Pancreatic Ductal Adenocarcinoma: Current and Evolving Therapies



Abstract
:1. Introduction
2. Disease Staging-Essential Factor in Pancreatic Ductal Adenocarcinoma (PDAC) Therapy
3. Therapy for Metastatic Cancer
3.1. Gemcitabine
3.2. Combination Therapies: Gemcitabine-Based Therapies
3.3. Abraxane and FOLFIRINOX: New Hope or Defeat?
4. Surgery—The Cornerstone of PDAC Therapy
5. Neoadjuvant and Adjuvant Therapies
5.1. Neoadjuvant Therapy in Resectable Patients
5.2. Neoadjuvant Therapy in Borderline Resectable and Locally Advanced PDAC
5.3. Adjuvant Therapy in PDAC
6. Targeted Therapies—A New Prospect for PDAC Treatment?
6.1. Targeting Growth Factor Receptors
6.2. KRAS Pathways Inhibition
6.3. Targeting Angiogenesis
6.4. Other Targets
6.5. Targeting Tumour–Stroma Interactions
7. Immunotherapy for Pancreatic Cancer
8. miRNAs in PDAC Therapy
9. Second-Line Therapies
10. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| ARBs | Angiotensin II receptor blockers |
| BRPC | Borderline resectable pancreatic cancer |
| CA19-9 | Carbohydrate antigen 19-9 |
| CAR T | Chimeric antigen receptor T |
| CXC | Chemokine |
| CDF | Difluorinated-curcumin |
| CDKN | Cyclin-dependent kinase inhibitor |
| CRP | C-reactive protein |
| CSF1R | Colony stimulating factor 1 receptor |
| CT | Computed tomography; |
| CTGF | Connective tissue growth factor |
| CTLA4 | Cytotoxic T-lymphocyte-associated protein 4 |
| DIM | 3,3′-diindolylmethane |
| DDL4 | Delta like canonical notch ligand 4 |
| ECE1 | Endothelin converting enzyme 1 |
| ECF | Extracellular matrix |
| EGF | Epidermal growth factor |
| FAK | Focal adhesion kinase |
| FDA | Food and Drug Administration |
| FLT3 | Tyrosine-protein kinase |
| Gy | Gray |
| HA | Hyaluronic acid |
| hENT | Human equilibrative nucleoside transporter |
| IGF1R | Insulin-like growth factor 1 receptor |
| JAK | Janus kinase |
| LAPC | Locally advanced pancreatic cancer |
| LN | Lymph-node ratio |
| LV | Leucovorin |
| MAGE-A3 | Melanoma-associated antigen 3 |
| MAPK | Mitogen-activated protein kinase |
| MLH1 | MutL homolog 1 |
| neoCRT | Neoadjuvant chemoradiotherapy |
| OS | Overall survival |
| PanIN | Pancreatic intraepithelial neoplasia |
| PARP | Poly ADP ribose polymerase |
| PD | Pancreaticoduodenectomy |
| PDAC | Pancreatic ductal adenocarcinoma |
| PDGFR | Platelet-derived growth factor receptor |
| PD-L1 | Programmed death-ligand 1 |
| PFS | Progression free survival |
| PS | Performance status |
| PSCs | Pancreatic stellate cells |
| PV | Portal vein |
| RT | Radiotherapy |
| SMAD4 | Mothers against decapentaplegic homolog 4 |
| SMV | Superior mesenteric vein |
| SOCS1 | Suppressor of cytokine signalling 1 |
| PUMA | p53 upregulated modulator of apoptosis |
| TK | Tyrosine kinase |
| TNM | Tumour node metastasis |
| VEGFR | Vascular endothelial growth factor receptor |
References
- Garrido-Laguna, I.; Hidalgo, M. Pancreatic cancer: From state-of-the-art treatments to promising novel therapies. Nat. Rev. Clin. Oncol. 2015, 12, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Vincent, A.; Herman, J.; Schulick, R.; Hruban, R.H.; Goggins, M. Pancreatic cancer. Lancet 2011, 378, 607–620. [Google Scholar] [CrossRef]
- Maitra, A.; Hruban, R.H. Pancreatic cancer. Annu. Rev. Pathol. 2008, 3, 157–188. [Google Scholar] [CrossRef] [PubMed]
- Bailey, P.; Chang, D.K.; Nones, K.; Johns, A.L.; Patch, A.-M.; Gingras, M.-C.; Miller, D.K.; Christ, A.N.; Bruxner, T.J.C.; Quinn, M.C.; et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature 2016, 531, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Pothula, S.P.; Wilson, J.S.; Apte, M.V. Pancreatic cancer and its stroma: A conspiracy theory. World J. Gastroenterol. 2014, 20, 11216–11229. [Google Scholar] [CrossRef] [PubMed]
- Neesse, A.; Krug, S.; Gress, T.M.; Tuveson, D.A.; Michl, P. Emerging concepts in pancreatic cancer medicine: Targeting the tumor stroma. OncoTargets Ther. 2013, 7, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Feig, C.; Gopinathan, A.; Neesse, A.; Chan, D.S.; Cook, N.; Tuveson, D.A. The pancreas cancer microenvironment. Clin. Cancer Res. 2012, 18, 4266–4276. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H.; Pisters, P.W.T.; Evans, D.B.; Sun, C.C.; Lee, J.E.; Fleming, J.B.; Vauthey, J.N.; Abdalla, E.K.; Crane, C.H.; Wolff, R.A.; et al. Borderline resectable pancreatic cancer: The importance of this emerging stage of disease. J. Am. Coll. Surg. 2008, 206, 833–846. [Google Scholar]
- Fishman, E.K.; Horton, K.M. Imaging pancreatic cancer: The role of multidetector CT with three-dimensional ct angiography. Pancreatology 2001, 1, 610–624. [Google Scholar] [CrossRef] [PubMed]
- Lal, A.; Christians, K.; Evans, D.B. Management of borderline resectable pancreatic cancer. Surg. Oncol. Clin. 2010, 19, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Semelka, R.C.; Escobar, L.A.; Ansari, N.A.; Semelka, C.T.A. Magnetic resonance imaging of adenocarcinoma of the pancreas. In Abdomen and Thoracic Imaging: An Engineering & Clinical Perspective; El-Baz, A.S., Saba, L., Suri, J., Eds.; Springer: Boston, MA, USA, 2014; pp. 209–231. [Google Scholar]
- Ahmed, S.I.; Bochkarev, V.; Oleynikov, D.; Sasson, A.R. Patients with pancreatic adenocarcinoma benefit from staging laparoscopy. J. Laparoendosc. Adv. Surg. Tech. 2006, 16, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.C.; Kim, H.J.; Park, J.H.; Park, D.I.; Cho, Y.K.; Sohn, C.I.; Jeon, W.K.; Kim, B.I.; Shin, J.H. Can preoperative CA19–9 and CEA levels predict the resectability of patients with pancreatic adenocarcinoma? J. Gastroenterol. Hepatol. 2009, 24, 1869–1875. [Google Scholar] [CrossRef] [PubMed]
- TNM Classification for Pancreatic Cancer. Available online: http://emedicine.medscape.com/article/2007121overview?pa=7JOgwY44yH5KPOj7lOoHr90n1HBozexR7tG2ZcdMvk9XnTOjrYyWn0RWz46AAKcqQ%2Fcre5qzB2a9T3Us%2F7EKdTRbGMQ7s%2F89oYHt2gMBBbM%3D (accessed on 10 May 2017).
- Katz, M.H.G.; Hwang, R.; Fleming, J.B.; Evans, D.B. Tumor-node-metastasis staging of pancreatic adenocarcinoma. CA Cancer J. Clin. 2008, 58, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Sohn, T.A.; Yeo, C.J.; Cameron, J.L.; Koniaris, L.; Kaushal, S.; Abrams, R.A.; Sauter, P.K.; Coleman, J.; Hruban, R.H.; Lillemoe, K.D. Resected adenocarcinoma of the pancreas-616 patients: Results, outcomes, and prognostic indicators. J. Gastrointest. Surg. 2000, 4, 567–579. [Google Scholar] [CrossRef]
- Kondo, S.; Katoh, H.; Hirano, S.; Ambo, Y.; Tanaka, E.; Okushiba, S.; Morikawa, T. Results of radical distal pancreatectomy with en bloc resection of the celiac artery for locally advanced cancer of the pancreatic body. Langenbeck's Arch. Surg. 2003, 388, 101–106. [Google Scholar]
- Hammel, P.; Huguet, F.; van Laethem, J.L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouche, O.; Shannon, J.; Andre, T.; et al. Effect of chemoradiotherapy vs. chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib: The LAP07 randomized clinical trial. JAMA 2016, 315, 1844–1853. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R. Pancreatic Cancer: Treatment Options. Available online: http://www.cancer.net/cancer-types/pancreatic-cancer/treatment-options (accessed on 10 September 2016).
- Neoptolemos, J.P.; Cunningham, D.; Friess, H.; Bassi, C.; Stocken, D.D.; Tait, D.M.; Dunn, J.A.; Dervenis, C.; Lacaine, F.; Hickey, H.; et al. Adjuvant therapy in pancreatic cancer: Historical and current perspectives. Ann. Oncol. 2003, 14, 675–692. [Google Scholar] [CrossRef] [PubMed]
- Mallinson, C.N.; Rake, M.; Cocking, J.B.; Fox, C.A.; Cwynarski, M.T.; Diffey, B.L.; Jackson, G.A.; Hanley, J.; Wass, V.J. Chemotherapy in pancreatic cancer: Results of a controlled, prospective, randomised, multicentre trial. Br. Med. J. 1980, 281, 1589–1591. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A., 3rd; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [PubMed]
- Rothenberg, M.L.; Moore, M.J.; Cripps, M.C.; Andersen, J.S.; Portenoy, R.K.; Burris, H.A., 3rd; Green, M.R.; Tarassoff, P.G.; Brown, T.D.; Casper, E.S.; et al. A phase II trial of gemcitabine in patients with 5-FU-refractory pancreas cancer. Ann. Oncol. 1996, 7, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Di Costanzo, F.; Carlini, P.; Doni, L.; Massidda, B.; Mattioli, R.; Iop, A.; Barletta, E.; Moscetti, L.; Recchia, F.; Tralongo, P.; et al. Gemcitabine with or without continuous infusion 5-FU in advanced pancreatic cancer: A randomised phase II trial of the Italian oncology group for clinical research (GOIRC). Br. J. Cancer 2005, 93, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, M.; di Cicilia, R.; Macchini, M.; Nobili, E.; Vecchiarelli, S.; Brandi, G.; Biasco, G. Metastatic pancreatic cancer: Is gemcitabine still the best standard treatment? (Review). Oncol. Rep. 2010, 23, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.J.; Joo, K.R.; Park, N.H.; Yun, T.K.; Nah, Y.W.; Nam, C.W.; Park, J.H. Gemcitabine therapy in patients with advanced pancreatic cancer. Korean J. Intern. Med. 2002, 17, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Poplin, E.; Wasan, H.; Rolfe, L.; Raponi, M.; Ikdahl, T.; Bondarenko, I.; Davidenko, I.; Bondar, V.; Garin, A.; Boeck, S.; et al. Randomized, multicenter, phase II study of CO-101 versus gemcitabine in patients with metastatic pancreatic ductal adenocarcinoma: Including a prospective evaluation of the role of hENT1 in gemcitabine or CO-101 sensitivity. J. Clin. Oncol. 2013, 31, 4453–4461. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R. A Clinical Study Comparing Acelarin with Gemcitabine in Patient with Metastatic Pancreatic Carcinoma. Available online: http://www.isrctn.com/ISRCTN16765355 (accessed on 1 March 2017).
