
Adventitial Tertiary Lymphoid Organs as Potential Source of MicroRNA Biomarkers for Abdominal Aortic Aneurysm

 ,
,
Abstract
:
1. Introduction
2. Results and Discussion
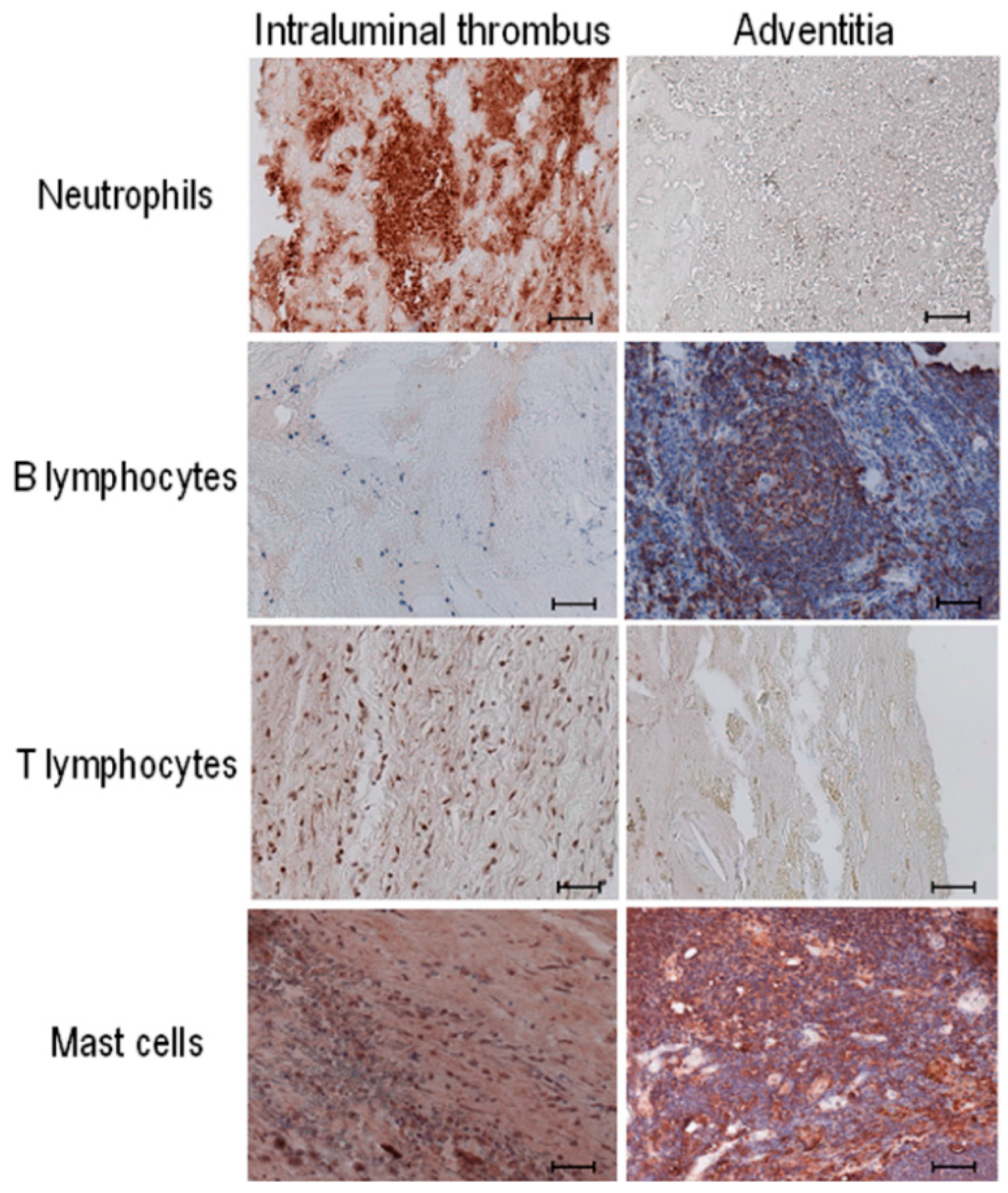
2.1. Distribution of Inflammatory Cells in the Human Aneurysmal Aortic Wall

2.2. Presence of Adventitial Tertiary Lymphoid Organs


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Number | Thickness (mm) | ATLO (%) | Area (mm²) | ATLO (%) | ||
|---|---|---|---|---|---|---|
| ATLO | Total | ATLO | Total | |||
| 6 | 2.1 | 6 | 35.0 | 3.9 | 25.0 | 15.6 |
| 8 | 1.4 | 3.3 | 42.4 | 3.5 | 12.8 | 27.3 |
| 11 | 0.7 | 4.5 | 15.6 | 0.5 | 30.5 | 1.6 |
| 13 | 0.5 | 5.5 | 9.1 | 0.4 | 20.3 | 2.0 |
| 15 | 0.5 | 2.4 | 20.8 | 0.4 | 62.1 | 0.6 |
| 19 | 2.2 | 5.8 | 37.9 | 5.3 | 29.5 | 18.0 |
| 20 | 1.7 | 4.4 | 38.6 | 5.1 | 19.6 | 26.0 |
| Mean | 1.3 | 4.6 | 28.5 | 2.7 | 28.5 | 9.6 |
2.3. Profile and Quantification of miRNAs in Adventitial Tertiary Lymphoid Organs (ATLOs) Isolated by Laser Capture Microdissection
| miRNA | Normalized Mean Values ± SD [Sample 1–Sample 2] | miRNA | Normalized Mean Values ± SD [Sample 1–Sample 2] |
|---|---|---|---|
| let-7b-3p | 4.73 ± 2.21 [6.30–3.17] | miR-320b | 8.93 ± 0.22 [9.08–8.77] |
| let-7e-5p | 5.24 ± 0.032 [5.22–5.27] | miR-325 | 5.15 ± 0.72 [4.64–5.66] |
| let-7f-5p | 5.24 ± 1.49 [4.18–6.29] | miR-330-3p | 9.23 ± 2.37 [7.56–10.91] |
| let-7f-2-3p | 7.90 ± 0.10 [7.83–7.97] | miR-337-3p | 2.70 ± 1.19 [1.86–3.54] |
| miR-101-3p | 5.71 ± 0.37 [5.97–5.45] | miR-337-5p | 2.70 ± 1.139 [1.86–3.54] |
| miR-106a-3p | 10.56 ± 0.99 [11.26–9.86] | miR-339-5p | 3.74 ± 2.02 [5.17–2.31] |
| miR-107 | 8.38 ± 0.11 [8.31–8.46] | miR-33a-3p | 3.13 ± 1.58 [2.02–4.24] |
| miR-1179 | 4.42 ± 0.48 [4.76–4.08] | miR-340-5p | 4.22 ± 2.40 [2.52–5.92] |
| miR-1181 | 3.79 ± 0.49 [4.14–3.44] | miR-342-3p | 5.72 ± 0.19 [5.58–5.85] |
| miR-1183 | 4.92 ± 1.85 [3.61–6.22] | miR-345-5p | 3.43 ± 1.29 [4.34–2.52] |
| miR-1201_v15.0 | 4.73 ± 2.21 [6.29–3.17] | miR-34a-5p | 6.41 ± 1.14 [5.61–7.22] |
| miR-1203 | 5.72 ± 0.19 [5.58–5.85] | miR-34a-3p | 3.62 ± 2.49 [5.38–1.86] |
| miR-1208 | 7.05 ± 0.00 [7.05–7.05] | miR-34c-3p | 8.40 ± 0.26 [8.58–8.22] |
| miR-122-5p | 3.01 ± 1.82 [4.29–1.72] | miR-362-3p | 5.89 ± 1.13 [5.09–6.69] |
| miR-1224-3p | 4.73 ± 2.21 [6.29–3.17] | miR-369-5p | 10.56 ± 0.99 [11.26–9.86] |
| miR-1224-5p | 3.19 ± 1.92 [4.55–1.84] | miR-370-3p | 2.55 ± 2.73 [4.48–0.62] |
| miR-1226-3p | 1.59 ± 0.91 [2.23–0.95] | miR-374a-3p | 7.66 ± 0.03 [7.68–7.64] |
