Yeh, I.; Lipson, D.; Otto, G.; Brennan, K.; Murali, R.; et al. Kinase Fusions are Frequent in Spitz Tumours and Spitzoid Melanomas. Nat. Commun. 2014, 5, 3116. [Google Scholar] [CrossRef] [PubMed]
- Batra, S. Spitzoid Melanoma of Childhood: A Case Series and Review. Melanoma Manag. 2015, 2, 121–125. [Google Scholar] [CrossRef]
- Benton, S.; Roth, A.; Khan, A.U.; Zhao, J.; Kim, D.; Compres, E.V.; Wagner, A.M.; Kruse, L.L.; Zhang, B.; Gerami, P. Risk Factors for the Development of Spitz Neoplasms. Pediatr. Dermatol. 2022, 39, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Ritter, A.; Tronnier, M.; Vaske, B.; Mitteldorf, C. Reevaluation of Established and New Criteria in Differential Diagnosis of Spitz Nevus and Melanoma. Arch. Dermatol. Res. 2018, 310, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.W.; Ahern, M.C.; Giubellino, A. The Spectrum of Spitz Melanocytic Lesions: From Morphologic Diagnosis to Mo-lecular Classification. Front. Oncol. 2022, 12, 889223. [Google Scholar] [CrossRef]
- Dimonitsas, E.; Liakea, A.; Sakellariou, S.; Thymara, I.; Giannopoulos, A.; Stratigos, A.; Soura, E.; Saetta, A.; Korkolopoulou, P. An Update on Molecular Alterations in Melanocytic Tumors with Emphasis on Spitzoid Lesions. Ann. Transl. Med. 2018, 6, 249. [Google Scholar] [CrossRef]
- Ma, Y.; Xia, R.; Ma, X.; Judson-Torres, R.L.; Zeng, H. Mucosal Melanoma: Pathological Evolution, Pathway Dependency and Targeted Therapy. Front. Oncol. 2021, 11, 702287. [Google Scholar] [CrossRef]
- Santeufemia, D.A.; Palmieri, G.; Miolo, G.; Colombino, M.; Doro, M.G.; Frogheri, L.; Paliogiannis, P.; Capobianco, G.; Madonia, M.; Cossu, A.; et al. Current Trends in Mucosal Melanomas: An Overview. Cancers 2023, 15, 1356. [Google Scholar] [CrossRef]
- Schoenewolf, N.L.; Bull, C.; Belloni, B.; Holzmann, D.; Tonolla, S.; Lang, R.; Mihic-Probst, D.; Andres, C.; Dummer, R. Sinonasal, Genital and Acrolentiginous Melanomas Show Distinct Characteristics of KIT Expression and Mutations. Eur. J. Cancer 2012, 48, 1842–1852. [Google Scholar] [CrossRef]
- Kinsler, V.A.; O’Hare, P.; Bulstrode, N.; Calonje, J.E.; Chong, W.K.; Hargrave, D.; Jacques, T.; Lomas, D.; Sebire, N.J.; Slater, O. Melanoma in Congenital Melanocytic Naevi. Br. J. Dermatol. 2017, 176, 1131–1143. [Google Scholar] [CrossRef]
- Noto, G. On the Clinical Significance of Cutaneous Melanoma′s Precursors. Indian Dermatol. Online J. 2012, 3, 83–88. [Google Scholar] [CrossRef]
- Frischhut, N.; Zelger, B.; Andre, F.; Zelger, B.G. The Spectrum of Melanocytic Nevi and Their Clinical Implications. JDDG—J. Ger. Soc. Dermatol. 2022, 20, 483–504. [Google Scholar] [CrossRef]
- Bauer, J.; Curtin, J.A.; Pinkel, D.; Bastian, B.C. Congenital Melanocytic Nevi Frequently Harbor NRAS Mutations but No BRAF Mutations. J. Investig. Dermatol. 2007, 127, 179–182. [Google Scholar] [CrossRef]
- Bahrami, A.; Barnhill, R.L. Pathology and Genomics of Pediatric Melanoma: A Critical Reexamination and New Insights. Pediatr. Blood Cancer 2018, 65, e26792. [Google Scholar] [CrossRef]
- Keung, E.Z.; Gershenwald, J.E. The Eighth Edition American Joint Committee on Cancer (AJCC) Melanoma Staging System: Implications for Melanoma Treatment and Care. Expert Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge from a Population-based to a More “Personalized” Approach to Cancer Staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Garbe, C.; Keim, U.; Amaral, T.; Berking, C.; Eigentler, T.K.; Flatz, L.; Gesierich, A.; Leiter, U.; Stadler, R.; Sunderkötter, C.; et al. Prognosis of Patients with Primary Melanoma Stage I and II According to American Joint Committee on Cancer Version 8 Validated in Two Independent Cohorts: Implications for Adjuvant Treatment. J. Clin. Oncol. 2022, 40, 3741–3749. [Google Scholar] [CrossRef]
- Scolyer, R.A.; Shaw, H.M.; Thompson, J.F.; Li, L.X.L.; Colman, M.H.; Lo, S.K.; McCarthy, S.W.; Palmer, A.A.; Nicoll, K.D.; Dutta, B.; et al. Interobserver Reproducibility of Histopathologic Prognostic Variables in Primary Cutaneous Melanomas. Am. J. Surg. Pathol. 2003, 27, 1571–1576. [Google Scholar] [CrossRef]
- Ge, L.; Vilain, R.E.; Lo, S.; Aivazian, K.; Scolyer, R.A.; Thompson, J.F. Breslow Thickness Measurements of Melanomas Around American Joint Committee on Cancer Staging Cut-Off Points: Imprecision and Terminal Digit Bias Have Important Impli-cations for Staging and Patient Management. Ann. Surg. Oncol. 2016, 23, 2658–2663. [Google Scholar] [CrossRef] [PubMed]
- Bunnell, A.M.; Nedrud, S.M.; Fernandes, R.P. Classification and Staging of Melanoma in the Head and Neck. Oral Maxillofac. Surg. Clin. N. Am. 2022, 34, 221–234. [Google Scholar] [CrossRef]
- Han, D.; van Akkooi, A.C.J.; Straker, R.J.; Shannon, A.B.; Karakousis, G.C.; Wang, L.; Kim, K.B.; Reintgen, D. Current Man-agement of Melanoma Patients with Nodal Metastases. Clin. Exp. Metastasis 2022, 39, 181–199. [Google Scholar] [CrossRef]
- Love, T.P.; Delman, K.A. Management of Regional Lymph Node Basins in Melanoma. Ochsner J. 2010, 10, 99–107. [Google Scholar]
- Bartlett, E.K. Current management of regional lymph nodes in patients with melanoma. J. Surg. Oncol. 2019, 119, 200–207. [Google Scholar] [CrossRef]
- Papageorgiou, C.; Apalla, Z.; Manoli, S.; Lallas, K. Dermatology Practical & Conceptual Melanoma: Staging and Follow-Up. Dermatol. Pract. Concept. 2021, 11, e2021162S. [Google Scholar] [CrossRef]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final Version of 2009 AJCC Melanoma Staging and Classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef]
- Maverakis, E.; Cornelius, L.A.; Bowen, G.M.; Phan, T.; Patel, F.B.; Fitzmaurice, S.; He, Y.; Burrall, B.; Duong, C.; Kloxin, A.M.; et al. Metastatic Melanoma—A Review of Current and Future Treatment Options. Acta Derm. Venereol. 2015, 95, 516–524. [Google Scholar] [CrossRef]
- National Cancer Institute (NCI). Advances in Melanoma and Other Skin Cancers Research. 2024. Available online: https://www.cancer.gov/types/skin/research (accessed on 1 April 2024).
