Treatment of Single or Multiple Brain Metastases by Hypofractionated Stereotactic Radiotherapy Using Helical Tomotherapy

Abstract
:
1. Introduction
2. Results
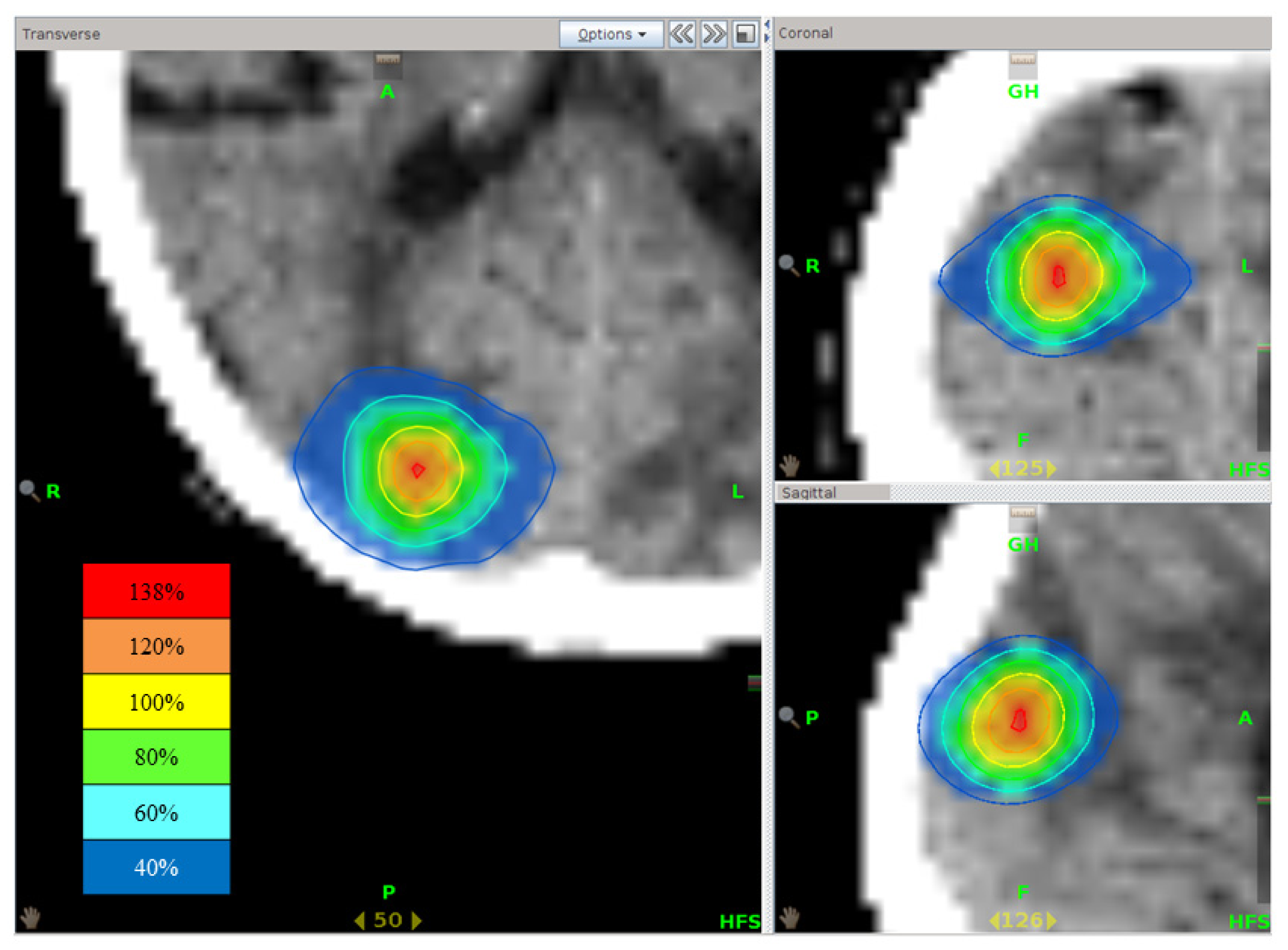
2.1. Treatment Plan Analysis
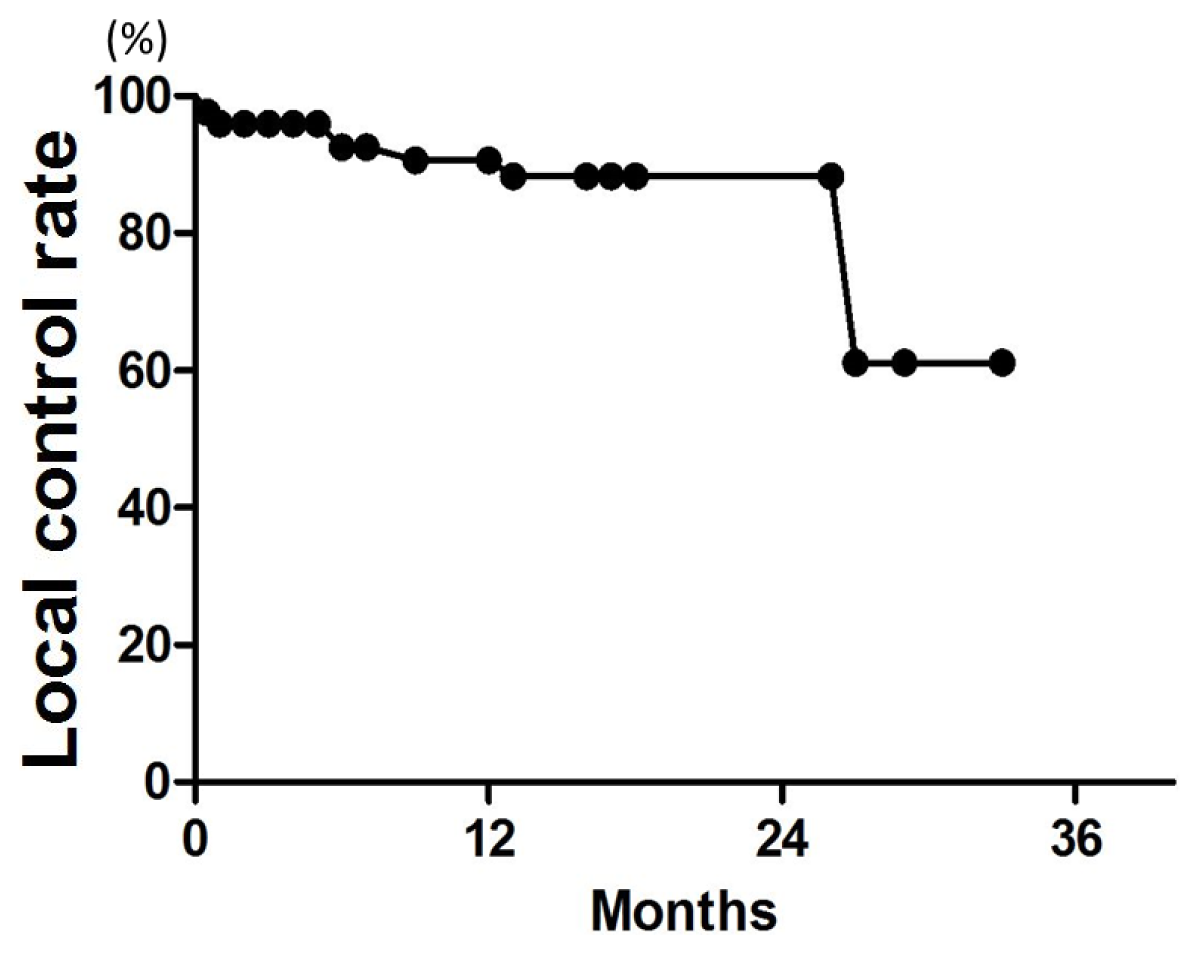
