Improved Bonding of Partially Osteomyelitic Bone to Titanium Pins Owing to Biomimetic Coating of Apatite

Abstract
:1. Introduction
2. Results
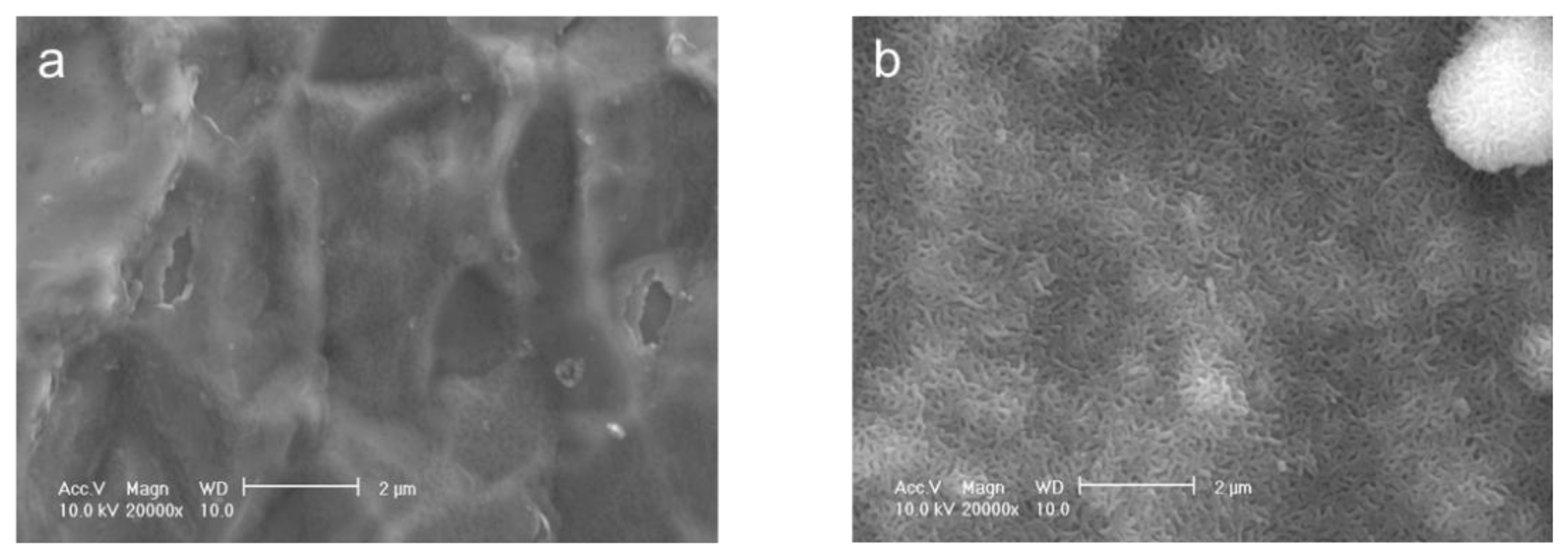
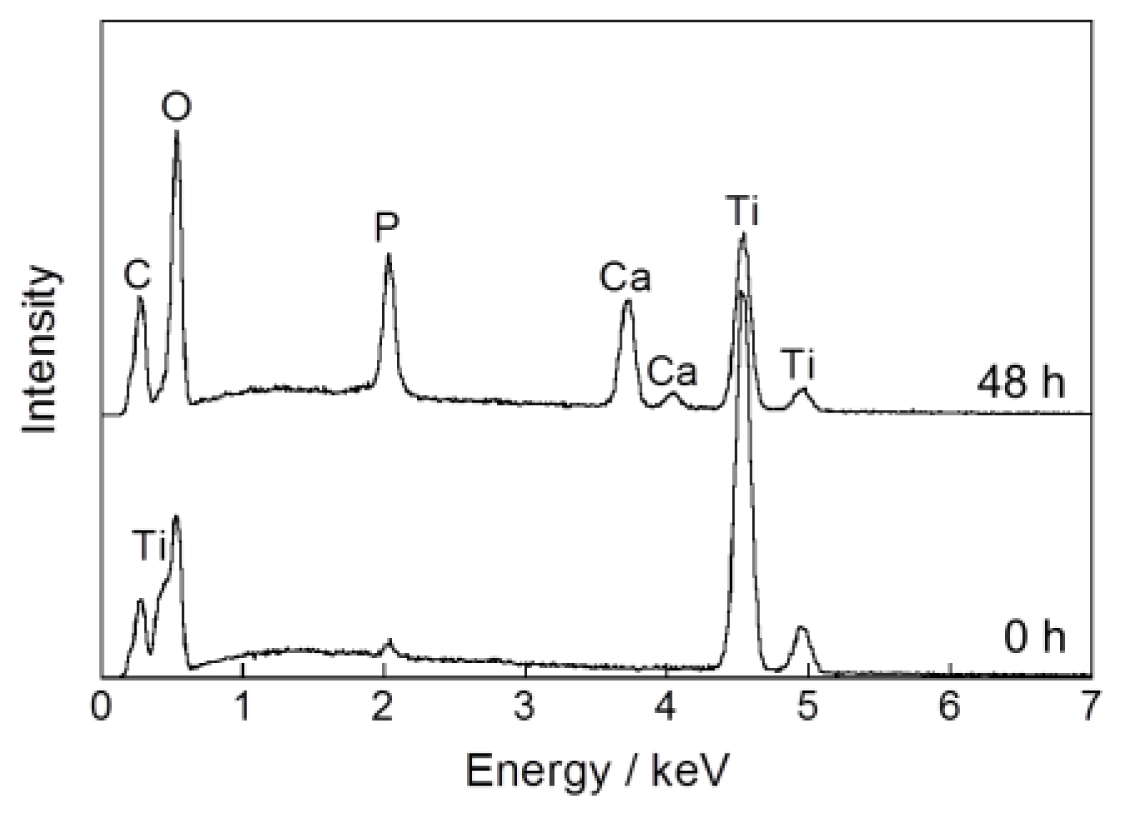
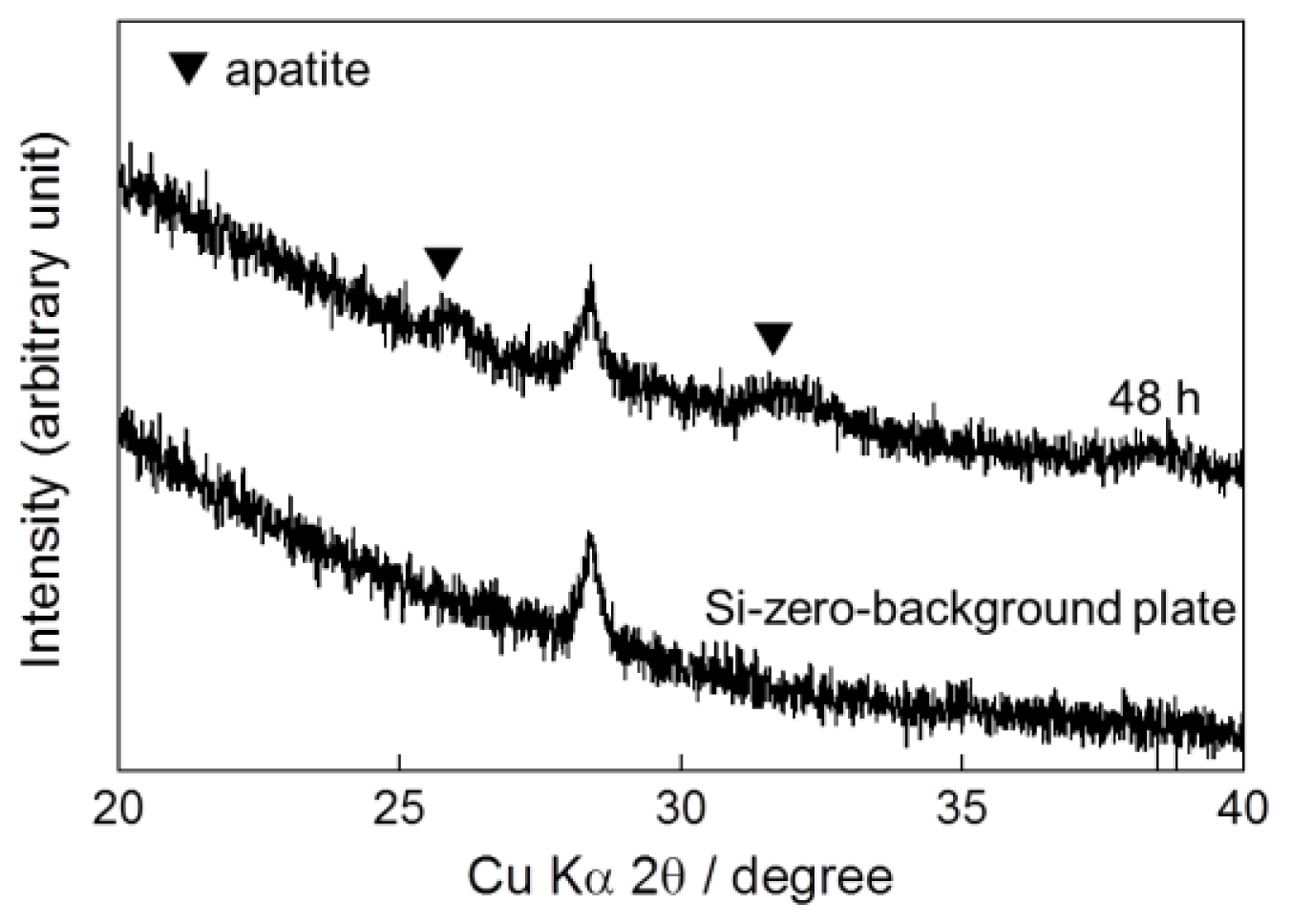
2.1. One-Step Formation of Apatite Coating on Ti Pins at 25 °C
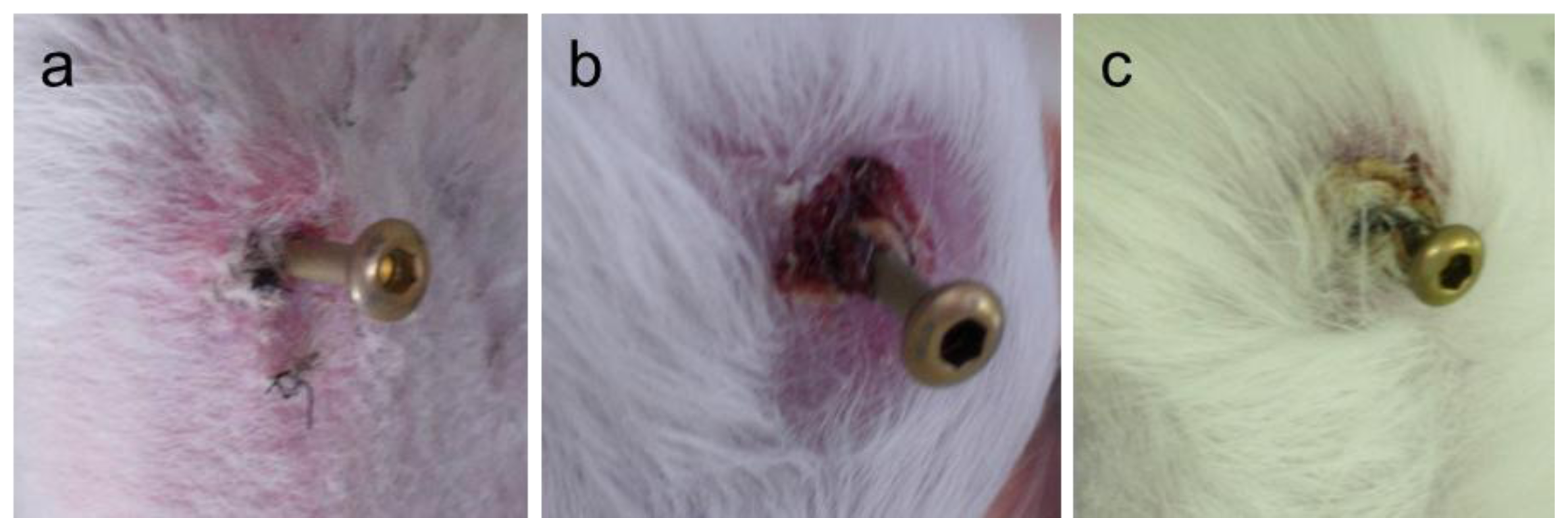
2.2. Classification of Pin-Tract Infections by Visual Inspection
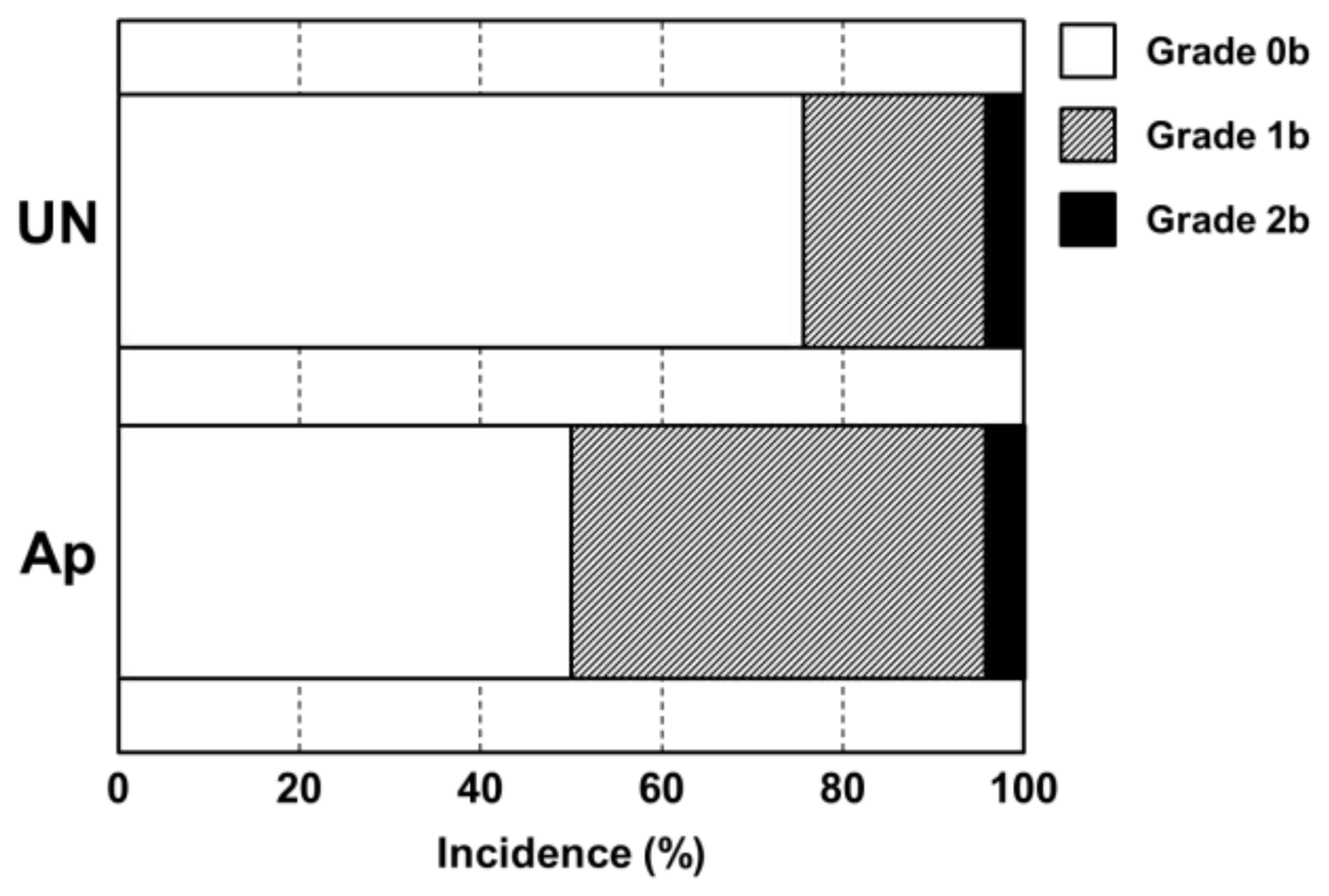
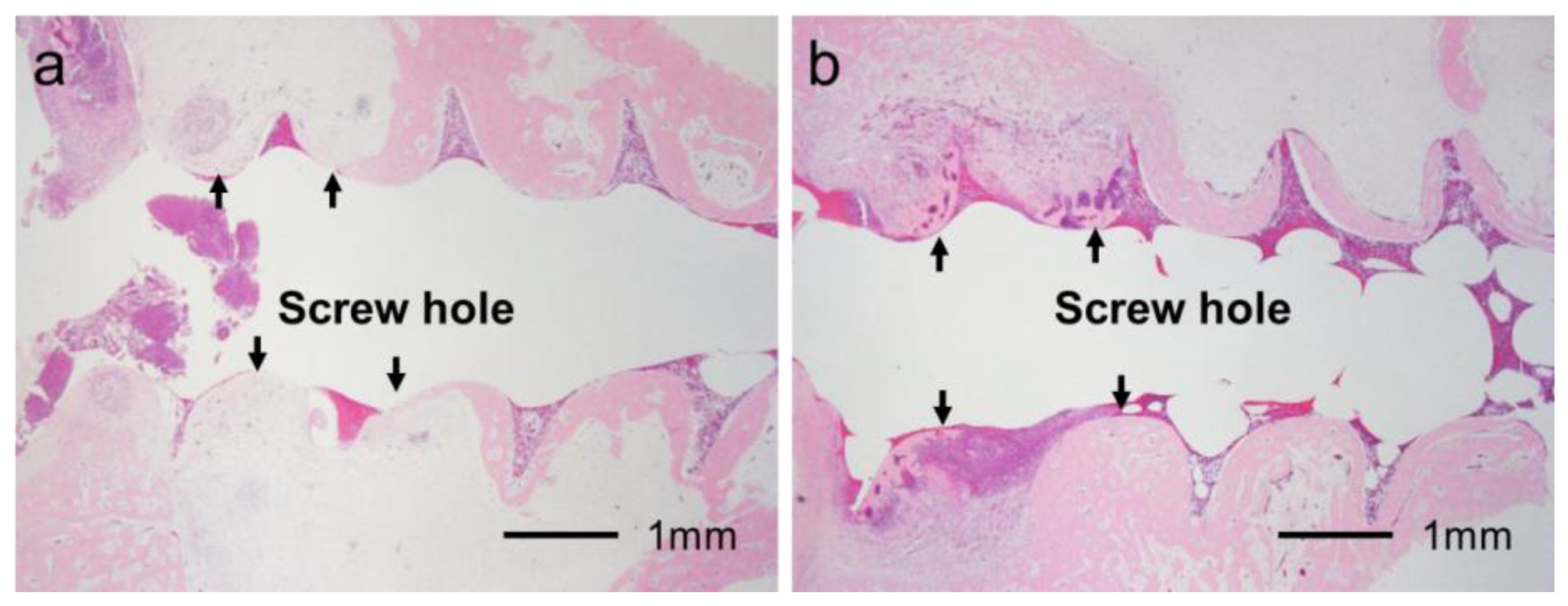
2.3. Classification of Inflammation Grade by Histological Observation
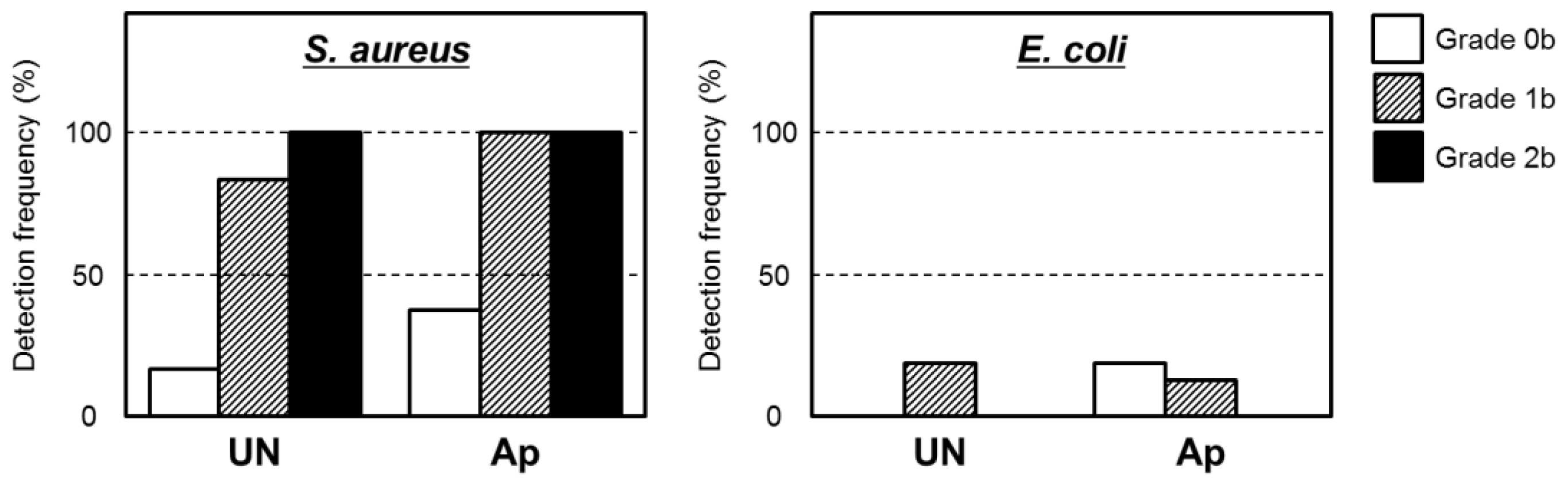
2.4. Bacterial Identification in Pin Tracts
2.5. Extraction Torque
3. Discussion
4. Materials and Methods
4.1. Preparation of an Infusion Fluid-Based Supersaturated CaP Solution
4.2. Immersion of Ti Pins in the Supersaturated CaP Solution
4.3. Characterization of the Surface Layer
4.4. Animal Experiments
4.5. Classification of Pin Tract Infections by Visual Inspection
4.6. Histological Analysis
4.7. Reanalysis of Osteomyelitis Status and Extraction Torque Data
4.8. Bacterial Culture and Identification
