Nipple Discharge of CA15-3, CA125, CEA and TSGF as a New Biomarker Panel for Breast Cancer

 ,
,
Abstract
:1. Introduction
2. Results and Discussion
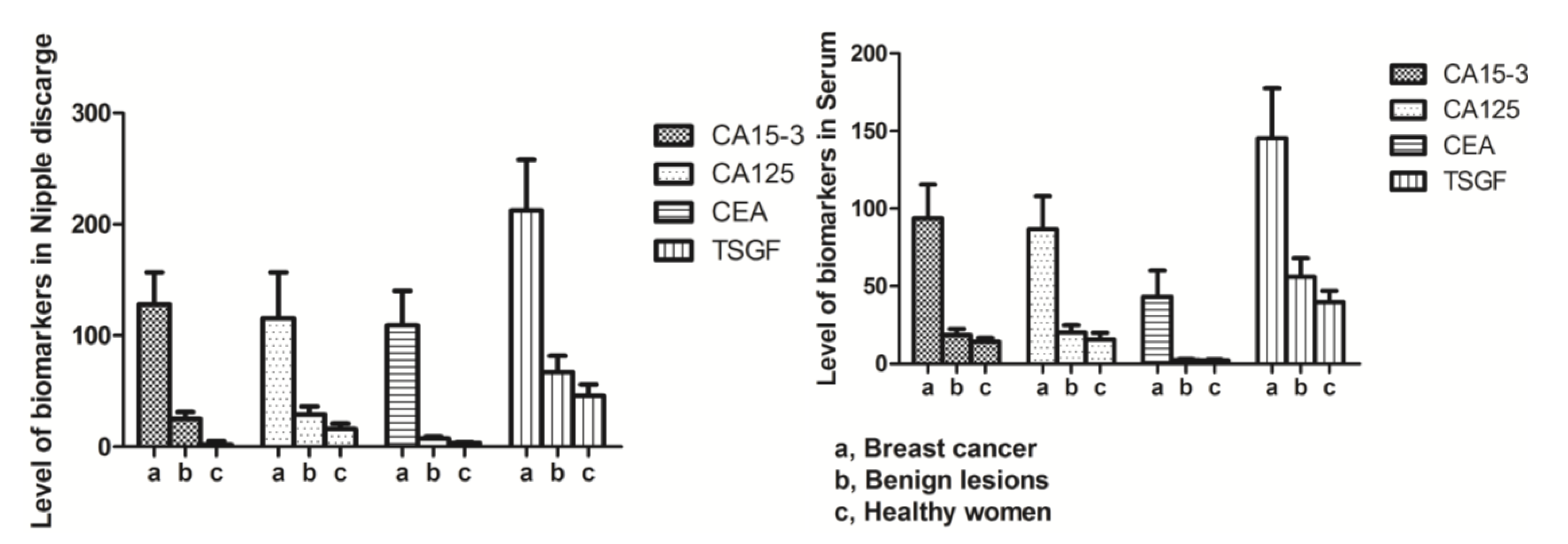
2.1. The Levels of Biomarkers in the Serum and Nipple Discharge in Three Patient Groups

{kind=link}
{kind=link}
{kind=link}
| Group | n | CA15-3 (U/mL) | CA125 (U/mL) | CEA (ng/mL) | TSGF (U/mL) |
|---|---|---|---|---|---|
| Nipple discharge | |||||
| Breast cancer | 86 | 128.21 ± 28.63 | 115.71 ± 41.08 | 109.23 ± 30.94 | 212.42 ± 45.71 |
| Benign lesions | 136 | 25.13 ± 6.14 a | 29.41 ± 7.22 a | 7.46 ± 1.75 a | 67.01 ± 14.98 a |
| Healthy women | 60 | 15.95 ± 3.23 b | 16.11 ± 4.76 b | 3.28 ± 0.87 b | 45.78 ± 10.36 b |
| Serum | |||||
| Breast cancer | 86 | 93.79 ± 21.80 | 86.68 ± 21.37 | 43.29 ± 16.81 | 145.46 ± 32.11 |
| Benign lesions | 136 | 18.61 ± 3.98 c | 20.29 ± 4.60 c | 2.40 ± 0.72 c | 56.01 ± 11.99 c |
| Healthy women | 60 | 14.22 ± 2.47 d | 15.76 ± 4.25 d | 2.33 ± 0.54 d | 39.78 ± 7.36 d |

2.2. Discriminative Diagnostic Value of Biomarkers in the Nipple Discharge and Serum of Breast Cancer Patients
| Groups | Sensitivity | Accuracy | Specificity | PV+ | PV− |
|---|---|---|---|---|---|
| Nipple discharge | |||||
| CA15-3 | 74.4 | 80.5 | 82.4 | 57.1 | 91.1 |
| CA125 | 72.1 | 81.0 | 83.8 | 58.5 | 90.5 |
| CEA | 69.8 | 82.2 | 86.0 | 61.2 | 90.0 |
| TSGF | 69.8 | 79.9 | 83.1 | 56.6 | 86.7 |
| Serum | |||||
| CA15-3 | 60.5 | 84.4 | 91.9 | 70.3 | 88.0 |
| CA125 | 55.8 | 82.2 | 90.4 | 64.9 | 88.6 |
| CEA | 53.5 | 80.5 | 89.0 | 60.5 | 85.8 |
| TSGF | 62.8 | 84.4 | 91.2 | 69.3 | 88.6 |
| Combination | 97.7 * | 80.5 | 75.0 | 55.3 | 99.0 * |

| Parameter | AUC | 95% CI | p value | |
|---|---|---|---|---|
| Lower bound | Upper bound | |||
| Nipple discharge | ||||
| CA153 (U/mL) | 0.784 | 0.719 | 0.849 | <0.01 |
| TSGF (U/mL) | 0.764 | 0.697 | 0.842 | <0.01 |
| CA125 (U/mL) | 0.780 | 0.713 | 0.846 | <0.01 |
| CEA (ng/mL) | 0.779 | 0.712 | 0.846 | <0.01 |
| Combination ND | 0.827 | 0.769 | 0.885 | <0.01 |
| Serum | ||||
| CA153 (U/mL) | 0.762 | 0.692 | 0.832 | <0.01 |
| TSGF (U/mL) | 0.770 | 0.701 | 0.839 | <0.01 |
| CA125 (U/mL) | 0.732 | 0.659 | 0.804 | <0.01 |
| CEA (ng/mL) | 0.712 | 0.639 | 0.786 | <0.01 |
| Combination ND + Serum | 0.863 | 0.814 | 0.913 | <0.01 |
2.3. The Relationship between the Nipple Discharge Levels of Tumor Markers and Biological Parameters within a Breast Cancer Group
| Subgroup | n | CA15-3 (U/mL) mean ± SD | CA125 (U/mL) mean ± SD | CEA (ng/mL) mean ± SD | TSGF (U/mL) mean ± SD |
|---|---|---|---|---|---|
| Tumor size | |||||