- Rocha Lima, C.M.; Green, M.R.; Rotche, R.; Miller, W.H., Jr.; Jeffrey, G.M.; Cisar, L.A.; Morganti, A.; Orlando, N.; Gruia, G.; Miller, L.L. Irinotecan plus gemcitabine results in no survival advantage compared with gemcitabine monotherapy in patients with locally advanced or metastatic pancreatic cancer despite increased tumor response rate. J. Clin. Oncol. 2004, 22, 3776–3783. [Google Scholar] [CrossRef] [PubMed]
- Louvet, C.; Labianca, R.; Hammel, P.; Lledo, G.; Zampino, M.G.; Andre, T.; Zaniboni, A.; Ducreux, M.; Aitini, E.; Taieb, J.; et al. Gemcitabine in combination with oxaliplatin compared with gemcitabine alone in locally advanced or metastatic pancreatic cancer: Results of a GERCOR and GISCAD phase III trial. J. Clin. Oncol. 2005, 23, 3509–3516. [Google Scholar] [CrossRef] [PubMed]
- Oettle, H.; Richards, D.; Ramanathan, R.K.; van Laethem, J.L.; Peeters, M.; Fuchs, M.; Zimmermann, A.; John, W.; Von Hoff, D.; Arning, M.; et al. A phase III trial of pemetrexed plus gemcitabine versus gemcitabine in patients with unresectable or metastatic pancreatic cancer. Ann. Oncol. 2005, 16, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Colucci, G.; Giuliani, F.; Gebbia, V.; Biglietto, M.; Rabitti, P.; Uomo, G.; Cigolari, S.; Testa, A.; Maiello, E.; Lopez, M. Gemcitabine alone or with cisplatin for the treatment of patients with locally advanced and/or metastatic pancreatic carcinoma: A prospective, randomized phase III study of the Gruppo Oncologia dell’Italia Meridionale. Cancer 2002, 94, 902–910. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, V.; Quietzsch, D.; Gieseler, F.; Gonnermann, M.; Schonekas, H.; Rost, A.; Neuhaus, H.; Haag, C.; Clemens, M.; Heinrich, B.; et al. Randomized phase III trial of gemcitabine plus cisplatin compared with gemcitabine alone in advanced pancreatic cancer. J. Clin. Oncol. 2006, 24, 3946–3952. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Chau, I.; Stocken, D.D.; Valle, J.W.; Smith, D.; Steward, W.; Harper, P.G.; Dunn, J.; Tudur-Smith, C.; West, J.; et al. Phase III randomized comparison of gemcitabine versus gemcitabine plus capecitabine in patients with advanced pancreatic cancer. J. Clin. Oncol. 2009, 27, 5513–5518. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, V.; Boeck, S.; Hinke, A.; Labianca, R.; Louvet, C. Meta-analysis of randomized trials: Evaluation of benefit from gemcitabine-based combination chemotherapy applied in advanced pancreatic cancer. BMC Cancer 2008, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sultana, A.; Tudur Smith, C.; Cunningham, D.; Starling, N.; Neoptolemos, J.P.; Ghaneh, P. Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer: Results of secondary end points analyses. Br. J. Cancer 2008, 99, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Reni, M.; Cordio, S.; Milandri, C.; Passoni, P.; Bonetto, E.; Oliani, C.; Luppi, G.; Nicoletti, R.; Galli, L.; Bordonaro, R.; et al. Gemcitabine versus cisplatin, epirubicin, fluorouracil, and gemcitabine in advanced pancreatic cancer: A randomised controlled multicentre phase III trial. Lancet Oncol. 2005, 6, 369–376. [Google Scholar] [CrossRef]
- Sudo, K.; Nakamura, K.; Yamaguchi, T. S-1 in the treatment of pancreatic cancer. World J. Gastroenterol. 2014, 20, 15110–15118. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Sun, J.; Jiang, Z.; Zhang, L.; Liu, G. Gemcitabine and S-1 combination chemotherapy versus gemcitabine alone for locally advanced and metastatic pancreatic cancer: A meta-analysis of randomized controlled trials in Asia. J. Chemother. 2015, 27, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, T.L.; Lertpiriyapong, K.; Cocco, L.; Martelli, A.M.; Libra, M.; Candido, S.; Montalto, G.; Cervello, M.; Steelman, L.; Abrams, S.L.; et al. Roles of EGFR and KRAS and their downstream signaling pathways in pancreatic cancer and pancreatic cancer stem cells. Adv. Biol. Regul. 2015, 59, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Luo, G.; Liu, C.; Cheng, H.; Lu, Y.; Jin, K.; Liu, Z.; Long, J.; Liu, L.; Xu, J.; et al. The prognostic and predictive role of epidermal growth factor receptor in surgical resected pancreatic cancer. Int. J. Mol. Sci. 2016, 17, 1090. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A.; et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: A phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Ottaiano, A.; Capozzi, M.; de Divitiis, C.; de Stefano, A.; Botti, G.; Avallone, A.; Tafuto, S. Gemcitabine mono-therapy versus gemcitabine plus targeted therapy in advanced pancreatic cancer: A meta-analysis of randomized phase III trials. Acta Oncol. 2017, 56, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, R.; Bodoky, G.; Ruhstaller, T.; Glimelius, B.; Bajetta, E.; Schuller, J.; Saletti, P.; Bauer, J.; Figer, A.; Pestalozzi, B.; et al. Gemcitabine plus capecitabine compared with gemcitabine alone in advanced pancreatic cancer: A randomized, multicenter, phase III trial of the Swiss Group for Clinical Cancer Research and the Central European Cooperative Oncology Group. J. Clin. Oncol. 2007, 25, 2212–2217. [Google Scholar] [CrossRef] [PubMed]
- Boeck, S.; Hoehler, T.; Seipelt, G.; Mahlberg, R.; Wein, A.; Hochhaus, A.; Boeck, H.P.; Schmid, B.; Kettner, E.; Stauch, M.; et al. Capecitabine plus oxaliplatin (CapOx) versus capecitabine plus gemcitabine (CapGem) versus gemcitabine plus oxaliplatin (mGemOx): Final results of a multicenter randomized phase II trial in advanced pancreatic cancer. Ann. Oncol. 2008, 19, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Fine, R.L.; Fogelman, D.R.; Schreibman, S.M.; Desai, M.; Sherman, W.; Strauss, J.; Guba, S.; Andrade, R.; Chabot, J. The gemcitabine, docetaxel, and capecitabine (GTX) regimen for metastatic pancreatic cancer: A retrospective analysis. Cancer Chemother. Pharmacol. 2008, 61, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Hurt, C.N.; Bridgewater, J.; Falk, S.; Cummins, S.; Wasan, H.; Crosby, T.; Jephcott, C.; Roy, R.; Radhakrishna, G.; et al. Gemcitabine-based or capecitabine-based chemoradiotherapy for locally advanced pancreatic cancer (SCALOP): A multicentre, randomised, phase II trial. Lancet Oncol. 2013, 14, 317–326. [Google Scholar] [CrossRef]
- Heinemann, V.; Wilke, H.; Mergenthaler, H.-G.; Clemens, M.; König, H.; Illiger, H.J.; Arning, M.; Schalhorn, A.; Possinger, K.; Fink, U. Gemcitabine and cisplatin in the treatment of advanced or metastatic pancreatic cancer. Ann. Oncol. 2000, 11, 1399–1403. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; El-Maraghi, R.H.; Hammel, P.; Heinemann, V.; Kunzmann, V.; Sastre, J.; Scheithauer, W.; Siena, S.; Tabernero, J.; Teixeira, L.; et al. nab-Paclitaxel plus gemcitabine for metastatic pancreatic cancer: Long-term survival from a phase III trial. J. Natl. Cancer Inst. 2015, 107, dju413. [Google Scholar] [CrossRef] [PubMed]
- Frese, K.K.; Neesse, A.; Cook, N.; Bapiro, T.E.; Lolkema, M.P.; Jodrell, D.I.; Tuveson, D.A. nab-Paclitaxel potentiates gemcitabine activity by reducing cytidine deaminase levels in a mouse model of pancreatic cancer. Cancer Discov. 2012, 2, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Thota, R.; Pauff, J.M.; Berlin, J.D. Treatment of metastatic pancreatic adenocarcinoma: A review. Oncology 2014, 28, 70–74. [Google Scholar] [PubMed]
- Martín, A.J.M.; Alfonso, P.G.; Rupérez, A.B.; Jiménez, M.M. Nab-paclitaxel plus gemcitabine as first-line palliative chemotherapy in a patient with metastatic pancreatic cancer with Eastern Cooperative Oncology Group performance status of 2. Oncol. Lett. 2016, 12, 727–730. [Google Scholar] [PubMed]
- Corrie, P.; Qian, W.; Jodrell, D.I.; Lao-Sirieix, S.; Whittaker, P.; Gopinathan, A.; Chhabra, A.; Dalchau, K.; Basu, B.; Hardy, R.; et al. 747TiP scheduling Nab-Paclitaxel with Gemcitabine (Siege): Randomised phase II trial to investigate two different schedules of Nab-Paclitaxel (ABX) combined with Gemcitabine (Gem) as first line treatment for metastatic pancreatic adenocarcinoma (PDAC). Ann. Oncol. 2014, 25, iv252. [Google Scholar]
- Ueno, H.; Okusaka, T.; Funakoshi, A.; Ishii, H.; Yamao, K.; Ishikawa, O.; Ohkawa, S.; Saitoh, S. A phase II study of weekly irinotecan as first-line therapy for patients with metastatic pancreatic cancer. Cancer Chemother. Pharmacol. 2007, 59, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Azrak, R.G.; Cao, S.; Slocum, H.K.; Toth, K.; Durrani, F.A.; Yin, M.B.; Pendyala, L.; Zhang, W.; McLeod, H.L.; Rustum, Y.M. Therapeutic synergy between irinotecan and 5-fluorouracil against human tumor xenografts. Clin. Cancer Res. 2004, 10, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Mitry, E.; Ould-Kaci, M.; Boige, V.; Seitz, J.F.; Bugat, R.; Breau, J.L.; Bouche, O.; Etienne, P.L.; Tigaud, J.M.; et al. Randomized phase II study evaluating oxaliplatin alone, oxaliplatin combined with infusional 5-FU, and infusional 5-FU alone in advanced pancreatic carcinoma patients. Ann. Oncol. 2004, 15, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Zeghari-Squalli, N.; Raymond, E.; Cvitkovic, E.; Goldwasser, F. Cellular pharmacology of the combination of the DNA topoisomerase I inhibitor SN-38 and the diaminocyclohexane platinum derivative oxaliplatin. Clin. Cancer Res. 1999, 5, 1189–1196. [Google Scholar] [PubMed]
- Ychou, M.; Conroy, T.; Seitz, J.F.; Gourgou, S.; Hua, A.; Mery-Mignard, D.; Kramar, A. An open phase I study assessing the feasibility of the triple combination: Oxaliplatin plus irinotecan plus leucovorin/5-fluorouracil every 2 weeks in patients with advanced solid tumors. Ann. Oncol. 2003, 14, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Gourgou-Bourgade, S.; Bascoul-Mollevi, C.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Boige, V.; et al. Impact of FOLFIRINOX compared with gemcitabine on quality of life in patients with metastatic pancreatic cancer: Results from the PRODIGE 4/ACCORD 11 randomized trial. J. Clin. Oncol. 2012, 31, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Sirohi, B.; Dawood, S.; Rastogi, S.; Pandey, A.; Bal, M.; Shetty, N.; Shrikhande, S.V. Treatment of patients with metastatic pancreatic cancer: Experience from a tertiary Indian cancer center. Indian J. Cancer 2015, 52, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Peddi, P.F.; Lubner, S.; McWilliams, R.; Tan, B.R.; Picus, J.; Sorscher, S.M.; Suresh, R.; Lockhart, A.C.; Wang, J.; Menias, C.; et al. Multi-institutional experience with FOLFIRINOX in pancreatic adenocarcinoma. J. Pancreas 2012, 13, 497–501. [Google Scholar]
- Mahaseth, H.; Brutcher, E.; Kauh, J.; Hawk, N.; Kim, S.; Chen, Z.; Kooby, D.A.; Maithel, S.K.; Landry, J.; El-Rayes, B.F. Modified FOLFIRINOX regimen with improved safety and maintained efficacy in pancreatic adenocarcinoma. Pancreas 2013, 42, 1311–1315. [Google Scholar] [CrossRef] [PubMed]
- Berlin, J.D.; Catalano, P.; Thomas, J.P.; Kugler, J.W.; Haller, D.G.; Benson, A.B., 3rd. Phase III study of gemcitabine in combination with fluorouracil versus gemcitabine alone in patients with advanced pancreatic carcinoma: Eastern Cooperative Oncology Group Trial E2297. J. Clin. Oncol. 2002, 20, 3270–3275. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Surgery for Pancreatic Cancer. Available online: https://www.cancer.org/cancer/pancreatic-cancer/treating/surgery.html (accessed on 12 May 2017).
- Michalski, C.W.; Weitz, J.; Buchler, M.W. Surgery insight: Surgical management of pancreatic cancer. Nat. Clin. Pract. Oncol. 2007, 4, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Dunn, J.A.; Almond, J.; Beger, H.G.; Pederzoli, P.; Bassi, C.; Dervenis, C.; Fernandez-Cruz, L.; Lacaine, F.; et al. Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial. Ann. Surg. 2001, 234, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.G., II; Scoggins, C.R.; Egnatashvili, V.; Staley, C.A.; McMasters, K.M.; Kooby, D.A. Arterial and venous resection for pancreatic adenocarcinoma: Operative and long-term outcomes. Arch. Surg. 2009, 144, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.F.; Raut, C.P.; Lee, J.E.; Pisters, P.W.T.; Vauthey, J.-N.; Abdalla, E.K.; Gomez, H.F.; Sun, C.C.; Crane, C.H.; Wolff, R.A.; et al. Pancreaticoduodenectomy with vascular resection: Margin status and survival duration. J. Gastrointest. Surg. 2004, 8, 935–950. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Tao, R.; Lei, R.; Han, B.; Cheng, D.; Shen, B.; Peng, C. Distal pancreatectomy combined with celiac axis resection in treatment of carcinoma of the body/tail of the pancreas: A single-center experience. Ann. Surg. Oncol. 2010, 17, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Hirano, S.; Kondo, S.; Hara, T.; Ambo, Y.; Tanaka, E.; Shichinohe, T.; Suzuki, O.; Hazama, K. Distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic body cancer: Long-term results. Ann. Surg. 2007, 246, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Gebhardt, C.; Meyer, W.; Reichel, M.; Wünsch, P.H. Prognostic factors in the operative treatment of ductal pancreatic carcinoma. Langenbeck’s Arch. Surg. 2000, 385, 14–20. [Google Scholar] [CrossRef]
- Kedra, B.; Popiela, T.; Sierzega, M.; Precht, A. Prognostic factors of long-term survival after resective procedures for pancreatic cancer. Hepatogastroenterology 2001, 48, 1762–1766. [Google Scholar] [PubMed]
