Regulation of Inflammatory Response in Human Osteoarthritic Chondrocytes by Novel Herbal Small Molecules

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Results
2.1. Toxicity Assay for the Compounds on Human Osteoarthritic Chondrocytes
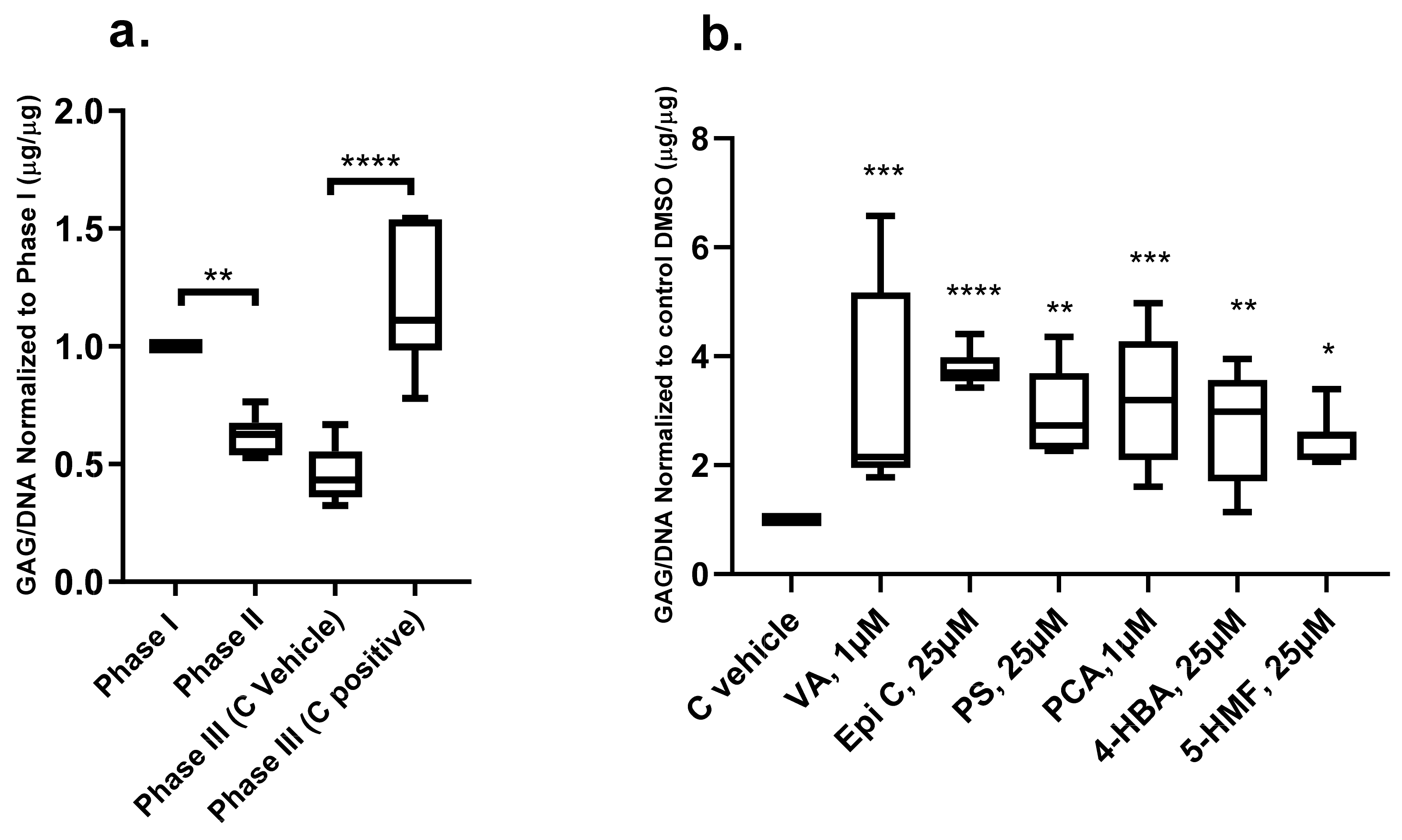
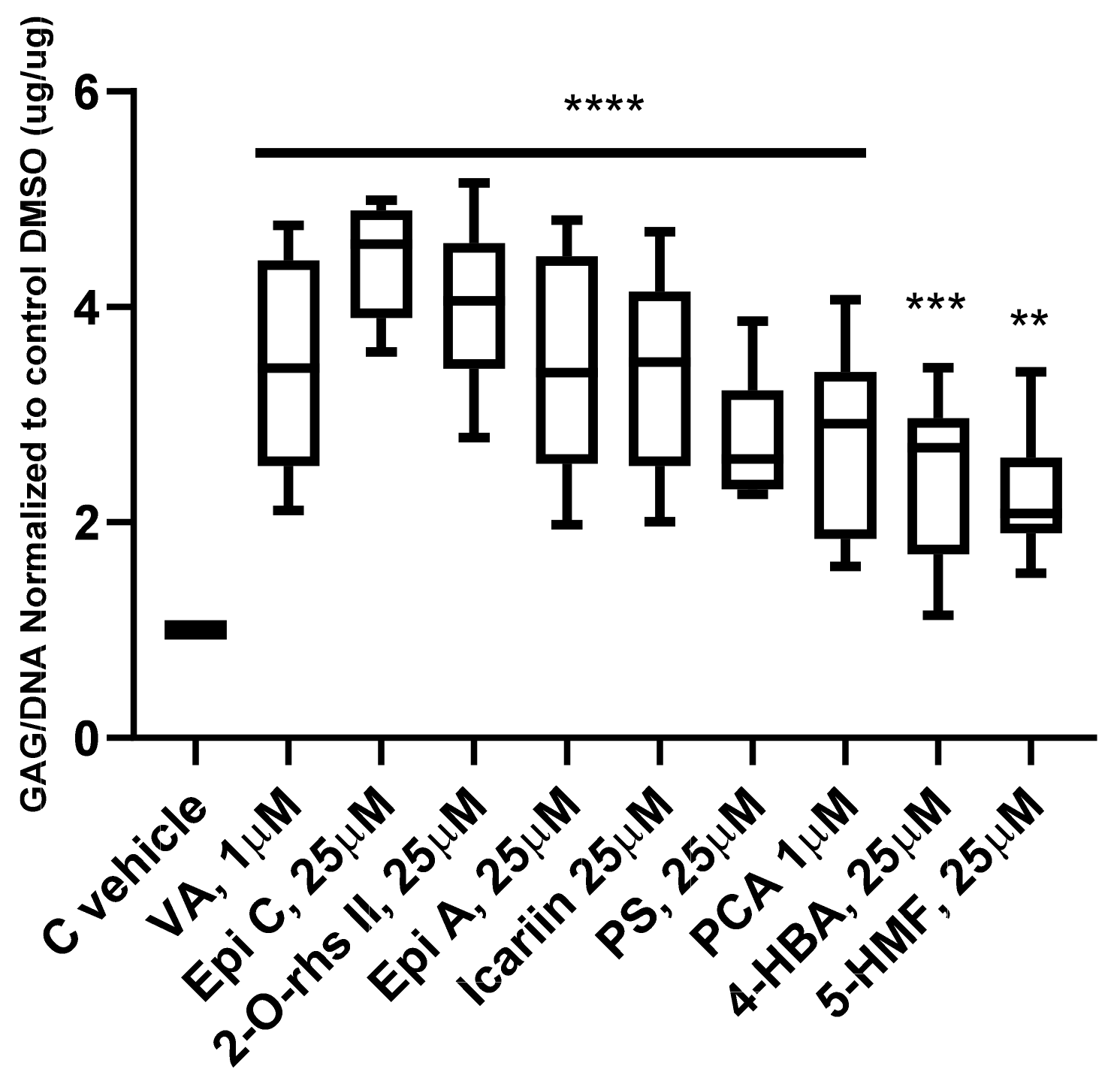
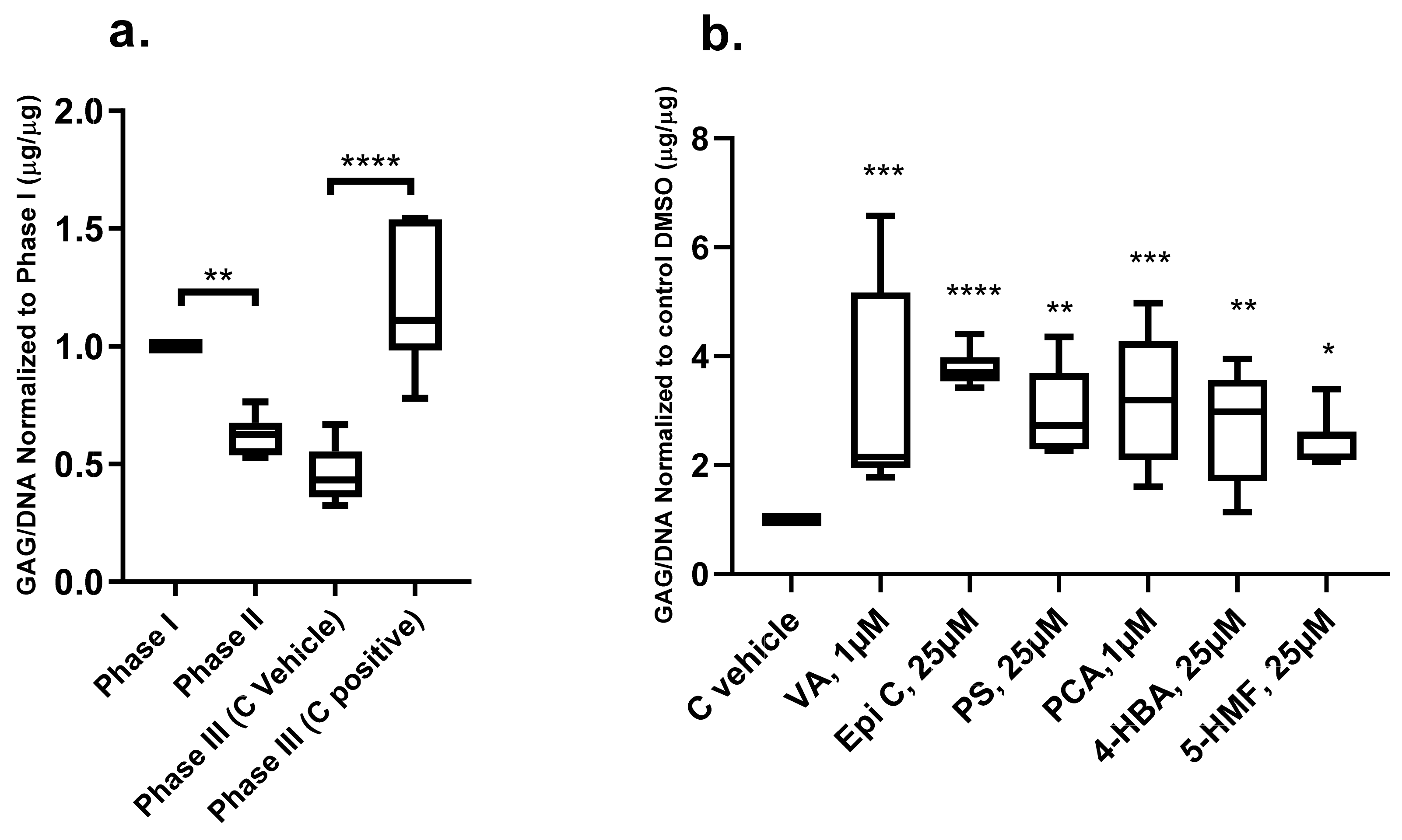
2.2. Anabolic Effects of Traditional Chinese Medicine (TCM) Compounds on Glycosaminoglycan Production
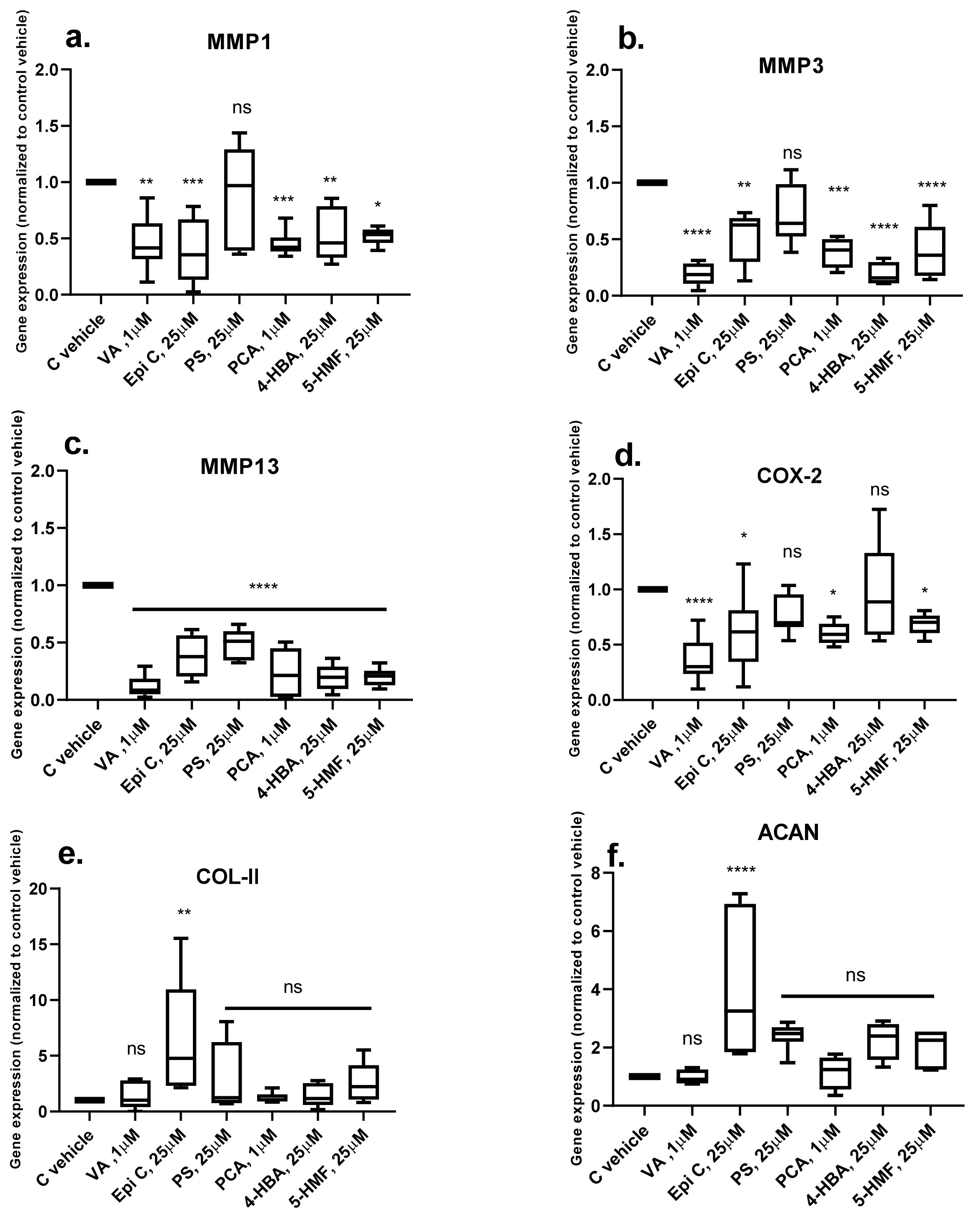
2.3. Effects of TCM Compounds on Pro-Inflammatory and Pro-Catabolic Gene Expression under Inflammatory Conditions
2.4. Effect of TCM Compounds on Matrix Production under Inflammatory Conditions
3. Discussion
4. Materials and Methods
4.1. Drugs Screening on Human Osteoarthritic Chondrocytes
4.2. Isolation of Human Osteoarthritic Chondrocytes and Cell Expansion
4.3. Cell Toxicity Assay
4.4. Anabolic Effects of the TCM Compounds on Osteoarthritic Chondrocytes Pellet Cultures
4.5. Anti-Catabolic Effects of the TCM Compounds on Osteoarthritic Chondrocytes Pellet Cultures
4.6. Biochemical Analysis
4.7. Gene Expression Analysis
4.8. Histological and Immunohistochemical Analysis
4.9. Statistical Analysis
Ethic Approval and Consent to Participate
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lawrence, R.C.; Felson, D.T.; Helmick, C.G.; Arnold, L.M.; Choi, H.; Deyo, R.A.; Gabriel, S.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008, 58, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Wallace, I.J.; Worthington, S.; Felson, D.T.; Jurmain, R.D.; Wren, K.T.; Maijanen, H.; Woods, R.J.; Lieberman, D.E. Knee osteoarthritis has doubled in prevalence since the mid-20th century. Proc. Natl. Acad. Sci. USA 2017, 114, 9332. [Google Scholar] [CrossRef] [PubMed]
- Mobasheri, A. The future of osteoarthritis therapeutics: Emerging biological therapy. Curr. Rheumatol. Rep. 2013, 15, 385. [Google Scholar] [CrossRef] [PubMed]
- Shane Anderson, A.; Loeser, R.F. Why is osteoarthritis an age-related disease? Best Pract. Res. Clin. Rheumatol. 2010, 24, 15–26. [Google Scholar] [CrossRef]
- Carames, B.; Taniguchi, N.; Otsuki, S.; Blanco, F.J.; Lotz, M. Autophagy is a protective mechanism in normal cartilage, and its aging-related loss is linked with cell death and osteoarthritis. Arthritis Rheum. 2010, 62, 791–801. [Google Scholar] [CrossRef]
- Loeser, R.F. Age-related changes in the musculoskeletal system and the development of osteoarthritis. Clin. Geriatr. Med. 2010, 26, 371–386. [Google Scholar] [CrossRef]
- Krishnan, Y.; Grodzinsky, A.J. Cartilage diseases. Matrix Biol. J. Int. Soc. Matrix Biol. 2018, 51–69. [Google Scholar] [CrossRef]
- Clockaerts, S.; Bastiaansen-Jenniskens, Y.M.; Runhaar, J.; Van Osch, G.J.; Van Offel, J.F.; Verhaar, J.A.; De Clerck, L.S.; Somville, J. The infrapatellar fat pad should be considered as an active osteoarthritic joint tissue: A narrative review. Osteoarthr. Cartil. Osteoarthr. Res. Soc. 2010, 18, 876–882. [Google Scholar] [CrossRef]
- Williams, A.; Kamper, S.J.; Wiggers, J.H.; O’Brien, K.M.; Lee, H.; Wolfenden, L.; Yoong, S.L.; Robson, E.; McAuley, J.H.; Hartvigsen, J.; et al. Musculoskeletal conditions may increase the risk of chronic disease: A systematic review and meta-analysis of cohort studies. BMC Med. 2018, 16, 167. [Google Scholar] [CrossRef]