4.9. Biomechanical Analysis
5. Conclusions
Conflicts of Interest
References
- Mahan, J.; Seligson, D.; Henry, S.L.; Hynes, P.; Dobbins, J. Factors in pin tract infections. Orthopedics 1991, 14, 305–308. [Google Scholar]
- Sims, M.; Saleh, M. External fixation—The incidence of pin site infection: Aprospective audit. J. Orthop. Nurs 2000, 4, 59–63. [Google Scholar]
- Parameswaran, A.D.; Roberts, C.S.; Seligson, D.; Voor, M. Pin tract infection with contemporary external fixation: How much of a problem? J. Orthop. Trauma 2003, 17, 503–507. [Google Scholar]
- Rafique, A.; Ghani, S.; Sadiq, M.; Siddiqui, I.A. Kirschner wire pin tract infection rates between percutaneous and buried wires in treating metacarpal and phalangeal fractures. J. Coll. Phys. Surg. Pakistan 2006, 16, 518–520. [Google Scholar]
- Zlowodzki, M.; Prakash, J.S.; Aggerwal, N.K. External fixation of complex femoral shaft fracture. Int. Orthop 2007, 31, 409–413. [Google Scholar]
- Schalamon, J.; Petnehazy, T.; Ainoedhofer, H.; Zwick, E.B.; Singer, G.; Hoellwarth, M.E. Pin tract infection with external fixation of pediatric fractures. J. Pediatr. Surg 2007, 42, 1584–1587. [Google Scholar]
