The Effect of Postoperative Hyperbaric Oxygen Treatment on Intra-Abdominal Adhesions in Rats

Abstract
:1. Introduction
2. Results and Discussion
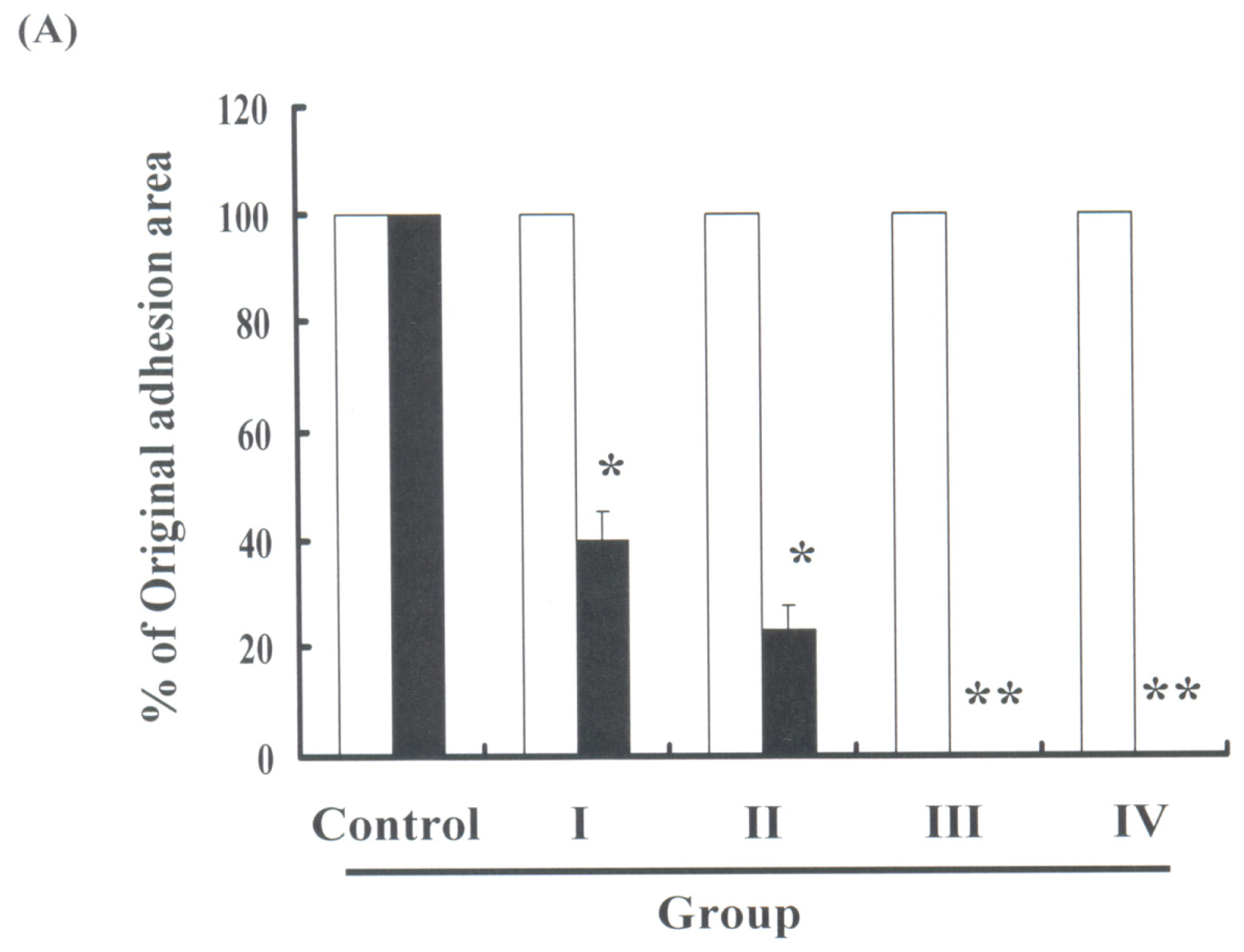
2.1. HBO Therapy Reduced Adhesion Formation
3. Experimental Section
3.1. Animal Methods
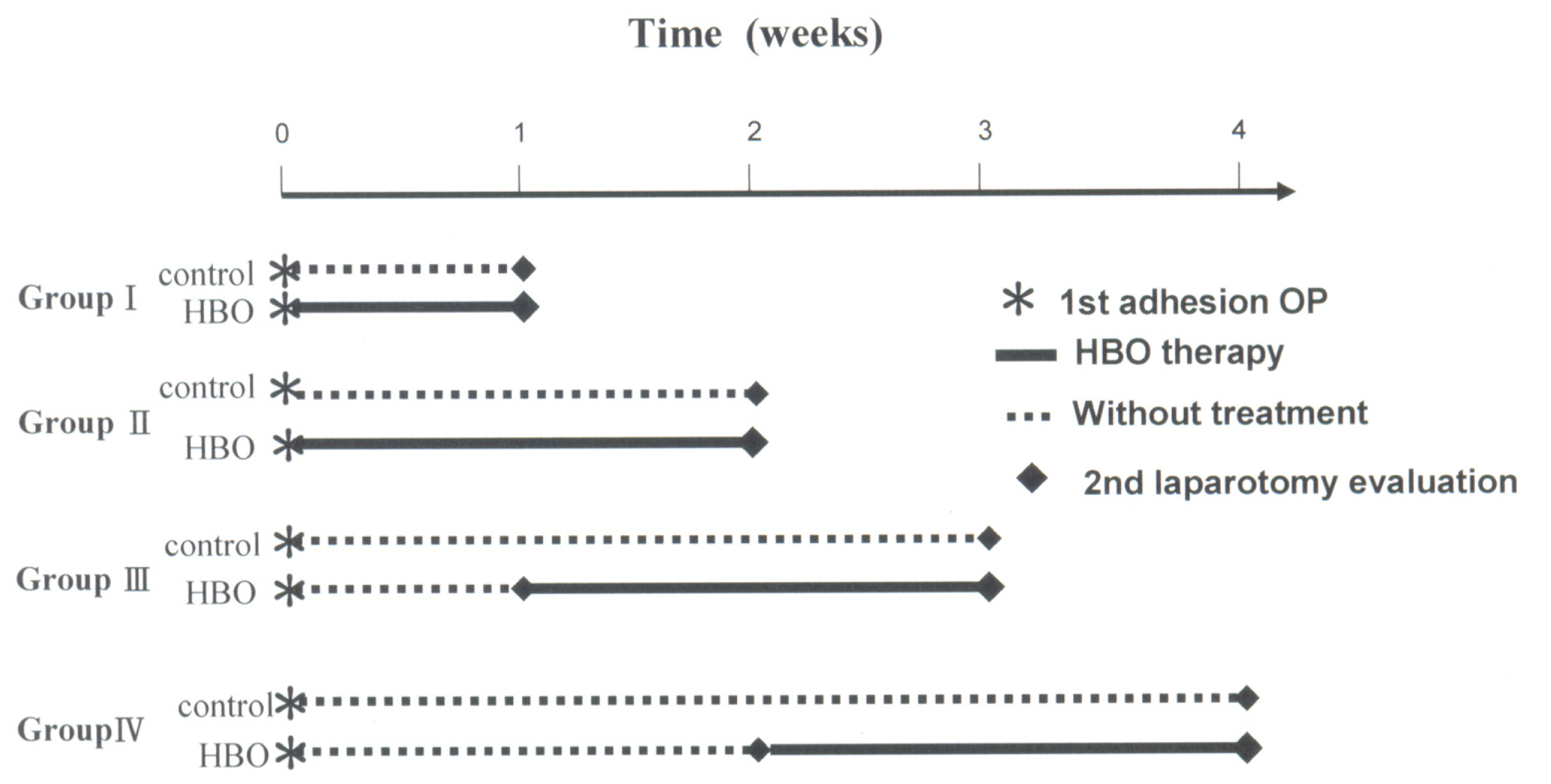
3.2. HBO Therapy Models
3.3. Evaluating Adhesion Formation
3.4. Quantification of Intra-Abdominal Adhesions
3.5. Statistical Analysis
4. Conclusions
References
- Menzies, D.; Ellis, H. Intestinal obstruction from adhesion—How big is the problem? Ann. R. Coll. Surg. Engl 1990, 72, 60–63. [Google Scholar]
- Tinelli, A.; Malvasi, A.; Guido, M.; Tsin, D.A.; Hudelist, G.; Stark, M.; Mettler, L. Laparoscopy entry in patients with previous abdominal and pelvic surgery. Surg. Innov 2011, 18, 201–205. [Google Scholar]
- Buttenschoen, K.; Fathimani, K.; Buttenschoen, D.C. Effect of major abdominal surgery on the host immune response to infection. Curr. Opin. Infect. Dis 2010, 23, 259–267. [Google Scholar]
- Schwemmle, K. Causes for adhesions in the abdomen (in German). Langenbecks. Arch. Chir. Suppl. II Verh. Dtsch. Ges. Chir 1990, 1017–1021. [Google Scholar]
- Rajab, T.K.; Ahmad, U.N.; Kelly, E. Implications of late complications from adhesions for preoperative informed consent. J. R. Soc. Med 2010, 103, 317–321. [Google Scholar]
- Imai, A.; Suzuki, N. Topical non-barrier agents for postoperative adhesion prevention in animal models. Eur. J. Obstet. Gynecol. Reprod. Biol 2010, 149, 131–135. [Google Scholar]
- Awonuga, A.O.; Fletcher, N.M.; Saed, G.M.; Diamond, M.P. Postoperative adhesion development following cesarean and open intra-abdominal gynecological operation: A review. Reprod. Sci 2011, 18, 1166–1185. [Google Scholar]