- Raut, C.P.; Tseng, J.F.; Sun, C.C.; Wang, H.; Wolff, R.A.; Crane, C.H.; Hwang, R.; Vauthey, J.-N.; Abdalla, E.K.; Lee, J.E.; et al. Impact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann. Surg. 2007, 246, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Michalski, C.W.; Kleeff, J.; Wente, M.N.; Diener, M.K.; Büchler, M.W.; Friess, H. Systematic review and meta-analysis of standard and extended lymphadenectomy in pancreaticoduodenectomy for pancreatic cancer. Br. J. Surg. 2007, 94, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Riall, T.S.; Cameron, J.L.; Lillemoe, K.D.; Campbell, K.A.; Sauter, P.K.; Coleman, J.; Abrams, R.A.; Laheru, D.; Hruban, R.H.; Yeo, C.J. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinomad—Part 3: Update on 5-year survival. J. Gastrointest. Surg. 2005, 9, 1191–1206. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, R.E.; Smith, D.D. Extent of lymph node retrieval and pancreatic cancer survival: Information from a large US population database. Ann. Surg. Oncol. 2006, 13, 1189–1200. [Google Scholar] [CrossRef] [PubMed]
- Prashant, S.; Jonathan, T.; Mauricio, S.; James, S.; Peter, D. Advanced age is a risk factor for post-operative complications and mortality after a pancreaticoduodenectomy: A meta-analysis and systematic review. HPB 2012, 14, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Hishinuma, S.; Ogata, Y.; Tomikawa, M.; Ozawa, I.; Hirabayashi, K.; Igarashi, S. Patterns of recurrence after curative resection of pancreatic cancer, based on autopsy findings. J. Gastrointest. Surg. 2006, 10, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Oettle, H.; Post, S.; Neuhaus, P.; Gellert, K.; Langrehr, J.; Ridwelski, K.; Schramm, H.; Fahlke, J.; Zuelke, C.; Burkart, C.; et al. Adjuvant chemotherapy with gemcitabine vs. observation in patients undergoing curative-intent resection of pancreatic cancer: A randomized controlled trial. JAMA 2007, 297, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A.; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N. Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.H.; Ellenberg, S.S. Pancreatic cancer: Adjuvant combined radiation and chemotherapy following curative resection. Arch. Surg. 1985, 120, 899–903. [Google Scholar] [CrossRef]
- Cooper, A.B.; Tzeng, C.-W.D.; Katz, M.H.G. Treatment of borderline resectable pancreatic cancer. Curr. Treat. Opt. Oncol. 2013, 14, 293–310. [Google Scholar] [CrossRef] [PubMed]
- Pisters, P.W.T.; Hudec, W.A.; Lee, J.E.; Raijman, I.; Lahoti, S.; Janjan, N.A.; Rich, T.A.; Crane, C.H.; Lenzi, R.; Wolff, R.A.; et al. Preoperative chemoradiation for patients with pancreatic cancer: Toxicity of endobiliary stents. J. Clin. Oncol. 2000, 18, 860. [Google Scholar] [CrossRef] [PubMed]
- Quiros, R.M.; Brown, K.M.; Hoffman, J.P. Neoadjuvant therapy in pancreatic cancer. Cancer Investig. 2007, 25, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Spitz, F.R.; Abbruzzese, J.L.; Lee, J.E.; Pisters, P.W.; Lowy, A.M.; Fenoglio, C.J.; Cleary, K.R.; Janjan, N.A.; Goswitz, M.S.; Rich, T.A.; et al. Preoperative and postoperative chemoradiation strategies in patients treated with pancreaticoduodenectomy for adenocarcinoma of the pancreas. J. Clin. Oncol. 1997, 15, 928–937. [Google Scholar] [CrossRef] [PubMed]
- Papavasiliou, P.; Chun, Y.S.; Hoffman, J.P. How to define and manage borderline resectable pancreatic cancer. Surg. Clin. N. Am. 2013, 93, 663–674. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, S.; Schäfer, M.; Weber, A.; Hany, T.F.; Bhure, U.; Pestalozzi, B.C.; Clavien, P.-A. Neoadjuvant chemotherapy generates a significant tumor response in resectable pancreatic cancer without increasing morbifity: Results of a prospective phase II trial. Ann. Surg. 2008, 248, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Stokes, J.B.; Nolan, N.J.; Stelow, E.B.; Walters, D.M.; Weiss, G.R.; de Lange, E.E.; Rich, T.A.; Adams, R.B.; Bauer, T.W. Preoperative capecitabine and concurrent radiation for borderline resectable pancreatic cancer. Ann. Surg. Oncol. 2011, 18, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; O’Reilly, E.M. Novel directions in neoadjuvant therapy for pancreas adenocarcinoma. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 585–601. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.B.; Rich, T.A.; Byrd, D.R.; Cleary, K.R.; Connelly, J.H.; Levin, B.; Charnsangavej, C.; Fenoglio, C.J.; Ames, F.C. Preoperative chemoradiation and pancreaticoduodenectomy for adenocarcinoma of the pancreas. Arch. Surg. 1992, 127, 1335–1339. [Google Scholar] [CrossRef] [PubMed]
- Greer, S.E.; Pipas, J.M.; Sutton, J.E.; Zaki, B.I.; Tsapakos, M.; Colacchio, T.A.; Gibson, J.J.; Wiener, D.C.; Ripple, G.H.; Barth, R.J., Jr. Effect of neoadjuvant therapy on local recurrence after resection of pancreatic adenocarcinoma. J. Am. Coll. Surg. 2008, 206, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Motoi, F.; Unno, M.; Takahashi, H.; Okada, T.; Wada, K.; Sho, M.; Nagano, H.; Matsumoto, I.; Satoi, S.; Murakami, Y.; et al. Influence of preoperative anti-cancer therapy on resectability and perioperative outcomes in patients with pancreatic cancer: Project study by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J. Hepatobiliary Pancreat. Sci. 2014, 21, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Tajima, H.; Ohta, T.; Kitagawa, H.; Okamoto, K.; Sakai, S.; Makino, I.; Kinoshita, J.; Furukawa, H.; Nakamura, K.; Hayashi, H.; et al. Pilot study of neoadjuvant chemotherapy with gemcitabine and oral S-1 for resectable pancreatic cancer. Exp. Ther. Med. 2012, 3, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.B.; Varadhachary, G.R.; Crane, C.H.; Sun, C.C.; Lee, J.E.; Pisters, P.W.T.; Vauthey, J.-N.; Wang, H.; Cleary, K.R.; Staerkel, G.A.; et al. Preoperative gemcitabine-based chemoradiation for patients with resectable adenocarcinoma of the pancreatic head. J. Clin. Oncol. 2008, 26, 3496–3502. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.H.; Stocken, D.D.; Hewitt, H.; Markham, C.E.; Hassan, A.B.; Johnson, P.J.; Buckels, J.A.C.; Bramhall, S.R. A randomized phase 2 trial of neoadjuvant chemotherapy in resectable pancreatic cancer: Gemcitabine alone versus gemcitabine combined with cisplatin. Ann. Surg. Oncol. 2007, 14, 2088–2096. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, S.; Pestalozzi, B.C.; Schäfer, M.; Weber, A.; Bauerfeind, P.; Knuth, A.; Clavien, P.-A. Prospective phase II trial of neoadjuvant chemotherapy with gemcitabine and cisplatin for resectable adenocarcinoma of the pancreatic head. J. Clin. Oncol. 2008, 26, 2526–2531. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.J.; Ben-Josef, E.; Herman, J.M.; Bekaii-Saab, T.; Dawson, L.A.; Griffith, K.A.; Francis, I.R.; Greenson, J.K.; Simeone, D.M.; Lawrence, T.S.; et al. A multi-institutional phase 2 study of neoadjuvant gemcitabine and oxaliplatin with radiation therapy in patients with pancreatic cancer. Cancer 2013, 119, 2692–2700. [Google Scholar] [CrossRef] [PubMed]
- Varadhachary, G.R.; Wolff, R.A.; Crane, C.H.; Sun, C.C.; Lee, J.E.; Pisters, P.W.T.; Vauthey, J.-N.; Abdalla, E.; Wang, H.; Staerkel, G.A.; et al. Preoperative gemcitabine and cisplatin followed by gemcitabine-based chemoradiation for resectable adenocarcinoma of the pancreatic head. J. Clin. Oncol. 2008, 26, 3487–3495. [Google Scholar] [CrossRef] [PubMed]
- Stessin, A.M.; Meyer, J.E.; Sherr, D.L. Neoadjuvant radiation is associated with improved survival in patients with resectable pancreatic cancer: An analysis of data from the surveillance, epidemiology, and end results (SEER) registry. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.P.; Xue, X.J.; Liang, N.; Xu, D.G.; Liu, F.J.; Yu, X.S.; Zhang, J.D. Effect of chemoradiotherapy and neoadjuvant chemoradiotherapy in resectable pancreatic cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2014, 140, 549–559. [Google Scholar] [CrossRef] [PubMed]
- Gillen, S.; Schuster, T.; Meyer zum Büschenfelde, C.; Friess, H.; Kleeff, J. Preoperative/neoadjuvant therapy in pancreatic cancer: A systematic review and meta-analysis of response and resection percentages. PLoS Med. 2010, 7, e1000267. [Google Scholar] [CrossRef] [PubMed]
- Russo, S.; Ammori, J.; Eads, J.; Dorth, J. The role of neoadjuvant therapy in pancreatic cancer: A review. Future Oncol. 2016, 12, 669–685. [Google Scholar] [CrossRef] [PubMed]
- Pisters, P.W.; Abbruzzese, J.L.; Janjan, N.A.; Cleary, K.R.; Charnsangavej, C.; Goswitz, M.S.; Rich, T.A.; Raijman, I.; Wolff, R.A.; Lenzi, R.; et al. Rapid-fractionation preoperative chemoradiation, pancreaticoduodenectomy, and intraoperative radiation therapy for resectable pancreatic adenocarcinoma. J. Clin. Oncol. 1998, 16, 3843–3850. [Google Scholar] [CrossRef] [PubMed]
- Pisters, P.W.T.; Wolff, R.A.; Janjan, N.A.; Cleary, K.R.; Charnsangavej, C.; Crane, C.N.; Lenzi, R.; Vauthey, J.N.; Lee, J.E.; Abbruzzese, J.L.; et al. Preoperative paclitaxel and concurrent rapid-fractionation radiation for resectable pancreatic adenocarcinoma: Toxicities, histologic response rates, and event-free outcome. J. Clin. Oncol. 2002, 20, 2537–2544. [Google Scholar] [CrossRef] [PubMed]
- Tran Cao, H.S.; Balachandran, A.; Wang, H.; Nogueras-González, G.M.; Bailey, C.E.; Lee, J.E.; Pisters, P.W.T.; Evans, D.B.; Varadhachary, G.; Crane, C.H.; et al. Radiographic tumor-vein interface as a predictor of intraoperative, pathologic, and oncologic outcomes in resectable and borderline resectable pancreatic cancer. J. Gastrointest. Surg. 2014, 18, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Varadhachary, G.R.; Tamm, E.P.; Abbruzzese, J.L.; Xiong, H.Q.; Crane, C.H.; Wang, H.; Lee, J.E.; Pisters, P.W.T.; Evans, D.B.; Wolff, R.A. Borderline resectable pancreatic cancer: Definitions, management, and role of preoperative therapy. Ann. Surg. Oncol. 2006, 13, 1035–1046. [Google Scholar] [CrossRef] [PubMed]
- Callery, M.P.; Chang, K.J.; Fishman, E.K.; Talamonti, M.S.; William Traverso, L.; Linehan, D.C. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: Expert consensus statement. Ann. Surg. Oncol. 2009, 16, 1727–1733. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.P.; O’Dwyer, P.; Agarwal, P.; Salazar, H.; Ahmad, N. Preoperative chemoradiotherapy for localized pancreatic carcinoma: A perspective. Cancer 1996, 78, 592–597. [Google Scholar] [CrossRef]
- White, R.R.; Paulson, E.K.; Freed, K.S.; Keogan, M.T.; Hurwitz, H.I.; Lee, C.; Morse, M.A.; Gottfried, M.R.; Baillie, J.; Branch, M.S.; et al. Staging of pancreatic cancer before and after neoadjuvant chemoradiation. J. Gastrointest. Surg. 2001, 5, 626–633. [Google Scholar] [CrossRef]
- Katz, M.H.G.; Fleming, J.B.; Bhosale, P.; Varadhachary, G.; Lee, J.E.; Wolff, R.; Wang, H.; Abbruzzese, J.; Pisters, P.W.T.; Vauthey, J.-N.; et al. Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer 2012, 118, 5749–5756. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.K.; Fisher, G.; Ford, J.A.; Poen, J.C.; Vierra, M.A.; Oberhelman, H.; Niederhuber, J.; Augusto Bastidas, J. Preoperative chemoradiation for marginally resectable adenocarcinoma of the pancreas. J. Gastrointest. Surg. 2001, 5, 27–35. [Google Scholar] [CrossRef]
- Landry, J.; Catalano, P.J.; Staley, C.; Harris, W.; Hoffman, J.; Talamonti, M.; Xu, N.; Cooper, H.; Benson, A.B. Randomized phase II study of gemcitabine plus radiotherapy versus gemcitabine, 5-fluorouracil, and cisplatin followed by radiotherapy and 5-fluorouracil for patients with locally advanced, potentially resectable pancreatic adenocarcinoma. J. Surg. Oncol. 2010, 101, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Sahora, K.; Kuehrer, I.; Eisenhut, A.; Akan, B.; Koellblinger, C.; Goetzinger, P.; Teleky, B.; Jakesz, R.; Peck-Radosavljevic, M.; Ba’ssalamah, A.; et al. NeoGemOx: Gemcitabine and oxaliplatin as neoadjuvant treatment for locally advanced, nonmetastasized pancreatic cancer. Surgery 2011, 149, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-L.; Kim, S.C.; Kim, J.-H.; Lee, S.S.; Kim, T.-W.; Park, D.H.; Seo, D.W.; Lee, S.K.; Kim, M.-H.; Kim, J.H.; et al. Prospective efficacy and safety study of neoadjuvant gemcitabine with capecitabine combination chemotherapy for borderline-resectable or unresectable locally advanced pancreatic adenocarcinoma. Surgery 2012, 152, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Motoi, F.; Ishida, K.; Fujishima, F.; Ottomo, S.; Oikawa, M.; Okada, T.; Shimamura, H.; Takemura, S.; Ono, F.; Akada, M.; et al. Neoadjuvant chemotherapy with gemcitabine and S-1 for resectable and borderline pancreatic ductal adenocarcinoma: Rresults from a prospective multi-institutional phase 2 trial. Ann. Surg. Oncol. 2013, 20, 3794–3801. [Google Scholar] [CrossRef] [PubMed]
- Satoi, S.; Toyokawa, H.; Yanagimoto, H.; Yamamoto, T.; Kamata, M.; Ohe, C.; Sakaida, N.; Uemura, Y.; Kitade, H.; Tanigawa, N.; et al. Neo-adjuvant chemoradiation therapy using S-1 followed by surgical resection in patients with pancreatic cancer. J. Gastrointest. Surg. 2012, 16, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.M.; Chung, Y.E.; Park, J.Y.; Sung, J.S.; Hwang, H.K.; Choi, H.J.; Kim, H.; Song, S.Y.; Lee, W.J. Potential contribution of preoperative neoadjuvant concurrent chemoradiation therapy on margin-negative resection in borderline resectable pancreatic cancer. J. Gastrointest. Surg. 2012, 16, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Sho, M.; Akahori, T.; Tanaka, T.; Kinoshita, S.; Tamamoto, T.; Nomi, T.; Yamato, I.; Hokuto, D.; Yasuda, S.; Kawaguchi, C.; et al. Pathological and clinical impact of neoadjuvant chemoradiotherapy using full-dose gemcitabine and concurrent radiation for resectable pancreatic cancer. J. Hepatobiliary Pancreat. Sci. 2013, 20, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Lopez, N.E.; Prendergast, C.; Lowy, A.M. Borderline resectable pancreatic cancer: Definitions and management. World J. Gastroenterol. 2014, 20, 10740–10751. [Google Scholar] [CrossRef] [PubMed]