- W-Dahl, A.; Toksvig-Larsen, S. No clinical benefits using a new design of pins for external fixation: A randomized study in 50 patients operated on by the hemicallotasis technique. Arch. Orthop. Trauma Surg 2008, 128, 661–667. [Google Scholar]
- Green, S.A.; Ripley, M.J. Chronic osteomyelitis in pin tracks. J. Bone Joint Surg. Am 1984, 66, 1092–1098. [Google Scholar]
- Saithna, A. The influence of hydroxyApatite coating of external fixator pins on pin loosening and pin tract in fection: A systematic review. Injury 2010, 41, 128–132. [Google Scholar]
- Moroni, A.; Heikkila, J.; Magyar, G.; Toksvig-Larsen, S.; Giannini, S. Fixation strength and pin tract infection of hydroxyapatite-coated tapered pins. Clin. Ortop. Relat. Res 2001, 388, 209–217. [Google Scholar]
- Moroni, A.; Cadossi, M.; Romagnoli, M.; Faldini, C.; Giannini, S. A biomechanical and histological analysis of standard versus hydroxyApatite-coated pins for external fixation. J. Biomed. Mater. Res. B 2008, 86, 417–421. [Google Scholar]
- Pizà, G.; Caja, V.L.; González-Viejo, M.A.; Navarro, A. HydroxyApatite-coated external-fixation pins. The effect on pin loosening and pin-track infection in leg lengthening for short stature. J. Bone Joint Surg. Br 2004, 86, 892–897. [Google Scholar]
- Placzek, R.; Ruffer, M.; Deuretzbacher, G.; Heijens, E.; Meiss, A.L. The fixation strength of hydroxyApatite-coated Schanz screws and standard stainless steel Schanz screws in lower extremity lengthening: A comparison based on a new torque value index: The fixation index. Arch. Orthop. Trauma Surg 2006, 126, 369–373. [Google Scholar]
- Pieske, O.; Kaltenhauser, F.; Pichlmaier, L.; Schramm, N.; Trentzsch, H.; Löffler, T.; Greiner, A.; Piltz, S. Clinical benefit of hydroxyApatite-coated pins compared with stainless steel pins in external fixation at the wrist: A randomised prospective study. Injury 2010, 41, 1031–1036. [Google Scholar]
- Mutsuzaki, H.; Ito, A.; Sakane, M.; Sogo, Y.; Oyane, A.; Ebihara, Y.; Ichinose, N.; Ochiai, N. Calcium phosphate coating formed in infusion fluid mixture to enhance fixation strength of titanium screws. J. Mater. Sci 2007, 18, 1799–1808. [Google Scholar]
- Mutsuzaki, H.; Ito, A.; Sakane, M.; Sogo, Y.; Oyane, A.; Ochiai, N. FGF-2-apatite composite layers on titanium screws to reduce pin tract infection rate. J. Biomed. Mater. Res. B 2008, 86, 365–374. [Google Scholar]