- Tellegen, A.R.; Rudnik-Jansen, I.; Pouran, B.; de Visser, H.M.; Weinans, H.H.; Thomas, R.E.; Kik, M.J.L.; Grinwis, G.C.M.; Thies, J.C.; Woike, N.; et al. Controlled release of celecoxib inhibits inflammation, bone cysts and osteophyte formation in a preclinical model of osteoarthritis. Drug Deliv. 2018, 25, 1438–1447. [Google Scholar] [CrossRef]
- Cokelaere, S.M.; Plomp, S.G.M.; de Boef, E.; de Leeuw, M.; Bool, S.; van de Lest, C.H.A.; van Weeren, P.R.; Korthagen, N.M. Sustained intra-articular release of celecoxib in an equine repeated LPS synovitis model. Eur. J. Pharm. Biopharm. 2018, 128, 327–336. [Google Scholar] [CrossRef] [PubMed]
- van den Driest, J.J.; Pijnenburg, P.; Bindels, P.J.E.; Bierma-Zeinstra, S.M.A.; Schiphof, D. Analgesic Use in Dutch Patients with Osteoarthritis: Frequent but Low Doses. J. Clin. Rheumatol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.H.; Husni, M.E.; Libby, P.A.; Yeomans, N.D.; Lincoff, A.M.; Lupsilonscher, T.F.; Menon, V.; Brennan, D.M.; Wisniewski, L.M.; Nissen, S.E.; et al. The Risk of Major NSAID Toxicity with Celecoxib, Ibuprofen, or Naproxen: A Secondary Analysis of the PRECISION Trial. Am. J. Med. 2017, 130, 1415–1422.e1414. [Google Scholar] [CrossRef] [PubMed]
- Pincus, T.; Koch, G.; Lei, H.; Mangal, B.; Sokka, T.; Moskowitz, R.; Wolfe, F.; Gibofsky, A.; Simon, L.; Zlotnick, S.; et al. Patient Preference for Placebo, Acetaminophen (paracetamol) or Celecoxib Efficacy Studies (PACES): Two randomised, double blind, placebo controlled, crossover clinical trials in patients with knee or hip osteoarthritis. Ann. Rheum. Dis. 2004, 63, 931–939. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, R.W.; Abramson, S.B.; Berenbaum, F.; Simon, L.S.; Hochberg, M. Coxibs and NSAIDs--is the air any clearer? Perspectives from the OARSI/International COX-2 Study Group Workshop 2007. Osteoarthr. Cartil. OARS Osteoarthr. Res. Soc. 2007, 15, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Marcu, K.B.; Otero, M.; Olivotto, E.; Borzi, R.M.; Goldring, M.B. NF-kappaB signaling: Multiple angles to target OA. Curr. Drug Targets 2010, 11, 599–613. [Google Scholar] [CrossRef] [PubMed]
- Urech, D.M.; Feige, U.; Ewert, S.; Schlosser, V.; Ottiger, M.; Polzer, K.; Schett, G.; Lichtlen, P. Anti-inflammatory and cartilage-protecting effects of an intra-articularly injected anti-TNFa single-chain Fv antibody (ESBA105) designed for local therapeutic use. Ann. Rheum. Dis. 2010, 69, 443–449. [Google Scholar] [CrossRef]
- Goldring, M.B.; Otero, M. Inflammation in osteoarthritis. Curr. Opin. Rheumatol. 2011, 23, 471–478. [Google Scholar] [CrossRef]
- Rovati, L.C.; Girolami, F.; Persiani, S. Crystalline glucosamine sulfate in the management of knee osteoarthritis: Efficacy, safety, and pharmacokinetic properties. Ther. Adv. Musculoskelet. Dis. 2012, 4, 167–180. [Google Scholar] [CrossRef]
- Jevsevar, D.; Donnelly, P.; Brown, G.A.; Cummins, D.S. Viscosupplementation for Osteoarthritis of the Knee: A Systematic Review of the Evidence. J. Bone Jt. Surg. Am. Vol. 2015, 97, 2047–2060. [Google Scholar] [CrossRef]
- Clough, T.M.; Alvi, F.; Majeed, H. Total ankle arthroplasty: What are the risks? Bone Jt. J. 2018, 1352–1358. [Google Scholar] [CrossRef] [PubMed]
- Ronn, K.; Reischl, N.; Gautier, E.; Jacobi, M. Current surgical treatment of knee osteoarthritis. Arthritis 2011, 2011, 454873. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Moskowitz, R.W.; Nuki, G.; Abramson, S.; Altman, R.D.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthr. Cartil. OARS Osteoarthr. Res. Soc. 2008, 16, 137–162. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Ma, X.H.; Qin, C.; Tao, L.; Liu, X.; Shi, Z.; Zhang, C.L.; Tan, C.Y.; Chen, Y.Z.; Jiang, Y.Y. Drug discovery prospect from untapped species: Indications from approved natural product drugs. PLoS ONE 2012, 7, e39782. [Google Scholar] [CrossRef]