| miR-1234-3p | 4.73 ± 2.21 [6.29–3.17] | miR-379-3p | 3.07 ± 1.37 [4.05–2.10] |
| miR-1238-3p | 3.07 ± 1.37 [4.05–2.10] | miR-409-5p | 1.59 ± 0.91 [2.23–0.95] |
| miR-1250-5p | 7.48 ± 0.77 [8.02–6.93] | miR-431-3p | 5.30 ± 1.02 [4.58–6.03] |
| miR-1251-5p | 4.92 ± 1.85 [3.61–6.22] | miR-432-3p | 1.59 ± 0.91 [2.23–0.95] |
| miR-1252-5p | 4.63 ± 1.54 [3.54–5.72] | miR-451a | 4.92 ± 1.85 [3.61–6.22] |
| miR-125b-1-3p | 1.76 ± 2.44 [3.49–0.03] | miR-452-3p | 4.79 ± 0.21 [4.94–4.64] |
| miR-1262 | 6.13 ± 0.74 [6.65–5.61] | miR-454-5p | 5.98 ± 0.18 [5.85–6.10] |
| miR-1267 | 4.73 ± 2.21 [6.29–3.17] | miR-483-5p | 2.95 ± 2.34 [1.30–4.61] |
| miR-127-3p | 5.71 ± 0.37 [5.97–5.45] | miR-486-5p | 6.10 ± 1.24 [6.98–5.22] |
| miR-1280 | 1.76 ± 2.44 [3.49–0.03] | miR-487a-3p | 4.42 ± 0.48 [4.76–4.08] |
| miR-1281 | 5.15 ± 0.72 [4.64–5.66] | miR-487b-3p | 7.30 ± 0.79 [7.82–6.74] |
| miR-1282 | 3.74 ± 2.02 [5.17–2.31] | miR-488-5p | 2.34 ± 1.03 [3.07–1.61] |
| miR-1290 | 4.66 ± 0.60 [4.24–5.08] | miR-489-3p | 12.42 ± 0.00 [12.42–12.42] |
| miR-1294 | 3.43 ± 0.70 [3.93–2.94] | miR-493-3p | 6.52 ± 1.05 [7.26–5.78] |
| miR-1296-5p | 3.53 ± 2.19 [5.08–1.99] | miR-497-5p | 5.71 ± 0.37 [5.97–5.45] |
| miR-1303 | 5.15 ± 0.72 [4.64–5.66] | miR-504-5p | 4.15 ± 0.59 [3.73–4.57] |
| miR-1307-3p | 5.37 ± 0.62 [4.93–5.81] | miR-508-5p | 4.22 ± 2.40 [2.52–5.92] |
| miR-130b-5p | 6.12 ± 0.45 [5.80–6.44] | miR-513a-5p | 6.26 ± 1.77 [5.00–7.51] |
| miR-132-5p | 4.73 ± 2.21 [6.29–3.17] | miR-517a-3p | 8.90 ± 0.34 [8.65–9.14] |
| miR-1321 | 5.71 ± 0.376 [5.97–5.45] | miR-517b-3p | 10.35 ± 0.26 [10.53–10.16] |
| miR-1323 | 7.57 ± 0.63 [7.13–8.02] | miR-518a-5p | 4.73 ± 2.21 [6.29–3.17] |
| miR-136-5p | 6.43 ± 0.96 [5.75–7.11] | miR-518c-5p | 3.79 ± 0.49 [4.14–3.44] |
| miR-136-3p | 3.91 ± 1.75 [2.68–5.15] | miR-519e-5p | 3.07 ± 1.36 [2.11–4.03] |
| miR-140-3p | 3.42 ± 1.83 [2.13–4.72] | miR-522-3p | 9.29 ± 0.41 [9.59–9.00] |
| miR-144-5p | 6.87 ± 0.03 [6.89–6.85] | miR-548c-3p | 8.38 ± 0.11 [8.31–8.46] |
| miR-146a-5p | 9.65 ± 0.37 [9.92–9.39] | miR-548g-3p | 2.70 ± 1.19 [1.86–3.54] |
| miR-147a | 3.92 ± 0.07 [3.98–3.87] | miR-548m | 4.66 ± 0.60 [4.24–5.08] |
| miR-155-3p | 6.52 ± 1.05 [7.26–5.78] | miR-548p | 4.73 ± 2.21 [6.29–3.17] |
| miR-15a-3p | 10.35 ± 0.26 [10.53–10.16] | miR-550a-5p | 3.92 ± 2.18 [5.46–2.38] |
| miR-17-3p | 0.95 ± 0.77 [1.50–0.41] | miR-551b-3p | 2.55 ± 2.73 [4.48–0.62] |
| miR-181a-5p | 7.72 ± 0.04 [7.75–7.70] | miR-552-3p | 3.13 ± 1.58 [2.02–4.24] |
| miR-181a-2-3p | 7.54 ± 1.05 [6.80–8.28] | miR-555 | 3.42 ± 1.89 [2.08–4.75] |