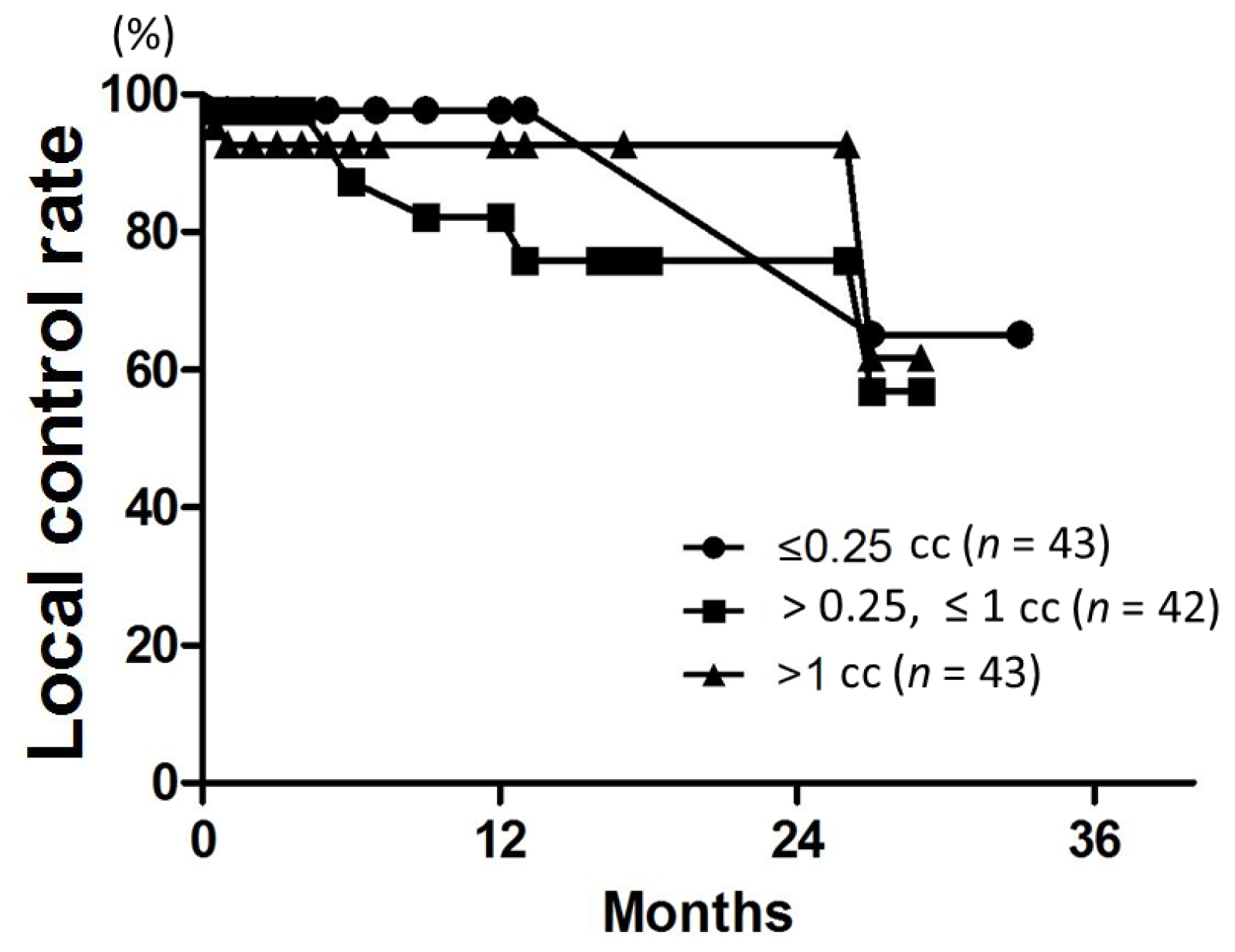
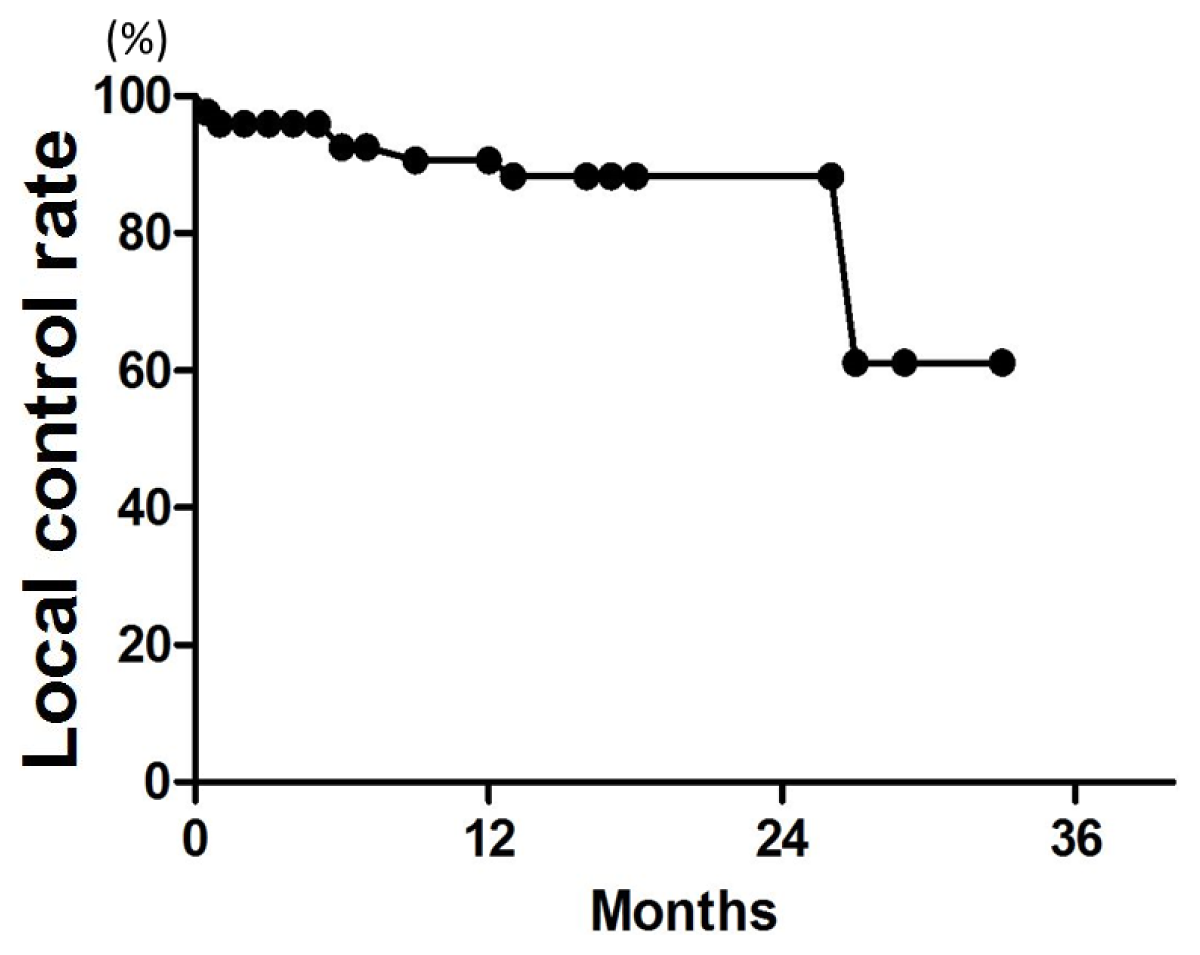
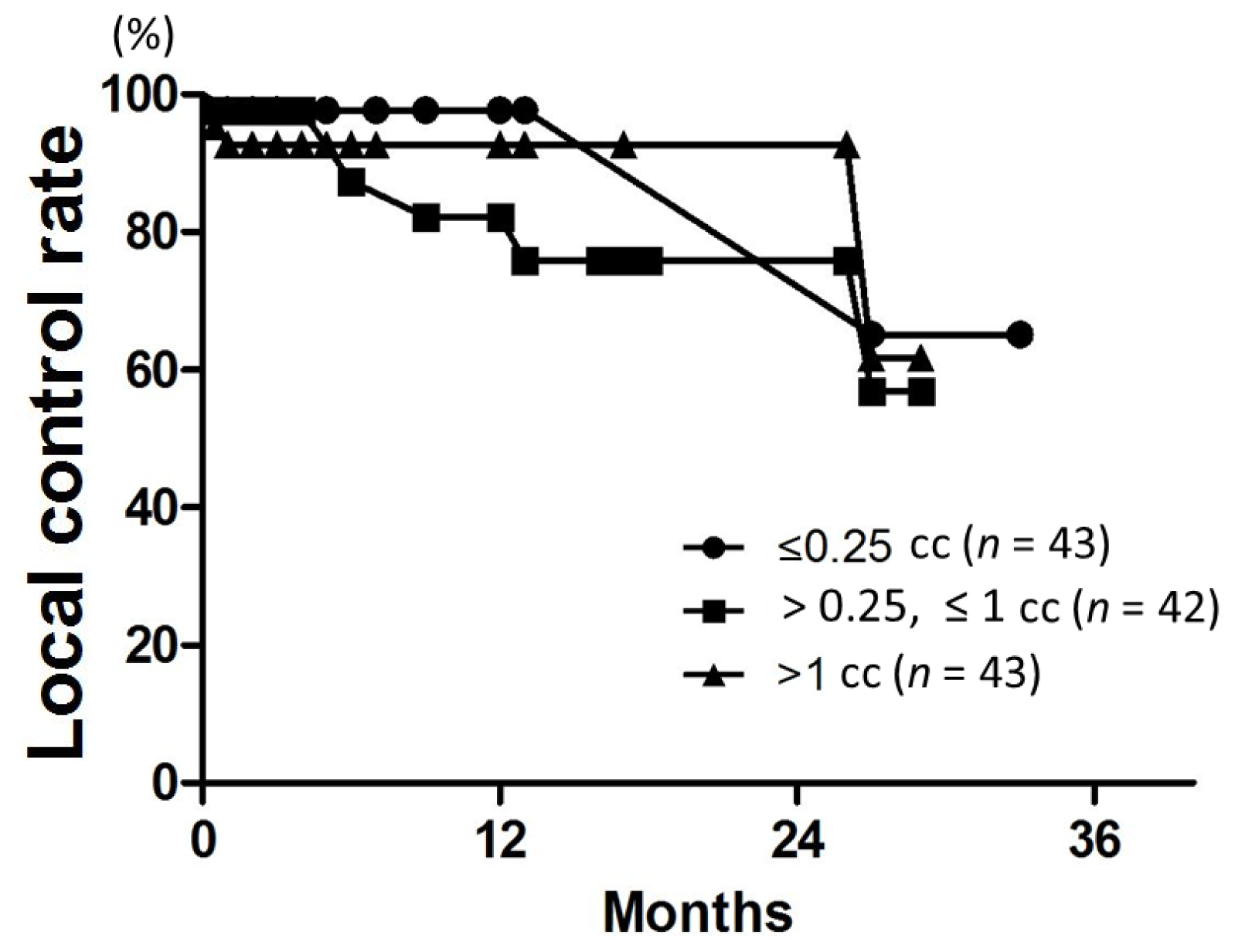
2.2. Local Control
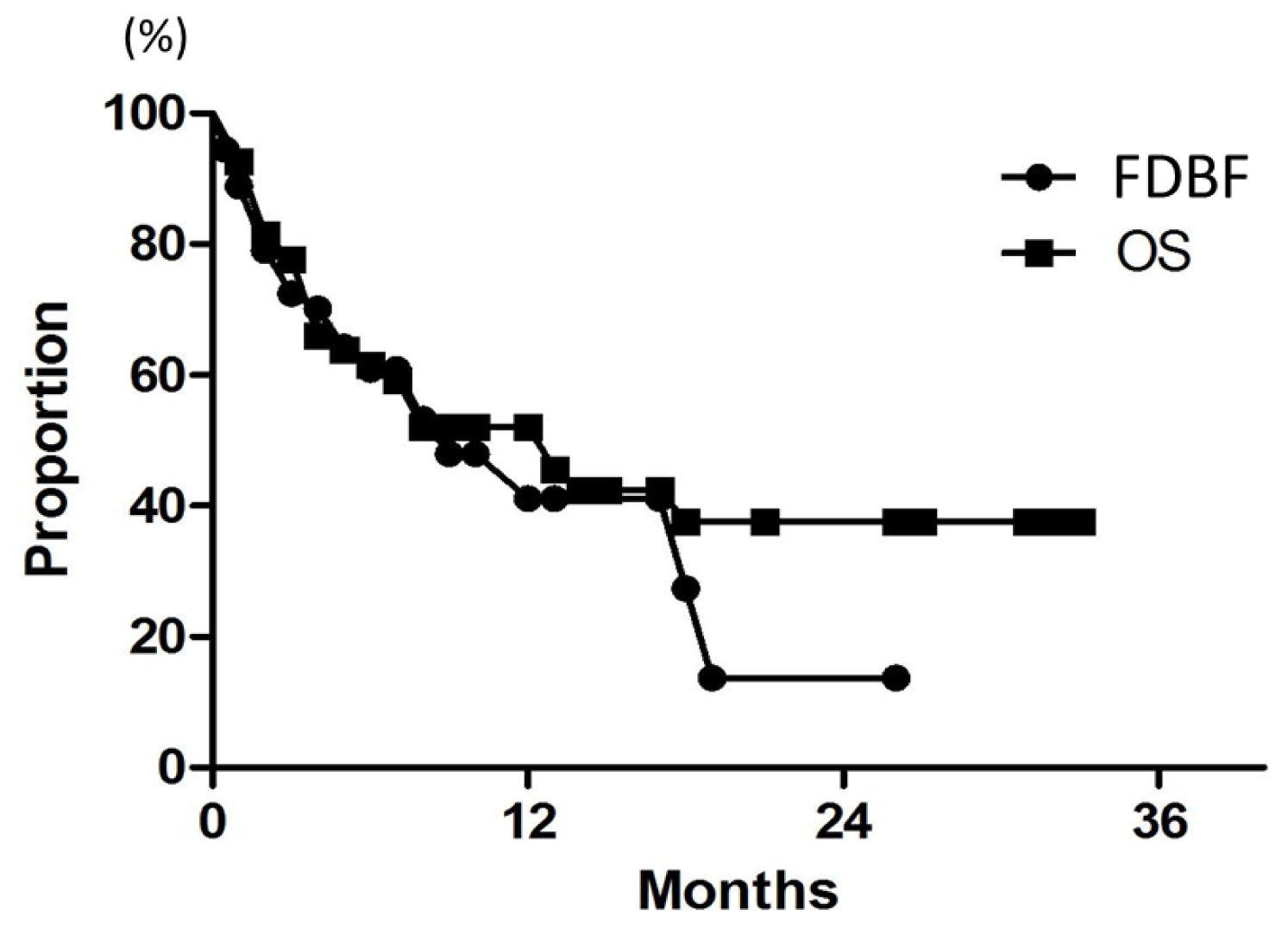
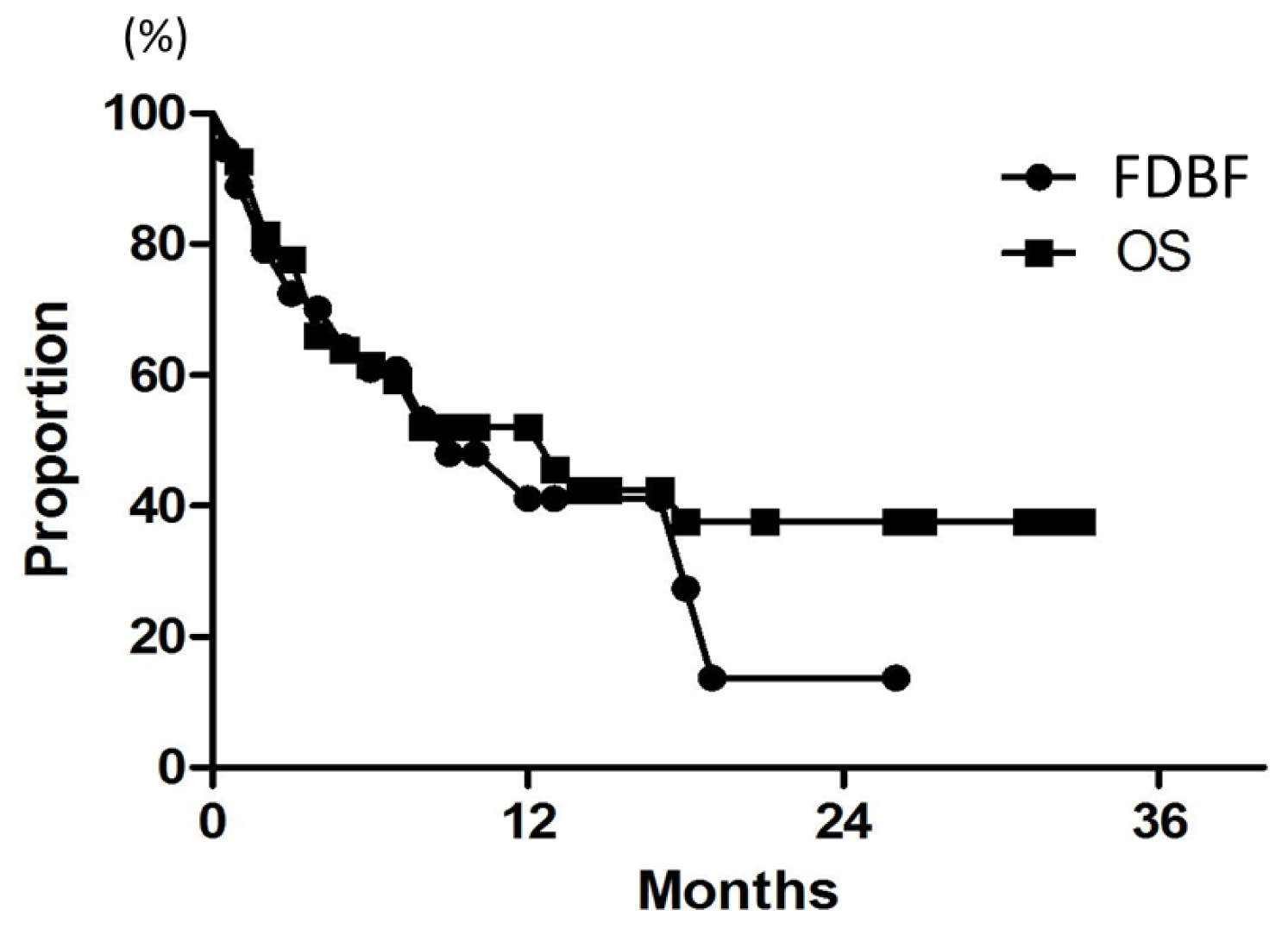