- Newman, D.J.; Cragg, G.M.; Snader, K.M. Natural products as sources of new drugs over the period 1981-2002. J. Nat. Prod. 2003, 66, 1022–1037. [Google Scholar] [CrossRef]
- Toegel, S.; Wu, S.Q.; Otero, M.; Goldring, M.B.; Leelapornpisid, P.; Chiari, C.; Kolb, A.; Unger, F.M.; Windhager, R.; Viernstein, H. Caesalpinia sappan extract inhibits IL1beta-mediated overexpression of matrix metalloproteinases in human chondrocytes. Genes Nutr. 2012, 7, 307–318. [Google Scholar] [CrossRef]
- Moussaieff, A.; Shohami, E.; Kashman, Y.; Fride, E.; Schmitz, M.L.; Renner, F.; Fiebich, B.L.; Munoz, E.; Ben-Neriah, Y.; Mechoulam, R. Incensole acetate, a novel anti-inflammatory compound isolated from Boswellia resin, inhibits nuclear factor-kappa B activation. Mol. Pharmacol. 2007, 72, 1657–1664. [Google Scholar] [CrossRef]
- Kim, J.H.; Kismali, G.; Gupta, S.C. Natural products for the prevention and treatment of chronic inflammatory diseases: Integrating traditional medicine into modern chronic diseases care. Evid. Based Complementary Altern. Med. eCAM 2018, 2018, 9837863. [Google Scholar] [CrossRef]
- Mobasheri, A.; Henrotin, Y.; Biesalski, H.K.; Shakibaei, M. Scientific evidence and rationale for the development of curcumin and resveratrol as nutraceutricals for joint health. Int. J. Mol. Sci. 2012, 13, 4202–4232. [Google Scholar] [CrossRef]
- Chen, Y.J.; Tsai, K.S.; Chan, D.C.; Lan, K.C.; Chen, C.F.; Yang, R.S.; Liu, S.H. Honokiol, a low molecular weight natural product, prevents inflammatory response and cartilage matrix degradation in human osteoarthritis chondrocytes. J. Orthop. Res.: Off. Publ. Orthop. Res. Soc. 2014, 32, 573–580. [Google Scholar] [CrossRef]
- Gui, L.; Shen, H. Application of Xianlinggubao in bone and arthrosis disease. Chin. J. New Drugs Clin. Rem. 2007, 26, 619–622. [Google Scholar]
- Zhu, H.M.; Qin, L.; Garnero, P.; Genant, H.K.; Zhang, G.; Dai, K.; Yao, X.; Gu, G.; Hao, Y.; Li, Z.; et al. The first multicenter and randomized clinical trial of herbal Fufang for treatment of postmenopausal osteoporosis. Osteoporos. Int. J. Establ. Result Coop. Eur. Found. Osteoporos. National Osteoporos. Found. USA 2012, 23, 1317–1327. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.R.; Cheng, L.M.; Wang, K.Z.; Yang, N.P.; Yang, S.H.; He, W.; Wang, Y.S.; Wang, Z.M.; Yang, P.; Liu, X.Z.; et al. Herbal Fufang Xian Ling Gu Bao prevents corticosteroid-induced osteonecrosis of the femoral head-A first multicentre, randomised, double-blind, placebo-controlled clinical trial. J. Orthop. Transl. 2018, 12, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Shi, L.; Zhang, Y.; Wang, K.; Pei, F.; Zhu, H.; Shi, Z.; Tao, T.; Li, Z.; Zeng, P.; et al. A traditional herbal formula xianlinggubao for pain control and function improvement in patients with knee and hand oSteoarthritis: A multicenter, randomized, open-label, controlled trial. Evid. Based Complementary Altern. Med. eCAM 2018, 2018, 1827528. [Google Scholar] [CrossRef]
- Dai, Y.; Tu, F.J.; Yao, Z.H.; Ding, B.; Xu, W.; Qiu, X.H.; Yao, X.S. Rapid identification of chemical constituents in traditional Chinese medicine fufang preparation xianling gubao capsule by LC-linear ion trap/Orbitrap mass spectrometry. Am. J. Chin. Med. 2013, 41, 1181–1198. [Google Scholar] [CrossRef]