| miR-183-5p | 4.1 ± 1.18 [3.24–4.93] | miR-571 | 4.73 ± 2.21 [6.29–3.17] |
| miR-184 | 6.01 ± 0.45 [5.69–6.33] | miR-573 | 4.73 ± 2.21 [6.29–3.17] |
| miR-185-3p | 6.87 ± 0.03 [6.89–6.85] | miR-574-5p | 8.38 ± 0.27 [8.18–8.57] |
| miR-186-5p | 1.82 ± 0.35 [1.58–2.07] | miR-578 | 4.64 ± 0.92 [5.29–3.99] |
| miR-186-3p | 2.04 ± 2.62 [3.90–0.19] | miR-584-5p | 10.34 ± 1.44 [9.32–11.36] |
| miR-187-5p | 3.74 ± 2.02 [5.17–2.31] | miR-591 | 5.95 ± 0.77 [5.41–6.50] |
| miR-18b-5p | 8.08 ± 0.00 [8.08–8.08] | miR-592 | 6.73 ± 0.53 [7.10–6.35] |
| miR-1912 | 3.04 ± 0.08 [3.09–2.98] | miR-593-3p | 4.76 ± 2.32 [3.12–6.40] |
| miR-196b-5p | 3.42 ± 1.89 [2.08–4.75] | miR-599 | 5.98 ± 0.12 [5.90–6.07] |
| miR-197-3p | 8.17 ± 1.03 [7.44–8.89] | miR-607 | 0.95 ± 0.77 [1.50–0.41] |
| miR-199a-3p | 6.01 ± 0.45 [5.69–6.33] | miR-615-3p | 2.70 ± 1.19 [1.86–3.54] |
| miR-200a-5p | 4.73 ± 2.21 [6.29–3.17] | miR-616-5p | 7.62 ± 0.44 [7.94–7.31] |
| miR-200c-3p | 3.91 ± 1.75 [2.68–5.15] | miR-619-3p | 4.73 ± 2.21 [6.29–3.17] |
| miR-202-3p | 1.57 ± 1.087 [2.34–0.80] | miR-621 | 8.38 ± 0.27 [8.18–8.57] |
| miR-202-5p | 6.87 ± 0.03 [6.89–6.85] | miR-624-5p | 9.15 ± 0.47 [8.81–9.48] |
| miR-205-5p | 4.64 ± 0.92 [5.29–3.99] | miR-628-3p | 6.26 ± 1.77 [5.00–7.51] |
| miR-206 | 5.98 ± 0.18 [5.85–6.10] | miR-637 | 3.19 ± 1.92 [4.55–1.84] |
| miR-218-1-3p | 3.43 ± 1.29 [4.34–2.52] | miR-642a-5p | 6.78 ± 0.27 [6.59–6.98] |
| miR-218-2-3p | 5.02 ± 2.39 [6.72–3.33] | miR-646 | 4.73 ± 2.21 [6.29–3.17] |
| miR-220c_v15.0 | 4.64 ± 0.92 [5.29–3.99] | miR-654-5p | 9.29 ± 0.41 [9.59–9.00] |
| miR-23b-3p | 5.02 ± 2.39 [6.72–3.33] | miR-661 | 3.17 ± 2.65 [5.05–1.30] |
| miR-26b-5p | 9.86 ± 0.24 [10.03–9.69] | miR-663b | 4.80 ± 0.12 [4.72–4.89] |
| miR-27a-5p | 8.69 ± 0.06 [8.73–8.65] | miR-758-3p | 6.43 ± 0.96 [5.75–7.11] |
| miR-296-5p | 8.93 ± 0.22 [9.08–8.77] | miR-770-5p | 4.92 ± 1.85 [3.61–6.22] |
| miR-29a-3p | 3.92 ± 2.18 [5.46–2.38] | miR-802 | 4.42 ± 0.48 [4.76–4.08] |
| miR-29c-3p | 3.04 ± 0.08 [3.09–2.98] | miR-873-5p | 4.22 ± 2.40 [2.52–5.92] |
| miR-302b-3p | 2.57 ± 2.64 [4.44–0.71] | miR-875-5p | 3.13 ± 1.58 [2.02–4.24] |
| miR-302d-5p | 4.15 ± 0.59 [3.73–4.57] | miR-877-3p | 2.01 ± 0.489 [2.35–1.68] |
| miR-30a-5p | 12.42 ± 0.00 [12.42–12.42] | miR-891b | 7.62 ± 0.44 [7.94–7.31] |
| miR-30a-3p | 3.43 ± 1.29 [4.34–2.52] | miR-922 | 2.12 ± 2.78 [4.09–0.16] |
| miR-30c-1-3p | 8.09 ± 0.43 [8.39–7.78] | miR-924 | 2.70 ± 1.19 [1.86–3.54] |
| miR-32-5p | 4.15 ± 0.51 [4.51–3.80] | miR-92b-5p | 4.63 ± 1.54 [3.54–5.72] |
