Recontamination of Healthcare Surfaces by Repeated Wiping with Biocide-Loaded Wipes: “One Wipe, One Surface, One Direction, Dispose” as Best Practice in the Clinical Environment

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
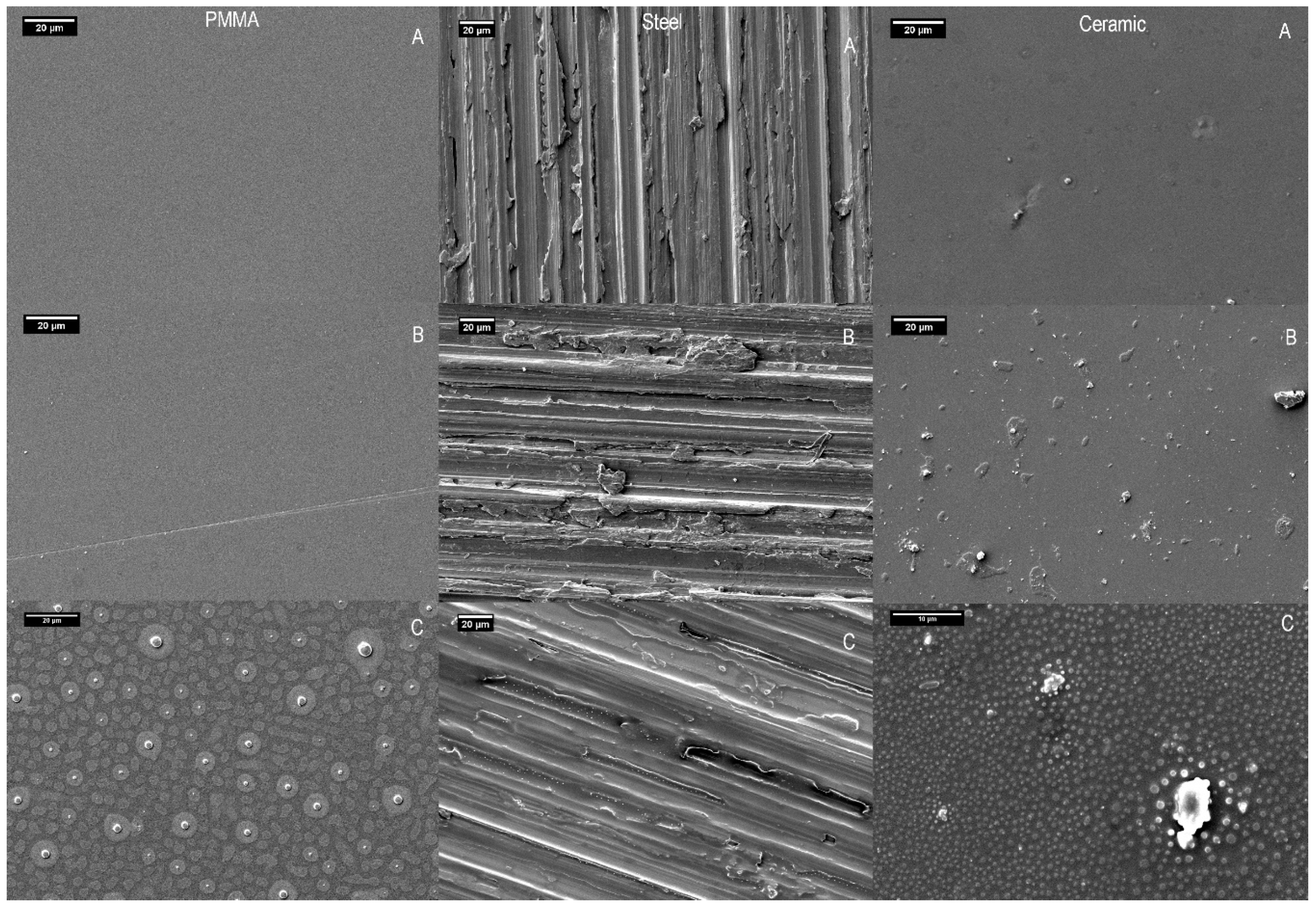
2.1. Analysis of Surfaces
2.2. Residual Antimicrobial Activity
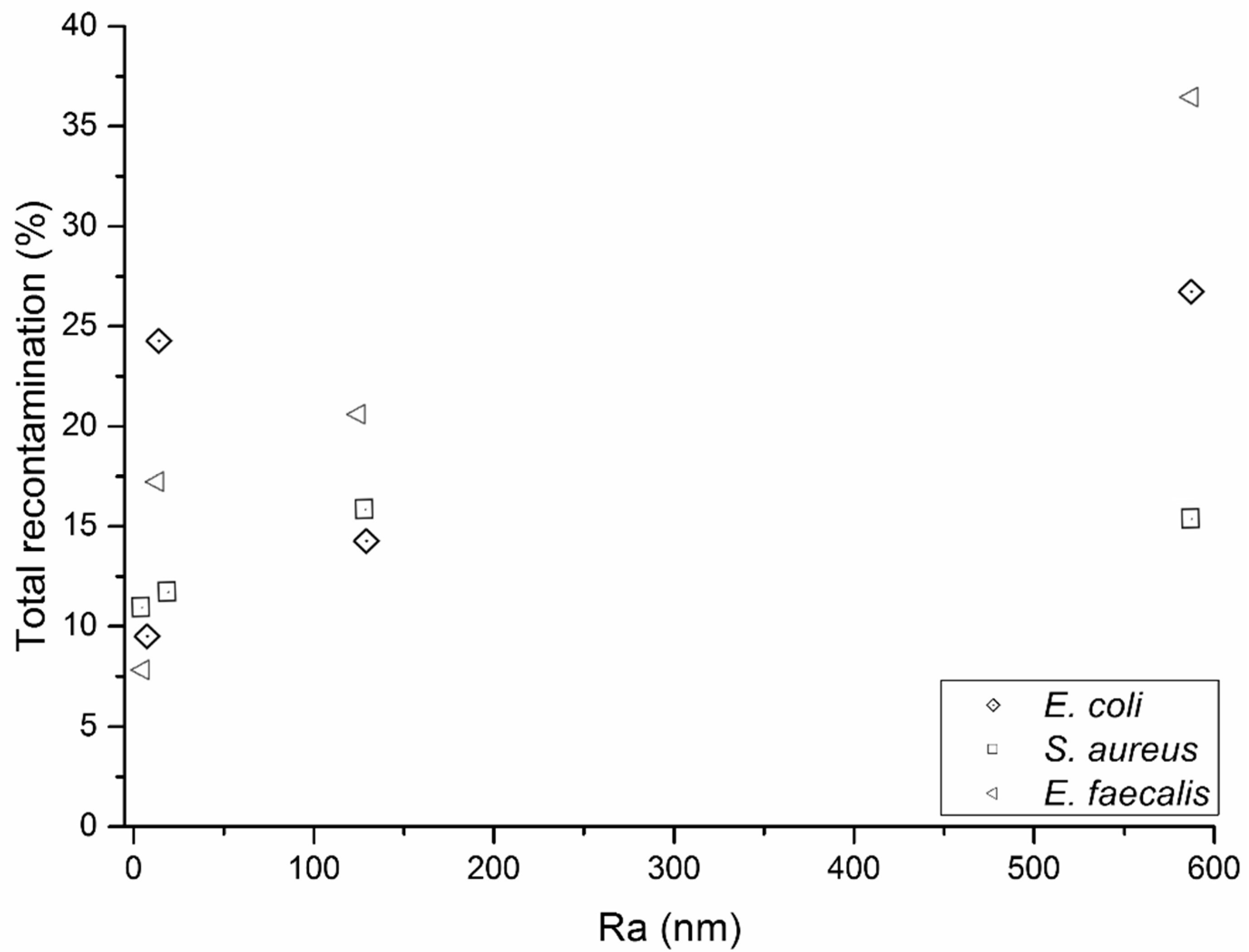
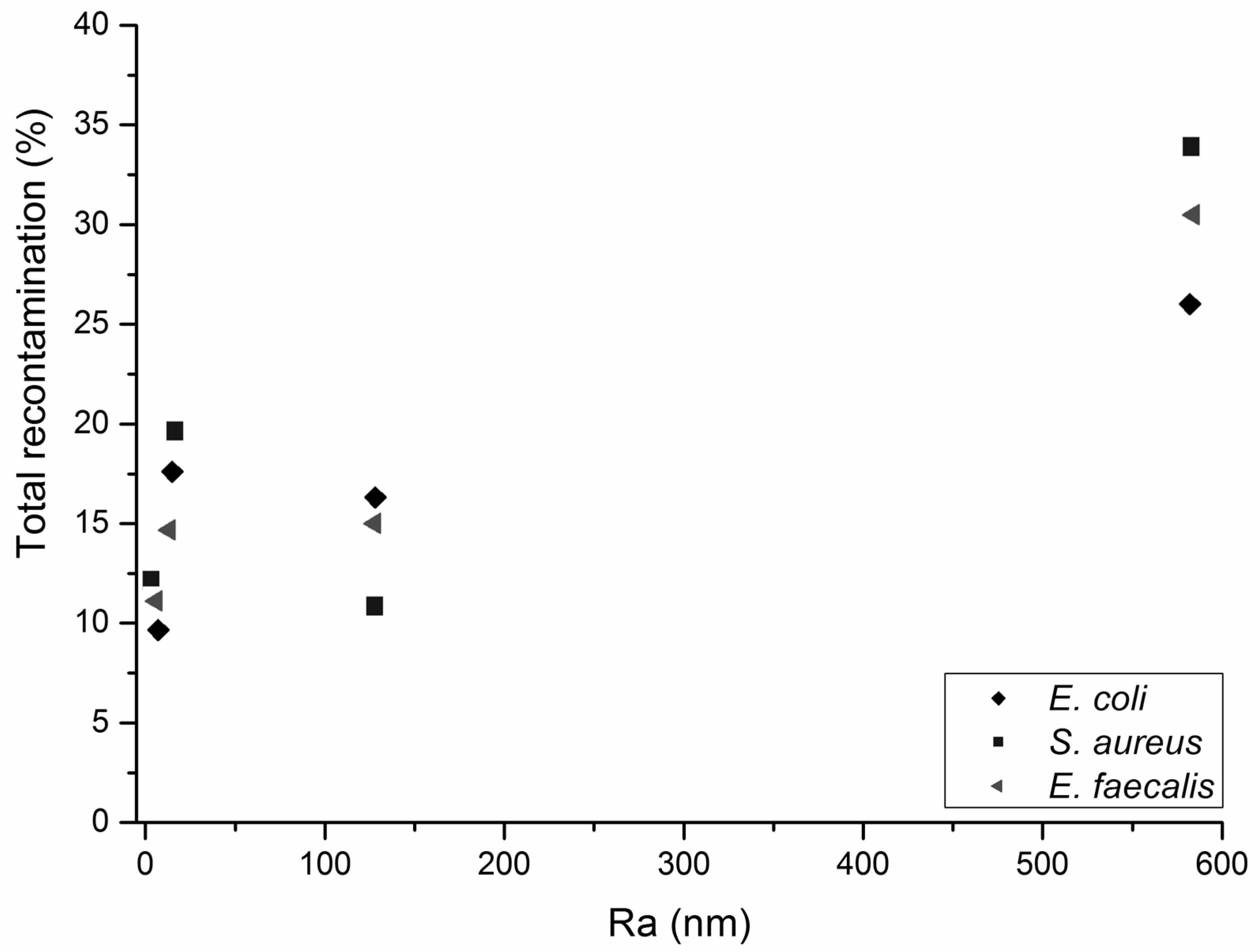
2.3. Bacterial Removal Efficiency and the Effect of Surface Roughness
2.4. Surface Recontamination during Successive Wiping Cycles
3. Materials and Methods
3.1. Nonwoven Production
3.2. Biocide and Neutraliser
3.2.1. Biocide
3.2.2. Neutraliser Toxicity and Efficacy Tests
3.2.3. Impregnation of the Wipe with Biocide
3.3. Model Healthcare Surfaces
3.4. Scanning Electron Microscopy and Energy-Dispersive X-ray Spectroscopy
3.5. Surface Roughness
3.6. Bacterial Strains