- Li, D.; Yuan, T.; Zhang, X.; Xiao, Y.; Wang, R.; Fan, Y.; Zhang, X. Icariin: A potential promoting compound for cartilage tissue engineering. Osteoarthr. Cartil. OARS Osteoarthr. Res. Soc. 2012, 20, 1647–1656. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Li, Q.; Mei, Q.; Lu, T. Pharmacological effects and pharmacokinetic properties of icariin, the major bioactive component in Herba Epimedii. Life Sci. 2015, 126, 57–68. [Google Scholar] [CrossRef]
- Pietschmann, P.; Mechtcheriakova, D.; Meshcheryakova, A.; Foger-Samwald, U.; Ellinger, I. Immunology of Osteoporosis: A Mini-Review. Gerontology 2016, 62, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Ginaldi, L.; Di Benedetto, M.C.; De Martinis, M. Osteoporosis, inflammation and ageing. Immun. Ageing 2005, 2, 14. [Google Scholar] [CrossRef] [Green Version]
- Faienza, M.F.; Ventura, A.; Marzano, F.; Cavallo, L. Postmenopausal osteoporosis: The role of immune system cells. Clin. Dev. Immunol. 2013, 2013, 575936. [Google Scholar] [CrossRef] [Green Version]
- Sapir-Koren, R.; Livshits, G. Postmenopausal osteoporosis in rheumatoid arthritis: The estrogen deficiency-immune mechanisms link. Bone 2017, 103, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Mathy-Hartert, M.; Jacquemond-Collet, I.; Priem, F.; Sanchez, C.; Lambert, C.; Henrotin, Y. Curcumin inhibits pro-inflammatory mediators and metalloproteinase-3 production by chondrocytes. Inflamm. Res. 2009, 58, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Csaki, C.; Mobasheri, A.; Shakibaei, M. Synergistic chondroprotective effects of curcumin and resveratrol in human articular chondrocytes: Inhibition of IL-1beta-induced NF-kappaB-mediated inflammation and apoptosis. Arthritis Res. Ther. 2009, 11, R165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Shi, D.; Shen, Y.; Xu, Z.; Dai, J.; Chen, D.; Teng, H.; Jiang, Q. Full-thickness cartilage defects are repaired via a microfracture technique and intraarticular injection of the small-molecule compound kartogenin. Arthritis Res. Ther. 2015, 17, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.K.; Choi, Y.W.; Lee, E.N.; Park, J.K.; Kim, S.G.; Park, D.J.; Kim, B.S.; Lim, Y.T.; Yoon, S. 5-Hydroxymethylfurfural from black garlic extract prevents TNFalpha-induced monocytic cell adhesion to HUVECs by suppression of vascular cell adhesion molecule-1 expression, reactive oxygen species generation and NF-kappaB activation. Phytother. Res. PTR 2011, 25, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Wang, W.; Rong, X.F.; Zhong, Y.; Jia, P.; Zhou, G.Q.; Li, R.H. Chondroprotective effects and multi-target mechanisms of Icariin in IL-1 beta-induced human SW 1353 chondrosarcoma cells and a rat osteoarthritis model. Int. Immunopharmacol. 2014, 18, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Zhang, F.; He, Q.; Wang, J.; Shiu, H.T.; Shu, Y.; Tsang, W.P.; Liang, S.; Zhao, K.; Wan, C. Flavonoid Compound Icariin Activates Hypoxia Inducible Factor-1alpha in Chondrocytes and Promotes Articular Cartilage Repair. PLoS ONE 2016, 11, e0148372. [Google Scholar] [CrossRef]
- Kankala, R.K.; Lu, F.J.; Liu, C.G.; Zhang, S.S.; Chen, A.Z.; Wang, S.B. Effect of Icariin on Engineered 3D-Printed Porous Scaffolds for Cartilage Repair. Materials 2018, 11. [Google Scholar] [CrossRef] [Green Version]