| ≤2 cm | 54 | 126.48 ± 23.34 | 113.96 ± 27.58 | 108.84 ± 25.12 | 206.78 ± 36.67 |
| >2 cm | 32 | 129.03 ± 28.37 | 116.89 ± 40.98 | 111.13 ± 32.84 | 214.89 ± 39.95 |
| Age | |||||
| ≥50 years | 58 | 129.01 ± 30.54 | 116.37 ± 41.24 | 112.94 ± 31.06 | 215.78 ± 38.91 |
| <50 years | 28 | 127.72 ± 29.66 | 76.54 ± 22.43 | 107.01 ± 28.38 | 209.67 ± 35.53 |
| Age at Menarche | |||||
| ≤14 years | 60 | 125.28 ± 25.69 | 113.65 ± 30.23 | 111.24 ± 29.33 | 210.83 ± 35.98 |
| >14 years | 26 | 130.06 ± 31.77 | 116.89 ± 41.01 | 108.20 ± 28.27 | 213.77 ± 37.93 |
| Age at Menopause | |||||
| ≤50 years | 69 | 136.61 ± 33.39 | 145.17 ± 51.72 | 131.42 ± 41.88 | 233.43 ± 41.23 |
| >50 years | 17 | 115.89 ± 18.25 | 112.57 ± 39.53 | 99.91 ± 28.39 | 198.87 ± 32.56 |
| BMI | |||||
| <30 kg/m2 | 62 | 129.74 ± 31.64 | 117.01 ± 42.75 | 107.91 ± 28.91 | 215.72 ± 38.21 |
| ≥30 kg/m2 | 24 | 127.51 ± 29.36 | 112.09 ± 30.01 | 112.62 ± 29.47 | 210.65 ± 34.37 |
| ER & PR | |||||
| positive | 72 | 129.46 ± 22.98 | 119.98 ± 28.87 | 92.62 ± 29.89 | 189.23 ± 32.31 |
| negative | 14 | 157.83 ± 37.56 | 121.38 ± 30.32 | 128.98 ± 31.11 | 251.71 ± 53.89 |
| HER2/neu | |||||
| positive | 28 | 151.43 ± 32.42 | 120.69 ± 31.37 | 117.34 ± 29.65 | 243.56 ± 54.76 |
| negative | 58 | 125.74 ± 26.05 | 98.55 ± 20.79 | 85.62 ± 27.47 | 187.34 ± 33.96 |
| VEGF | |||||
| positive | 59 | 147.62 ± 41.23 | 111.42 ± 31.88 | 123.33 ± 32.46 | 242.45 ± 43.88 |
| negative | 27 | 112.28 ± 26.72 | 80.99 ± 22.39 | 104.44 ± 25.12 | 189.79 ± 31.96 |
| Ki-67 | |||||
| >14% | 21 | 165.24 ± 39.33 | 139.19 ± 44.32 | 125.17 ± 33.42 | 237.78 ± 46.53 |
| ≤14% | 65 | 110.36 ± 25.78 | 106.35 ± 25.17 | 103.56 ± 25.67 | 201.78 ± 31.56 |
| Grade | |||||
| III | 33 | 312.56 ± 66.13 | 165.31 ± 63.42 | 195.67 ± 56.32 | 263.21 ± 68.43 |
| II | 53 | 68.20 ± 24.35 | 96.42 ± 26.34 | 78.32 ± 14.69 | 176.42 ± 23.69 |
| Lymph node metastasis | |||||
| positive | 42 | 128.21 ± 28.63 | 115.71 ± 41.08 | 109.23 ± 30.94 | 212.42 ± 45.71 |
| negative | 44 | 20.01 ± 10.97 | 21.43 ± 7.83 | 5.49 ± 2.78 | 46.891 ± 16.77 |
| Distal metastasis | |||||
| positive | 17 | 572.23 ± 105.25 | 198.62 ± 47.24 | 158.23 ± 55.24 | 228.22 ± 73.15 |
| negative | 69 | 90.64 ± 23.33 | 143.63 ± 26.02 | 105.01 ± 28.32 | 189.63 ± 26.31 |
| Recurrence | |||||
| positive | 17 | 176.32 ± 105.25 | 189.62 ± 98.78 | 171.77 ± 56.76 | 236.65 ± 98.76 |
| negative | 69 | 107.43 ± 24.68 | 101.34 ± 89.34 | 87.62 ± 23.19 | 176.76 ± 32.34 |
2.4. The Relationship between Prognosis and Immunohistochemistry Staining Results according to ER, PR, and HER2/neu Status
| Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR a | 95% CI b | p value | HR a | 95% CI b | p value | |
| Age | 0.945 | 0.890–1.097 | 0.079 | 0.945 | 0.899–0.993 | 0.113 |
| Tumor size | 0.476 | 0.219–0.836 | 0.682 | 0.528 | 0.327–2.073 | 0.598 |
| Lymph node status | 0.369 | 0.175–0.794 | 0.008 | 0.762 | 0.275–2.197 | 0.049 |
| Histologic grade | 0.422 | 0.374–0.510 | 0.001 | 0.592 | 0.117–2.013 | 0.067 |
| Disease stage | 1.432 | 0.789–2.876 | 0.021 | 1.673 | 1.016–2.942 | 0.032 |
| ER & PR status | 1.231 | 0.598–2.763 | 0.465 | 1.234 | 0.465–3.279 | 0.659 |
| HER2/neu status | 1.989 | 1.386–2.785 | 0.001 | 1.592 | 1.076–3.118 | 0.072 |
| Serum | ||||||
| CA153 | 0.959 | 0.835–1.101 | 0.549 | 0.353 | 0.114–1.095 | 0.071 |
| TSGF | 1.000 | 0.974–1.027 | 0.996 | 1.024 | 0.962–1.091 | 0.449 |
| CA125 | 0.985 | 0.903–1.033 | 0.312 | 1.202 | 0.867–1.666 | 0.270 |
| CEA | 1.033 | 0.959–1.112 | 1.394 | 1.492 | 0.958–2.323 | 0.076 |
| Combination serum | 1.112 | 0.998–1.102 | 0.142 | 1.108 | 0.798–1.423 | 0.621 |
| Nipple discharge | ||||||
| CA153 | 1.262 | 1.066–1.493 | 0.007 | 4.911 | 0.925–16.084 | 0.062 |
| TSGF | 1.558 | 0.774–2.332 | 0.254 | 2.834 | 0.962–4.231 | 0.317 |
| CA125 | 1.019 | 0.971–1.069 | 0.441 | 0.741 | 0.499–1.100 | 0.137 |
| CEA (ng/mL) | 1.059 | 0.966–1.160 | 0.224 | 1.396 | 0.943–2.067 | 0.095 |
| Combination ND | 1.418 | 0.838–2.319 | 0.018 | 1.562 | 0.732–3.442 | 0.263 |
| Combination serum/ND | 1.760 | 1.083–2.597 | 0.015 | 1.879 | 1.091–3.214 | 0.021 |

| ER & PR status | SD | PD | p value |
|---|---|---|---|
| ER & PR negative | 5 | 9 | <0.001 |
| ER & PR positive | 53 | 19 |
| ER & PR status | SD | PD | p value |
|---|---|---|---|
| ER & PR negative | 49 | 9 | <0.001 |
| ER & PR positive | 9 | 19 |
3. Materials and Methods
3.1. Ethical Statement
3.2. Patients
3.3. Measurement of Biomarkers in Patient Serum and Nipple Discharge Samples
3.4. Pathologic Analysis
3.5. Statistical Analysis
4. Conclusions
Abbreviations
| CA15-3 | cancer antigen 15-3 |
| CEA | carcinoembryonic antigen |
| CA125 | cancer antigen 125 |
| TSGF | malignant tumor-specific growth factor |
| ER | estrogen receptor |
| PR | progestrone receptor |
| HER2/neu | human epidermal growth factor receptor type 2 |
| VEGF | vascular endothelial growth factor |
| ND | Nipple Discharge |
| HR | Hazard ratio |
| SD | standard deviation |
| PD | progressive disease |
| PFS | Progression-free survival |
| OS | overall survival |
| CI | confidence interval |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| BMI | body mass index |
| IQR | inter-quartile range |