- Chiono, V.; Gentile, P.; Boccafoschi, F.; Carmagnola, I.; Ninov, M.; Georgieva, V.; Georgiev, G.; Ciardelli, G. Photoactive chitosan switching on bone-like apatite deposition. Biomacromolecules 2010, 11, 309–315. [Google Scholar]
- Oyane, A. Development of apatite-based composites by a biomimetic process for biomedical applications. J. Ceram. Soc. Jpn 2010, 118, 77–81. [Google Scholar]
- Oyane, A.; Wang, X.P.; Sogo, Y.; Ito, A.; Tsurushima, H. Calcium phosphate composite layers for surface-mediated gene transfer. Acta Biomater 2012, 8, 2034–2046. [Google Scholar]
- Li, X.; Wang, X.P.; Ito, A.; Sogo, Y.; Cheng, K.; Oyane, A.; Yamazaki, A. Effect of coprecipitation temperature on the properties and activity of fibroblast growth factor-2 apatite composite layer. Mater. Sci. Eng. C 2009, 29, 216–221. [Google Scholar]
- Sogo, Y.; Ito, A.; Onoguchi, M.; Oyane, A.; Tsurushima, H.; Ichinose, N. Formation of FGF-2 and calcium phosphate composite layer on hydroxyapatite ceramic for promoting bone formation. Biomed. Mater 2007, 2, S175–S180. [Google Scholar]