- Calixto-Campos, C.; Carvalho, T.T.; Hohmann, M.S.; Pinho-Ribeiro, F.A.; Fattori, V.; Manchope, M.F.; Zarpelon, A.C.; Baracat, M.M.; Georgetti, S.R.; Casagrande, R.; et al. Vanillic Acid Inhibits Inflammatory Pain by Inhibiting Neutrophil Recruitment, Oxidative Stress, Cytokine Production, and NFkappaB Activation in Mice. J. Nat. Prod. 2015, 78, 1799–1808. [Google Scholar] [CrossRef]
- Rao, Z.; Wang, S.; Wang, J. Protective effects of psoralidin on IL1betainduced chondrocyte apoptosis. Mol. Med. Rep. 2018, 17, 3418–3424. [Google Scholar] [CrossRef]
- Cao, H.J.; Li, C.R.; Wang, L.Y.; Ziadlou, R.; Grad, S.; Zhang, Y.; Cheng, Y.; Lai, Y.X.; Yao, X.S.; Alini, M.; et al. Effect and mechanism of psoralidin on promoting osteogenesis and inhibiting adipogenesis. Phytomedicine 2019, 61, 152860. [Google Scholar] [CrossRef] [PubMed]
- Echtermeyer, F.; Bertrand, J.; Dreier, R.; Meinecke, I.; Neugebauer, K.; Fuerst, M.; Lee, Y.J.; Song, Y.W.; Herzog, C.; Theilmeier, G.; et al. Syndecan-4 regulates ADAMTS-5 activation and cartilage breakdown in osteoarthritis. Nature Med. 2009, 15, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Sampson, E.R.; Jin, H.; Li, J.; Ke, Q.H.; Im, H.J.; Chen, D. MMP13 is a critical target gene during the progression of osteoarthritis. Arthritis Res. Ther. 2013, 15, R5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Wang, D.; Yuan, Y.; Min, J. New insights on the MMP-13 regulatory network in the pathogenesis of early osteoarthritis. Arthritis Res. Ther. 2017, 19, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laine, L.; White, W.B.; Rostom, A.; Hochberg, M. COX-2 selective inhibitors in the treatment of osteoarthritis. Semin. Arthritis Rheum. 2008, 38, 165–187. [Google Scholar] [CrossRef] [PubMed]
- Rainsford, K.D. Anti-inflammatory drugs in the 21st century. Sub-Cell. Biochem. 2007, 42, 3–27. [Google Scholar] [PubMed]
- Kopp, E.; Ghosh, S. Inhibition of NF-kappa B by sodium salicylate and aspirin. Science 1994, 265, 956–959. [Google Scholar] [CrossRef]
- Lee, J.-K.; Lee, S.L.; Shin, T.-Y.S.; Khang, D.K.; Kim, S.-H.K. Anti-inflammatory effect of o-vanillic acid on lipopolysaccharide-stimulated macrophages and inflammation models. J. Food Nutr. Res. 2018, 6, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.A.; Chatterjee, S.S.; Kumar, V. Low dose aspirin like analgesic and anti-inflammatory activities of mono-hydroxybenzoic acids in stressed rodents. Life Sci. 2016, 148, 53–62. [Google Scholar] [CrossRef]
- Lende, A.B.; Kshirsagar, A.D.; Deshpande, A.D.; Muley, M.M.; Patil, R.R.; Bafna, P.A.; Naik, S.R. Anti-inflammatory and analgesic activity of protocatechuic acid in rats and mice. Inflammopharmacology 2011, 19, 255–263. [Google Scholar] [CrossRef]
- Ti, H.; Wu, P.; Xu, L.; Wei, X. A novel icariin type flavonoid from Epimedium pseudowushanense. Nat. Prod. Res. 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.C.; Jeong, Y.H.; Cho, W.K.; Ha, J.H.; Lee, S.J.; Ma, J.Y. Inhibitory Effects of Epimedium Herb on the Inflammatory Response In Vitro and In Vivo. Am. J. Chin. Med. 2015, 43, 953–968. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.H.; Sun, J.S.; Tsai, S.W.; Sheu, S.Y.; Chen, M.H. Icariin protects murine chondrocytes from lipopolysaccharide-induced inflammatory responses and extracellular matrix degradation. Nutr. Res. 2010, 30, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, B.; Hering, T.M.; Caplan, A.I.; Goldberg, V.M.; Yoo, J.U. In vitro chondrogenesis of bone marrow-derived mesenchymal progenitor cells. Exp. Cell Res. 1998, 238, 265–272. [Google Scholar] [CrossRef]