2.3. Overall Survival
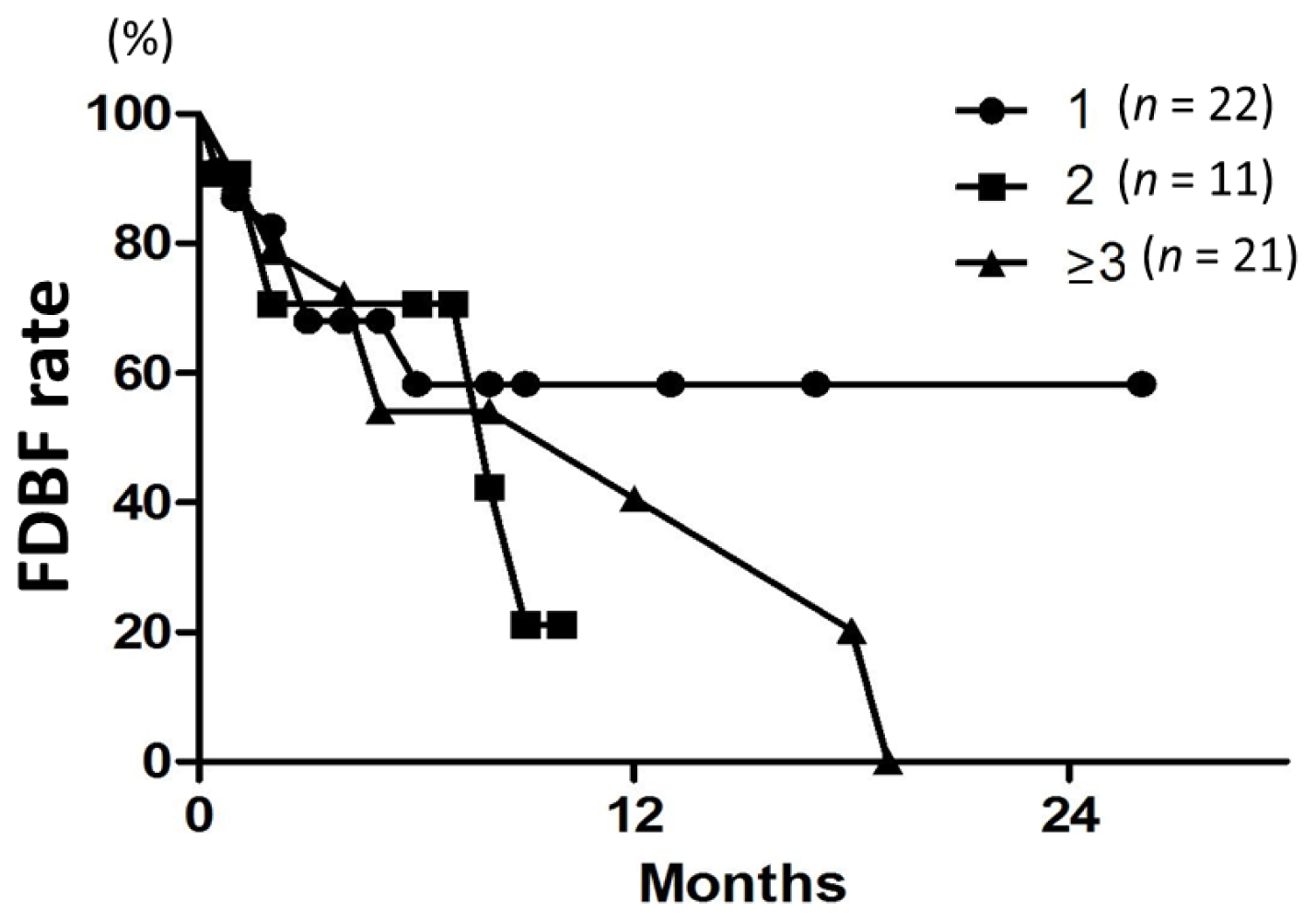
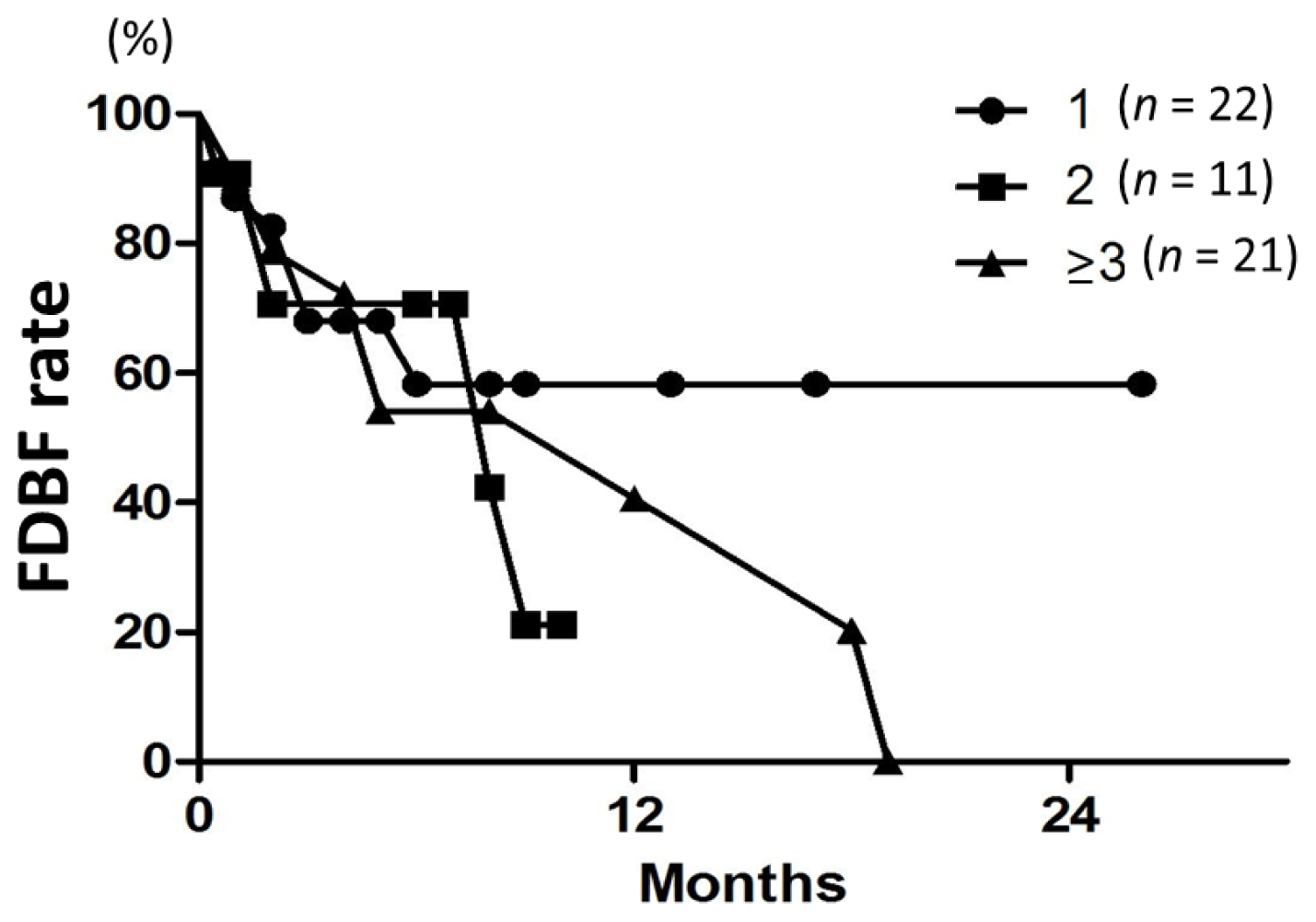
2.4. Freedom from Distant Brain Failure
2.5. Toxicity
3. Discussion
4. Methods and Materials
4.1. Study Design and Eligibility Criteria
4.2. Patient Characteristics
4.3. Treatment Methods
4.4. Evaluation
4.5. Statistical Methods
5. Conclusions
Acknowledgments
Conflicts of Interest
- Author ContributionsA.N. designed the study, contributed to the data acquisition, performed the statistical analysis, and prepared the manuscript. Y.S. designed the study and prepared the manuscript. M.Y. designed the study and contributed to the data acquisition. K.W. and Y.K. contributed to the data acquisition. All authors have read and approved the final manuscript.