- Rahimi, A.; Esmaeili, Y.; Dana, N.; Dabiri, A.; Rahimmanesh, I.; Jandaghian, S.; Vaseghi, G.; Shariati, L.; Zarrabi, A.; Haghjooy Javanmard, S.; et al. A Comprehensive Review on Novel Targeted Therapy Methods and Nanotechnology-Based Gene De-livery Systems in Melanoma. Eur. J. Pharm. Sci. 2023, 187, 106476. [Google Scholar] [CrossRef]
- Swetter, S.M.; Thompson, J.A.; Albertini, M.R.; Barker, C.A.; Baumgartner, J.; Boland, G.; Chmielowski, B.; DiMaio, D.; Durham, A.; Fields, R.C.; et al. Melanoma: Cutaneous, Version 2.2021 Featured Updates to the NCCN Guidelines. JNCCN J. Natl. Compr. Cancer Netw. 2021, 19, 364–376. [Google Scholar] [CrossRef]
- Curti, N.; Veronesi, G.; Dika, E.; Misciali, C.; Marcelli, E.; Giampieri, E. Breslow Thickness: Geometric Interpretation, Potential Pitfalls, and Computer Automated Estimation. Pathol. Res. Pract. 2022, 238, 154117. [Google Scholar] [CrossRef]
- Jang, S.S.; Davis, M.E.; Vera, D.R.; Lai, S.Y.; Guo, T.W. Role of sentinel lymph node biopsy for oral squamous cell carcinoma: Current evidence and future challenges. Head Neck 2023, 45, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Sharon, C.E.; Straker, R.J.; Gimotty, P.A.; Chu, E.Y.; Mitchell, T.C.; Miura, J.T.; Marchetti, M.A.; Bartlett, E.K.; Karakousis, G.C. Sentinel Lymph Node Biopsy Status Improves Adjuvant Therapy Decision-Making in Patients with Clinical Stage IIB/C Melanoma: A Population-Based Analysis. J. Am. Acad. Dermatol. 2023, 88, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, O.; Das, M.; Hajarizadeh, B.; Mathy, J.A. Impact of Shave Biopsy on Diagnosis and Management of Cutaneous Melanoma: A Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2021, 28, 6168–6176. [Google Scholar] [CrossRef] [PubMed]
- Stassen, R.C.; Mulder, E.E.A.P.; Mooyaart, A.L.; Francken, A.B.; van der Hage, J.; Aarts, M.J.B.; van der Veldt, A.A.M.; Verhoef, C.; Grünhagen, D.J. Clinical Evaluation of the Clinicopathologic and Gene Expression Profile (CP-GEP) in Patients with Melanoma Eligible for Sentinel Lymph Node Biopsy: A Multicenter Prospective Dutch Study. Eur. J. Surg. Oncol. 2023, 49, 107249. [Google Scholar] [CrossRef]
- Van Akkooi, A.C.J.; Schadendorf, D.; Eggermont, A.M.M. Alternatives and Reduced Need for Sentinel Lymph Node Biopsy (SLNB) Staging for Melanoma. Eur. J. Cancer 2023, 182, 163–169. [Google Scholar] [CrossRef]
- Cullen, J.K.; Simmons, J.L.; Parsons, P.G.; Boyle, G.M. Topical Treatments for Skin Cancer. Adv. Drug Deliv. Rev. 2020, 153, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Trepanowski, N.; Grant-Kels, J.M.; Leboeuf, M. Mohs micrographic surgery in the surgical treatment paradigm of melanoma in situ and invasive melanoma: A clinical review of treatment efficacy and ongoing controversies. J. Am. Acad. Dermatol. 2024, 19. [Google Scholar] [CrossRef] [PubMed]
- Huerta, T.; Swetter, S.M.; Nehal, K.S.; Coit, D.G.; Bichakjian, C.K.; Durham, A.B. Current evidence does not support Mohs micrographic surgery or staged excision as equivalent to wide excision for primary cutaneous melanoma. J. Am. Acad. Dermatol. 2023, 88, 959–960. [Google Scholar] [CrossRef] [PubMed]
- Dann, A.M.; Ariyan, C. The Role of Surgery for Stage IV Melanoma. Adv. Surg. 2024, 58, 223–234. [Google Scholar] [CrossRef]
- Carlos-Reyes, A.; Muñiz-Lino, M.A.; Romero-Garcia, S.; López-Camarillo, C.; Hernández-de la Cruz, O.N. Biological Adaptations of Tumor Cells to Radiation Therapy. Front. Oncol. 2021, 11, 718636. [Google Scholar] [CrossRef]
- Borzillo, V.; Muto, P. Radiotherapy in the Treatment of Subcutaneous Melanoma. Cancers 2021, 13, 5859. [Google Scholar] [CrossRef]
- Bliley, R.; Avant, A.; Medina, T.M.; Lanning, R.M. Radiation and Melanoma: Where Are We Now? Curr. Oncol. Rep. 2024, 26, 904–914. [Google Scholar] [CrossRef]
- Bhandari, M.; Othus, M.; Kirkwood, J.; Sondak, V.; Ahmad, T.; Sharon, E.; Grossmann, K.; Ribas, A.; Patel, S.; Wuthrick, E.J. Role of Adjuvant Regional Nodal Irradiation in Resected Melanoma: A Secondary Analysis of SWOG S1404. Int. J. Radiat. Oncol. Biol. Phys. 2022, 114, S82–S83. [Google Scholar] [CrossRef]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A.; et al. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Rulli, E.; Legramandi, L.; Salvati, L.; Mandala, M. The impact of targeted therapies and immunotherapy in melanoma brain metastases: A systematic review and meta-analysis. Cancer 2019, 125, 3776–3789. [Google Scholar] [CrossRef]
- Skin Cancer Foundation. Melanoma Treatment, 2024. Available online: https://www.skincancer.org/skin-cancer-information/melanoma/melanoma-treatments/ (accessed on 1 March 2024).