- Chuong, M.D.; Springett, G.M.; Freilich, J.M.; Park, C.K.; Weber, J.M.; Mellon, E.A.; Hodul, P.J.; Malafa, M.P.; Meredith, K.L.; Hoffe, S.E.; et al. Stereotactic body radiation therapy for locally advanced and borderline resectable pancreatic cancer is effective and well tolerated. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Nanda, R.H.; El-Rayes, B.; Maithel, S.K.; Landry, J. Neoadjuvant modified FOLFIRINOXfolfirinox and chemoradiation therapy for locally advanced pancreatic cancer improves resectability. J. Surg. Oncol. 2015, 111, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Reni, M.; Cereda, S.; Balzano, G.; Passoni, P.; Rognone, A.; Zerbi, A.; Nicoletti, R.; Mazza, E.; Arcidiacono, P.G.; di Carlo, V.; et al. Outcome of upfront combination chemotherapy followed by chemoradiation for locally advanced pancreatic adenocarcinoma. Cancer Chemother. Pharm. 2009, 64, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Blazer, M.A.; Wu, C.; Goldberg, R. Tolerability and efficacy of modified FOLFIRINOX (mFOLFIRINOX) in patients with borderline-resectable pancreatic cancer (BRPC) and locally advanced unresectable pancreatic cancer (LAURPC). J. Clin. Oncol. 2014, 32. [Google Scholar] [CrossRef]
- Vasile, E.; de Lio, N.; Cappelli, C. Phase II study of neoadjuvant chemotherapy with modified FOLFOXIRI in borderline resectable or unresectable stage III pancreatic cancer. J. Clin. Oncol. 2013, 31. [Google Scholar] [CrossRef]
- Kunzmann, V.; Herrmann, K.; Bluemel, C.; Kapp, M.; Hartlapp, I.; Steger, U. Intensified neoadjuvant chemotherapy with nab-Paclitaxel plus gemcitabine followed by FOLFIRINOX in a patient with locally advanced unresectable pancreatic cancer. Case Rep. Oncol. 2014, 7, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Hosein, P.J.; Macintyre, J.; Kawamura, C.; Maldonado, J.C.; Ernani, V.; Loaiza-Bonilla, A.; Narayanan, G.; Ribeiro, A.; Portelance, L.; Merchan, J.R.; et al. A retrospective study of neoadjuvant FOLFIRINOX in unresectable or borderline-resectable locally advanced pancreatic adenocarcinoma. BMC Cancer 2012, 12, 199. [Google Scholar] [CrossRef] [PubMed]
- Christians, K.K.; Tsai, S.; Mahmoud, A.; Ritch, P.; Thomas, J.P.; Wiebe, L.; Kelly, T.; Erickson, B.; Wang, H.; Evans, D.B.; et al. Neoadjuvant FOLFIRINOX for borderline resectable pancreas cancer: A new treatment paradigm? Oncologist 2014, 19, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, G.; Kountourakis, P.; Papadimitriou, K.; Vassiliou, V.; Papamichael, D. Adjuvant therapy for resectable pancreatic adenocarcinoma: Review of the current treatment approaches and future directions. Cancer Treat. Rev. 2014, 40, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Klinkenbijl, J.H.; Jeekel, J.; Sahmoud, T.; van Pel, R.; Couvreur, M.L.; Veenhof, C.H.; Arnaud, J.P.; Gonzalez, D.G.; de Wit, L.T.; Hennipman, A.; et al. Adjuvant radiotherapy and 5-Fluorouracil after curative resection of cancer of the pancreas and periampullary region: Phase III trial of the EORTC Gastrointestinal Tract Cancer Cooperative Group. Ann. Surg. 1999, 230, 776. [Google Scholar] [CrossRef] [PubMed]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zülke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Bassi, C.; Ghaneh, P.; Cunningham, D.; Goldstein, D.; Padbury, R.; Moore, M.J.; Gallinger, S.; Mariette, C.; et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs. gemcitabine following pancreatic cancer resection: A randomized controlled trial. JAMA 2010, 304, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Regine, W.F.; Winter, K.A.; Abrams, R.; Safran, H.; Hoffman, J.P.; Konski, A.; Benson, A.B.; Macdonald, J.S.; Rich, T.A.; Willett, C.G. Fluorouracil-based chemoradiation with either eemcitabine or fluorouracil chemotherapy after resection ofpPancreatic adenocarcinoma: 5-year analysis of the U.S. Intergroup/RTOG 9704 phase III trial. Ann. Surg. Oncol. 2011, 18, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Uesaka, K.; Boku, N.; Fukutomi, A.; Okamura, Y.; Konishi, M.; Matsumoto, I.; Kaneoka, Y.; Shimizu, Y.; Nakamori, S.; Sakamoto, H.; et al. Adjuvant chemotherapy of S-1 versus gemcitabine for resected pancreatic cancer: A phase 3, open-label, randomised, non-inferiority trial (JASPAC 01). Lancet 2016, 388, 248–257. [Google Scholar] [CrossRef]
- Sinn, M.L.T.; Gellert, K.; Messmann, H.; Bechstein, W.O.; Waldschmidt, D.; Jacobasch, L.; Wilhelm, M.; Rau, B.M.; Grützmann, R.; Weinmann, A.; et al. CONKO-005: Adjuvant therapy in R0 resected pancreatic cancer patients with gemcitabine plus erlotinib versus gemcitabine for 24 weeks—A prospective randomized phase III study. J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Fundation, R. A Phase IIR and a Phase III Trial Evaluating Both Erlotinib (Ph IIR) and Chemoradiation (Ph III) as Adjuvant Treatment for Patients with Resected Head of Pancreas Adenocarcinoma. Available online: https://www.rtog.org/ClinicalTrials/ProtocolTable/StudyDetails.aspx?study=0848 (accessed on 15 May 2017).
- Epelboym, I.; DiNorcia, J.; Winner, M.; Lee, M.K.; Lee, J.A.; Schrope, B.A.; Chabot, J.A.; Allendorf, J.D. Neoadjuvant therapy and vascular resection during pancreaticoduodenectomy: Shifting the survival curve for patients with locally advanced pancreatic cancer. World J. Surg. 2014, 38, 1184–1195. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H.G.; Shi, Q.; Ahmad, S.A.; Herman, J.M.; de Wilton Marsh, R.; Collisson, E.A.; Schwartz, L.H.; Martin, R.C.G.; Conway, W.C.; Truty, M.; et al. Preoperative modified FOLFIRINOX (mFOLFIRINOX) followed by chemoradiation (CRT) for borderline resectable (BLR) pancreatic cancer (PDAC): Initial results from Alliance Trial A021101. J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Bittoni, A.; Santoni, M.; Lanese, A.; Pellei, C.; Andrikou, K.; Stefano, C. Neoadjuvant therapy in pancreatic cancer: An emerging strategy. Gastroenterol. Res. Pract. 2014, 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Lohr, M.; Kloppel, G.; Maisonneuve, P.; Lowenfels, A.B.; Luttges, J. Frequency of K-ras mutations in pancreatic intraductal neoplasias associated with pancreatic ductal adenocarcinoma and chronic pancreatitis: A meta-analysis. Neoplasia 2005, 7, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Eser, S.; Schnieke, A.; Schneider, G.; Saur, D. Oncogenic KRAS signalling in pancreatic cancer. Br. J. Cancer 2014, 111, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Scarpa, A.; Capelli, P.; Mukai, K.; Zamboni, G.; Oda, T.; Iacono, C.; Hirohashi, S. Pancreatic adenocarcinomas frequently show p53 gene mutations. Am. J. Pathol. 1993, 142, 1534–1543. [Google Scholar] [PubMed]
- Yachida, S.; Iacobuzio-Donahue, C.A. Evolution and dynamics of pancreatic cancer progression. Oncogene 2013, 32, 5253–5260. [Google Scholar] [CrossRef] [PubMed]
- Boucher, M.-J.; Morisset, J.; Vachon, P.H.; Reed, J.C.; Lainé, J.; Rivard, N. MEK/ERK signaling pathway regulates the expression of Bcl-2, Bcl-XL, and Mcl-1 and promotes survival of human pancreatic cancer cells. J. Cell. Biochem. 2000, 79, 355–369. [Google Scholar] [CrossRef]
- Jones, S.; Zhang, X.; Parsons, D.W.; Lin, J.C.H.; Leary, R.J.; Angenendt, P.; Mankoo, P.; Carter, H.; Kamiyama, H.; Jimeno, A.; et al. Core signaling pathways in human pancreatic cancers revealed by global genomic analyses. Science 2008, 321, 1801–1806. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Upadhyay, G.; Srivastava, R.K.; Shankar, S. Recent advances in pancreatic cancer: Biology, treatment, and prevention. Biochim. Biophys. Acta 2015, 1856, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.H.; Farrell, A.; Justice, R.; Pazdur, R. Approval summary: Imatinib mesylate in the treatment of metastatic and/or nnresectable malignant gastrointestinal stromal tumors. Oncologist 2009, 14, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.H.; Gootenberg, J.; Keegan, P.; Pazdur, R. FDA drug approval summary: Bevacizumab (Avastin®) plus carboplatin and paclitaxel as first-line treatment of advanced/metastatic recurrent nonsquamous non-small cell lung cancer. Oncologist 2007, 12, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.; Santoni, M.; Amantini, C.; Burattini, L.; Berardi, R.; Santoni, G.; Cascinu, S.; Muzzonigro, G. Progress of molecular targeted therapies for advanced renal cell carcinoma. BioMed Res. Int. 2013, 2013, 9. [Google Scholar] [CrossRef] [PubMed]
- Borja-Cacho, D.; Jensen, E.H.; Saluja, A.K.; Buchsbaum, D.J.; Vickers, S.M. Molecular targeted therapies for pancreatic cancer. Am. J. Surg. 2008, 196, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.A.; Benedetti, J.; Corless, C.L.; Wong, R.; O’Reilly, E.M.; Flynn, P.J.; Rowland, K.M.; Atkins, J.N.; Mirtsching, B.C.; Rivkin, S.E.; et al. Phase III study comparing gemcitabine plus cetuximab versus gemcitabine in patients with advanced pancreatic adenocarcinoma: Southwest Oncology Group-directed intergroup trial S0205. J. Clin. Oncol. 2010, 28, 3605–3610. [Google Scholar] [CrossRef] [PubMed]
- Fountzilas, G.; Bobos, M.; Kalogera-Fountzila, A.; Xiros, N.; Murray, S.; Linardou, H.; Karayannopoulou, G.; Koutras, A.K.; Bafaloukos, D.; Samantas, E.; et al. Gemcitabine combined with gefitinib in patients with inoperable or metastatic pancreatic cancer: A phase II study of the Hellenic Cooperative Oncology Group with biomarker evaluation. Cancer Investig. 2008, 26, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Sawada, T.; Komatsu, M.; Inoue, M.; Muguruma, K.; Nishihara, T.; Yamashita, Y.; Yamada, N.; Ohira, M.; Hirakawa, K. Antitumor effect of trastuzumab for pancreatic cancer with high HER-2 expression and enhancement of effect by combined therapy with gemcitabine. Clin. Cancer Res. 2006, 12, 4925–4932. [Google Scholar] [CrossRef] [PubMed]
- Harder, J.; Ihorst, G.; Heinemann, V.; Hofheinz, R.; Moehler, M.; Buechler, P.; Kloeppel, G.; Rocken, C.; Bitzer, M.; Boeck, S.; et al. Multicentre phase II trial of trastuzumab and capecitabine in patients with HER2 overexpressing metastatic pancreatic cancer. Br. J. Cancer 2012, 106, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Safran, H.; Miner, T.; Bahary, N.; Whiting, S.; Lopez, C.D.; Sun, W.; Charpentier, K.; Shipley, J.; Anderson, E.; McNulty, B.; et al. Lapatinib and gemcitabine for metastatic pancreatic cancer. A phase II study. Am. J. Clin. Oncol. 2011, 34, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Gabrielson, A.; Hwang, J.J.; Pishvaian, M.J.; Weiner, L.M.; Zhuang, T.; Ley, L.; Marshall, J.L.; He, A.R. Phase II study of lapatinib and capecitabine in second-line treatment for metastatic pancreatic cancer. Cancer Chemother. Pharmacol. 2015, 76, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Su, D.; Jiao, S.C.; Wang, L.J.; Shi, W.W.; Long, Y.Y.; Li, J.; Bai, L. Efficacy of nimotuzumab plus gemcitabine usage as first-line treatment in patients with advanced pancreatic cancer. Tumour Biol. 2014, 35, 2313–2318. [Google Scholar] [CrossRef] [PubMed]
- Afatinib as Cancer Therapy for Exocrine Pancreatic Tumours. NCT01728818. Available online: https://clinicaltrials.gov/ct2/show/NCT01728818 (accessed on 4 September 2016).
- Sachdev, D.; Yee, D. Disrupting insulin-like growth factor signaling as a potential cancer therapy. Mol. Cancer Ther. 2007, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.A.; Goldman, B.; Ramanathan, R.K.; Lenz, H.-J.; Lowy, A.M.; Whitehead, R.P.; Wakatsuki, T.; Iqbal, S.; Gaur, R.; Benedetti, J.K.; et al. Dual blockade of epidermal growth factor receptor and insulin-like growth factor receptor-1 signaling in metastatic pancreatic cancer: Phase Ib and randomized phase II trial of gemcitabine, erlotinib, and cixutumumab versus gemcitabine plus erlotinib (SWOG S0727). Cancer 2014, 120, 2980–2985. [Google Scholar] [PubMed]
- Fuchs, C.S.; Azevedo, S.; Okusaka, T.; Van Laethem, J.L.; Lipton, L.R.; Riess, H.; Szczylik, C.; Moore, M.J.; Peeters, M.; Bodoky, G.; et al. A phase 3 randomized, double-blind, placebo-controlled trial of ganitumab or placebo in combination with gemcitabine as first-line therapy for metastatic adenocarcinoma of the pancreas: The GAMMA trial. Ann. Oncol. 2015, 26, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; van de Velde, H.; Karasek, P.; Oettle, H.; Vervenne, W.L.; Szawlowski, A.; Schoffski, P.; Post, S.; Verslype, C.; Neumann, H.; et al. Phase III trial of gemcitabine plus tipifarnib compared with gemcitabine plus placebo in advanced pancreatic cancer. J. Clin. Oncol. 2004, 22, 1430–1438. [Google Scholar] [CrossRef] [PubMed]
- Bodoky, G.; Timcheva, C.; Spigel, D.R.; la Stella, P.J.; Ciuleanu, T.E.; Pover, G.; Tebbutt, N.C. A phase II open-label randomized study to assess the efficacy and safety of selumetinib (AZD6244 [ARRY-142886]) versus capecitabine in patients with advanced or metastatic pancreatic cancer who have failed first-line gemcitabine therapy. Investig. New Drugs 2012, 30, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Infante, J.R.; Somer, B.G.; Park, J.O.; Li, C.P.; Scheulen, M.E.; Kasubhai, S.M.; Oh, D.Y.; Liu, Y.; Redhu, S.; Steplewski, K.; et al. A randomised, double-blind, placebo-controlled trial of trametinib, an oral MEK inhibitor, in combination with gemcitabine for patients with untreated metastatic adenocarcinoma of the pancreas. Eur. J. Cancer 2014, 50, 2072–2081. [Google Scholar] [CrossRef] [PubMed]
- BVD-523 Plus Nab-Paclitaxel and Gemcitabine in Patients with Metastatic Pancreatic Cancer (NCT02608229). Available online: https://clinicaltrials.gov/ct2/show/NCT02608229?term=BVD-523&rank=3 (accessed on 5 September 2015).