- Brochhausen, C.; Schmitt, V.H.; Rajab, T.K.; Planck, C.N.; Krämer, B.; Wallwiener, M.; Hierlemann, H.; Kirkpatrick, C.J. Intraperitoneal adhesions—An ongoing challenge between biomedical engineering and the life sciences. J. Biomed. Mater. Res. A 2011, 98, 143–156. [Google Scholar]
- Gago, L.A.; Saed, G.M.; Chauhan, S.; Elhammady, E.F.; Diamond, M.P. Seprafilm (modified hyaluronic acid and carboxymethylcellulose) acts as a physical barrier. Fertil. Steril 2003, 80, 612–616. [Google Scholar]
- Darmas, B. Use of barrier products in the prevention of adhesion formation following surgery. J. Wound Care 2008, 17, 405–411. [Google Scholar]
- Eroglu, A.; Demirci, S.; Kurtman, C.; Akbay, A.; Eroglu, N. Prevention of intra-abdominal adhesions by using Seprafilm in rats undergoing bowel resection and radiation therapy. Colorectal Dis 2001, 3, 33–37. [Google Scholar]
- Kece, C.; Yildiz, F.; Simsek, A.; Ozer, M.T.; Deveci, S.; Ozgurtas, T.; Sadir, S.; Korkmaz, A.; Korkmaz, O.; Ersoz, N.; et al. Synergistic effects of hyperbaric oxygen and granulocytecolony stimulating factor on postoperative adhesion formation in a rat cecal abrasion model. Bratisl. Lek. Listy 2010, 111, 115–120. [Google Scholar]
- Buras, J. Basic mechanisms of hyperbaric oxygen in the treatment of ischemia-reperfusion injury. Int. Anesthesiol. Clin 2000, 38, 91–109. [Google Scholar]
- Liakakos, T.; Thomakos, N.; Fine, P.M.; Dervenis, C.; Young, R.L. Peritoneal adhesions: Etiology, pathophysiology, and clinical significance. Recent advances in prevention and management. Dig. Surg 2001, 18, 260–273. [Google Scholar]
- Chegini, N.; Rong, H.; Bennett, B.; Stone, I.K. Peritoneal fluid cytokine and eicosanoid levels and their relation to the incidence of peritoneal adhesion. J. Soc. Gynecol. Invest 1999, 6, 153–157. [Google Scholar]
- Lauder, C.I.; Garcea, G.; Strickland, A.; Maddern, G.J. Abdominal adhesion prevention: Still a sticky subject? Dig. Surg 2010, 27, 347–358. [Google Scholar]