- Zhu, Y.; Xiao, W.; Zhong, W.; Xi, C.; Ye, J.; Zhang, Q.; Wu, H.; Du, S. Study of the Skin-Penetration Promoting Effect and Mechanism of Combined System of Curcumin Liposomes Prepared by Microfluidic Chip and Skin Penetrating Peptides TD-1 for Topical Treatment of Primary Melanoma. Int. J. Pharm. 2023, 643, 123256. [Google Scholar] [CrossRef]
- Slavkova, M.; Tzankov, B.; Popova, T.; Voycheva, C. Gel Formulations for Topical Treatment of Skin Cancer: A Review. Gels 2023, 9, 352. [Google Scholar] [CrossRef]
- National Cancer Institute. Targeted Therapy for Cancer—NCI. 2022. Available online: https://www.cancer.gov/about-cancer/treatment/types/targeted-therapies (accessed on 31 May 2022).
- Kim, S.; Youssef, S.H.; Song, Y.; Garg, S. Development and Application of a Chromatographic Method for Simultaneous Quantification of 5-Fluorouracil and Imiquimod in Drug-in-Adhesive Topical Patches. Sustain. Chem. Pharm. 2022, 27, 100711. [Google Scholar] [CrossRef]
- Mironiuk-Puchalska, E.; Karatsai, O.; Żuchowska, A.; Wróblewski, W.; Borys, F.; Lehka, L.; Rędowicz, M.J.; Koszytkowska-Stawińska, M. Development of 5-Fluorouracil-Dichloroacetate Mutual Prodrugs as Anticancer Agents. Bioorg. Chem. 2023, 140, 106784. [Google Scholar] [CrossRef]
- Fan, Z.; Wu, C.; Chen, M.; Jiang, Y.; Wu, Y.; Mao, R.; Fan, Y. The Generation of PD-L1 and PD-L2 in Cancer Cells: From Nuclear Chromatin Reorganization to Extracellular Presentation. Acta Pharm. Sin. B 2022, 12, 1041–1053. [Google Scholar] [CrossRef] [PubMed]
- Vaienti, S.; Calzari, P.; Nazzaro, G. Topical Treatment of Melanoma In Situ, Lentigo Maligna, and Lentigo Maligna Melanoma with Imiquimod Cream: A Systematic Review of the Literature. Dermatol. Ther. 2023, 13, 2187–2215. [Google Scholar] [CrossRef]
- Ogbourne, S.M.; Suhrbier, A.; Jones, B.; Cozzi, S.J.; Boyle, G.M.; Morris, M.; CMAlpine, D.; Johns, J.; Scott, T.M.; Sutherland, K.P.; et al. Antitumor Activity of 3-Ingenyl Angelate: Plasma Membrane and Mitochondrial Disruption and Necrotic Cell Death. Cancer Res. 2004, 64, 2833–2839. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Shukla, S.; Lee, A.; Garfield, S.H.; Maloney, D.J.; Ambudkar, S.V.; Yuspa, S.H. The Skin Cancer Chemotherapeutic Agent Ingenol-3-Angelate (PEP005) Is a Substrate for the Epidermal Multidrug Transporter (ABCB1) and Targets Tumor Vasculature. Cancer Res. 2010, 70, 4509–4519. [Google Scholar] [CrossRef]
- Ogawa, H.; Luxardi, G.; Kirane, A.; Kulkarni, R.; Monjazeb, A.M.; Cheng, M.Y.; Ma, C.; Maverakis, E. T Cells Dominate the Local Immune Response Induced by Intralesional IL-2 in Combination with Imiquimod and Retinoid for In-Transit Metastatic Melanoma. J. Investig. Dermatol. 2018, 138, 1442–1445. [Google Scholar] [CrossRef] [PubMed]
- Shi, V.Y.; Tran, K.; Patel, F.; Leventhal, J.; Konia, T.; Fung, M.A.; Wilken, R.; Garcia, M.S.; Fitzmaurice, S.D.; Joo, J.; et al. 100% Complete Response Rate in Patients with Cutaneous Metastatic Melanoma Treated with Intralesional Interleukin (IL)-2, Imiquimod, and Topical Retinoid Combination Therapy: Results of a Case Series. J. Am. Acad. Dermatol. 2015, 73, 645–654. [Google Scholar] [CrossRef]
- Franklin, C.; Livingstone, E.; Roesch, A.; Schilling, B.; Schadendorf, D. Immunotherapy in Melanoma: Recent Advances and Future Directions. Eur. J. Surg. Oncol. 2017, 43, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Garutti, M.; Targato, G.; Buriolla, S.; Palmero, L.; Minisini, A.M.; Puglisi, F. Cdk4/6 Inhibitors in Melanoma: A Comprehensive Review. Cells 2021, 10, 1334. [Google Scholar] [CrossRef]
- Ottaviano, M.; Giunta, E.F.; Tortora, M.; Curvietto, M.; Attademo, L.; Bosso, D.; Cardalesi, C.; Rosanova, M.; De Placido, P.; Pietroluongo, E.; et al. BRAF Gene and Melanoma: Back to the Future. Int. J. Mol. Sci. 2021, 22, 3474. [Google Scholar] [CrossRef]
- Dang, H.; Sui, M.; He, Q.; Xie, J.; Liu, Y.; Hou, P.; Ji, M. Pin1 Inhibitor API-1 Sensitizes BRAF-Mutant Thyroid Cancers to BRAF Inhibitors by Attenuating HER3-Mediated Feedback Activation of MAPK/ERK and PI3K/AKT Pathways. Int. J. Biol. Macromol. 2023, 248, 125867. [Google Scholar] [CrossRef]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.-F.; Testori, A.; Grob, J.-J.; et al. Ipilimumab plus Dacarbazine for Previously Untreated Metastatic Melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.; Chen, T.; Zhang, T.; Shi, S.; Zhang, M.; Qin, X.; Liu, Y.; Li, L.; Lin, Y. Transdermal Treatment for Malignant Melanoma by Aptamer-Modified Tetrahedral Framework Nucleic Acid Delivery of Vemurafenib. Chin. Chem. Lett. 2023, 35, 108602. [Google Scholar] [CrossRef]