References
- Soffietti, R.; Costanza, A.; Laguzzi, E.; Nobile, M.; Rudà, R. Radiotherapy and chemotherapy of brain metastases. J. Neurooncol 2005, 75, 31–42. [Google Scholar]
- Richards, C.M.; Khuntia, D.; Mehta, M.P. Therapeutic management of metastatic brain tumors. Crit. Rev. Oncol. Hematol 2007, 61, 70–78. [Google Scholar]
- Shibamoto, Y.; Sugie, C.; Iwata, H. Radiotherapy for metastatic brain tumors. Int. J. Clin. Oncol 2009, 14, 281–288. [Google Scholar]
- Caffo, M.; Barresi, V.; Caruso, G.; Cutugno, M.; la Fata, G.; Venza, M.; Alafaci, C.; Tomasello, F. Innovative therapeutic strategies in the treatment of brain metastases. Int. J. Mol. Sci 2013, 14, 2135–2174. [Google Scholar]
- Tsao, M.N.; Rades, D.; Wirth, A.; Lo, S.S.; Danielson, B.L.; Gaspar, L.E.; Sperduto, P.W.; Vogelbaum, M.A.; Radawski, J.D.; Wang, J.Z.; et al. Radiotherapeutic and surgical management for newly diagnosed brain metastasis (es): An American society for radiation oncology evidence-based guideline. Pract. Radiat. Oncol 2012, 2, 210–225. [Google Scholar]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases. JAMA 2006, 295, 2483–2491. [Google Scholar]
- Mehta, M.P.; Tsao, M.N.; Whelan, T.J.; Morris, D.E.; Hayman, J.A.; Flickinger, J.C.; Mills, M.; Rogers, C.L.; Souhami, L. The American society for therapeutic radiology and oncology (ASTRO) evidence-based review of the role of radiosurgery for brain metastases. Int. J. Radiat. Oncol. Biol. Phys 2005, 63, 37–46. [Google Scholar]
- Sanghavi, S.N.; Miranpuri, S.S.; Chappell, R.; Buatti, J.M.; Sneed, P.K.; Suh, J.H.; Regine, W.F.; Weltman, E.; King, V.J.; Goetsch, S.J.; et al. Radiosurgery for patients with brain metastases: Multi-institutional analysis, stratified by the RTOG recursive partitioning analysis method. Int. J. Radiat. Oncol. Biol. Phys 2001, 51, 426–434. [Google Scholar]
- Hall, E.J.; Brenner, D.J. The radiobiology of radiosurgery: Rationale for different treatment regimes for AVMs and malignancies. Int. J. Radiat. Oncol. Biol. Phys 1993, 25, 381–385. [Google Scholar]
- Shibamoto, Y.; Yukawa, Y.; Tsutsui, K.; Takahashi, M.; Abe, M. Variation in the hypoxic fraction among mouse tumors of different types, sizes, and sites. Jpn. J. Cancer Res 1986, 77, 908–915. [Google Scholar]
- Tomita, N.; Shibamoto, Y.; Ito, M.; Ogino, H.; Sugie, C.; Ayakawa, S.; Iwata, H. Biological effect of intermittent radiation exposure in vivo: Recovery from sublethal damage versus reoxygenation. Radiother. Oncol 2008, 86, 369–374. [Google Scholar]
- Shibamoto, Y.; Hashizume, C.; Baba, F.; Ayakawa, S.; Manabe, Y.; Nagai, A.; Miyakawa, A.; Murai, T.; Iwata, H.; Mori, Y.; et al. Stereotactic body radiotherapy using a radiobiology-based regimen for stage I nonsmall cell lung cancer. Cancer 2012, 118, 2078–2084. [Google Scholar]
- Chen, J.C.; Petrovich, Z.; O’Day, S.; Morton, D.; Essner, R.; Giannotta, S.L.; Yu, C.; Apuzzo, M.L. Stereotactic radiosurgery in the treatment of metastatic disease to the brain. Neurosurgery 2000, 47, 268–279. [Google Scholar]
- Shiau, C.Y.; Sneed, P.K.; Shu, H.K.; Lamborn, K.R.; McDermott, M.W.; Chang, S.; Nowak, P.; Petti, P.L.; Smith, V.; Verhey, L.J.; et al. Radiosurgery for brain metastases: Relationship of dose and pattern of enhancement to local control. Int. J. Radiat. Oncol. Biol. Phys 1997, 37, 375–383. [Google Scholar]
- Tomita, N.; Kodaira, T.; Tachibana, H.; Nakamura, T.; Nakahara, R.; Inokuchi, H.; Shibamoto, Y. Helical tomotherapy for brain metastases: Dosimetric evaluation of treatment plans and early clinical results. Technol. Cancer Res. Treat 2008, 7, 417–424. [Google Scholar]
- Rodrigues, G.; Yartsev, S.; Yaremko, B.; Perera, F.; Dar, A.R.; Hammond, A.; Lock, M.; Yu, E.; Ash, R.; Caudrelier, J.M.; et al. Phase I trial of simultaneous in-field boost with helical tomotherapy for patients with one to three brain metastases. Int. J. Radiat. Oncol. Biol. Phys 2011, 80, 1128–1133. [Google Scholar]
- Kirova, Y.M.; Chargari, C.; Zefkili, S.; Campana, F. Could helical tomotherapy do whole brain radiotherapy and radiosurgery? World J. Radiol 2010, 2, 148–150. [Google Scholar]
- Levegrün, S.; Pöttgen, C.; Wittig, A.; Lübcke, W.; Abu Jawad, J.; Stuschke, M. Helical tomotherapy for whole-brain irradiation with integrated boost to multiple brain metastases: Evaluation of dose distribution characteristics and comparison with alternative techniques. Int. J. Radiat. Oncol. Biol. Phys 2013, 86, 734–742. [Google Scholar]
- Vanderspek, L.; Bauman, G.; Wang, J.Z.; Yartsev, S.; Ménard, C.; Cho, Y.B.; Mundt, A.J.; Lawson, J.D.; Murphy, K.T. Dosimetric comparison of intensity-modulated radiosurgery and helical tomotherapy for the treatment of multiple intracranial metastases. Technol. Cancer Res. Treat 2009, 8, 361–367. [Google Scholar]
- Peñagarícano, J.A.; Yan, Y.; Shi, C.; Linskey, M.E.; Ratanatharathorn, V. Dosimetric comparison of helical tomotherapy and gamma knife stereotactic radiosurgery for single brain metastasis. Radiat. Oncol 2006, 1, 26–31. [Google Scholar]
- Hasegawa, T.; Kondziolka, D.; Flickinger, J.C.; Germanwala, A.; Lunsford, L.D. Brain metastases treated with radiosurgery alone: An alternative to whole brain radiotherapy? Neurosurgery 2003, 52, 1318–1326. [Google Scholar]
- Minniti, G.; Clarke, E.; Lanzetta, G.; Osti, M.F.; Trasimeni, G.; Bozzao, A.; Romano, A.; Enrici, R.M. Stereotactic radiosurgery for brain metastases: Analysis of outcome and risk of brain radionecrosis. Radiat. Oncol 2011, 6, 48–56. [Google Scholar]
- Nishizaki, T.; Saito, K.; Jimi, Y.; Harada, N.; Kajiwara, K.; Nomura, S.; Ishihara, H.; Yoshikawa, K.; Yoneda, H.; Suzuki, M.; et al. The role of cyberknife radiosurgery/radiotherapy for brain metastases of multiple or large-size tumors. Minim. Invasive Neurosurg 2006, 49, 203–209. [Google Scholar]