- LeGeros, R.Z. Apatites in biological systems. Prog. Cryst. Growth Charact 1981, 4, 1–45. [Google Scholar]
- Zablotsky, M.H. Hydroxyapatite coatings in implant dentistry. Implant Dent 1992, 1, 253–257. [Google Scholar]
- Piattelli, A.; Cosci, F.; Scarano, A.; Trisi, P. Localized chronic suppurative bone infection as a sequel of peri-implantitis in a hydroxyapatite-coated dental implant. Biomaterials 1995, 16, 917–920. [Google Scholar]
- Mutsuzaki, H.; Oyane, A.; Sogo, Y.; Sakane, M.; Ito, A. Cefazolin-containing poly(ɛ-caprolactone) sponge pad to reduce the pin tract infection rate in rabbits. Asia Pac. Sports Med. Arthrosc. Rehabil. Technol 2013, in press. [Google Scholar]
- Yildirim, O.S.; Aksakal, B.; Celik, H.; Vangolu, Y.; Okur, A. An investigation of the effects of hydroxyapatite coatings on the fixation strength of cortical screws. Med. Eng. Phys 2005, 27, 221–228. [Google Scholar]
- Savarino, L.; Stea, S.; Granchi, D.; Donati, M.E.; Cervellati, M.; Moroni, A.; Paganetto, G.; Pizzoferrato, A. X-ray diffraction of bone at the interface with hydroxyApatite-coated versus uncoated metal implants. J. Mater. Sci 1998, 9, 109–115. [Google Scholar]