- Falasca, M.; Selvaggi, F.; Buus, R.; Sulpizio, S.; Edling, C.E. Targeting phosphoinositide 3-kinase pathways in pancreatic cancer--from molecular signalling to clinical trials. Anticancer Agents Med. Chem. 2011, 11, 455–463. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, B.H.; Scott, A.J.; Ma, W.W.; Cohen, S.J.; Aisner, D.L.; Menter, A.R.; Tejani, M.A.; Cho, J.K.; Granfortuna, J.; Coveler, L.; et al. A phase II/III randomized study to compare the efficacy and safety of rigosertib plus gemcitabine versus gemcitabine alone in patients with previously untreated metastatic pancreatic cancer†. Ann. Oncol. 2015, 26, 1923–1929. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.; Marincola, P.; Öberg, K. Everolimus in the treatment of patients with advanced pancreatic neuroendocrine tumors: Latest findings and interpretations. Ther. Adv. Gastroenterol. 2013, 6, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Wiedmann, M.W.; Mössner, J. Safety and efficacy of sunitinib in patients with unresectable pancreatic neuroendocrine tumors. Clin. Med. Insights Oncol. 2012, 6, 381–393. [Google Scholar] [CrossRef] [PubMed]
- Kordes, S.; Klümpen, H.J.; Weterman, M.J.; Schellens, J.H.M.; Richel, D.J.; Wilmink, J.W. Phase II study of capecitabine and the oral mTOR inhibitor everolimus in patients with advanced pancreatic cancer. Cancer Chemother. Pharmacol. 2015, 75, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Wolpin, B.M.; Hezel, A.F.; Abrams, T.; Blaszkowsky, L.S.; Meyerhardt, J.A.; Chan, J.A.; Enzinger, P.C.; Allen, B.; Clark, J.W.; Ryan, D.P.; et al. Oral mTOR inhibitor everolimus in patients with gemcitabine-refractory metastatic pancreatic cancer. J. Clin. Oncol. 2009, 27, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Javle, M.M.; Shroff, R.T.; Xiong, H.; Varadhachary, G.A.; Fogelman, D.; Reddy, S.A.; Davis, D.; Zhang, Y.; Wolff, R.A.; Abbruzzese, J.L. Inhibition of the mammalian target of rapamycin (mTOR) in advanced pancreatic cancer: Results of two phase II studies. BMC Cancer 2010, 10, 368. [Google Scholar] [CrossRef] [PubMed]
- Jokinen, E.; Koivunen, J.P. MEK and PI3K inhibition in solid tumors: Rationale and evidence to date. Ther. Adv. Med. Oncol. 2015, 7, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Ioka, T.; Okusaka, T.; Ohkawa, S.; Boku, N.; Sawaki, A.; Fujii, Y.; Kamei, Y.; Takahashi, S.; Namazu, K.; Umeyama, Y.; et al. Efficacy and safety of axitinib in combination with gemcitabine in advanced pancreatic cancer: Subgroup analyses by region, including Japan, from the global randomized phase III trial. Jpn. J. Clin. Oncol. 2015, 45, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Kindler, H.L.; Ioka, T.; Richel, D.J.; Bennouna, J.; Letourneau, R.; Okusaka, T.; Funakoshi, A.; Furuse, J.; Park, Y.S.; Ohkawa, S.; et al. Axitinib plus gemcitabine versus placebo plus gemcitabine in patients with advanced pancreatic adenocarcinoma: A double-blind randomised phase 3 study. Lancet Oncol. 2011, 12, 256–262. [Google Scholar] [CrossRef]
- Kindler, H.L.; Friberg, G.; Singh, D.A.; Locker, G.; Nattam, S.; Kozloff, M.; Taber, D.A.; Karrison, T.; Dachman, A.; Stadler, W.M.; et al. Phase II trial of bevacizumab plus gemcitabine in patients with advanced pancreatic cancer. J. Clin. Oncol. 2005, 23, 8033–8040. [Google Scholar] [CrossRef] [PubMed]
- Pfizer Pfizer Discontinues Global Phase III Trial of Axitinib for Futility in Advanced Pancreatic Cancer. Available online: http://press.pfizer.com/press-release/pfizer-discontinues-global-phase-iii-trial-axitinib-futility-advanced-pancreatic-cance (accessed on 15 May 2017).
- Kindler, H.L.; Wroblewski, K.; Wallace, J.A.; Hall, M.J.; Locker, G.; Nattam, S.; Agamah, E.; Stadler, W.M.; Vokes, E.E. Gemcitabine plus sorafenib in patients with advanced pancreatic cancer: A phase II trial of the University of Chicago Phase II Consortium. Investig. New Drug 2012, 30, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Rougier, P.; Riess, H.; Manges, R.; Karasek, P.; Humblet, Y.; Barone, C.; Santoro, A.; Assadourian, S.; Hatteville, L.; Philip, P.A. Randomised, placebo-controlled, double-blind, parallel-group phase III study evaluating aflibercept in patients receiving first-line treatment with gemcitabine for metastatic pancreatic cancer. Eur. J. Cancer 2013, 49, 2633–2642. [Google Scholar] [CrossRef] [PubMed]
- Momenta Pharmaceuticals Inc. M402 in Combination with Nab-Paclitaxel and Gemcitabine in Pancreatic Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT01621243 (accessed on 15 May 2017).
- Lili, L.N.; Matyunina, L.V.; Walker, L.D.; Daneker, G.W.; McDonald, J.F. Evidence for the importance of personalized molecular profiling in pancreatic cancer. Pancreas 2014, 43, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, H.I.; Uppal, N.; Wagner, S.A.; Bendell, J.C.; Beck, J.T.; Wade, S.M., III; Nemunaitis, J.J.; Stella, P.J.; Pipas, J.M.; Wainberg, Z.A.; et al. Randomized, double-blind, phase II study of ruxolitinib or placebo in combination with capecitabine in patients with metastatic pancreatic cancer for whom therapy with gemcitabine has failed. J. Clin. Oncol. 2015, 33, 4039–4047. [Google Scholar] [PubMed]
- O’Reilly, E.M.; Walker, C.; Clark, J.; Brill, K.J.; Dawkins, F.W.; Bendell, J.C.; David, M. JANUS 2: A phase III study of survival, tumor response, and symptom response with ruxolitinib plus capecitabine or placebo plus capecitabine in patients with advanced or metastatic pancreatic cancer (mPC) who failed or were intolerant to first-line chemotherapy. J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Wang, Z.; Li, Y.; Kong, D.; Banerjee, S.; Ahmad, A.; Azmi, A.S.; Ali, S.; Abbruzzese, J.L.; Gallick, G.E.; Sarkar, F.H. Acquisition of epithelial-mesenchymal transition phenotype of gemcitabine-resistant pancreatic cancer cells is linked with activation of the Notch signaling pathway. Cancer Res. 2009, 69, 2400. [Google Scholar] [CrossRef] [PubMed]
- Mullendore, M.E.; Koorstra, J.-B.; Li, Y.-M.; Offerhaus, G.J.; Fan, X.; Henderson, C.M.; Matsui, W.; Eberhart, C.G.; Maitra, A.; Feldmann, G. Ligand-dependent Notch signaling is involved in tumor initiation and tumor maintenance in pancreatic cancer. Clin. Cancer Res. 2009, 15, 2291. [Google Scholar] [CrossRef] [PubMed]
- Yen, W.-C.; Fischer, M.M.; Hynes, M.; Wu, J.; Kim, E.; Beviglia, L.; Yeung, V.P.; Song, X.; Kapoun, A.M.; Lewicki, J.; et al. Anti-DLL4 has broad spectrum activity in pancreatic cancer dependent on targeting DLL4-Notch signaling in both tumor and vasculature cells. Clin. Cancer Res. 2012, 18, 5374–5386. [Google Scholar] [CrossRef] [PubMed]
- Pharma, O. Demcizumab in Combination with Abraxane (Paclitaxel Protein-Bound Particles for Injectable Suspension) (Albumin Bound) + Gemcitabine Fails Phase II Trial for Metastatic Pancreatic Cancer. Available online: https://www.epgonline.org/global/news/demcizumab--in-combination-with-abraxane--paclitaxel-protein-bound-particles-for-injectable-suspension---albumin-bound----gemcitabine-fails-phase-ii-trial-for-metastatic-pancreatic-cancer---oncomed-pharma.html (accessed on 15 May 2017).
- MK0752 and Gemcitabine Hydrochloride in Treating Patients with Stage III and IV Pancreatic Cancer That Cannot Be Removed by Surgery. Available online: https://clinicaltrials.gov/show/NCT01098344 (accessed on 3 September 2016).
- De Jesus-Acosta, A.; Laheru, D.; Maitra, A.; Arcaroli, J.; Rudek, M.A.; Dasari, A.; Blatchford, P.J.; Quackenbush, K.; Messersmith, W. A phase II study of the gamma secretase inhibitor RO4929097 in patients with previously treated metastatic pancreatic adenocarcinoma. Investig. New Drug 2014, 32, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.-W.; Andrabi, S.A.; Wang, H.; Kim, N.S.; Poirier, G.G.; Dawson, T.M.; Dawson, V.L. Apoptosis-inducing factor mediates poly(ADP-ribose) (PAR) polymer-induced cell death. Proc. Natl. Acad. Sci. USA 2006, 103, 18314–18319. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, B.; Shapira-Frommer, R.; Schmutzler, R.K.; Audeh, M.W.; Friedlander, M.; Balmaña, J.; Mitchell, G.; Fried, G.; Stemmer, S.M.; Hubert, A.; et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J. Clin. Oncol. 2015, 33, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Two Phase II Studies of Veliparib for Pancreatic Cancer with a BRCA or PALB2 Mutation: Gemcitabine & Cisplatin with/without Veliparib in Untreated Pancreatic Cancer (Part I) & Veliparib Alone for Patients with Previously Treated Pancreatic Cancer. Available online: https://www.mskcc.org/cancer-care/clinical-trials/12-045 (accessed on 16 May 2017).
- National Cancer Institute (NCI). Gemcitabine Hydrochloride and Cisplatin with or without Veliparib or Veliparib alone in Treating Patients with Locally Advanced or Metastatic Pancreatic Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT01585805 (accessed on 16 May 2017).
- Mendel, D.B.; Laird, A.D.; Xin, X.; Louie, S.G.; Christensen, J.G.; Li, G.; Schreck, R.E.; Abrams, T.J.; Ngai, T.J.; Lee, L.B.; et al. In vivo antitumor activity of SU11248, a novel tyrosine kinase inhibitor targeting vascular endothelial growth factor and platelet-derived growth factor receptors. Clin. Cancer Res. 2003, 9, 327–337. [Google Scholar] [PubMed]
- Bergers, G.; Song, S.; Meyer-Morse, N.; Bergsland, E.; Hanahan, D. Benefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J. Clin. Investig. 2003, 111, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Pasca di Magliano, M.; Hebrok, M. Hedgehog signaling pathways in pancreatic cancer pathogenesis. In Pancreatic Cancer; Springer: New York, NY, USA, 2010; pp. 403–418. [Google Scholar]
- Bailey, J.M.; Swanson, B.J.; Hamada, T.; Eggers, J.P.; Singh, P.K.; Caffery, T.; Ouellette, M.M.; Hollingsworth, M.A. Sonic Hedgehog promotes desmoplasia in pancreatic cancer. Clin. Cancer Res. 2008, 14, 5995–6004. [Google Scholar] [CrossRef] [PubMed]
- Feldmann, G.; Dhara, S.; Fendrich, V.; Bedja, D.; Beaty, R.; Mullendore, M.; Karikari, C.; Alvarez, H.; Iacobuzio-Donahue, C.; Jimeno, A.; et al. Blockade of Hedgehog signaling inhibits pancreatic cancer invasion and metastases: A new paradigm for combination therapy in solid cancers. Cancer Res. 2007, 67, 2187. [Google Scholar] [CrossRef] [PubMed]
- Olive, K.P.; Jacobetz, M.A.; Davidson, C.J.; Gopinathan, A.; McIntyre, D.; Honess, D.; Madhu, B.; Goldgraben, M.A.; Caldwell, M.E.; Allard, D.; et al. Inhibition of hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science 2009, 324, 1457–1461. [Google Scholar] [CrossRef] [PubMed]
- Olive, K. Clinical Trial: IPI-926–03 for Metastatic Pancreatic Ductal Adenocarcinoma Patients Who Have Not Been Treated with Other Chemotherapy. Available online: http://www.olivelab.org/ipi-926–03.html (accessed on 18 March 2017).
- Catenacci, D.V.T.; Junttila, M.R.; Karrison, T.; Bahary, N.; Horiba, M.N.; Nattam, S.R.; Marsh, R.; Wallace, J.; Kozloff, M.; Rajdev, L.; et al. Randomized phase Ib/II study of gemcitabine plus placebo or vismodegib, a Hedgehog pathway inhibitor, in patients with metastatic pancreatic cancer. J. Clin. Oncol. 2015, 33, 4284–4292. [Google Scholar] [CrossRef] [PubMed]
- Bax, L. Hedgehog Inhibition for Pancreatic Ductal Adenocarcinoma (PDAC) in the Preoperative Setting (HIPPoS) (HIPPoS). Available online: https://clinicaltrials.gov/ct2/show/NCT01096732 (accessed on 15 May 2017).