| ROC | receiver operating characteristic |
| AUC | area under the curve |
| FDA | Food and Drug Administration |
| DCIS | ductal carcinoma in situ |
| DAB | Diaminobenzidine |
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Opstal-van Winden, A.W.J.; Rodenburg, W.; Pennings, J.L.A.; van Oostrom, C.T.M.; Beijnen, J.H.; Peeters, P.H.; van Gils, C.H.; de Vries, A. A bead-based multiplexed immunoassay to evaluate breast cancer biomarkers for early detection in pre-diagnostic Serum. Int. J. Mol. Sci. 2012, 13, 13587–13604. [Google Scholar] [CrossRef]
- Ghadge, M.S.; Naik, P.P.; Tiwari, B.P.; Hegde, R.M.; Matale, T.J. A comparative study of bone scan findings and serum levels of tumor marker CA153 in patients with breast carcinoma. Indian J. Clin. Biochem. 2012, 27, 97–99. [Google Scholar] [CrossRef]
- Pitteri, S.J.; Amon, L.M.; Buson, T.B.; Zhang, Y.; Johnson, M.M.; Chin, A.; Kennedy, J.; Wong, C.H.; Zhang, Q.; Wang, H.; et al. Detection of elevated plasma levels of EGF receptor prior to breast cancer diagnosis among hormone therapy users. Cancer Res. 2010, 70, 8598–8606. [Google Scholar] [CrossRef]
- Sahab, Z.J.; Man, Y.-G.; Byers, S.W.; Sang, Q.-X. Putative biomarkers and targets of estrogen receptor negative human breast cancer. Int. J. Mol. Sci. 2011, 12, 4504–4521. [Google Scholar] [CrossRef]
- Zhang, S.J.; Hu, Y.; Qian, H.L.; Jiao, S.C.; Liu, Z.F.; Tao, H.T.; Han, L. Expression and signifcance of ER, PR, VEGF, CA15–3, CA125 and CEA in judging the prognosis of breast cancer. Asian Pac. J. Cancer Prev. 2013, 14, 3937–3940. [Google Scholar] [CrossRef]
- Boyd, N.F.; Guo, H.; Martin, L.J.; Sun, L.; Stone, J.; Fishell, E.; Jong, R.A.; Hislop, G.; Chiarelli, A.; Minkin, S.; et al. Mammographic density and the risk and detection of breast cancer. N. Engl. J. Med. 2007, 356, 227–236. [Google Scholar] [CrossRef]
- Mannello, F.; Medda, V.; Tonti, G.A. Protein profile analysis of the breast microenvironment to differentiate healthy women from breast cancer patients. Expert Rev. Proteomics 2009, 6, 43–60. [Google Scholar] [CrossRef]
- Huijbers, A.; Velstra, B.; Dekker, T.J.A.; Mesker, W.E.; Burgt, Y.E.M.; Mertens, B.J.; Deelder, A.M.; Tollenaar, R.A.E.M. Proteomic serum biomarkers and their potential application in cancer screening programs. Int. J. Mol. Sci. 2010, 11, 4175–4193. [Google Scholar] [CrossRef]
- Sun, M.Q.; Meng, A.F.; Huang, X.E.; Wang, M.X. Comparison of psychological infuence on breast cancer patients between breast-conserving surgery and modifed radical mastectomy. Asian Pac. J. Cancer Prev. 2013, 14, 149–152. [Google Scholar] [CrossRef]