- O’Leary, B.; Finn, R.S.; Turner, N.C. Treating Cancer with Selective CDK4/6 Inhibitors. Nat. Rev. Clin. Oncol. 2016, 13, 417–430. [Google Scholar] [CrossRef]
- American Cancer Society. Melanoma Targeted Therapy, Targeted Drugs for Melanoma. 2023. Available online: https://www.cancer.org/cancer/types/melanoma-skin-cancer/treating/targeted-therapy.html (accessed on 27 October 2023).
- Chapman, P.B.; Hauschild, A.; Robert, C.; Haanen, J.B.; Ascierto, P.; Larkin, J.; Dummer, R.; Garbe, C.; Testori, A.; Maio, M.; et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N. Engl. J. Med. 2011, 364, 2507–2516. [Google Scholar] [CrossRef]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Overall survival in patients with BRAF-mutant melanoma receiving encorafenib plus binimetinib versus vemurafenib or encorafenib (COLUMBUS): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1315–1327. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Mcarthur, G.A.; Dréno, B.; Atkinson, V.; Liszkay, G.; Di Giacomo, A.M.; Mandalà, M.; Demidov, L.; Stroyakovskiy, D.; Thomas, L.; et al. Cobimetinib combined with vemurafenib in advanced BRAF(V600)-mutant melanoma (coBRIM): Updated efficacy results from a randomised, double-blind, phase 3 trial. Lancet Oncol. 2016, 17, 1248–1260. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; Amonkar, M.M.; Stroyakovskiy, D.; Levchenko, E.; Gogas, H.; De Braud, F.; Grob, J.-J.; Bondarenko, I.; Garbe, C.; Lebbe, C.; et al. Health-related quality of life impact in a randomised phase III study of the combination of dabrafenib and trametinib versus dabrafenib monotherapy in patients with BRAF V600 metastatic melanoma. Eur. J. Cancer 2015, 51, 833–840. [Google Scholar] [CrossRef]
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Combi-V: A Randomised, Open-Label, Phase III Study Comparing the Combination of Dabrafenib (D) and Trametinib (T) with Vemurafenib (V) As First-Line Therapy in Patients (Pts) with Unresectable or Metastatic Braf V600E/K Mutation-Positive Cutaneous Melanoma. Ann. Oncol. 2014, 25, v1–v41. [Google Scholar] [CrossRef]
- Berking, C.; Livingstone, E.; Debus, D.; Loquai, C.; Weichenthal, M.; Leiter, U.; Kiecker, F.; Mohr, P.; Eigentler, T.K.; Remy, J.; et al. COMBI-r: A Prospective, Non-Interventional Study of Dabrafenib Plus Trametinib in Unselected Patients with Unresectable or Metastatic BRAF V600-Mutant Melanoma. Cancers 2023, 15, 4436. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Mao, L.; Chi, Z.; Sheng, X.; Cui, C.; Kong, Y.; Dai, J.; Wang, X.; Li, S.; Tang, B.; et al. Efficacy Evaluation of Imatinib for the Treatment of Melanoma: Evidence from a Retrospective Study. Oncol. Res. 2019, 27, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Pham, D.M.; Guhan, S.; Tsao, H. Kit and Melanoma: Biological Insights and Clinical Implications. Yonsei Med. J. 2020, 61, 562–571. [Google Scholar] [CrossRef]
- Livingstone, E.; Zimmer, L.; Vaubel, J.; Schadendorf, D. BRAF, MEK and KIT Inhibitors for Melanoma: Adverse Events and Their Management. Chin. Clin. Oncol. 2014, 3, 29. [Google Scholar] [CrossRef]
- Xu, M.; Ma, X.; Wang, Y.; Yu, Z.; Zheng, X.; Dai, H.; Xue, C. Developing a prognostic model for skin melanoma based on the persistent tumor mutation burden and determining IL17REL as a therapeutic target. J. Cancer Res. Clin. Oncol. 2024, 150, 313. [Google Scholar] [CrossRef] [PubMed]
- Yao, Z.; Lu, L.; Xu, Q.; Hua, S.; Wang, H.; Jiang, H. Integrated Analysis Reveals COL4A3 as a Novel Diagnostic and Therapeutic Target in UV-Related Skin Cutaneous Melanoma. Clin. Cosmet. Investig. Dermatol. 2024, 17, 1429–1446. [Google Scholar] [CrossRef]
- Li, C.; Wu, N.; Lin, X.; Zhou, Q.; Xu, M. Integrated transcriptomic and immunological profiling reveals new diagnostic and prognostic models for cutaneous melanoma. Front. Pharmacol. 2024, 15, 1389550. [Google Scholar] [CrossRef]
- Li, Y.; Grenklo, S.; Higgins, T.; Karlsson, R. The profilin: Actin complex localizes to sites of dynamic actin polymerization at the leading edge of migrating cells and pathogen-induced actin tails. Eur. J. Cell Biol. 2008, 87, 893–904. [Google Scholar] [CrossRef] [PubMed]
- Knight, A.; Karapetyan, L.; Kirkwood, J.M. Immunotherapy in Melanoma: Recent Advances and Future Directions. Cancers 2023, 15, 1106. [Google Scholar] [CrossRef]
- Donninger, H.; Li, C.; Eaton, J.W.; Yaddanapudi, K. Cancer Vaccines: Promising Therapeutics or an Unattainable Dream. Vaccines 2021, 9, 668. [Google Scholar] [CrossRef]
- Liu, H.; Shen, W.; Liu, W.; Yang, Z.; Yin, D.; Xiao, C. From Oncolytic Peptides to Oncolytic Polymers: A New Paradigm for Oncotherapy. Bioact. Mater. 2024, 31, 206–230. [Google Scholar] [CrossRef]