- Zhen, G.; Wen, C.; Jia, X.; Li, Y.; Crane, J.L.; Mears, S.C.; Askin, F.B.; Frassica, F.J.; Chang, W.; Yao, J.; et al. Inhibition of TGF-β signaling in mesenchymal stem cells of subchondral bone attenuates osteoarthritis. Nat. Med. 2013, 19, 704–712. [Google Scholar] [CrossRef]
- Jakob, M.; Demarteau, O.; Schafer, D.; Hintermann, B.; Dick, W.; Heberer, M.; Martin, I. Specific growth factors during the expansion and redifferentiation of adult human articular chondrocytes enhance chondrogenesis and cartilaginous tissue formation in vitro. J. Cell. Biochem. 2001, 81, 368–377. [Google Scholar] [CrossRef]
- Vainieri, M.L.; Wahl, D.; Alini, M.; van Osch, G.; Grad, S. Mechanically stimulated osteochondral organ culture for evaluation of biomaterials in cartilage repair studies. Acta Biomater. 2018, 81, 256–266. [Google Scholar] [CrossRef]
- Tu, F.; Dai, Y.; Yao, Z.; Wang, X.; Yao, X.; Qin, L. Flavonol glycosides from Epimedium pubescens. Chem. Pharm. Bull. 2011, 59, 1317–1321. [Google Scholar] [CrossRef] [Green Version]
- Müller, S.; Acevedo, L.; Wang, X.; Karim, M.Z.; Matta, A.; Mehrkens, A.; Schaeren, S.; Feliciano, S.; Jakob, M.; Martin, I.; et al. Notochordal cell conditioned medium (NCCM) regenerates end-stage human osteoarthritic articular chondrocytes and promotes a healthy phenotype. Arthritis Res. Ther. 2016, 18, 125. [Google Scholar]
- Liu, S.Q.; Saijo, K.; Todoroki, T.; Ohno, T. Induction of human autologous cytotoxic T lymphocytes on formalin-fixed and paraffin-embedded tumour sections. Nat. Med. 1995, 1, 267–271. [Google Scholar] [CrossRef]
- Li, Z.; Lang, G.; Chen, X.; Sacks, H.; Mantzur, C.; Tropp, U.; Mader, K.T.; Smallwood, T.C.; Sammon, C.; Richards, R.G.; et al. Polyurethane scaffold with in situ swelling capacity for nucleus pulposus replacement. Biomaterials 2016, 84, 196–209. [Google Scholar] [CrossRef] [PubMed]
- de Abreu Costa, L.; Henrique Fernandes Ottoni, M.; Dos Santos, M.G.; Meireles, A.B.; Gomes de Almeida, V.; de Fatima Pereira, W.; Alves de Avelar-Freitas, B.; Eustaquio Alvim Brito-Melo, G. Dimethyl Sulfoxide (DMSO) Decreases Cell Proliferation and TNF-alpha, IFN-gamma, and IL-2 Cytokines Production in Cultures of Peripheral Blood Lymphocytes. Molecules 2017, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, A.J.; Gardner, O.F.; Williams, R.; Alini, M.; Archer, C.W.; Stoddart, M.J. Human Articular Cartilage Progenitor Cells Are Responsive to Mechanical Stimulation and Adenoviral-Mediated Overexpression of Bone-Morphogenetic Protein 2. PLoS ONE 2015, 10, e0136229. [Google Scholar] [CrossRef] [PubMed]
- Scotti, C.; Osmokrovic, A.; Wolf, F.; Miot, S.; Peretti, G.M.; Barbero, A.; Martin, I. Response of human engineered cartilage based on articular or nasal chondrocytes to interleukin-1beta and low oxygen. Tissue Eng. Part A 2012, 18, 362–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitley, C.B.; Ridnour, M.D.; Draper, K.A.; Dutton, C.M.; Neglia, J.P. Diagnostic test for mucopolysaccharidosis. I. Direct method for quantifying excessive urinary glycosaminoglycan excretion. Clin. Chem. 1989, 35, 374–379. [Google Scholar]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Milz, S.; Aktas, T.; Putz, R.; Benjamin, M. Expression of extracellular matrix molecules typical of articular cartilage in the human scapholunate interosseous ligament. J. Anat. 2006, 208, 671–679. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | % Cell Numbers (Normalized to Control Vehicle) | ||||
|---|---|---|---|---|---|