- Aysan, E.; Bektas, H.; Ersoz, F. A new approach to postoperative peritoneal adhesions: Prevention of peritoneal trauma by aloe vera gel. Eur. J. Obstet. Gynecol. Reprod. Biol 2010, 149, 195–198. [Google Scholar]
- Paulo, N.M.; Malmonge, S.M.; Menezes, L.B.; Lima, F.G.; Faria, A.M.; Andrasckho, M.M.; Moreira, N.M.; Atayde, I.B.; Silva, M.S. Evaluation of peritoneal adhesions formation and tissue response to polypropylene-poli (2-hydroxyethyl methacrylate)-(polyHEMA) implant on rats’ abdominal wall. Acta Cir. Bras 2010, 25, 337–341. [Google Scholar]
- Binnebösel, M.; Klink, C.D.; Grommes, J.; Jansen, M.; Neumann, U.P.; Junge, K. Influence of small intestinal serosal defect closure on leakage rate and adhesion formation: a pilot study using rabbit models. Langenbecks. Arch Surg 2011, 396, 133–137. [Google Scholar]
- DiZerega, G.S. Contemporary adhesion prevention. Fertil. Steril 1994, 61, 219–235. [Google Scholar]
- Uzunköy, A.; Akinci, O.F.; Coskun, A.; Aslan, O.; Kocyigit, A. Effects of antiadhesive agents on the healing of intestinal anastomosis. Dis. Colon. Rectum 2000, 43, 370–375. [Google Scholar]
- Ambiru, S.; Furuyama, N.; Kimura, F.; Shimizu, H.; Yoshidome, H.; Miyazaki, M.; Ochiai, T. Effect of hyperbaric oxygen therapy on patients with adhesive intestinal obstruction associated with abdominal surgery who have failed to respond to more than 7 days of conservative treatment. Hepatogastroenterology 2008, 55, 491–495. [Google Scholar]
- Marshall, G.T.; Thirlby, R.C.; Bredfeldt, J.E.; Hampson, N.B. Treatment of gastrointestinal radiation injury with hyperbaric oxygen. Undersea Hyperb. Med 2007, 34, 35–42. [Google Scholar]
- Nair, S.K.; Bhat, I.K.; Aurora, A.L. Role of proteolytic enzyme in the prevention of postoperative intraperitoneal adhesions. Arch. Surg 1974, 108, 849–853. [Google Scholar]