- Giannopoulou, C.; Sideris, E.; Wade, R.; Moe-Byrne, T.; Eastwood, A.; McKenna, C. Ipilimumab for Previously Untreated Unresectable Malignant Melanoma: A Critique of the Evidence. Pharmacoeconomics 2015, 33, 1269–1279. [Google Scholar] [CrossRef] [PubMed]
- Boussiotis, V.A. Molecular and Biochemical Aspects of the PD-1 Checkpoint Pathway Immune Checkpoint Blockade As Cancer Therapy. N. Engl. J. Med. 2017, 375, 1767–1778. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.-A.; Reed, K.; et al. Safety and Clinical Activity of Combined PD-1 (Nivolumab) and CTLA-4 (Ipilimumab) Blockade in Advanced Melanoma Patients Jedd. Physiol. Behav. 2017, 169, 122–133. [Google Scholar]
- Stroyakovskiy, D.; Gogas, H.; Robert, C.; Lewis, K.; Protsenko, S.; Pereira, R.P.; Eigentler, T.; Rutkowski, P.; Demidov, L.; Manikhas, G.M.; et al. Atezolizumab, vemurafenib, and cobimetinib as first-line treatment for unresectable advanced BRAFV600 mutation-positive melanoma (IMspire150): Primary analysis of the randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2020, 395, 1835–1844. [Google Scholar] [CrossRef]
- Hamid, O.; Robert, C.; Daud, A.; Carlino, M.S.; Mitchell, T.C.; Hersey, P.; Schachter, J.; Long, G.V.; Hodi, F.S.; Wolchok, J.D.; et al. Long-term outcomes in patients with advanced melanoma who had initial stable disease with pembrolizumab in KEYNOTE-001 and KEYNOTE-006. Eur. J. Cancer 2021, 157, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.-J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.W.; Weber, J.S.; et al. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N. Engl. J. Med. 2013, 369, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Caisová, V.; Uher, O.; Nedbalová, P.; Jochmanová, I.; Kvardová, K.; Masáková, K.; Krejčová, G.; Paďouková, L.; Chmelař, J.; Kopecký, J.; et al. Effective Cancer Immunotherapy Based on Combination of TLR Agonists with Stimulation of Phagocytosis. Int. Immunopharmacol. 2018, 59, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Honda, K.; Yanai, H.; Negishi, H.; Asagiri, M.; Sato, M.; Mizutani, T.; Ohba, Y.; Takaoka, A.; Yoshida, N.; Taniguchi, T. IRF-7 Is the Master Regulator of Type-I Interferon-Dependent Immune Responses. Nature 2005, 434, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, K.D.; Irvine, D.J. Roles for Innate Immunity in Combination Immunotherapies. Cancer Res. 2017, 77, 5215–5221. [Google Scholar] [CrossRef]
- Patidar, A.; Selvaraj, S.; Chakravarti, M.; Guha, I.; Bhuniya, A.; Bera, S.; Dhar, S.; Roy, K.; Baral, R.; Chattopadhyay, D.; et al. TLR Induced IL-27 Plays Host-Protective Role against B16BL6 Melanoma in C57BL/6 Mice. Cytokine 2022, 154, 155871. [Google Scholar] [CrossRef]
- Haymaker, C.; Johnson, D.H.; Murthy, R.; Bentebibel, S.E.; Uemura, M.I.; Hudgens, C.W.; Safa, H.; James, M.; And Tbacka, R.H.I.; Johnson, D.B.; et al. Tilsotolimod with Ipilimumab Drives Tumor Responses in Anti–Pd-1 Refractory Melanoma. Cancer Discov. 2021, 11, 1996–2013. [Google Scholar] [CrossRef]
- Kirkwood, J.; Zakharia, Y.; Davar, D.; Buchbinder, E.; Medina, T.; Daud, A.; Ribas, A.; Chmielowski, B.; Niu, J.; Gibney, G.; et al. 950 Final analysis: Phase 1b study investigating intratumoral injection of toll-like receptor 9 agonist vidutolimod ± pembrolizumab in patients with PD-1 blockade–refractory melanoma. J. Immunotherap. Cancer 2021, 9, A999. [Google Scholar] [CrossRef]
- Milhem, M.; Zakharia, Y.; Davar, D.; Buchbinder, E.; Medina, T.; Daud, A.; Ribas, A.; Niu, J.; Gibney, G.; Margolin, K.; et al. 304 Intratumoral injection of CMP-001, a toll-like receptor 9 (TLR9) agonist, in combination with pembrolizumab reversed programmed death receptor 1 (PD-1) blockade resistance in advanced melanoma. J. Immunotherap. Cancer 2020, 8, A331. [Google Scholar] [CrossRef]
- Zhao, Y.; Deng, J.; Rao, S.; Guo, S.; Shen, J.; Du, F.; Wu, X.; Chen, Y.; Li, M.; Chen, M.; et al. Tumor Infiltrating Lymphocyte (TIL) Therapy for Solid Tumor Treatment: Progressions and Challenges. Cancers 2022, 14, 4160. [Google Scholar] [CrossRef]
- Rohaan, M.W.; Van Den Berg, J.H.; Kvistborg, P.; Haanen, J.B.A.G. Adoptive Transfer of Tumor-Infiltrating Lymphocytes in Melanoma: A Viable Treatment Option. J. Immunother. Cancer 2018, 6, 102. [Google Scholar] [CrossRef]
- Škuciová, V.; Drahošová, S.; Výbohová, D.; Cígerová, V.; Adamkov, M. The Relationships between PD-L1 Expression, CD8+ TILs and Clinico-Histomorphological Parameters in Malignant Melanomas. Pathol. Res. Pract. 2020, 216, 153071. [Google Scholar] [CrossRef]
