
Epidermal Growth Factor Receptor Status in Circulating Tumor Cells as a Predictive Biomarker of Sensitivity in Castration-Resistant Prostate Cancer Patients Treated with Docetaxel Chemotherapy


Abstract
:1. Introduction
2. Results
2.1. CTC Count
2.2. Baseline CTC Count Correlation with Patient Characteristics
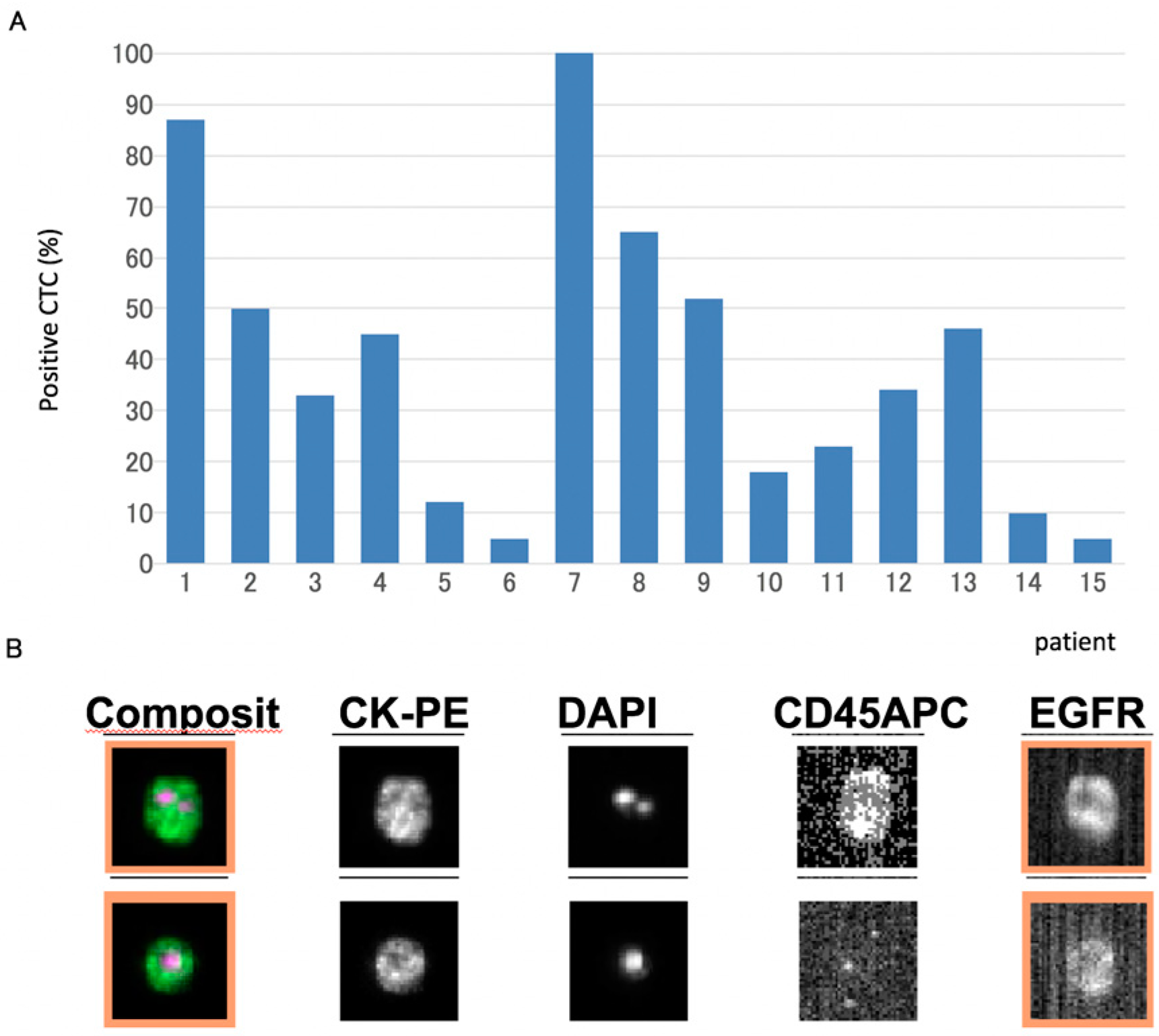
2.3. Analysis of Epidermal Growth Factor Receptor (EGFR) Protein Expression in CTCs
2.4. Multivariate Analyses Indicate that CTCs at Baseline Are an Independent Predictor of Overall Survival
3. Discussion
4. Materials and Methods
4.1. Patient Characteristics
4.2. Drug Administration
4.3. Samples
4.4. Isolation and Enumeration of Circulating Tumor Cells (CTCs—CellSearch System)
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Shah, R.B.; Ghosh, D.; Elder, J.T. Epidermal growth factor receptor (ErbB1) expression in prostate cancer progression: Correlation with androgen independence. Prostate 2006, 66, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Culig, Z.; Hobisch, A.; Cronauer, M.V.; Radmayr, C.; Hittmair, A.; Zhang, J.; Thurnher, M.; Bartsch, G.; Klocker, H. Regulation of prostatic growth and function by peptide growth factors. Prostate 1996, 28, 392–405. [Google Scholar] [CrossRef]
- MacDonald, A.; Habib, F.K. Divergent responses to epidermal growth factor in hormone sensitive and insensitive human prostate cancer cell lines. Br. J. Cancer 1992, 65, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Sherwood, E.R.; van Dongen, J.L.; Wood, C.G.; Liao, S.; Kozlowski, J.M.; Lee, C. Epidermal growth factor receptor activation in androgen-independent but not androgen-stimulated growth of human prostatic carcinoma cells. Br. J. Cancer 1998, 77, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Sarkis, A.; Reuter, V.; Cohen, D.; Netto, G.; Petrylak, D.; Lianes, P.; Fuks, Z.; Mendelsohn, J.; Cordon-Cardo, C. Changing pattern of expression of the epidermal growth factor receptor and transforming growth factor alpha in the progression of prostatic neoplasms. Clin. Cancer Res. 1995, 1, 545–550. [Google Scholar] [PubMed]
- Di Lorenzo, G.; Tortora, G.; D’Armiento, F.P.; de Rosa, G.; Staibano, S.; Autorino, R.; D’Armiento, M.; de Laurentiis, M.; de Placido, S.; Catalano, G.; et al. Expression of epidermal growth factor receptor correlates with disease relapse and progression to androgen-independence in human prostate cancer. Clin. Cancer Res. 2002, 8, 3438–3444. [Google Scholar] [PubMed]