- Elliot, J.C. Hydroxyapatite and Nonstoichiometric Apatites. In Structure and Chemistry of the Apatites and Other Calcium Orthophosphates. Studies in Inorganic Chemistry 18, 2nd Ed ed; Elsevier: Amsterdam, The Netherlands, 1994; Volume 18, pp. 111–190. [Google Scholar]
- Mutsuzaki, H.; Ito, A.; Sogo, Y.; Sakane, M.; Oyane, A.; Ochiai, N. Enhanced wound healing associated with Sharpey’s fiber-like tissue formation around FGF-2-apatite composite layers on percutaneous titanium screws in rabbits. Arch. Orthop. Trauma Surg 2012, 132, 113–121. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bacteria | UN (%) | Ap (%) |
|---|---|---|
| S. aureus | 35 | 65 |
| S. epidermidis | 0 | 5 |
| S. auricularis | 60 | 20 |
| Corynebacterium sp. | 20 | 0 |
| E. coli | 5 | 15 |
| GNF-GNR * | 20 | 5 |
| No bacteria | 0 | 5 |
| Chemical components | Present study (mM) | Previous study (mM) [15] |
|---|---|---|
| Na+ | 147.23 | 138.87 |
| K+ | 9.92 | 7.39 |
| Ca2+ | 8.92 | 3.67 |
| Mg2+ | 0.24 | 0.22 |
| Cl− | 153.46 | 134.39 |
| H2PO4− | 2.97 | 1.83 |
| HCO3− | 15.09 | 15.09 |
| CH3COO− | 1.9 | 1.8 |