| miR-32-3p | 5.34 ± 1.88 [4.01–6.67] | miR-935 | 9.23 ± 2.37 [7.56–10.91] |

| Cardiovascular Risk Factors | AAA ( n = 24) | PAD ( n = 18) | p |
|---|---|---|---|
| Age, years | 68.0 ± 6.1 | 63.3 ± 6.6 | 0.006 |
| Male gender (%) | 24 (100) | 18 (100) | ND |
| Current smoking | 4 (17) | 4 (22) | 0.71 |
| Past smoking | 14 (58) | 12 (67) | 0.75 |
| Hypercholesterolemia | 15 (63) | 10 (56) | 0.75 |
| Diabetes mellitus | 4 (17) | 5 (28) | 0.46 |
| Familial history of CAD | 4 (17) | 2 (13) | 1.0 |

3. Experimental Section
3.1. Human Abdominal Aorta and Plasma Samples
3.2. Histological Analysis and Immunohistochemistry
3.3. Laser Capture Microdissection (LCM)
3.4. RNA Extraction, miRNA Screening and qRT-PCR Analyses
3.5. Statistical Analysis
4. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kochanek, K.D.; Xu, J.; Murphy, S.L.; Miniño, A.M.; Kung, H.C. Deaths: Final data for 2009. Natl. Vital Stat. Rep. 2011, 60, 1–116. [Google Scholar] [PubMed]
- Moxon, J.V.; Parr, A.; Emeto, T.I.; Walker, P.; Norman, P.E.; Golledge, J. Diagnosis and monitoring of abdominal aortic aneurysm: Current status and future prospects. Curr. Probl. Cardiol. 2010, 35, 512–548. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ba, Y.; Ma, L.; Cai, X.; Yin, Y.; Wang, K.; Guo, J.; Zhang, Y.; Chen, J.; Guo, X.; et al. Characterization of microRNAs in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Pahl, M.C.; Derr, K.; Gäbel, G.; Hinterseher, I.; Elmore, J.R.; Schworer, C.M.; Peeler, T.C.; Franklin, D.P.; Gray, J.L.; Carey, D.J.; et al. MicroRNA expression signature in human abdominal aortic aneurysms. BMC Med. Genomics 2012, 5, 25. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.M. Controlling the expansion of abdominal aortic aneurysms. Br. J. Surg. 2003, 90, 879–898. [Google Scholar] [CrossRef]
- Reeps, C.; Pelisek, J.; Seidl, S.; Schuster, T.; Zimmermann, A.; Kuehnl, A.; Eckstein, H.H. Inflammatory infiltrates and neovessels are relevant sources of MMPs in abdominal aortic aneurysm wall. Pathobiology 2009, 76, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Lohoefer, F.; Reeps, C.; Lipp, C.; Rudelius, M.; Zimmermann, A.; Ockert, S.; Eckstein, H.H.; Pelisek, J. Histological analysis of cellular localization of cathepsins in abdominal aortic aneurysm wall. Int. J. Exp. Pathol. 