- Scher, H.I.; Jia, X.; de Bono, J.S.; Fleisher, M.; Pienta, K.J.; Raghavan, D.; Heller, G. Circulating tumour cells as prognostic markers in progressive, castration-resistant prostate cancer: A reanalysis of IMMC38 trial data. Lancet Oncol. 2009, 10, 233–239. [Google Scholar] [CrossRef]
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.; Uhr, J.W.; Terstappen, L.W. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef] [PubMed]
- De Bono, J.S.; Scher, H.I.; Montgomery, R.B.; Miller, M.C.; Tissing, H.; Doyle, G.V.; Terstappen, L.W.; Pienta, K.J.; Raghavan, D. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin. Cancer Res. 2008, 14, 6302–6309. [Google Scholar] [CrossRef] [PubMed]
- Olmos, D.; Arkenau, H.T.; Ang, J.E.; Ledaki, I.; Attard, G.; Carden, C.P.; Reid, A.H.; A‘Hern, R.; Fong, P.C.; Oomen, N.B.; et al. Circulating tumour cell (CTC) counts as intermediate end points in castration-resistant prostate cancer (CRPC): A single-centre experience. Ann. Oncol. 2009, 20, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Okegawa, T.; Nutahara, K.; Higashihara, E. Prognostic significance of circulating tumor cells in patients with hormone refractory prostate cancer. J. Urol. 2009, 181, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Goldkorn, A.; Ely, B.; Quinn, D.I.; Tangen, C.M.; Fink, L.M.; Xu, T.; Twardowski, P.; van Veldhuizen, P.J.; Agarwal, N.; Carducci, M.A.; et al. Circulating Tumor Cell Counts Are Prognostic of Overall Survival in SWOG S0421: A Phase III Trial of Docetaxel With or Without Atrasentan for Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2014, 32, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Heller, G.; Molina, A.; Attard, G.; Danila, D.C.; Jia, X.; Peng, W.; Sandhu, S.K.; Olmos, D.; Riisnaes, R.; et al. Circulating tumor cell biomarker panel as an individual-level surrogate for survival in metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2015, 33, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Okegawa, T.; Itaya, N.; Hara, H.; Tambo, M.; Nutahara, K. Circulating tumor cells as a biomarker predictive of sensitivity to docetaxel chemotherapy in patients with castration-resistant prostate cancer. Anti-Cancer Res. 2014, 34, 6705–6710. [Google Scholar]