- Gimbel, M.L.; Chelius, D.; Hunt, T.K.; Spencer, E.M. A novel approach to reducing postoperative intraperitoneal adhesions through the inhibition of insulinlike growth factor I activity. Arch. Surg 2001, 136, 311–317. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Condition |
|---|---|
| A | Room air, 1 ATA group (Control) |
| B | 100% O2 1 ATA group (A pressure of 1 ATA with 100% O2) |
| C | 100% O2 2.5 ATA group (A pressure of 2.5 ATA with 100% O2) |
| D | 20% O2, 80% N2, 2.5 ATA group (The mix air included 20% O2, 80% N2 with a pressure of 2.5 ATA) |
| E | 8% O2, 92% N2, 2.5 ATA group (The mix air included 8% O2, 92% N2 with a pressure of 2.5 ATA) |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chen, M.-J.; Chen, T.-Y.; Cheng, Y.-M.; Hsu, Y.-C. The Effect of Postoperative Hyperbaric Oxygen Treatment on Intra-Abdominal Adhesions in Rats. Int. J. Mol. Sci. 2012, 13, 12224-12231. https://doi.org/10.3390/ijms131012224
Chen M-J, Chen T-Y, Cheng Y-M, Hsu Y-C. The Effect of Postoperative Hyperbaric Oxygen Treatment on Intra-Abdominal Adhesions in Rats. International Journal of Molecular Sciences. 2012; 13(10):12224-12231. https://doi.org/10.3390/ijms131012224
Chicago/Turabian StyleChen, Ming-Jenn, Tzu-Yu Chen, Ya-Min Cheng, and Yi-Chiang Hsu. 2012. "The Effect of Postoperative Hyperbaric Oxygen Treatment on Intra-Abdominal Adhesions in Rats" International Journal of Molecular Sciences 13, no. 10: 12224-12231. https://doi.org/10.3390/ijms131012224
APA StyleChen, M.-J., Chen, T.-Y., Cheng, Y.-M., & Hsu, Y.-C. (2012). The Effect of Postoperative Hyperbaric Oxygen Treatment on Intra-Abdominal Adhesions in Rats. International Journal of Molecular Sciences, 13(10), 12224-12231. https://doi.org/10.3390/ijms131012224