- Piura, E.; Piura, B. Autoantibodies to tumor-associated antigens in breast carcinoma. J. Oncol. 2010, 2010, 264926. [Google Scholar]
- Zervoudis, S.; Iatrakis, G.; Economides, P.; Polyzos, D.; Navrozoglou, I. Nipple discharge screening. Women’s Health 2010, 6, 135–151. [Google Scholar]
- Kulasingam, V.; Zheng, Y.; Soosaipillai, A.; Leon, A.E.; Gion, M.; Diamandis, E.P. Activated leukocyte cell adhesion molecule: A novel biomarker for breast cancer. Int. J. Cancer 2009, 125, 9–14. [Google Scholar] [CrossRef]
- Hwa, H.L.; Kuo, W.H.; Chang, L.Y.; Wang, M.Y.; Tung, T.H.; Chang, K.J.; Hsieh, F.J. Prediction of breast cancer and lymph node metastatic status with tumour markers using logistic regression models. J. Eval. Clin. Pract. 2008, 14, 275–280. [Google Scholar] [CrossRef]
- Sturgeon, C.M.; Duffy, M.J.; Stenman, U.H.; Lilja, H.; Brunner, N.; Chan, D.W.; Babaian, R.; Bast, R.C., Jr.; Dowell, B.; Esteva, F.J.; et al. National academy of clinical biochemistry laboratory medicine practice guidelines for use of tumor markers in testicular, prostate, colorectal, breast, and ovarian cancers. Clin. Chem. 2008, 54, e11–e79. [Google Scholar] [CrossRef]
- Perou, C.M.; Sorlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Jiang, S.W.; Chen, H.; Dowdy, S.; Fu, A.; Attewell, J.; Kalogera, E.; Drapkin, R.; Podratz, K.; Broaddus, R.; Li, J. HE4 Transcription- and splice variants-specific expression in endometrial cancer and correlation with patient survival. Int. J. Mol. Sci. 2013, 14, 22655–22677. [Google Scholar] [CrossRef]
- Xiang, M.; Zhou, W.; Gao, D.; Fang, X.; Liu, Q. Inhibitor of apoptosis protein-like protein-2 as a novel serological biomarker for breast cancer. Int. J. Mol. Sci. 2012, 13, 16737–16750. [Google Scholar] [CrossRef]
- Zhu, C.S.; Pinsky, P.F.; Cramer, D.W.; Ransohoff, D.F.; Hartge, P.; Pfeiffer, R.M.; Urban, N.; Mor, G.; Bast, R.C., Jr.; Moore, L.E.; et al. A framework for evaluating biomarkers for early detection: Validation of biomarker panels for ovarian cancer. Cancer Prev. Res. 2011, 4, 375–383. [Google Scholar] [CrossRef]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C., Jr.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef]
- Baker, S.G.; Sargent, D.J. Designing a randomized clinical trial to evaluate personalized medicine: A new approach based on risk prediction. J. Natl. Cancer Inst. 2010, 102, 1756–1759. [Google Scholar] [CrossRef]
- Chen, S.; Wang, J.; Gou, W.F.; Xiu, Y.L.; Zheng, H.C.; Zong, Z.H.; Takano, Y.; Zhao, Y. The involvement of RhoA and Wnt-5a in the tumorigenesis and progression of ovarian epithelial carcinoma. Int. J. Mol. Sci. 2013, 14, 24187–24199. [Google Scholar] [CrossRef]