| xylitol | 31.65 | 29.93 |
© 2013 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Mutsuzaki, H.; Sogo, Y.; Oyane, A.; Ito, A. Improved Bonding of Partially Osteomyelitic Bone to Titanium Pins Owing to Biomimetic Coating of Apatite. Int. J. Mol. Sci. 2013, 14, 24366-24379. https://doi.org/10.3390/ijms141224366
Mutsuzaki H, Sogo Y, Oyane A, Ito A. Improved Bonding of Partially Osteomyelitic Bone to Titanium Pins Owing to Biomimetic Coating of Apatite. International Journal of Molecular Sciences. 2013; 14(12):24366-24379. https://doi.org/10.3390/ijms141224366
Chicago/Turabian StyleMutsuzaki, Hirotaka, Yu Sogo, Ayako Oyane, and Atsuo Ito. 2013. "Improved Bonding of Partially Osteomyelitic Bone to Titanium Pins Owing to Biomimetic Coating of Apatite" International Journal of Molecular Sciences 14, no. 12: 24366-24379. https://doi.org/10.3390/ijms141224366
APA StyleMutsuzaki, H., Sogo, Y., Oyane, A., & Ito, A. (2013). Improved Bonding of Partially Osteomyelitic Bone to Titanium Pins Owing to Biomimetic Coating of Apatite. International Journal of Molecular Sciences, 14(12), 24366-24379. https://doi.org/10.3390/ijms141224366