| Conc.[µM] | 1 | 10 | 25 | 50 | |
| 5-Hydroxymethylfurfural | 111.4 ± 6.6 | 107.0 ± 11.2 | 110.2 ± 9.4 | 107.9 ± 3.3 | |
| Protocatechuicaldehyde | 100.1 ± 4.2 | 96.0 ± 9.3 | 94.8 ± 6.4 | 81.2 ± 5.4 | |
| Vanilic acid | 102.1 ± 2.4 | 96.8 ± 3.7 | 115.7 ± 3.2 | 112.6 ± 2.1 | |
| 4-Hydroxybenzoic acid | 103.4 ± 2.5 | 102 ± 9.6 | 105 ± 3.4 | 78.6 ± 6.9 | |
| Chlorogenic acid | 77.8 ± 3.2 | 78.6 ± 4.8 | 77.8 ± 5.2 | 79.8 ± 5.6 | |
| Cryptochlorogenic acid | 86.2 ± 8.5 | 86 ± 7.9 | 93.8 ± 5.2 | 78.3 ± 8.4 | |
| Loganic acid | 85.6 ± 3.6 | 94.7 ± 3 | 91.5 ± 1.7 | 93.6 ± 4.9 | |
| Loganin | 107 ± 5.6 | 109.2 ± 5.1 | 110.6 ± 9.8 | 102.8 ± 3.6 | |
| Isobavachalcone | 102.1 ± 6.6 | 108.7 ± 5.7 | 105.7 ± 0.6 | 88.4 ± 8.8 | |
| Sweroside | 110.2 ± 2.3 | 106.7 ± 4.1 | 112.5 ± 1.8 | 107.7 ± 9.8 | |
| (+)-Cycloolivil | 101.5 ± 1.5 | 98. ± 2.1 | 105.6 ± 4.9 | 103.2 ± 8.2 | |
| Baohuoside I | 82.8 ± 6.3 | 76.3 ± 1.8 | 77.5 ± 0.4 | 79.8 ± 5.8 | |
| 2’-O-rhamnosylicariside II | 102.1 ± 6.6 | 105.5 ± 4.7 | 91.8 ± 3.2 | 102.9 ± 2.1 | |
| Epimedin A | 83.9 ± 5.6 | 84.8 ± 8.1 | 97.1 ± 6.9 | 111.3 ± 5.1 | |
| Epimedin B | 82.7 ± 9.2 | 88 ± 9.9 | 87.8 ± 9.1 | 94. ± 7.9 | |
| Epimedin C | 87.5 ± 0.6 | 89.5 ± 6.5 | 88.1 ± 3.7 | 89.8 ± 6.4 | |
| Isobavachin | 87.3 ± 1.3 | 91.5 ± 8.2 | 89.2 ± 0.8 | 85.7 ± 0.1 | |
| Bavachin | 109.1 ± 2.1 | 102 ± 8.4 | 89.2 ± 9.5 | 91.7 ± 2.1 | |
| Bavachinin | 96.4 ± 1.1 | 78.1 ± 6.6 | 79.9 ± 5.1 | 79.7 ± 3 | |
| Neobavaisoflavone | 84.4 ± 8.6 | 89.6 ± 1.9 | 99 ± 2.5 | 76.1 ± 2.2 | |
| Corylin | 89.6 ± 2.4 | 94 ± 3.7 | 87.8 ± 1.6 | 79.3 ± 3.1 | |
| Epimedin A1 | 95.48 ± 4.3 | 85.49 ± 0.5 | 88.21 ± 3.1 | 95.46 ± 2.4 | |
| Psoralen | 83.6 ± 5.1 | 80.3 ± 5.3 | 85.1 ± 6.4 | 84.8 ± 8.3 | |
| Isopsoralen | 86.2 ± 8.6 | 80.2 ± 1.9 | 83 ± 2.7 | 85.4 ± 3.2 | |
| (S)-Bukuchiol | 89.1 ± 4.4 | 94.4 ± 3.5 | 104.7 ± 4.2 | 88.4 ± 4.2 | |
| Psoralidin | 106.5 ± 6.3 | 84.7 ± 1.4 | 86.4 ± 5.9 | 85.1 ± 4.8 | |
| Asperosaponin VI | 93.9 ± 2.8 | 99 ± 9.2 | 103.8 ± 4.5 | 93.9 ± 4.8 | |
| Baohuoside II | 103.6 ± 5.9 | 96.4 ± 7.6 | 95 ± 5.2 | 79.7 ± 2.9 | |
| Epimedoside A | 89 ± 4.7 | 87.9 ± 3.1 | 90.6 ± 4.4 | 85.6 ± 3.7 | |
| Baohuoside V | 98.6 ± 8.7 | 100 ± 6.5 | 100.9 ± 7.8 | 78.5 ± 3.8 | |
| Corylifol A | 86.1 ± 3.3 | 85.3 ± 1.8 | 94.6 ± 0.9 | 103.8 ± 2.6 | |
| 4’-O-Methyl-broussochalcone | 81.4 ± 2.9 | 85.4 ± 2.4 | 95.4 ± 3.6 | 97.5 ± 2.3 | |
| Anhydroicaritin | 85.2 ± 2.2 | 83.4 ± 6.6 | 86.2 ± 1.5 | 81.8 ± 2.4 | |
| Icariin | 95.7 ± 3.6 | 101.4 ± 3.7 | 95.5 ± 3.2 | 101.5 ± 5.7 | |
| No | Name of the Compound | Molecular Formula | Molecular Weight | Component Herb |
|---|---|---|---|---|
| 1 | 5-Hydroxymethylfurfural | C6H6O3 | 126 | H.E |
| 2 | Protocatechuicaldehyde | C7H6O3 | 138 | R.S |
| 3 | Vanilic acid | C8H8O4 | 168 | R.S |
| 4 | 4-Hydroxybenzoic acid | C7H6O3 | 138 | R.S |
| 5 | Chlorogenic acid | C16H18O9 | 354 | H.E |
| 6 | Cryptochlorogenic acid | C16H18O9 | 354 | H.E |
| 7 | Loganic acid | C16H24O10 | 376 | R.D |
| 8 | Loganin | C17H26O10 | 390 | R.D |
| 9 | Isobavachalcone | C20H20O4 | 324 | F.P |
| 10 | Sweroside | C16H22O9 | 358 | R.D |
| 11 | (+)-Cycloolivil | C20H24O7 | 376 | H.E |
| 12 | Baohuside I | C27H30O10 | 514 | H.E |
| 13 | 2′′-O-rhamnosylicariside II | C33H40O14 | 660 | H.E |
| 14 | Epimedin A | C39H50O2 | 838 | H.E |
| 15 | Epimedin B | C38H48O19 | 808 | H.E |
| 16 | Epimedin C | C39H50O19 | 822 | H.E |
| 17 | Isobavachin | C20H20O4 | 324 | F.P |
| 18 | Bavachin | C20H20O4 | 324 | F.P |