- Hynes, N.E.; Lane, H.A. ERBB receptors and cancer: The complexity of targeted inhibitors. Nat. Rev. Cancer 2005, 5, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Baek, K.H.; Hong, M.E.; Jung, Y.Y.; Lee, C.H.; Lee, T.J.; Park, E.S.; Kim, M.K.; Yoo, J.H.; Lee, S.W. Correlation of AR, EGFR, and HER2 Expression Levels in Prostate Cancer: Immunohistochemical Analysis and Chromogenic In situ Hybridization. Cancer Res. Treat. 2012, 44, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Leotoing, L.; Manin, M.; Monte, D.; Baron, S.; Communal, Y.; Lours, C.; Veyssière, G.; Morel, L.; Beaudoin, C. Crosstalk between androgen receptor and epidermal growth factor receptor-signalling pathways: A molecular switch for epithelial cell differentiation. J. Mol. Endocrinol. 2007, 39, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Theil, G.; Fischer, K.; Weber, E.; Medek, R.; Hoda, R.; Lücke, K.; Fornara, P. The Use of a New CellCollector to Isolate Circulating Tumor Cells from the Blood of Patients with Different Stages of Prostate Cancer and Clinical Outcomes—A Proof-of-Concept Study. PLoS ONE 2016, 11, e0158354. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, D.R.; Leversha, M.A.; Danila, D.C.; Lin, O.; Gonzalez-Espinoza, R.; Gu, B.; Anand, A.; Smith, K.; Maslak, P.; Doyle, G.V.; et al. Circulating tumor cell analysis in patients with progressive castration-resistant prostate cancer. Clin. Cancer Res. 2007, 13, 2023–2029. [Google Scholar] [CrossRef] [PubMed]
- Vila, A.; Abal, M.; Muinelo-Romay, L.; Rodriguez-Abreu, C.; Rivas, J.; López-López, R.; Costa, C. EGFR-Based Immunoisolation as a Recovery Target for Low-EpCAM CTC Subpopulation. PLoS ONE 2016, 11, e0163705. [Google Scholar] [CrossRef] [PubMed]
- Serrano, M.J.; Ortega, F.G.; Alvarez-Cubero, M.J.; Nadal, R.; Sanchez-Rovira, P.; Salido, M.; Rodríguez, M.; García-Puche, J.L.; Delgado-Rodriguez, M.; Solé, F.; et al. EMT and EGFR in CTCs cytokeratin negative non-metastatic breast cancer. Oncotarget 2014, 5, 7486–7497. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Lu, C.; Wang, H.; Luber, B.; Nakazawa, M.; Roeser, J.C.; Chen, Y.; Mohammad, T.A.; Chen, Y.; Fedor, H.L.; et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N. Engl. J. Med. 2014, 371, 1028–1038. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Lu, C.; Luber, B.; Wang, H.; Chen, Y.; Nakazawa, M.; Nadal, R.; Paller, C.J.; Denmeade, S.R.; Carducci, M.A.; et al. Androgen Receptor Splice Variant 7 and Efficacy of Taxane Chemotherapy in Patients With Metastatic Castration-Resistant Prostate Cancer. JAMA Oncol. 