- Norum, L.F.; Erikstein, B.; Nustad, K. Elevated CA125 in breast cancer—A sign of advanceddisease. Tumor Biol. 2001, 22, 223–228. [Google Scholar] [CrossRef]
- American Joint Committee on Cancer (AJCC). Cancer Stanging Manual, 7th ed.; Edge, S.B., Byrd, D.R., Compton, C.C., Fritz, A.G., Greene, F.L., Trotti, A., Eds.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Lang, J.E.; Kuerer, H.M. Breast ductal secretions: Clinical features, potential uses, and possible applications. Cancer Control 2007, 14, 350–359. [Google Scholar]
- Dolan, R.T.; Butler, J.S.; Kell, M.R.; Gorey, T.F.; Stokes, M.A. Nipple discharge and the efficacy of duct cytology in evaluating breast cancer risk. Surgeon 2010, 8, 252–258. [Google Scholar] [CrossRef]
- Chen, L.; Zhou, W.B.; Zhao, Y.; Liu, X.A.; Ding, Q.; Zha, X.M.; Wang, S. Bloody nipple discharge is a predictor of breast cancer risk: A meta–analysis. Breast Cancer Res. Treat. 2012, 132, 9–14. [Google Scholar] [CrossRef]
- Parthasarathy, V.; Rathnam, U. Nipple discharge: An early warning sign of breast cancer. Int. J. Prev. Med. 2012, 3, 810–814. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Xie, F.; Yang, H.; Wang, S.; Zhou, B.; Tong, F.; Yang, D.; Zhang, J. A logistic regression model for predicting axillary lymph node metastases in early breast carcinoma patients. Sensors 2012, 12, 9936–9950. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Wang, G.; Qin, Y.; Zhang, J.; Zhao, J.; Liang, Y.; Zhang, Z.; Qin, M.; Sun, Y. Nipple Discharge of CA15-3, CA125, CEA and TSGF as a New Biomarker Panel for Breast Cancer. Int. J. Mol. Sci. 2014, 15, 9546-9565. https://doi.org/10.3390/ijms15069546
Wang G, Qin Y, Zhang J, Zhao J, Liang Y, Zhang Z, Qin M, Sun Y. Nipple Discharge of CA15-3, CA125, CEA and TSGF as a New Biomarker Panel for Breast Cancer. International Journal of Molecular Sciences. 2014; 15(6):9546-9565. https://doi.org/10.3390/ijms15069546
Chicago/Turabian StyleWang, Gangping, Yan Qin, Junxi Zhang, Jinhui Zhao, Yun'ai Liang, Zuofeng Zhang, Meihua Qin, and Yanqing Sun. 2014. "Nipple Discharge of CA15-3, CA125, CEA and TSGF as a New Biomarker Panel for Breast Cancer" International Journal of Molecular Sciences 15, no. 6: 9546-9565. https://doi.org/10.3390/ijms15069546
APA StyleWang, G., Qin, Y., Zhang, J., Zhao, J., Liang, Y., Zhang, Z., Qin, M., & Sun, Y. (2014). Nipple Discharge of CA15-3, CA125, CEA and TSGF as a New Biomarker Panel for Breast Cancer. International Journal of Molecular Sciences, 15(6), 9546-9565. https://doi.org/10.3390/ijms15069546