2012, 93, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Houard, X.; Touat, Z.; Ollivier, V.; Louedec, L.; Philippe, M.; Sebbag, U.; Meilhac, O.; Rossignol, P.; Michel, J.B. Mediators of neutrophil recruitment in human abdominal aortic aneurysms. Cardiovasc. Res. 2009, 82, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Boytard, L.; Spear, R.; Chinetti-Gbaguidi, G.; Acosta-Martin, A.E.; Vanhoutte, J.; Lamblin, N.; Staels, B.; Amouyel, P.; Haulon, S.; Pinet, F. Role of proinflammatory CD68+ mannose receptor− macrophages in peroxiredoxin-1 expression and in abdominal aortic aneurysms in humans. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Chertov, O.; Ueda, H.; Xu, L.L.; Tani, K.; Murphy, W.J.; Wang, J.M.; Howard, O.M.Z.; Sayers, T.J.; Oppenheimet, J.J. Identification of human neutrophil-derived cathepsin G and azurocidin/CAP37 as chemoattractants for mononuclear cells and neutrophils. J. Exp. Med. 1997, 186, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, V.; Jacob, M.P.; Houard, X.; Rossignol, P.; Plissonnier, D.; Angles-Cano, E.; Michel, J.B. Involvement of the mural thrombus as a site of protease release and activation in human aortic aneurysms. Am. J. Pathol. 2002, 161, 1701–1710. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Sun, J.; Lindholt, J.S.; Sukhova, G.K.; Sinnamon, M.; Stevens, R.L.; Adachi, R.; Libby, P.; Thompson, R.W.; Shi, G.P. Mast cell tryptase deficiency attenuates mouse abdominal aortic aneurysm formation. Circ. Res. 2011, 108, 1316–1327. [Google Scholar] [CrossRef] [PubMed]
- Krishnaswamy, G.; Ajitawi, O.; Chi, D.S. The human mast cell: An overview. Methods Mol. Biol. 2006, 315, 13–34. [Google Scholar] [PubMed]
- Moos, M.P.; John, N.; Gräbner, R.; Nossmann, S.; Günther, B.; Vollandt, R.; Funk, C.D.; Kaiser, B.; Habenicht, A.J. The lamina adventitia is the major site of immune cell accumulation in standard chow-fed apolipoprotein E-deficient mice. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2386–2391. [Google Scholar] [CrossRef] [PubMed]
- Gräbner, R.; Lötzer, K.; Döpping, S.; Hildner, M.; Radke, D.; Beer, M.; Spanbroek, R.; Lippert, B.; Reardon, C.A.; Getz, G.S.; et al. Lymphotoxin β receptor signaling promotes tertiary lymphoid organogenesis in the aorta adventitia of aged ApoE−/− mice. J. Exp. Med. 2009, 206, 233–248. [Google Scholar] [CrossRef] [PubMed]
- Neyt, K.; Perros, F.; Geurtsvankessel, C.H.; Hammad, H.; Lambrecht, B.N. Tertiary lymphoid organs in infection and autoimmunity. Trends Immunol. 2012, 33, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Akhavanpoor, M.; Wangler, S.; Gleissner, C.A.; Korosoglou, G.; Katus, H.A.; Erbel, C. Adventitial inflammation and its interaction with intimal atherosclerotic lesions. Front. Physiol. 2014, 5, 296. [Google Scholar] [CrossRef] [PubMed]