2015, 1, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Bryce, A.H.; Antonarakis, E.S. Androgen receptor splice variant 7 in castration-resistant prostate cancer: Clinical considerations. Int. J. Urol. 2016, 23, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Okegawa, T.; Nutahara, K.; Higashihara, E. Immunomagnetic quantification of circulating tumors cell as a prognostic factor of androgen-deprivation responsiveness in hormone-naive metastatic prostate cancer patients. J. Urol. 2008, 180, 1342–1347. [Google Scholar] [CrossRef] [PubMed]
- Soloway, M.S.; Hardeman, S.W.; Hickey, D.; Raymond, J.; Todd, B.; Soloway, S.; Moinuddin, M. Stratification of patients with metastatic prostate cancer based on extent of disease on initial bone scan. Cancer 1998, 61, 195–202. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | N | CTC/7.5 mL | p-Value | |
|---|---|---|---|---|
| Mean | Range | |||
| CTC count at base | 60 | 8 | 0–184 | 0.042 |
| PSA (ng/mL) | ||||
| <30 | 30 | 2 | 0–3 | 0.021 |
| ≥30 | 30 | 15 | 0–184 | |
| Biopsy Gleason score | ||||
| 7–8 | 29 | 2 | 0–6 | 0.003 |
| 9–10 | 31 | 19 | 0–184 | |
| EOD | ||||
| 1–2 | 39 | 1 | 0–14 | 0.034 |
| 3–4 | 21 | 23 | 0–184 | |
| Hemoglobin (g/dL) | ||||
| <11.5 | 35 | 18 | 0–184 | 0.059 |
| ≥11.5 | 25 | 5 | 0–13 | |
| Serum albumin (g/dL) | ||||
| <3.7 | 28 | 19 | 0–184 | 0.059 |
| ≥3.7 | 22 | 4 | 0–12 | |
| Alkaline phosphatase (IU/L) | ||||
| <313 | 21 | 3 | 0–34 | 0.002 |
| ≥313 | 39 | 18 | 0–184 | |
| Lactate dehydrogenase (IU/L) | ||||
| <226 | 26 | 2 | 0–18 | 0.066 |
| ≥226 | 34 | 19 | 0–184 | |
| Disease involvement | ||||
| Only bone | 42 | 6 | 0–45 | 0.014 |
| Bone plus node | 18 | 15 | 0–184 | |
| Variables | No. | Univariate Analysis | Multivariate Analysis | Hazard Ratio | 95% CI |
|---|---|---|---|---|---|
| CTC count | |||||
| CTC < 5 | 23 | 0.001 | 0.002 | 3.24 | 1.2–4.3 |
| CTC ≥ 5 | 37 | ||||
| CTC-EGFR | |||||
| (−) | 45 | <0.001 | <0.001 | 4.01 | 1.1–6.8 |
| (+) | 15 | ||||
| PSA (ng/mL) | |||||
| <30 | 30 | 0.015 | 0.053 | 4.01 | 1.1–6.8 |
| ≥30 | 30 | ||||
| Biopsy Gleason score | |||||
| 7–8 | 29 | 0.011 | 0.42 | 1.02 | 0.6–2.9 |
| 9–10 | 31 | ||||
| EOD | |||||
| 1–2 | 39 | 0.012 | 0.285 | 1.49 | 0.5–6.8 |
| 3–4 | 21 | ||||
| Hemoglobin (g/dL) | |||||
| <11.5 | 35 | 0.028 | 0.247 | 1.11 | 0.6–5.6 |
| ≥11.5 | 25 | ||||
| Serum albumin (g/dL) | |||||
| <3.7 | 38 | 0.029 | 0.312 | 1.08 | 0.7–5.9 |
| ≥3.7 | 22 | ||||
| Alkaline phosphatase (IU/L) | |||||
| <313 | 21 | 0.003 | 0.017 | 2.46 | 1.2-5.3 |
| ≥313 | 39 | ||||
| Lactate dehydrogenase (IU/L) | |||||