- Narayana, A.; Chang, J.; Yenice, K.; Chan, K.; Lymberis, S.; Brennan, C.; Gutin, P.H. Hypofractionated stereotactic radiotherapy using intensity-modulated radiotherapy in patients with one or two brain metastases. Stereotact. Funct. Neurosurg 2007, 85, 82–87. [Google Scholar]
- Inoue, H.K.; Seto, K.; Nozaki, A.; Torikai, K.; Suzuki, Y.; Saitoh, J.; Noda, S.E.; Nakano, T. Three-fraction cyberknife radiotherapy for brain metastases in critical areas: Referring to the risk evaluating radiation necrosis and the surrounding brain volumes circumscribed with a single dose equivalence of 14 Gy (V14). J. Radiat. Res 2013, 54, 727–735. [Google Scholar]
- Fahrig, A.; Ganslandt, O.; Lambrecht, U.; Grabenbauer, G.; Kleinert, G.; Sauer, R.; Hamm, K. Hypofractionated stereotactic radiotherapy for brain metastases—Results from three different dose concepts. Strahlenther. Onkol 2007, 183, 625–630. [Google Scholar]
- Märtens, B.; Janssen, S.; Werner, M.; Frühauf, J.; Christiansen, H.; Bremer, M.; Steinmann, D. Hypofractionated stereotactic radiotherapy of limited brain metastases: A single-centre individualized treatment approach. BMC Cancer 2012, 12, 497. [Google Scholar]
- Iwata, H.; Shibamoto, Y.; Murata, R.; Tomita, N.; Ayakawa, S.; Ogino, H.; Ito, M. Estimation of errors associated with use of linear-quadratic formalism for evaluation of biologic equivalence between single and hypofractionated radiation doses: An in vitro study. Int. J. Radiat. Oncol. Biol. Phys 2009, 75, 482–488. [Google Scholar]
- Shibamoto, Y.; Otsuka, S.; Iwata, H.; Sugie, C.; Ogino, H.; Tomita, N. Radiobiological evaluation of the radiation dose as used in high-precision radiotherapy: Effect of prolonged delivery time and applicability of the linear-quadratic model. J. Radiat. Res 2012, 53, 1–9. [Google Scholar]
- Han, C.; Liu, A.; Schultheiss, T.E.; Pezner, R.D.; Chen, Y.J.; Wong, J.Y. Dosimetric comparisons of helical tomotherapy treatment plans and step-and-shoot intensity-modulated radiosurgery treatment plans in intracranial stereotactic radiosurgery. Int. J. Radiat. Oncol. Biol. Phys 2006, 65, 608–616. [Google Scholar]
- Tannock, I.F. The relation between cell proliferation and the vascular system in a transplanted mouse mammary tumour. Br. J. Cancer 1968, 22, 258–273. [Google Scholar]
- Thomlinson, R.H.; Gray, L.H. The histological structure of some human lung cancers and the possible implications for radiotherapy. Br. J. Cancer 1955, 9, 539–549. [Google Scholar]
- Likhacheva, A.; Pinnix, C.C.; Parikh, N.R.; Allen, P.K.; McAleer, M.F.; Chiu, M.S.; Sulman, E.P.; Mahajan, A.; Guha-Thakurta, N.; Prabhu, S.S. Predictors of survival in contemporary practice after initial radiosurgery for brain metastases. Int. J. Radiat. Oncol. Biol. Phys 2013, 85, 656–661. [Google Scholar]
- Antoni, D.; Clavier, J.B.; Pop, M.; Benoît, C.; Lefebvre, F.; Noël, G. An institutional retrospective analysis of 93 patients with brain metastases from breast cancer: Treatment outcomes, diagnosis-specific prognostic factors. Int. J. Mol. Sci 2012, 13, 16489–16499. [Google Scholar]
- Sperduto, P.W.; Berkey, B.; Gaspar, L.E.; Mehta, M.; Curran, W. A new prognostic index and comparison to three other indices for patients with brain metastases: An analysis of 1960 patients in the RTOG database. Int. J. Radiat. Oncol. Biol. Phys 2008, 70, 510–514. [Google Scholar]
- Serizawa, T.; Hirai, T.; Nagano, O.; Higuchi, Y.; Matsuda, S.; Ono, J.; Saeki, N. Gamma knife surgery for 1–10 brain metastases without prophylactic whole-brain radiation therapy: Analysis of cases meeting the Japanese prospective multi-institute study (JLGK0901) inclusion criteria. J. Neurooncol 2010, 98, 163–167. [Google Scholar]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villà, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; et al. Adjuvant whole brain radiotherapy versus observation after radiosurgery or surgical resection of 1–3 cerebral metastases: Results of the EORTC 22952–26001 study. J. Clin. Oncol 2011, 29, 134–141. [Google Scholar]
- Shah, A.P.; Langen, K.M.; Ruchala, K.J.; Cox, A.; Kupelian, P.A.; Meeks, S.L. Patient dose from megavoltage computed tomography imaging. Int. J. Radiat. Oncol. Biol. Phys 2008, 70, 1579–1587. [Google Scholar]
- Soffietti, R.; Kocher, M.; Abacioglu, U.M.; Villa, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; et al. A european organisation for research and treatment of cancer phase III trial of adjuvant whole-brain radiotherapy versus observation in patients with one to three brain metastases from solid tumors after surgical resection or radiosurgery: Quality-of-life results. J. Clin. Oncol 2013, 31, 65–72. [Google Scholar]
- Shibamoto, Y.; Baba, F.; Oda, K.; Hayashi, S.; Kokubo, M.; Ishihara, S.; Itoh, Y.; Ogino, H.; Koizumi, M. Incidence of brain atrophy and decline in mini-mental state examination score after whole-brain radiotherapy in patients with brain metastases: A prospective study. Int. J. Radiat. Oncol. Biol. Phys 2008, 72, 1168–1173. [Google Scholar]
- Nagai, A.; Shibamoto, Y.; Mori, Y.; Hashizume, C.; Hagiwara, M.; Kobayashi, T. Increases in the number of brain metastases detected at frame-fixed, thin-slice MRI for gammaknife surgery planning. J. Neurooncol 2010, 12, 1187–1192. [Google Scholar]
- Soisson, E.T.; Hardcastle, N.; Tomé, W.A. Quality assurance of an image guided intracranial stereotactic positioning system for radiosurgery treatment with helical tomotherapy. J. Neurooncol 2010, 2, 277–285. [Google Scholar]
- Vaandering, A.; Lee, J.A.; Renard, L.; Grégoire, V. Evaluation of MVCT protocols for brain and head and neck tumor patients treated with helical tomotherapy. Radiother. Oncol 2009, 1, 50–56. [Google Scholar]