- Gao, R.; Brigstock, D.R. A novel integrin α5β1 binding domain in module 4 of connective tissue growth factor (CCN2/CTGF) promotes adhesion and migration of activated pancreatic stellate cells. Gut 2006, 55, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Ijichi, H.; Chytil, A.; Gorska, A.E.; Aakre, M.E.; Bierie, B.; Tada, M.; Mohri, D.; Miyabayashi, K.; Asaoka, Y.; Maeda, S.; et al. Inhibiting Cxcr2 disrupts tumor-stromal interactions and improves survival in a mouse model of pancreatic ductal adenocarcinoma. J. Clin. Investig. 2011, 121, 4106–4117. [Google Scholar] [CrossRef] [PubMed]
- Neesse, A.; Frese, K.K.; Bapiro, T.E.; Nakagawa, T.; Sternlicht, M.D.; Seeley, T.W.; Pilarsky, C.; Jodrell, D.I.; Spong, S.M.; Tuveson, D.A. CTGF antagonism with mAb FG-3019 enhances chemotherapy response without increasing drug delivery in murine ductal pancreas cancer. Proc. Natl. Acad. Sci. USA 2013, 110, 12325–12330. [Google Scholar] [CrossRef] [PubMed]
- Apte, M.V.; Park, S.; Phillips, P.A.; Santucci, N.; Goldstein, D.; Kumar, R.K.; Ramm, G.A.; Buchler, M.; Friess, H.; McCarroll, J.A.; et al. Desmoplastic reaction in pancreatic cancer: Role of pancreatic stellate cells. Pancreas 2004, 29, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.; Masamune, A.; Takikawa, T.; Suzuki, N.; Kikuta, K.; Hirota, M.; Hamada, H.; Kobune, M.; Satoh, K.; Shimosegawa, T. Pancreatic stellate cells enhance stem cell-like phenotypes in pancreatic cancer cells. Biochem. Biophys. Res. Commun. 2012, 421, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Erkan, M.; Kleeff, J.; Gorbachevski, A.; Reiser, C.; Mitkus, T.; Esposito, I.; Giese, T.; Büchler, M.W.; Giese, N.A.; Friess, H. Periostin creates a tumor-supportive microenvironment in the pancreas by sustaining fibrogenic stellate cell activity. Gastroenterology 2007, 132, 1447–1464. [Google Scholar] [CrossRef] [PubMed]
- Nakai, Y.; Isayama, H.; Ijichi, H.; Sasaki, T.; Sasahira, N.; Hirano, K.; Kogure, H.; Kawakubo, K.; Yagioka, H.; Yashima, Y.; et al. Inhibition of renin-angiotensin system affects prognosis of advanced pancreatic cancer receiving gemcitabine. Br. J. Cancer 2010, 103, 1644–1648. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, V.P.; Martin, J.D.; Liu, H.; Lacorre, D.A.; Jain, S.R.; Kozin, S.V.; Stylianopoulos, T.; Mousa, A.S.; Han, X.; Adstamongkonkul, P.; et al. Angiotensin inhibition enhances drug delivery and potentiates chemotherapy by decompressing tumour blood vessels. Nat. Commun. 2013, 4, 2516. [Google Scholar] [CrossRef] [PubMed]
- Bramhall, S.R.; Schulz, J.; Nemunaitis, J.; Brown, P.D.; Baillet, M.; Buckels, J.A.C. A double-blind placebo-controlled, randomised study comparing gemcitabine and marimastat with gemcitabine and placebo as first line therapy in patients with advanced pancreatic cancer. Br. J. Cancer 2002, 87, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, S.R.; Harris, W.P.; Beck, J.T.; Berdov, B.A.; Wagner, S.A.; Pshevlotsky, E.M.; Tjulandin, S.A.; Gladkov, O.A.; Holcombe, R.F.; Korn, R.; et al. Phase Ib study of PEGylated recombinant human hyaluronidase and gemcitabine in patients with advanced pancreatic cancer. Clin. Cancer Res. 2016, 22, 2848–2854. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, S.R.; Harris, W.P.; Hendifar, A.E.; Bullock, A.J.; Wu, X.W.; Huang, Y.; Jiang, P. High response rate and PFS with PEGPH20 added to nab-paclitaxel/gemcitabine in stage IV previously untreated pancreatic cancer patients with high-HA tumors: Interim results of a randomized phase II study. J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Falasca, M.; Kim, M.; Casari, I. Pancreatic cancer: Current research and future directions. Biochim. Biophys. Acta 2016, 1865, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Ko, A.H.; Tempero, M.A.; Bekail-Saab, T.B.; Kuhn, P.; Courtin, R.; Ziyeh, S.; Tahiri, S.; Kelley, R.K.; Dito, E.; Ong, A.; et al. Dual MEK/EGFR inhibition for advanced, chemotherapy-refractory pancreatic cancer: A multicenter phase II trial of selumetinib (AZD6244; ARRY-142886) plus erlotinib. J. Clin. Oncol. 2013, 31. [Google Scholar] [CrossRef]
- Gonçalves, A.; Gilabert, M.; François, E.; Dahan, L.; Perrier, H.; Lamy, R.; Re, D.; Largillier, R.; Gasmi, M.; Tchiknavorian, X.; et al. BAYPAN study: A double-blind phase III randomized trial comparing gemcitabine plus sorafenib and gemcitabine plus placebo in patients with advanced pancreatic cancer. Ann. Oncol. 2012, 23, 2799–2805. [Google Scholar] [CrossRef] [PubMed]
- Cutsem, E.V.; Vervenne, W.L.; Bennouna, J.; Humblet, Y.; Gill, S.; Laethem, J.-L.V.; Verslype, C.; Scheithauer, W.; Shang, A.; Cosaert, J.; et al. Phase III trial of bevacizumab in combination with gemcitabine and erlotinib in patients with metastatic pancreatic cancer. J. Clin. Oncol. 2009, 27, 2231–2237. [Google Scholar] [CrossRef] [PubMed]
- Nakai, Y.; Isayama, H.; Ijichi, H.; Sasaki, T.; Takahara, N.; Ito, Y.; Matsubara, S.; Uchino, R.; Yagioka, H.; Arizumi, T.; et al. A multicenter phase II trial of gemcitabine and candesartan combination therapy in patients with advanced pancreatic cancer: GECA2. Investig. New Drugs 2013, 31, 1294–1299. [Google Scholar] [CrossRef] [PubMed]
- Inc., I.P. A Study Evaluating IPI-926 in Combination with Gemcitabine in Patients with Metastatic Pancreatic Cancer. Available online: https://clinicaltrials.gov/ct2/show/record/NCT01130142 (accessed on 17 March 2017).
- A Randomized, Double-Blind, Phase 3 Study of the Jak 1/2 Inhibitor, Ruxolitinib or Placebo in Combination with Capecitabine in Subjects with Advanced or Metastatic Adenocarcinoma of the Pancreas Who Have Failed or Are Intolerant to First-Line Chemotherapy (The JANUS 1 Study). Available online: https://experts.umich.edu/en/projects/a-randomized-double-blind-phase-3-study-of-the-jak-12-inhibitor-r-2 (accessed on 20 May 2017).
- Le, D.T.; Lutz, E.; Uram, J.N.; Sugar, E.A.; Onners, B.; Solt, S.; Zheng, L.; Diaz, L.A., Jr.; Donehower, R.C.; Jaffee, E.M.; et al. Evaluation of ipilimumab in combination with allogeneic pancreatic tumor cells transfected with a GM-CSF gene in previously treated pancreatic cancer. J. Immunother. 2013, 36, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Middleton, G.; Silcocks, P.; Cox, T.; Valle, J.; Wadsley, J.; Propper, D.; Coxon, F.; Ross, P.; Madhusudan, S.; Roques, T.; et al. Gemcitabine and capecitabine with or without telomerase peptide vaccine GV1001 in patients with locally advanced or metastatic pancreatic cancer (TeloVac): An open-label, randomised, phase 3 trial. Lancet Oncol. 2014, 15, 829–840. [Google Scholar] [CrossRef]
- Zhang, Y.; Velez-Delgado, A.; Mathew, E.; Li, D.; Mendez, F.M.; Flannagan, K.; Rhim, A.D.; Simeone, D.M.; Beatty, G.L.; di Magliano, M.P. Myeloid cells are required for PD-1/PD-L1 checkpoint activation and the establishment of an immunosuppressive environment in pancreatic cancer. Gut 2017, 66, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti–PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [PubMed]
- Kalyan, A.; Kircher, S.M.; Mohindra, N.A.; Nimeiri, H.S.; Maurer, V.; Rademaker, A.; Benson, A.B.; Mulcahy, M.F. Ipilimumab and gemcitabine for advanced pancreas cancer: A phase Ib study. J. Clin. Oncol. 2016, 34. [Google Scholar] [CrossRef]
- Loskog, A.S.I.; Eliopoulos, A.G. The Janus faces of CD40 in cancer. Semin. Immunol. 2009, 21, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Vonderheide, R.H.; Bajor, D.L.; Winograd, R.; Evans, R.A.; Bayne, L.J.; Beatty, G.L. CD40 immunotherapy for pancreatic cancer. Cancer Immunol. Immunother. 2013, 62, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Beatty, G.L.; Chiorean, E.G.; Fishman, M.P.; Saboury, B.; Teitelbaum, U.R.; Sun, W.; Huhn, R.D.; Song, W.; Li, D.; Sharp, L.L.; et al. CD40 agonists alter tumor stroma and show efficacy against pancreatic carcinoma in mice and humans. Science 2011, 331, 1612–1616. [Google Scholar] [CrossRef] [PubMed]
- Bahary, N.; Garrido-Laguna, I.; Cinar, P.; O’Rourke, M.A.; Somer, B.G.; Nyak-Kapoor, A.; Lee, J.S.; Munn, D.; Kennedy, E.P.; Vahanian, N.N.; et al. Phase 2 trial of the indoleamine 2,3-dioxygenase pathway (IDO) inhibitor indoximod plus gemcitabine/nab-paclitaxel for the treatment of metastatic pancreas cancer: Interim analysis. J. Clin. Oncol. 2016, 34. [Google Scholar] [CrossRef]
- Bernhardt, S.L.; Gjertsen, M.K.; Trachsel, S.; Moller, M.; Eriksen, J.A.; Meo, M.; Buanes, T.; Gaudernack, G. Telomerase peptide vaccination of patients with non-resectable pancreatic cancer: A dose escalating phase I/II study. Br. J. Cancer 2006, 95, 1474–1482. [Google Scholar] [CrossRef] [PubMed]
- Gunturu, K.S.; Rossi, G.R.; Saif, M.W. Immunotherapy updates in pancreatic cancer: Are we there yet? Ther. Adv. Med. Oncol. 2013, 5, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Huang, J.; Yang, N.; Greshock, J.; Liang, S.; Hasegawa, K.; Giannakakis, A.; Poulos, N.; O’Brien-Jenkins, A.; Katsaros, D.; et al. Integrative genomic analysis of phosphatidylinositol 3′-kinase family identifies PIK3R3 as a potential therapeutic target in epithelial ovarian cancer. Clin. Cancer Res. 2007, 13 Pt 1, 5314–5321. [Google Scholar] [CrossRef] [PubMed]
- Lewis, B.P.; Burge, C.B.; Bartel, D.P. Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell 2005, 120, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, M.; Wang, H.; Fisher, W.E.; Lin, P.H.; Yao, Q.; Chen, C. Profiling of 95 microRNAs in pancreatic cancer cell lines and surgical specimens by real-time PCR analysis. World J. Surg. 2008, 33, 698. [Google Scholar] [CrossRef] [PubMed]
- Hong, T.H.; Park, I.Y. MicroRNA expression profiling of diagnostic needle aspirates from surgical pancreatic cancer specimens. Ann. Surg. Treat. Res. 2014, 87, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Schultz, N.A.; Werner, J.; Willenbrock, H.; Roslind, A.; Giese, N.; Horn, T.; Wojdemann, M.; Johansen, J.S. MicroRNA expression profiles associated with pancreatic adenocarcinoma and ampullary adenocarcinoma. Mod. Pathol. 2012, 25, 1609–1622. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Sarkar, F.H. MicroRNA targeted therapeutic approach for pancreatic cancer. Int. J. Biol. Sci. 2016, 12, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Papaconstantinou, I.G.; Manta, A.; Gazouli, M.; Lyberopoulou, A.; Lykoudis, P.M.; Polymeneas, G.; Voros, D. Expression of microRNAs in patients with pancreatic cancer and its prognostic significance. Pancreas 2013, 42, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Jiao, L.R.; Frampton, A.E.; Jacob, J.; Pellegrino, L.; Krell, J.; Giamas, G.; Tsim, N.; Vlavianos, P.; Cohen, P.; Ahmad, R.; et al. MicroRNAs targeting oncogenes are down-regulated in pancreatic malignant transformation from benign tumors. PLoS ONE 2012, 7, e32068. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, N.B.; Morran, D.C.; Morton, J.P.; Ali, A.; Dickson, E.J.; Carter, C.R.; Sansom, O.J.; Evans, T.R.J.; McKay, C.J.; Oien, K.A. MicroRNA molecular profiles associated with diagnosis, clinicopathologic criteria, and overall survival in patients with resectable pancreatic ductal adenocarcinoma. Clin. Cancer Res. 2012, 18, 534–545. [Google Scholar] [CrossRef] [PubMed]