| <226 | 26 | 0.008 | 0.121 | 1.9 | 0.5–2.9 |
| ≥226 | 34 | ||||
| Disease involvement | |||||
| Only bone | 42 | 0.071 | 0.226 | 1.17 | 0.6–2.4 |
| Bone plus node | 18 | ||||
| No. of Patients | n = 60 |
|---|---|
| Mean age | 71 (57–82) |
| median PSA (ng/mL) | 33.7 (9.4–3241.7) |
| ≤10.0 | 2 (3.3%) |
| 10.1–20 | 12 (20.0%) |
| 20.1–30 | 16 (26.7%) |
| 30.1–40 | 7 (11.7%) |
| 40.1–50 | 7 (11.7%) |
| 50.1–100 | 11 (18.3%) |
| ≥100.1 | 5 (8.3%) |
| Gleason score | |
| 7 | 8 (13.3%) |
| 8 | 21 (35.0%) |
| 9 | 19 (31.7%) |
| 10 | 12 (20.0%) |
| EOD | |
| 1 | 20 (33.3%) |
| 2 | 19 (31.7%) |
| 3 | 13 (21.7%) |
| 4 | 8 (13.3%) |
| Disease involvement | |
| Only bone | 32 (53.3%) |
| Bone plus node | 28 (46.7%) |
| WHO perfomance score | |
| 0 | 56 (93.3%) |
| 1 | 4 (6.7%) |
| Median Hemoglobin (g/dL) | 10.6 (9.1–12.9) |
| Median serum albumin (g/dL) | 3.4 (2.9–4.1) |
| Median alkaline phosphatase (IU/L) | 342 (178–561) |
| Median lactate dehydrogenase (IU/L) | 265 (189–438) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okegawa, T.; Itaya, N.; Hara, H.; Tambo, M.; Nutahara, K. Epidermal Growth Factor Receptor Status in Circulating Tumor Cells as a Predictive Biomarker of Sensitivity in Castration-Resistant Prostate Cancer Patients Treated with Docetaxel Chemotherapy. Int. J. Mol. Sci. 2016, 17, 2008. https://doi.org/10.3390/ijms17122008
Okegawa T, Itaya N, Hara H, Tambo M, Nutahara K. Epidermal Growth Factor Receptor Status in Circulating Tumor Cells as a Predictive Biomarker of Sensitivity in Castration-Resistant Prostate Cancer Patients Treated with Docetaxel Chemotherapy. International Journal of Molecular Sciences. 2016; 17(12):2008. https://doi.org/10.3390/ijms17122008
Chicago/Turabian StyleOkegawa, Takatsugu, Naoshi Itaya, Hidehiko Hara, Mitsuhiro Tambo, and Kikuo Nutahara. 2016. "Epidermal Growth Factor Receptor Status in Circulating Tumor Cells as a Predictive Biomarker of Sensitivity in Castration-Resistant Prostate Cancer Patients Treated with Docetaxel Chemotherapy" International Journal of Molecular Sciences 17, no. 12: 2008. https://doi.org/10.3390/ijms17122008
APA StyleOkegawa, T., Itaya, N., Hara, H., Tambo, M., & Nutahara, K. (2016). Epidermal Growth Factor Receptor Status in Circulating Tumor Cells as a Predictive Biomarker of Sensitivity in Castration-Resistant Prostate Cancer Patients Treated with Docetaxel Chemotherapy. International Journal of Molecular Sciences, 17(12), 2008. https://doi.org/10.3390/ijms17122008