- Nataf, F.; Schlienger, M.; Liu, Z.; Foulquier, J.N.; Grès, B.; Orthuon, A.; Vannetzel, J.M.; Escudier, B.; Meder, J.F.; Roux, F.X.; et al. Radiosuegery with or without a 2-mm margin for 93 single brain metastases. Int. J. Radiat. Oncol. Biol. Phys 2008, 70, 766–772. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number of tumors (%) | ||
|---|---|---|---|
| Total number of patients | 54 | ||
| Primary lesion | Histology | ||
| Lung | 46 (85) | Squamous | 10 (22) |
| Adeno | 28 (61) | ||
| Small | 4 (9) | ||
| Poorly differentiated | 1 (2) | ||
| Undifferentiated | 3 (6) | ||
| Liver | 1 (2) | Poorly differentiated | 1 |
| Unknown | 1 (2) | – | – |
| Colon | 1 (2) | Adeno | 1 |
| Breast | 4 (7) | Ductal | 3 (75) |
| Scirrhous | 1 (25) | ||
| Uterus cervix | 1 (2) | Squamous | 1 |
| Total number of metastases | 128 | ||
| Number of metastases, median (range) | 2 (1–8) | ||
| GTV (cc), median (range) | 1.9 (0.01–18) | ||
| PTV maximum (Gy), median (range) | 34 (28–39) | ||
| PTV minimum (Gy), median (range) | 27 (23–33) | ||
| HI, median (range) | 1.2 (1.0–1.4) | ||
| Characteristic | Number of patients (%) | |
|---|---|---|
| Total number of patients | 54 | |
| Gender | Male | 30 (56) |
| Female | 24 (44) | |
| Age (years) median (range) | 67 (38–89) | |
| Extracranial disease | Yes | 42 (78) |
| No | 12 (22) | |
| Previous SRS or SRT * | Yes | 38 (70) |
| No | 16 (30) | |
| Previous surgery | Yes | 4 (7) |
| No | 50 (93) | |
| Recurrence after surgery | Yes | 2 (50) |
| No | 2 (50) | |
| Total dose at 80% isodose | 28 Gy | 33 (61) |
| 28.8 Gy | 21 (39) | |
| RPA class | I | 7 |
| II | 42 | |
| III | 5 | |
| GPA score | 0–1 | 9 |
| 1.5–2.5 | 36 | |
| 3 | 6 | |
| 3.5–4 | 3 | |
| Factor (sort, n) | Rate at 12 months (p value) | ||
|---|---|---|---|
| LC | OS | FDBF | |
| Age (≤65 vs. >65 years, 25 vs. 29) | 82, 91 (0.2) | 42, 61 (0.4) | 66, 25 (0.1) |
| Gender (male vs. female, 31 vs. 23) | 96, 76 (0.7) | 49, 57 (0.3) | 42, 40 (0.9) |
| Tumor number (1 vs. ≥2, 22 vs. 32) | 100, 79 (0.04) | 53, 51 (0.2) | 58, 31 (0.4) |
| Tumor number (≤3 vs. ≥4, 42 vs. 12) | 86, 90 (0.2) | 56, 36 (0.08) | 38, 46 (0.7) |
| GTV (<1 vs. ≥1 cc, 85 vs. 43) | 90, 93 (0.8) | – | – |
| GTV (<2 vs. ≥2 cc, 100 vs. 28) | 91, 89 (0.1) | – | – |
| GTV (<3 vs. ≥3 cc, 104 vs. 24) | 91, 92 (0.3) | – | – |
| GTV (<5 vs. ≥5 cc, 112 vs. 16) | 89, 100 (0.7) | – | – |
| GTV (<10 vs. ≥10 cc, 122 vs. 6) | 90, 100 (0.9) | – | – |
| Cumulative GTV (<2 vs. ≥2 cc, 27 vs. 27) | 45, 71 (0.7) | 72, 31 (<0.0001) | 41, 45 (0.9) |
| Cumulative GTV (<3 vs. ≥3 cc, 32 vs. 22) | 52, 71 (0.8) | 63, 37 (0.2) | 41, 46 (0.6) |
| Extracranial disease (controlled vs. uncontrolled, 11 vs. 43) | 86, 93 (0.2) | 73, 34 (0.0002) | 41, 46 (0.5) |
| Factor (sort, n) | p value, HR, 95% CI | ||
|---|---|---|---|
| LC | OS | FDBF | |
| Tumor number (1 vs. ≥2, 22 vs. 32) | 0.9, 1.1, 0.09–13 | 0.4, 0.7, 0.3–1.7 | 0.7, 1.2, 0.5–3.0 |
| Cumulative GTV (<2 vs. ≥2 cc, 100 vs. 28) | 0.9, 0.0, 0.0–1.5 | 0.6, 1.2, 0.5–2.9 | 0.4, 0.7, 0.3–1.7 |
| Extracranial disease (controlled vs. uncontrolled, 11 vs. 43) | 0.6, 0.5, 0.04–6.1 | 0.002, 0.2, 0.09–0.6 | 0.5, 0.7, 0.3–1.8 |
| Primary lesion | Histology | ≤0.25 cc | >0.25 and ≤1 cc | >1 and ≤3 cc | >3 and ≤10 cc | >10 cc |
|---|---|---|---|---|---|---|
| Lung | Squamous | 5 | 3 | 6 | 2 | 1 |
| Adeno | 32 | 29 | 11 | 8 | 3 | |
| Small cell | 0 | 2 | 2 | 2 | 0 | |
| PD | 0 | 2 | 0 | 2 | 0 | |
| UD | 0 | 2 | 0 | 1 | 1 | |
| Liver | PD | 1 | 1 | 0 | 1 | 0 |
| Unknown | – | 0 | 0 | 0 | 0 | 1 |
| Colon | Adeno | 0 | 0 | 0 | 1 | 0 |
| Breast | Ductal | 5 | 1 | 0 | 0 | 0 |
| Scirrhous | 0 | 1 | 0 | 1 | 0 | |
| Uterus cervix | Squamous | 1 | 0 | 0 | 0 | 0 |
| Minniti | Fahrig | Martens | Inoue | Narayana | This study | |||
|---|---|---|---|---|---|---|---|---|
| Patient No | 206 | 150 | 75 | 145 | 12 | 54 | ||
| Median size | 1.9 cc (cumulative GTV) | 6.1 cc (PTV) | 1.5 cc (GTV) | 6.9 cc (GTV) | 3.5 cm (GTV) | 1.9 cc (cumulative GTV) | ||
| Dose (Gy)/fraction | 20/1, 18/1, (15–16)/1 | 35/5 | 35/7 | 40/10 | Mainly 30/6, 35/7, 30/5 | 27/3 | 30/5 | 28/4, 28.8/4 |
| BED10 (Gy) | – | 40–49.6 | 43.8 | 56 | – | 42.8 | 40 | 47.6, 48.6 |
| LC rate at 12 months (%) | 92 | (96) | (85) | (87) | 52 | (95.8) | 70 | 91 |
| Median OS (month) | 14 | 15 | 9.1 | 7 | 8.5 | 7 | ||
| Isodose line | 87 | – | – | 60 | 100 | 80 | ||
| ≥Gr 3 acute toxicity (%) | 5.8 | 0 | 0 | 0 | – | 6.2 | Increased steroid use: 15 | 0 |
| ≥Gr 3 late toxicity (%) | 22 | 7 | 0 | 1.3 | 0 |
© 2014 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Nagai, A.; Shibamoto, Y.; Yoshida, M.; Wakamatsu, K.; Kikuchi, Y. Treatment of Single or Multiple Brain Metastases by Hypofractionated Stereotactic Radiotherapy Using Helical Tomotherapy. Int. J. Mol. Sci. 2014, 15, 6910-6924. https://doi.org/10.3390/ijms15046910
Nagai A, Shibamoto Y, Yoshida M, Wakamatsu K, Kikuchi Y. Treatment of Single or Multiple Brain Metastases by Hypofractionated Stereotactic Radiotherapy Using Helical Tomotherapy. International Journal of Molecular Sciences. 2014; 15(4):6910-6924. https://doi.org/10.3390/ijms15046910
Chicago/Turabian StyleNagai, Aiko, Yuta Shibamoto, Masanori Yoshida, Koichi Wakamatsu, and Yuzo Kikuchi. 2014. "Treatment of Single or Multiple Brain Metastases by Hypofractionated Stereotactic Radiotherapy Using Helical Tomotherapy" International Journal of Molecular Sciences 15, no. 4: 6910-6924. https://doi.org/10.3390/ijms15046910
APA StyleNagai, A., Shibamoto, Y., Yoshida, M., Wakamatsu, K., & Kikuchi, Y. (2014). Treatment of Single or Multiple Brain Metastases by Hypofractionated Stereotactic Radiotherapy Using Helical Tomotherapy. International Journal of Molecular Sciences, 15(4), 6910-6924. https://doi.org/10.3390/ijms15046910