- Ryu, J.K.; Hong, S.M.; Karikari, C.A.; Hruban, R.H.; Goggins, M.G.; Maitra, A. Aberrant microRNA-155 expression is an early event in the multistep progression of pancreatic adenocarcinoma. Pancreatology 2010, 10, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Greither, T.; Grochola, L.F.; Udelnow, A.; Lautenschläger, C.; Würl, P.; Taubert, H. Elevated expression of microRNAs 155, 203, 210 and 222 in pancreatic tumors is associated with poorer survival. Int. J. Cancer 2010, 126, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.-J.; Zhao, Y.-P.; Zhang, T.-P.; Zhou, L.; Cui, Q.-C.; Zhou, W.-X.; You, L.; Chen, G.; Shu, H. MLH1 as a direct target of miR-155 and a potential predictor of favorable prognosis in pancreatic cancer. J. Gastrointest. Surg. 2013, 17, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Li, H.; Wu, W.; Jiang, T.; Qiu, Z. Regulation of miR-155 affects pancreatic cancer cell invasiveness and migration by modulating the STAT3 signaling pathway through SOCS1. Oncol. Rep. 2013, 30, 1223–1230. [Google Scholar] [PubMed]
- Ali, S.; Banerjee, S.; Logna, F.; Bao, B.; Philip, P.A.; Korc, M.; Sarkar, F.H. Inactivation of Ink4a/Arf leads to deregulated expression of miRNAs in K-Ras transgenic mouse model of pancreatic cancer. J. Cell. Physiol. 2012, 227, 3373–3380. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Komatsu, S.; Ichikawa, D.; Morimura, R.; Tsujiura, M.; Konishi, H.; Takeshita, H.; Nagata, H.; Arita, T.; Hirajima, S.; et al. Clinical impact of circulating miR-221 in plasma of patients with pancreatic cancer. Br. J. Cancer 2013, 108, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Farrell, J.J.; Toste, P.; Wu, N.; Li, L.; Wong, J.; Malkhassian, D.; Tran, L.M.; Wu, X.; Li, X.; Dawson, D.; et al. Endoscopically acquired pancreatic cyst fluid microRNA 21 and 221 are associated with invasive cancer. Am. J. Gastroenterol. 2013, 108, 1352–1359. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Dubaybo, H.; Ali, S.; Goncalves, P.; Kollepara, S.L.; Sethi, S.; Philip, P.A.; Li, Y. Down-regulation of miR-221 inhibits proliferation of pancreatic cancer cells through up-regulation of PTEN, p27(kip1), p57(kip2), and PUMA. Am. J. Cancer Res. 2013, 3, 465–477. [Google Scholar] [PubMed]
- Masamune, A.; Nakano, E.; Hamada, S.; Takikawa, T.; Yoshida, N.; Shimosegawa, T. Alteration of the microRNA expression profile during the activation of pancreatic stellate cells. Scand. J. Gastroenterol. 2014, 49, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; VandenBoom, T.G.; Wang, Z.; Kong, D.; Ali, S.; Philip, P.A.; Sarkar, F.H. miR-146a suppresses invasion of pancreatic cancer cells. Cancer Res. 2010, 70, 1486–1495. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Li, A.; Hong, S.-M.; Hruban, R.H.; Goggins, M. MicroRNA alterations of pancreatic intraepithelial neoplasias. Clin. Cancer Res. 2012, 18, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Cheng, H.; Shi, S.; Cui, X.; Yang, J.; Chen, L.; Cen, P.; Cai, X.; Lu, Y.; Wu, C.; et al. MicroRNA-34b inhibits pancreatic cancer metastasis through repressing Smad3. Curr. Mol. Med. 2013, 13, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Ji, Q.; Hao, X.; Zhang, M.; Tang, W.; Yang, M.; Li, L.; Xiang, D.; DeSano, J.T.; Bommer, G.T.; Fan, D.; et al. MicroRNA miR-34 inhibits human pancreatic cancer tumor-initiating cells. PLoS ONE 2009, 4, e6816. [Google Scholar] [CrossRef] [PubMed]
- Nalls, D.; Tang, S.-N.; Rodova, M.; Srivastava, R.K.; Shankar, S. Targeting epigenetic regulation of miR-34a for treatment of pancreatic cancer by inhibition of pancreatic cancer stem cells. PLoS ONE 2011, 6, e24099. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Duan, Q.; Ahmad, A.; Bao, B.; Banerjee, S.; Shi, Y.; Ma, J.; Geng, J.; Chen, Z.; Wahidur Rahman, K.M.; et al. Genistein inhibits cell growth and induces apoptosis through up-regulation of miR-34a in pancreatic cancer cells. Curr. Drug Targets 2012, 13, 1750–1756. [Google Scholar] [CrossRef] [PubMed]
- Dillhoff, M.; Liu, J.; Frankel, W.; Croce, C.; Bloomston, M. MicroRNA-21 is overexpressed in pancreatic cancer and a potential predictor of survival. J. Gastrointest. Surg. 2008, 12, 2171. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Wang, Z.-X.; Wang, R. MicroRNA-21: A novel therapeutic target in human cancer. Cancer Biol. Ther. 2010, 10, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Sicard, F.; Gayral, M.; Lulka, H.; Buscail, L.; Cordelier, P. Targeting miR-21 for the therapy of pancreatic cancer. Mol. Ther. 2013, 21, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, T.; Ohuchida, K.; Mizumoto, K.; Yu, J.; Sato, N.; Nabae, T.; Takahata, S.; Toma, H.; Nagai, E.; Tanaka, M. MicroRNA-21 modulates biological functions of pancreatic cancer cells including their proliferation, invasion, and chemoresistance. Mol. Cancer Ther. 2009, 8, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, E.; Funel, N.; Peters, G.J.; del Chiaro, M.; Erozenci, L.A.; Vasile, E.; Leon, L.G.; Pollina, L.E.; Groen, A.; Falcone, A.; et al. MicroRNA-21 in pancreatic cancer: Correlation with clinical outcome and pharmacologic aspects underlying its role in the modulation of gemcitabine activity. Cancer Res. 2010, 70, 4528–4538. [Google Scholar] [CrossRef] [PubMed]
- Kadera, B.E.; Li, L.; Toste, P.A.; Wu, N.; Adams, C.; Dawson, D.W.; Donahue, T.R. MicroRNA-21 in pancreatic ductal adenocarcinoma tumor-associated fibroblasts promotes metastasis. PLoS ONE 2013, 8, e71978. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.L.; Jiang, Q.Y.; Jin, X.; Shen, J.; Wang, K.; Li, Y.B.; Xu, F.J.; Tang, G.P.; Li, Z.H. Cationic microRNA-delivering nanovectors with bifunctional peptides for efficient treatment of PANC-1 xenograft model. Biomaterials 2013, 34, 2265–2276. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Swaminathan, S.K.; Kirtane, A.; Srivastava, S.K.; Bhardwaj, A.; Singh, S.; Panyam, J.; Singh, A.P. Synthesis, characterization, and evaluation of poly (d,l-lactide-Co-glycolide)-based nanoformulation of miRNA-150: Potential implications for pancreatic cancer therapy. Int. J. Nanomed. 2014, 9, 2933–2942. [Google Scholar]
- Zhao, Y.; Zhao, L.; Ischenko, I.; Bao, Q.; Schwarz, B.; Nieß, H.; Wang, Y.; Renner, A.; Mysliwietz, J.; Jauch, K.-W.; et al. Antisense inhibition of microRNA-21 and microRNA-221 in tumor-initiating stem-like cells modulates tumorigenesis, metastasis, and chemotherapy resistance in pancreatic cancer. Target Oncol. 2015, 10, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Mittal, A.; Chitkara, D.; Behrman, S.W.; Mahato, R.I. Efficacy of gemcitabine conjugated and miRNA-205 complexed micelles for treatment of advanced pancreatic cancer. Biomaterials 2014, 35, 7077–7087. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Go, V.L.W.; Sarkar, F.H. The role of nutraceuticals in pancreatic cancer prevention and therapy: Targeting cellular signaling, miRNAs and epigenome. Pancreas 2015, 44, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Cheng, L.; Mei, C.; Ma, J.; Shi, Y.; Zeng, F.; Wang, Z.; Wang, Z. Genistein inhibits cell growth and invasion through regulation of miR-27a in pancreatic cancer cells. Curr. Pharm. Des. 2014, 20, 5348–5353. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; VandenBoom, T.G.; Kong, D.; Wang, Z.; Ali, S.; Philip, P.A.; Sarkar, F.H. Up-regulation of miR-200 and let-7 by natural agents leads to the reversal of epithelial-to-mesenchymal transition in gemcitabine-resistant pancreatic cancer cells. Cancer Res. 2009, 69, 6704–6712. [Google Scholar] [CrossRef] [PubMed]
- Bao, B.; Ali, S.; Banerjee, S.; Wang, Z.; Logna, F.; Azmi, A.S.; Kong, D.; Ahmad, A.; Li, Y.; Padhye, S.; et al. Curcumin analogue CDF inhibits pancreatic tumor growth by switching on suppressor microRNAs and attenuating EZH2 expression. Cancer Res. 2012, 72, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Chen, M.; Greening, D.W.; He, W.; Rai, A.; Zhang, W.; Simpson, R.J. Deep sequencing of rna from three different extracellular vesicle (ev) subtypes released from the human lim1863 colon cancer cell line uncovers distinct mirna-enrichment signatures. PLoS ONE 2014, 9, e110314. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Liang, H.; Xia, Q.; Li, P.; Kong, H.; Lei, P.; Wang, S.; Tu, Z. Resveratrol induces apoptosis of pancreatic cancers cells by inhibiting miR-21 regulation of BCL-2 expression. Clin. Transl. Oncol. 2013, 15, 741–746. [Google Scholar] [CrossRef] [PubMed]
- González-Vallinas, M.; Molina, S.; Vicente, G.; Zarza, V.; Martín-Hernández, R.; García-Risco, M.R.; Fornari, T.; Reglero, G.; de Molina, A.R. Expression of microRNA-15b and the glycosyltransferase GCNT3 correlates with antitumor efficacy of rosemary diterpenes in colon and pancreatic cancer. PLoS ONE 2014, 9, e98556. [Google Scholar] [CrossRef] [PubMed]
- Pelzer, U.; Schwaner, I.; Stieler, J.; Adler, M.; Seraphin, J.; Dorken, B.; Riess, H.; Oettle, H. Best supportive care (BSC) versus oxaliplatin, folinic acid and 5-fluorouracil (OFF) plus BSC in patients for second-line advanced pancreatic cancer: A phase III-study from the German CONKO-study group. Eur. J. Cancer 2011, 47, 1676–1681. [Google Scholar] [CrossRef] [PubMed]
- Oettle, H.; Riess, H.; Stieler, J.M.; Heil, G.; Schwaner, I.; Seraphin, J.; Gorner, M.; Molle, M.; Greten, T.F.; Lakner, V.; et al. Second-line oxaliplatin, folinic acid, and fluorouracil versus folinic acid and fluorouracil alone for gemcitabine-refractory pancreatic cancer: Outcomes from the CONKO-003 trial. J. Clin. Oncol. 2014, 32, 2423–2429. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.; Ko, Y.-J.; Cripps, C.; Beaudoin, A.; Dhesy-Thind, S.; Zulfiqar, M.; Zalewski, P.; Do, T.; Cano, P.; Lam, W.Y.H.; et al. PANCREOX: A randomized phase III study of fluorouracil/leucovorin with or without oxaliplatin for second-line advanced pancreatic cancer in patients who have received gemcitabine-based chemotherapy. J. Clin. Oncol. 2016, 34, 3914–3920. [Google Scholar] [CrossRef] [PubMed]