- Haanen, J.; Los, C.; Phan, G.Q.; Betof Warner, A. Adoptive Cell Therapy for Solid Tumors: Current Status in Melanoma and Next-Generation Therapies. Am. Soc. Clin. Oncol. Educ. Book 2024, 44, e431608. [Google Scholar] [CrossRef]
- Belete, T.M. The Current Status of Gene Therapy for the Treatment of Cancer. Biol. Targets Ther. 2021, 15, 67–77. [Google Scholar] [CrossRef]
- Tamura, R.; Miyoshi, H.; Yoshida, K.; Okano, H.; Toda, M. Recent Progress in the Research of Suicide Gene Therapy for Malignant Glioma. Neurosurg. Rev. 2021, 44, 29–49. [Google Scholar] [CrossRef]
- Duarte, S.; Carle, G.; Faneca, H.; de Lima, M.C.P.; Pierrefite-Carle, V. Suicide Gene Therapy in Cancer: Where Do We Stand Now? Cancer Lett. 2012, 324, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Oraee-Yazdani, S.; Tavanaei, R.; Rostami, F.; Hajarizadeh, A.; Mehrabadi, M.; Akhlaghpasand, M.; Tamaddon, M.; Khannejad, S.; Yazdani, K.O.; Zali, A. Suicide gene therapy using allogeneic adipose tissue-derived mesenchymal stem cell gene delivery vehicles in recurrent glioblastoma multiforme: A first-in-human, dose-escalation, phase I clinical trial. J. Transl. Med. 2023, 21, 350. [Google Scholar] [CrossRef]
- Thoidingjam, S.; Sriramulu, S.; Freytag, S.; Brown, S.L.; Kim, J.H.; Chetty, I.J.; Siddiqui, F.; Movsas, B.; Nyati, S. Oncolytic virus-based suicide gene therapy for cancer treatment: A perspective of the clinical trials conducted at Henry Ford Health. Transl. Med. Commun. 2023, 8, 11. [Google Scholar] [CrossRef]
- Anchan, A.; Finlay, G.; Angel, C.E.; Hucklesby, J.J.W.; Graham, S.E. Melanoma Mediated Disruption of Brain Endothelial Barrier Integrity Is Not Prevented by the Inhibition of Matrix Metalloproteinases and Proteases. Biosensors 2022, 12, 660. [Google Scholar] [CrossRef] [PubMed]
- Drucker, K.L.; Paulsen, A.R.; Giannini, C.; Decker, P.A.; Blaber, S.I.; Blaber, M.; Uhm, J.H.; O’Neill, B.P.; Jenkins, R.B.; Scarisbrick, I.A. Clinical Significance and Novel Mechanism of Action of Kallikrein 6 in Glioblastoma. Neuro. Oncol. 2013, 15, 305–318. [Google Scholar] [CrossRef]
- Liyanage, C.; Fernando, A.; Batra, J. Differential Roles of Protease Isoforms in the Tumor Microenvironment. Cancer Metastasis Rev. 2019, 38, 389–415. [Google Scholar] [CrossRef] [PubMed]
- Quesnel, A.; Karagiannis, G.S.; Filippou, P.S. Extracellular Proteolysis in Glioblastoma Progression and Therapeutics. Biochim. Biophys. Acta—Rev. Cancer 2020, 1874, 188428. [Google Scholar] [CrossRef] [PubMed]
- Bonturi, C.R.; Teixeira, A.B.S.; Rocha, V.M.; Valente, P.F.; Oliveira, J.R.; Filho, C.M.B.; Batista, I.F.C.; Oliva, M.L.V. Plant Kunitz Inhibitors and Their Interaction with Proteases: Current and Potential Pharmacological Targets. Int. J. Mol. Sci. 2022, 23, 4742. [Google Scholar] [CrossRef]
- Hellinger, R.; Gruber, C.W. Peptide-Based Protease Inhibitors from Plants. Drug Discov. Today 2019, 24, 1877–1889. [Google Scholar] [CrossRef]
- Nakahata, A.M.; Mayer, B.; Ries, C.; De Paula, C.A.A.; Karow, M.; Neth, P.; Sampaio, M.U.; Jochum, M.; Oliva, M.L.V. The Effects of a Plant Proteinase Inhibitor from Enterolobium Contortisiliquum on Human Tumor Cell Lines. Biol. Chem. 2011, 392, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Nakahata, A.M.; Mayer, B.; Neth, P.; Hansen, D.; Sampaio, M.U.; Oliva, M.V. Blocking the Proliferation of Human Tumor Cell Lines by Peptidase Inhibitors from Bauhinia Seeds. Planta Med. 2013, 79, 227–235. [Google Scholar] [CrossRef]
- Eatemadi, A.; Aiyelabegan, H.T.; Negahdari, B.; Mazlomi, M.A.; Daraee, H.; Daraee, N.; Eatemadi, R.; Sadroddiny, E. Role of Protease and Protease Inhibitors in Cancer Pathogenesis and Treatment. Biomed. Pharmacother. 2017, 86, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Erices, J.I.; Torres, Á.; Niechi, I.; Bernales, I.; Quezada, C. Current Natural Therapies in the Treatment against Glioblastoma. Phyther. Res. 2018, 32, 2191–2201. [Google Scholar] [CrossRef]
- Ding, K.; Jiang, W.; Jia, H.; Lei, M. Synergistically Anti-Multiple Myeloma Effects: Flavonoid, Non-Flavonoid Polyphenols, and Bortezomib. Biomolecules 2022, 12, 1647. [Google Scholar] [CrossRef]
- Gomes, M.T.R.; Oliva, M.L.; Lopes, M.T.P.; Salas, C.E. Plant proteinases and inhibitors: An overview of biological function and pharmacological activity. Curr. Protein Pept. Sci. 2011, 12, 417–436. [Google Scholar] [CrossRef]
- Poddar, N.; Maurya, S.; Saxena, V. Role of Serine Proteases and Inhibitors in Cancer. In Proteases in Physiology and Pathology; Chakraborti, S., Dhalla, N., Eds.; Springer: Singapore, 2017. [Google Scholar] [CrossRef]
- Rosso, M.; Fibbi, G.; Pucci, M.; D’Alessio, S.; Rosso, A.; Magnelli, L.; Chiarugi, V. Multiple pathways of cell invasion are regulated by multiple families of serine proteases. Clin. Exp. Metastasis 2004, 19, 193–207. [Google Scholar] [CrossRef]