- Lamblin, N.; Ratajczak, P.; Hot, D.; Dubois, E.; Chwastyniak, M.; Beseme, O.; Drobecq, H.; Lemoine, Y.; Koussa, M.; Amouyel, P.; et al. Profile of macrophages in human abdominal aortic aneurysms: A transcriptomic, proteomic, and antibody protein array study. J. Proteome Res. 2010, 9, 3720–3729. [Google Scholar] [CrossRef] [PubMed]
- Dua, M.M.; Dalman, R.L. Hemodynamic influences on abdominal aortic aneurysm disease: Application of biomechanics to aneurysm pathophysiology. Vascul. Pharmacol. 2010, 53, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.B.; Martin-Ventura, J.L.; Egido, J.; Sakalihasan, N.; Treska, V.; Lindholt, J.; Allaire, E.; Thorsteinsdottir, U.; Cockerill, G.; Swedenborg, J. Novel aspects of the pathogenesis of aneurysms of the abdominal aorta in humans. Cardiovasc. Res. 2011, 90, 18–27. [Google Scholar] [CrossRef] [PubMed]
- McCormick, M.L.; Gavrila, D.; Weintraub, N.L. Role of oxidative stress in the pathogenesis of abdominal aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Sagan, A.; Mrowiecki, W.; Mikolajczyk, T.P.; Urbanski, K.; Siedlinski, M.; Nosalski, R.; Korbut, R.; Guzik, T.J. Local inflammation is associated with aortic thrombus formation in abdominal aortic aneurysms. Relationship to clinical risk factors. Thromb. Haemost. 2012, 108, 812–823. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.B.; Thaunat, O.; Houard, X.; Meilhac, O.; Caligiuri, G.; Nicoletti, A. Topological determinants and consequences of adventitial responses to arterial wall injury. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1259–1268. [Google Scholar] [CrossRef] [PubMed]
- Bobryshev, Y.V.; Lord, R.S. Vascular-associated lymphoid tissue (VALT) involvement in aortic aneurysm. Atherosclerosis 2001, 154, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Varin, A.; Gordon, S. Alternative activation of macrophages: Immune function and cellular biology. Immunobiology 2009, 214, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Sho, E.; Sho, M.; Nanjo, H.; Kawamura, K.; Masuda, H.; Dalman, R.L. Comparison of cell-type-specific vs. transmural aortic gene expression in experimental aneurysms. J. Vasc. Surg. 2005, 41, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Guedj, K.; Khallou-Laschet, J.; Clement, M.; Morvan, M.; Gaston, AT.; Fornasa, G.; Dai, J.; Gervais-Taurel, M.; Eberl, G.; Michel, J.B.; et al. M1 macrophages act as LTβR-independent lymphoid tissue inducer cells during atherosclerosis-related lymphoid neogenesis. Cardiovasc. Res. 2014, 101, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Das, K.; Saikolappan, S.; Dhandayuthapani, S. Differential expression of miRNAs by macrophages infected with virulent and avirulent Mycobacterium tuberculosis. Tuberculosis 2013, 93, S47–S50. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Wang, Y.H.; Qu, G.J.; Sun, T.T.; Li, F.Q.; Jiang, W.; Luo, S.S. Differentiated miRNA expression and validation of signaling pathways in apoE gene knockout mice by cross-verification microarray platform. Exp. Mol. Med. 2013, 45, e13. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.Y.; She, X.M.; Qin, Y.; Chu, Z.B.; Chen, L.; Ai, L.S.; Zhang, L.; Hu, Y. miR-15a and miR-16 affect the angiogenesis of multiple myeloma by targeting VEGF. Carcinogenesis 2013, 34, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Sixt, M.; Kanazawa, N.; Selg, M.; Samson, T.; Roos, G.; Reinhardt, D.P.; Pabst, R.; Lutz, M.B.; Sorokin, L. The conduit system transports soluble antigens from the afferent lymph to resident dendritic cells in the T cell area of the lymph node. Immunity 2005, 22, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Liu, F.; Zhou, L.Y.; Long, B.; Yuan, S.M.; Wang, Y.; Liu, C.Y.; Sun, T.; Zhang, X.J.; Li, P.F. The long noncoding RNA CHRF regulates cardiac hypertrophy by targeting miR-489. Circ. Res. 2014, 114, 1377–1388. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spear, R.; Boytard, L.; Blervaque, R.; Chwastyniak, M.; Hot, D.; Vanhoutte, J.; Staels, B.; Lemoine, Y.; Lamblin, N.; Pruvot, F.-R.; et al. Adventitial Tertiary Lymphoid Organs as Potential Source of MicroRNA Biomarkers for Abdominal Aortic Aneurysm. Int. J. Mol. Sci. 2015, 16, 11276-11293. https://doi.org/10.3390/ijms160511276
Spear R, Boytard L, Blervaque R, Chwastyniak M, Hot D, Vanhoutte J, Staels B, Lemoine Y, Lamblin N, Pruvot F-R, et al. Adventitial Tertiary Lymphoid Organs as Potential Source of MicroRNA Biomarkers for Abdominal Aortic Aneurysm. International Journal of Molecular Sciences. 2015; 16(5):11276-11293. https://doi.org/10.3390/ijms160511276
Chicago/Turabian StyleSpear, Rafaelle, Ludovic Boytard, Renaud Blervaque, Maggy Chwastyniak, David Hot, Jonathan Vanhoutte, Bart Staels, Yves Lemoine, Nicolas Lamblin, François-René Pruvot, and et al. 2015. "Adventitial Tertiary Lymphoid Organs as Potential Source of MicroRNA Biomarkers for Abdominal Aortic Aneurysm" International Journal of Molecular Sciences 16, no. 5: 11276-11293. https://doi.org/10.3390/ijms160511276