- Ettrich, T.J.; Perkhofer, L.; von Wichert, G.; Gress, T.M.; Michl, P.; Hebart, H.F.; Büchner-Steudel, P.; Geissler, M.; Muche, R.; Danner, B.; et al. DocOx (AIO-PK0106): A phase II trial of docetaxel and oxaliplatin as a second line systemic therapy in patients with advanced pancreatic ductal adenocarcinoma. BMC Cancer 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Bayoglu, I.V.; Varol, U.; Yildiz, I.; Muslu, U.; Alacacioglu, A.; Kucukzeybek, Y.; Akyol, M.; Demir, L.; Dirican, A.; Cokmert, S.; et al. Second-line capecitabine and oxaliplatin combination for gemcitabine-resistant advanced pancreatic cancer. Asian Pac. J. Cancer Prev. 2014, 15, 7119–7123. [Google Scholar] [CrossRef] [PubMed]
- Zaanan, A.; Trouilloud, I.; Markoutsaki, T.; Gauthier, M.; Dupont-Gossart, A.C.; Lecomte, T.; Aparicio, T.; Artru, P.; Thirot-Bidault, A.; Joubert, F.; et al. FOLFOX as second-line chemotherapy in patients with pretreated metastatic pancreatic cancer from the FIRGEM study. BMC Cancer 2014, 14, 441. [Google Scholar] [CrossRef] [PubMed]
- Zaniboni, A.; Aitini, E.; Barni, S.; Ferrari, D.; Cascinu, S.; Catalano, V.; Valmadre, G.; Ferrara, D.; Veltri, E.; Codignola, C.; et al. FOLFIRI as second-line chemotherapy for advanced pancreatic cancer: A GISCAD multicenter phase II study. Cancer Chemother. Pharmacol. 2012, 69, 1641–1645. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, C.; Hentic, O.; Rousseau, B.; Rebours, V.; Bengrine-Lefèvre, L.; Bonnetain, F.; Lévy, P.; Raymond, E.; Ruszniewski, P.; Louvet, C.; et al. FOLFIRI regimen in metastatic pancreatic adenocarcinoma resistant to gemcitabine and platinum-salts. World J. Gastroenterol. 2012, 18, 4533–4541. [Google Scholar] [CrossRef] [PubMed]
- Da Rocha Lino, A.; Abrahao, C.M.; Brandao, R.M.; Gomes, J.R.; Ferrian, A.M.; Machado, M.C.; Buzaid, A.C.; Maluf, F.C.; Peixoto, R.D. Role of gemcitabine as second-line therapy after progression on FOLFIRINOX in advanced pancreatic cancer: A retrospective analysis. J. Gastrointest. Oncol. 2015, 6, 511–515. [Google Scholar] [PubMed]
- Zhang, Y.; Hochster, H.; Stein, S.; Lacy, J. Gemcitabine plus nab-paclitaxel for advanced pancreatic cancer after first-line FOLFIRINOX: Single institution retrospective review of efficacy and toxicity. Exp. Hematol. Oncol. 2015, 4, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kulke, M.H.; Blaszkowsky, L.S.; Ryan, D.P.; Clark, J.W.; Meyerhardt, J.A.; Zhu, A.X. Capecitabine plus erlotinib in gemcitabine-refractory advanced pancreatic cancer. J. Clin. Oncol. 2007, 25, 4787–4792. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.; Li, C.P.; Wang-Gillam, A.; Bodoky, G.; Dean, A.; Jameson, G.; Macarulla, T.; Lee, K.H.; Cunningham, D.; Blanc, J.F.; et al. O-0003NAPOLI-1: Randomized phase 3 study of MM-398 (Nal-Iri), with or without 5-Fluorouracil and leucovorin, versus 5-Fluorouracil and Leucovorin, in metastatic pancreatic cancer progressed on or following Gemcitabine-based therapy. Ann. Oncol. 2014, 25 (Suppl. S2), ii105–ii106. [Google Scholar] [CrossRef]
- Van Houten, J.P.; White, R.R.; Jackson, G.P. A decision model of therapy for potentially resectable pancreatic cancer. J. Surg. Res. 2012, 174, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Karanikas, M.; Esempidis, A.; Chasan, Z.T.M.; Deftereou, T.; Antonopoulou, M.; Bozali, F.; Amarantidis, K.; Man, Y.G. Pancreatic cancer from molecular pathways to treatment opinion. J. Cancer 2016, 7, 1328–1339. [Google Scholar] [CrossRef] [PubMed]
- Chantrill, L.A.; Nagrial, A.M.; Watson, C.; Johns, A.L.; Martyn-Smith, M.; Simpson, S.; Mead, S.; Jones, M.D.; Samra, J.S.; Gill, A.J.; et al. Precision medicine for advanced pancreas cancer: The Individualized Molecular Pancreatic Cancer Therapy (IMPaCT) trial. Clin. Cancer Res. 2015, 21, 2029–2037. [Google Scholar] [CrossRef] [PubMed]
- Thota, R.; Maitra, A.; Berlin, J.D. Preclinical rationale for the phase III trials in metastatic pancreatic cancer: Is wishful thinking clouding successful drug development for pancreatic cancer? Pancreas 2017, 46, 143–150. [Google Scholar] [CrossRef] [PubMed]



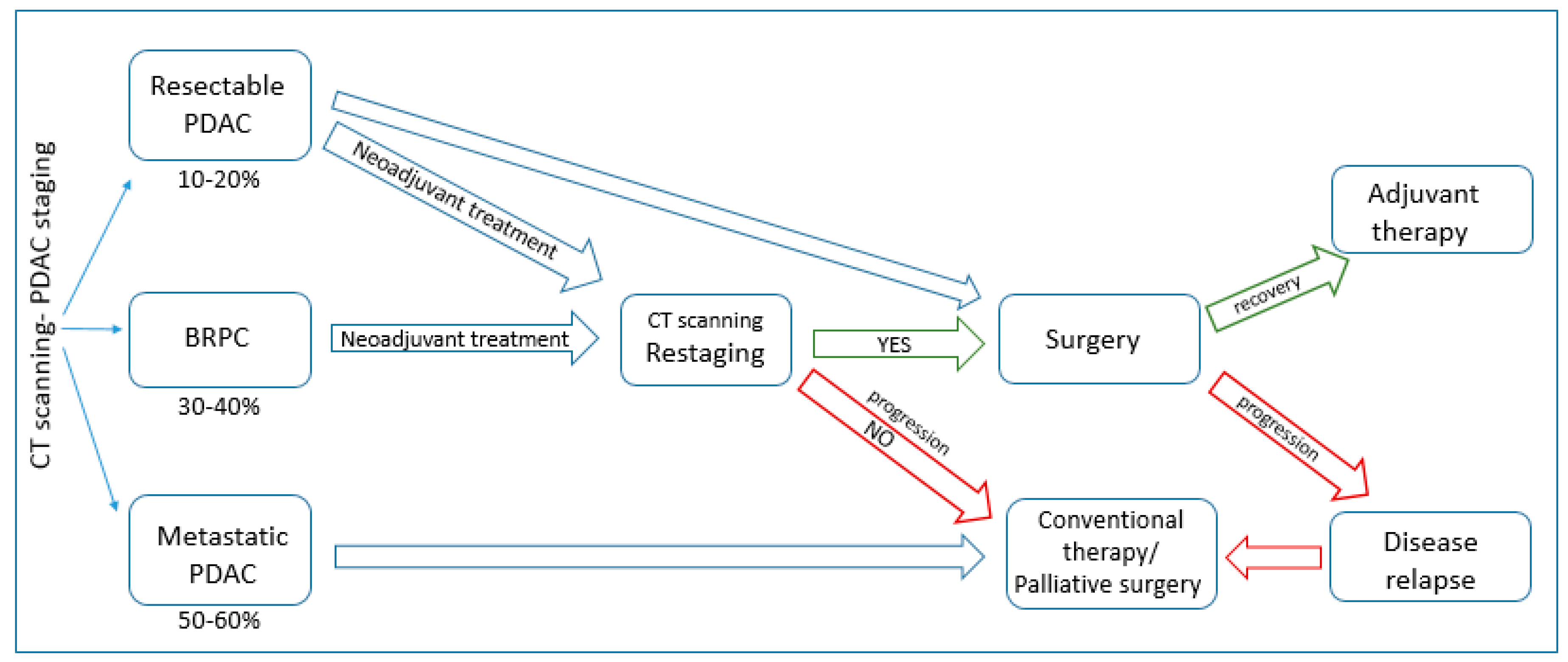{kind=link}
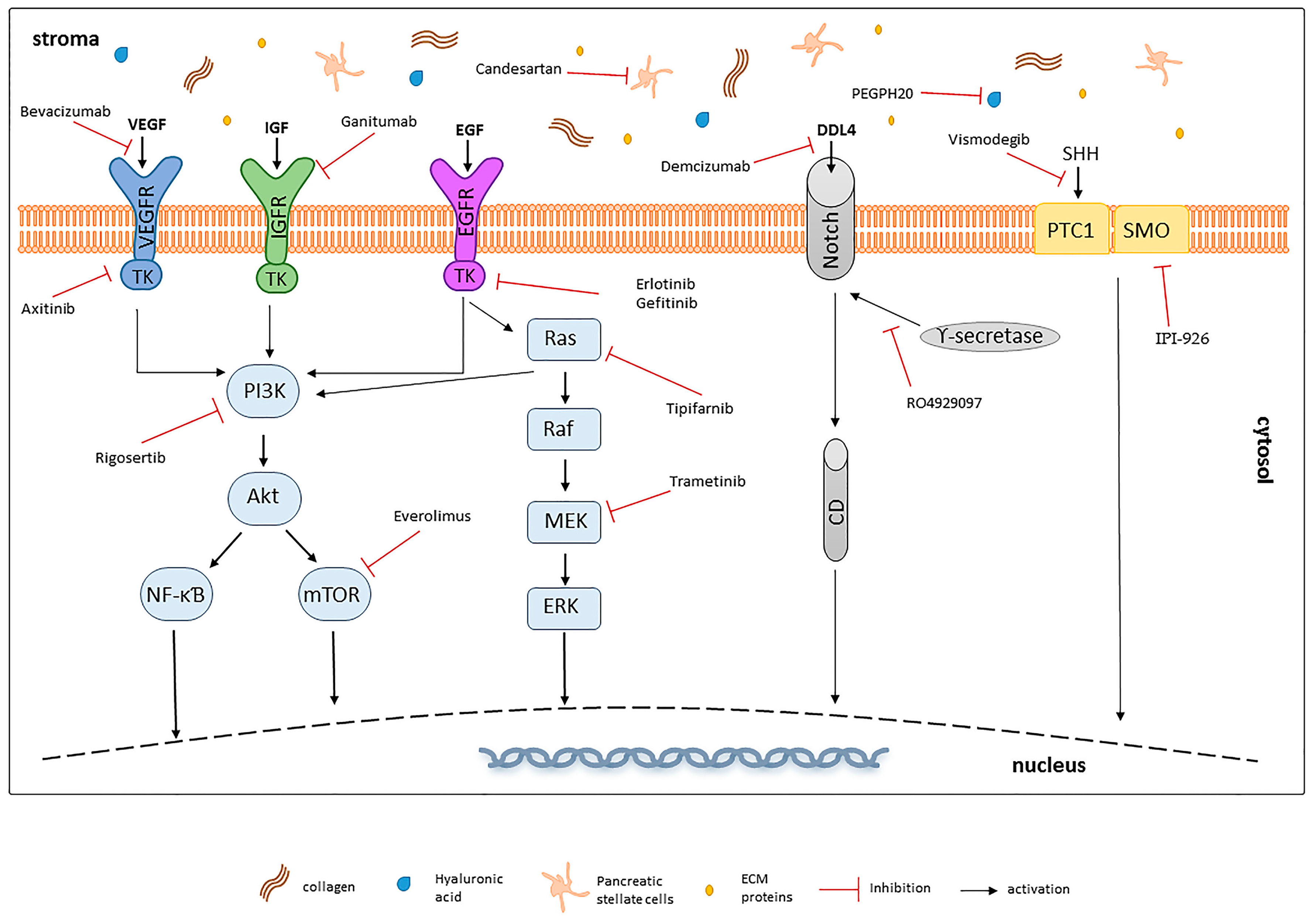{kind=link}
| Treatment | Phase | n | OS (Months)/Response Rate (%) | Outcome | p | Reference |
|---|---|---|---|---|---|---|
| Gem vs. 5-FU | R FL III | 126 | 5.65 vs. 4.4 | FDA approved | 0.0025 | [22] |
| Gem-5FU vs. gem | FL III | 322 | 6.7 vs. 5.6 | No statistically significant improvement in OS | 0.09 | [65] |
| FOLFIRINOX | R II/III | 342 | 11.1 vs. 6.8 | FDA approved | <0.001 | [60] |
| Abraxane | R III | 861 | 8.5 vs. 6.7 | FDA approved | <0.001 | [49] |
| Erlotinib + gem/gem | R III | 569 | 6.2 vs. 5.9 | FDA approved | 0.038 | [42] |
| Gem + cisplatin/gem | R III | 195 | 7.5 vs. 6.0 | Improved survival, but not statistically significant | 0.15 | [33] |
| R III | 400 | 7.2 vs. 8.3 | Failed to demonstrate improvement | 0.38 | [32] | |
| PEFG vs. gem | III | 99 | 38.5% vs. 8.5% | Little sample size | 0.0008 | [37] |
| Gem + oxaliplatin | III | 313 | 9.0 vs. 7.1 | Significant improvement in response rate and PFS, but not statistically significant OS | 0.13 | [30] |
| Gem + capecitabine vs. gem | III | 319 | 8.4 vs. 7.2 | Not statistically significant improvement in OS | 0.234 | [44] |
| III | 533 | 7.1 vs. 6.2 | Alternative treatment for patients with good PS | 0.08 | [34] | |
| S-1 + gem/gem | III | 834 | 9.7 vs. 8.8 | Not inferior to gemcitabine. Approved in Japan as alternative | <0.001 | [39] |
| Gem + irinotecan | III | 360 | 6.3 vs. 6.6 | Good tumour response but no improvement in OS | 0.789 | [29] |
| Drug Target | Treatment | Phase | n | OS | Comment | p | Reference |
|---|---|---|---|---|---|---|---|
| KRas pathway inhibitors | |||||||
| KRAS (farnesyl transferase) | Tipifarnib + gem vs. gem | R III | 688 | 193 vs. 182 (days) | Acceptable toxicity profile, but no statistically significant differences in survival parameters | 0.75 | [163] |
| MAPK | Selumetinib + erlotinib 2nd line | SA II | 46 | 7.5 | Modest antitumor activity. Specific molecular subtypes may provide greatest benefit | – | [216] |
| MAPK | Trametinib + gem vs. gem | R II | 160 | 8.4 vs. 6.7 | No statistical difference in OS, PFS and response rate was observed | 0.453 | [165] |
| MAPK | Selumetinib + cape vs. cape 2nd line | R II | 70 | 5.4 vs. 5.0 | No improvement in OS | 0.92 | [164] |
| MAPK | Sorafenib + gem vs. gem | 104 | 9.2 vs. 8.0 | No statistical significance was achieved in all parameters studied | 0.231 | [217] | |
| mTOR | Everolimus + erlotinib | SA II | 16 | 2.9 | Disease progression observed in 15 patients. Study stopped due to impossibility to reach preplanned OS of 6 months | – | [173] |
| PI3K | Rigosertib + gem vs. gem | R II/III | 160 | 6.1 vs. 6.4 | Study was discontinued due to no significant difference in survival | NR | [168] |
| Growth factor receptors inhibitors | |||||||
| EGFR | Erlotinib + gem vs. gem | R III | 569 | 6.2 vs. 5.9 | FDA approved | 0.038 | [42] |
| EGFR | Cetixumab + gem vs. gem | 743 | 6.3 vs. 5.9 | Combination arm did not achieve significance in improvement of OS | 0.19 | [152] | |
| EGFR/IGFR | Cixutumumab + erlotinib + gem vs. erlotinib + gem | R Ib/II | 116 | 7.0 vs. 6.7 | Dual inhibition of EGFR and IGFR did not improve OS or PFS | 0.64 | [161] |
| EGFR | Gefitinib + gem | SA II | 53 | 7.3 | Promising results, especially in patients with PTEN expression. | – | [153] |
| HER-2 | Trastuzumab + cape | SA II | 17 | 6.9 | No improvement in mOS or PFS; low number of patients and HER2 expression | NR | [155] |
| TK | Dasatinib | SA II | 51 | 4.7 | No activity of single agent dosatinib in metastatic PDAC, no improvement in OS and PFS | – | [216] |
| TK | Lapatinib + gem | SA II | 29 | 4 | No improvement in survival, small case sample | – | [156] |
| IGFR | Ganitumab + gem vs. gem | R III | 800 | 7.0 vs. 7.2 | No improvement in all assessed parameters | 0.494 | [162] |
| Angiogenesis inhibitors | |||||||
| VEGFR | Axitinib + gem vs. gem | R III | 632 | 8.5 vs. 8.3 | No significant survival benefit compared to single agent gem | 0.544 | [176] |
| VEGF-A | Bevacizumab + gem + erlotinib vs. gem + erlotinib | R III | 301 | 7.1 vs. 6.0 | Despite improvement in PFS could be observed (p = 0.0002), no statistically significant difference in OS was achieved | 0.209 | [218] |
| VEGF | Aflibercept + gem vs. gem | R III | 587 | 6.5 vs. 7.8 | Discontinued due to no improvement in primary end point, OS | 0.159 | [180] |
| Inhibition of tumour stroma | |||||||
| Matrix metalloproteinase | Matrimastat + gem vs. gem | R III | 239 | 5.4 vs. 5.4 | No significant differences in all assessed parameters | 0.95 | [212] |
| SHH | Vismodegib + gem vs. gem | R Ib/II | 106 | 6.9 vs. 6.1 | No difference in PFS, OS or response rate was noted | 0.84 | [202] |
| PSCs | Candesartan + gem | SA II | 35 | 9.1 | Treatment was well tolerated but failed to show significant activity | – | [219] |
| Hedgehog (Smoothened) | IPI-926 + gem vs. gem | R Ib/II | 122 | – | Decrease in survival in IPI-926 arm caused closure of study | NR | [220] |
| Hyaluronic acid | PEGPH20 + gem | Ib | 28 | 6.6 | Well tolerated, may be beneficial, especially for patients with high HA levels (13 months OS) | – | [213] |
| PEGPH20/Abraxane vs. Abraxane | R II | 237 | Ongoing | [214] | |||
| R III | 420 | Ongoing | |||||
| Other targets | |||||||
| JAK/STAT | Ruxolitinib + cape vs. cape | R II | 127 | 4.5 vs. 4.2 | Well tolerated, slight, but significant improvement in OS and PS | 0.011 | [183] |
| 2nd line therapy | R III | 270 | Phase III on larger population is ongoing | [184,221] | |||
| γ-secretase | RO4929097 2nd line | SA II | 18 | 4.1 | Study was discontinued as the primary endpoint-survival rate at 6 months—was not promising (27.8%) | – | [190] |
| Immunotherapy | |||||||
| CTLA-4 | Ipilimumab + GVAX vaccine vs. ipilimumab | R Ib/II | 30 | 5.7 vs. 3.6 | Despite the enhancement of the T cell repertoire (p = 0.031), no significant increase in OS or PFS was noted | 0.51 | [222] |
| Telomerase vaccination | GV1001 + gem + cape/gem + cape | R III | 1062 | 8.4 vs. 6.9 | No significant improvement in OS has been achieved | 0.11 | [223] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamska, A.; Domenichini, A.; Falasca, M. Pancreatic Ductal Adenocarcinoma: Current and Evolving Therapies. Int. J. Mol. Sci. 2017, 18, 1338. https://doi.org/10.3390/ijms18071338
Adamska A, Domenichini A, Falasca M. Pancreatic Ductal Adenocarcinoma: Current and Evolving Therapies. International Journal of Molecular Sciences. 2017; 18(7):1338. https://doi.org/10.3390/ijms18071338
Chicago/Turabian StyleAdamska, Aleksandra, Alice Domenichini, and Marco Falasca. 2017. "Pancreatic Ductal Adenocarcinoma: Current and Evolving Therapies" International Journal of Molecular Sciences 18, no. 7: 1338. https://doi.org/10.3390/ijms18071338