- Bonturi, C.R.; Salu, B.R.; Bonazza, C.N.; Sinigaglia, R.C.; Rodrigues, T.; Alvarez-Flores, M.P.; Chudzinski-Tavassi, A.M.; Oliva, M.L.V. Proliferation and Invasion of Melanoma Are Suppressed by a Plant Protease Inhibitor, Leading to Downregulation of Survival/Death-Related Proteins. Molecules 2022, 27, 2956. [Google Scholar] [CrossRef] [PubMed]
- Lyu, P.; Ge, L.; Ma, R.; Wei, R.; McCrudden, C.; Chen, T.; Shaw, C.; Kwok, H. Identification and pharmaceutical evaluation of novel frog skin-derived serine proteinase inhibitor peptide–PE-BBI (Pelophylax esculentus Bowman-Birk inhibitor) for po-tential cancer treatment. Sci. Rep. 2018, 8, 14502. [Google Scholar] [CrossRef]
- Chen, X.; Chen, D.; Huang, L.; Chen, X.; Zhou, M.; Xi, X.; Ma, C.; Chen, T.; Wang, L. Target identification and modification of SL-BBI: A novel Bowman-Birk-type trypsin inhibitor from Sylvirana latouchii. Biomolecules 2020, 10, 1254. [Google Scholar] [CrossRef]
- Gitlin-Domagalska, A.; Maciejewska, A.; Dębowski, D. Inibidores de Bowman-Birk: Insights sobre a família de proteínas e peptídeos multifuncionais com potenciais aplicações terapêuticas. Pharmaceuticals 2020, 13, 421. [Google Scholar] [CrossRef]
- Sato, A.; Fonseca, I.; Nagamine, M.; Toledo, G.; Olio, R.; Hernandez-Blazquez, F.; Yano, T.; Yeh, E.; Dagli, M. Effects of al-pha-connexin carboxyl-terminal peptide (aCT1) and Bowman-Birk protease inhibitor (BBI) on canine oral mucosal mela-noma cells (OMM). Front. Vet. Sci. 2021, 8, 670451. [Google Scholar] [CrossRef] [PubMed]
- Shigetomi, H.; Onogi, A.; Kajiwara, H.; Yoshida, S.; Furukawa, N.; Haruta, S.; Tanase, Y.; Kanayama, S.; Noguchi, T.; Yamada, Y.; et al. Anti-inflammatory actions of Kunitz domain-containing serine protease inhibitors. Inflamm. Res. 2010, 59, 679–687. [Google Scholar] [CrossRef]
- Maria, D.; Will, S.; Bosch, R.; Souza, J.; Sciani, J.; Goldfeder, M.; Rondon, G.; Chudzinski-Tavassi, A. Preclinical evaluation of Amblyomin-X, a Kunitz-type protease inhibitor with antitumor activity. Toxicol. Rep. 2018, 6, 51–63. [Google Scholar] [CrossRef]
- Ranasinghe, S.; Rivera, V.; Boyle, G.; McManus, D. Kunitz-type protease inhibitor from dog tapeworm as a potential ther-apeutic for melanoma. Sci. Rep. 2019, 9, 16207. [Google Scholar] [CrossRef]
- Liu, Y.; Bian, Y.; Bai, Y.; Yu, S.; Tian, Y.; Li, J.; Li, S.; Li, T. Potato protease inhibitors, a functional food material with antioxidant and anticancer potential. Food Sci. Hum. Wellness 2023, 12, 1762–1771. [Google Scholar] [CrossRef]
- Pinto, C.; Aluai-Cunha, C.; Santos, A. Human and animal malignant melanoma: Comparative tumor models and the role of the microbiome in dogs and humans. Melanoma Res. 2023, 33, 87–103. [Google Scholar] [CrossRef]
- Zhou, Y.; Xia, J.; Xu, S.; She, T.; Zhang, Y.; Sun, Y.; Wen, M.; Jiang, T.; Xiong, Y.; Lei, J. Experimental mouse models for translational research of human cancer. Front. Immunol. 2023, 14, 1095388. [Google Scholar] [CrossRef] [PubMed]
- Saleh, J. Murine models of melanoma. Pathol. Res. Pract. 2018, 214, 1235–1238. [Google Scholar] [CrossRef] [PubMed]
- Patton, E.; Mitchell, D.; Nairn, R. Genetic and environmental models of melanoma in fish. Pigm. Cell Melanoma Res. 2010, 23, 314–337. [Google Scholar] [CrossRef] [PubMed]
- Roy, U.K.; Lavignac, N.; Rahman, A.M.; Nielsen, B.V. Purification of Lectin and Kunitz Trypsin Inhibitor from Soya Seeds. J. Chromatogr. Sci. 2018, 56, 436–442. [Google Scholar] [CrossRef] [PubMed]
- De Paula, C.A.A.; Coulson-Thomas, V.J.; Ferreira, J.G.; Maza, P.K.; Suzuki, E.; Nakahata, A.M.; Nader, H.B.; Sampaio, M.U.; Oliva, M.L.V. Enterolobium Contortisiliquum Trypsin Inhibitor (EcTI), a Plant Proteinase Inhibitor, Decreases in Vitro Cell Adhesion and Invasion by Inhibition of Src Protein-Focal Adhesion Kinase (FAK) Signaling Pathways. J. Biol. Chem. 2012, 287, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Lobo, Y.A.; Bonazza, C.; Batista, F.P.; Castro, R.A.; Bonturi, C.R.; Salu, B.R.; de Cassia Sinigaglia, R.; Toma, L.; Vicente, C.M.; Pidde, G.; et al. EcTI Impairs Survival and Proliferation Pathways in Triple-Negative Breast Cancer by Modulating Cell-Glycosaminoglycans and Inflammatory Cytokines. Cancer Lett. 2020, 491, 108–120. [Google Scholar] [CrossRef] [PubMed]
- Lie, K.C.M.; Bonturi, C.R.; Salu, B.R.; de Oliveira, J.R.; Bonini Galo, M.; Paiva, P.M.G.; Correia, M.T.D.S.; Oliva, M.L.V. Impairment of SK-MEL-28 Development—A Human Melanoma Cell Line—By the Crataeva Tapia Bark Lectin and Its Sequence-Derived Peptides. Int. J. Mol. Sci. 2023, 24, 10617. [Google Scholar] [CrossRef]