| 19 | Bavachinin | C21H22O4 | 338 | F.P |
| 20 | Neobavaisoflavone | C20H18O4 | 322 | F.P |
| 21 | Corylin | C20H16O4 | 320 | F.P |
| 22 | Epimedin A1 | C39H50O20 | 838 | H.E |
| 23 | Psoralen | C11H6O3 | 186 | F.P |
| 24 | Isopsoralen | C11H6O3 | 186 | F.P |
| 25 | (S)-Bukuchiol | C18H24O | 256 | F.P |
| 26 | Psoralidin | C20H16O5 | 336 | F.P |
| 27 | Asperosaponin VI | C47H76O18 | 390 | R.D |
| 28 | Baohuside II | C26H28O10 | 500 | H.E |
| 29 | Epimedoside A | C32H38O15 | 662 | H.E |
| 30 | Baohuside V | C39H50O19 | 822 | H.E |
| 31 | Corylifol A | C25H26O4 | 390 | F.P |
| 32 | 4′-Methylbavachalcone | C21H22O4 | 338 | F.P |
| 33 | Icaitin | C21H20O6 | 368 | H.E |
| 34 | Icariin | C33H40O15 | 676 | H.E |
| Pellet Culture | Group | Culture Phase I (Cartilage Generation) | Culture Phase II (IL-1β/TNFα Exposure; Inflammatory phase) | Culture Phase III (Treatment) | ||
|---|---|---|---|---|---|---|
| Time | Time | Compound | Time | Compound | ||
| Control (IL-1β/TNFα) | 1 week | 3 days | -- | n/a | ||
| Short term | Treatment group (IL-1β/TNFα + compound) | 1 week | 3 days | + | n/a | |
| Control (IL-1β/TNFα) | 2 weeks | 3 days | -- | 2 weeks | -- | |
| Long term | Treatment group (IL-1β/TNFα - compound) | 2 weeks | 3 days | + | 2 weeks | + |
| Gene | Probe Type | Assay ID |
|---|---|---|
| MMP-1 | 5′ FAM-3′ NFQ | Hs00899658_m1 |
| MMP-3 | 5′ FAM-3′ NFQ | Hs00968305_m1 |
| 18s fast | 5′ FAM-3′ NFQ | Hs99999901_s1 |
| Gene | Primer/Probe Type | Sequence |
|---|---|---|
| MMP-13 | Primer forward (5′-3′) Primer reverse (5′-3′) Probe (5′ FAM/3′ TAMRA) | CGGCCACTCCTTAGGTCTTG TTTTGCCGGTGTAGGTGTAGATAG CTCCAAGGACCCTGGAGCACTCATGT |
| COX-2 | Primer forward (5′-3′) Primer reverse (5′-3′) Probe (5′ FAM/3′ TAMRA) | TTGTACCCGGACAGGATTCTATG TGTTTGGAGTGGGTTTCAGAAATA GAAAACTGCTCAACACCGGAATTTTTGACAA |
| Col2a1 | Primer forward (5′-3′) Primer reverse (5′-3′) Probe (5′ FAM/3′ TAMRA) | GGCAATAGCAGGTTCACGTACA GATAACAGTCTTGCCCCACTTACC CCTGAAGGATGGCTGCACGAAACATAC |
| ACAN | Primer forward (5′-3′) Primer reverse (5′-3′) Probe (5′ FAM/3′ TAMRA) | AGTCCTCAAGCCTCCTGTACTCA CGGGAAGTGGCGGTAACA CCGGAATGGAAACGTGAATCAGAATCAACT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziadlou, R.; Barbero, A.; Stoddart, M.J.; Wirth, M.; Li, Z.; Martin, I.; Wang, X.-l.; Qin, L.; Alini, M.; Grad, S. Regulation of Inflammatory Response in Human Osteoarthritic Chondrocytes by Novel Herbal Small Molecules. Int. J. Mol. Sci. 2019, 20, 5745. https://doi.org/10.3390/ijms20225745
Ziadlou R, Barbero A, Stoddart MJ, Wirth M, Li Z, Martin I, Wang X-l, Qin L, Alini M, Grad S. Regulation of Inflammatory Response in Human Osteoarthritic Chondrocytes by Novel Herbal Small Molecules. International Journal of Molecular Sciences. 2019; 20(22):5745. https://doi.org/10.3390/ijms20225745
Chicago/Turabian StyleZiadlou, Reihane, Andrea Barbero, Martin J. Stoddart, Michael Wirth, Zhen Li, Ivan Martin, Xin-luan Wang, Ling Qin, Mauro Alini, and Sibylle Grad. 2019. "Regulation of Inflammatory Response in Human Osteoarthritic Chondrocytes by Novel Herbal Small Molecules" International Journal of Molecular Sciences 20, no. 22: 5745. https://doi.org/10.3390/ijms20225745
APA StyleZiadlou, R., Barbero, A., Stoddart, M. J., Wirth, M., Li, Z., Martin, I., Wang, X. -l., Qin, L., Alini, M., & Grad, S. (2019). Regulation of Inflammatory Response in Human Osteoarthritic Chondrocytes by Novel Herbal Small Molecules. International Journal of Molecular Sciences, 20(22), 5745. https://doi.org/10.3390/ijms20225745