- Zhang, F.; Walcott, B.; Zhou, D.; Gustchina, A.; Lasanajak, Y.; Smith, D.F.; Ferreira, R.S.; Correia, M.T.S.; Paiva, P.M.G.; Bovin, N.V.; et al. Structural Studies of the Interaction of Crataeva Tapia Bark Protein with Heparin and Other Glycosaminoglycans. Biochemistry 2013, 52, 2148–2156. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| TNM Classification 1 | Description |
|---|---|
| Primary staging of melanoma | |
| Tis | Melanoma in situ—The melanoma is confined to the outermost layer of the skin (epidermis) and has not invaded the basal layer. Also called carcinoma in situ. |
| T1 | The tumor is thin, usually less than 1 mm thick. May or may not have ulcerated. |
| T2 | The tumor is of moderate thickness, 1 to 2 mm in depth. It may or may not have ulcerated. |
| T3 | The tumor is thicker, 2 to 4 mm deep. It may or may not have ulcerated. |
| T4 | The tumor is very thick, over 4 mm deep. It may or may not have ulcerated. |
| Melanoma staging for regional lymph nodes | |
| N0 | There is no evidence of regional lymph node metastasis. |
| N1 | The melanoma has spread to a nearby lymph node but is micrometastasized (can only be detected with a microscope, cannot be seen or felt). |
| N2 | The melanoma has spread to nearby lymph nodes and is considered macrometastatic metastasis (can be seen or felt). |
| N3 | The melanoma has spread to nearby or distant lymph nodes, being multiple, grouped or with extranodal growth. |
| Metastatic Melanoma | |
| M0 | There is no evidence of distant metastasis. |
| M1 | The melanoma has spread to other parts of the body beyond the primary tumor area and regional lymph nodes. |
| Protease Inhibitor: Bowman-Birk Inhibitors (BBI) | |
|---|---|
| Source | Soybean (Glycine max) and other legumes. |
| Type of protease inhibited | Serine proteases (trypsin and chymotrypsin). |
| Biological effects | Inhibits cell proliferation and induce apoptosis in tumor cells. Demonstrates anticancer, anti-inflammatory, and antioxidant properties. Protects against oxidative damage and inflammation and may help prevent cancers such as melanoma. |
| Research status | Studied in preclinical and early clinical models; showed efficacy in reducing tumor growth and cell protection. |
| References | Lyu et al. [177]; Chen et al. [178]; Gitlin-Domagalska et al. [179]; Sato et al. [180]. |
| Protease Inhibitor: Soybean Trypsin Inhibitor (Kunitz-Type) | |
| Source | Soybean (Glycine max) and other legumes. |
| Type of protease inhibited | Serine proteases (trypsin and chymotrypsin). |
| Biological effects | Reduces tumoral cell proliferation and blocks cell invasion, especially in melanoma cells. Affects angiogenesis, decreasing the formation of blood vessels that feed tumors. |
| Research status | In vitro and in vivo studies demonstrate efficacy in reducing melanoma cell growth. |
| References | Shigetomi et al. [181]; Maria et al. [182]; Ranasinghe et al. [183]. |
| Protease Inhibitor: Potato Trypsin Inhibitor | |
| Source | Potato (Solanum tuberosum). |
| Type of protease inhibited | Serine protease (trypsin). |
| Biological effects | Affects cell cycle regulation, inhibiting cancer cell growth. Reduces tumoral metastasis and invasion in melanoma models by stabilizing the extracellular matrix. Demonstrates anti-inflammatory properties, which may be useful in autoimmune diseases. |
| Research status | Promising results in laboratory studies and animal model. Focused on formulation for clinical use. |
| References | Liu et al. [184] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boleti, A.P.D.A.; Jacobowski, A.C.; Monteiro-Alfredo, T.; Pereira, A.P.R.; Oliva, M.L.V.; Maria, D.A.; Macedo, M.L.R. Cutaneous Melanoma: An Overview of Physiological and Therapeutic Aspects and Biotechnological Use of Serine Protease Inhibitors. Molecules 2024, 29, 3891. https://doi.org/10.3390/molecules29163891
Boleti APDA, Jacobowski AC, Monteiro-Alfredo T, Pereira APR, Oliva MLV, Maria DA, Macedo MLR. Cutaneous Melanoma: An Overview of Physiological and Therapeutic Aspects and Biotechnological Use of Serine Protease Inhibitors. Molecules. 2024; 29(16):3891. https://doi.org/10.3390/molecules29163891
Chicago/Turabian StyleBoleti, Ana Paula De Araújo, Ana Cristina Jacobowski, Tamaeh Monteiro-Alfredo, Ana Paula Ramos Pereira, Maria Luiza Vilela Oliva, Durvanei Augusto Maria, and Maria Lígia Rodrigues Macedo. 2024. "Cutaneous Melanoma: An Overview of Physiological and Therapeutic Aspects and Biotechnological Use of Serine Protease Inhibitors" Molecules 29, no. 16: 3891. https://doi.org/10.3390/molecules29163891