3.7. Microorganism Removal Efficiency from Healthcare Surfaces
3.8. Recontamination of Surfaces
3.9. Residual Antimicrobial Activity
3.10. Surface Wetting Tension
3.11. Statistical Analysis
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Williams, G.J.; Denyer, S.; Hosein, I.; Hill, D.; Maillard, J.-Y. The development of a new three-step protocol to determine the efficacy of disinfectant wipes on surfaces contaminated with Staphylococcus aureus. J. Hosp. Infect. 2007, 67, 329–335. [Google Scholar] [CrossRef]
- Oelberg, D.G.; Joyner, S.E.; Jiang, X.; Laborde, D.; Islam, M.P.; Pickering, L.K. Detection of pathogen transmission in neonatal nurseries using DNA markers as surrogate indicators. Pediatrics 2000, 105, 311–315. [Google Scholar] [CrossRef]
- Mary, K.H.; Donald, W.B.; Elizabeth, A.L.; Charity, G.M.; Robert, A.W. Risk of Hand or Glove Contamination After Contact with Patients Colonized with Vancomycin-Resistant Enterococcus or the Colonized Patients’ Environment. Infect. Control Hosp. Epidemiol. 2008, 29, 149–154. [Google Scholar]
- Drees, M.L.; Snydman, D.R.; Schmid, C.H.; Barefoot, L.; Hansjosten, K.; Vue, P.M.; Cronin, M.; Nasraway, S.A.; Golan, Y. Prior Environmental Contamination Increases the Risk of Acquisition of Vancomycin-Resistant Enterococci. Clin. Infect. Dis. 2008, 46, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Datta, R.; Platt, R.; Yokoe, D.S.; Huang, S.S. Environmental Cleaning Intervention and Risk of Acquiring Multidrug-Resistant Organisms From Prior Room Occupants. Arch. Intern. Med. 2011, 171, 491–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rampling, A.; Wiseman, S.; Davis, L.; Hyett, A.; Walbridge, A.; Payne, G.; Cornaby, A. Evidence that hospital hygiene is important in the control of methicillin-resistant Staphylococcus aureus. J. Hosp. Infect. 2001, 49, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Siani, H.; Cooper, C.J.; Maillard, J.-Y. Efficacy of ‘sporicidal’ wipes against Clostridium difficile. Am. J. Infect. Control 2011, 39, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Koh, E.; Russell, S.J.; Mao, N. Influence of Fabric Structure on Dynamic Dirt Removal in Hydroentangled Wipes in Nonwovens Research Academy (NRA); EDANA: Chemnitz, Germany, 2008; pp. 268–280. [Google Scholar]
- Oathout, J. Determining the Dynamic Efficiency of Cleanroom Wipers for Removal of Liquids and Particles from Surfaces. J. IEST 1999, 42, 17–26. [Google Scholar] [CrossRef]
- Ramm, L.; Siani, H.; Wesgate, R.; Maillard, J.-Y. Pathogen transfer and high variability in pathogen removal by detergent wipes. Am. J. Infect. Control 2015, 43, 724–728. [Google Scholar] [CrossRef]
- Neely, A.N.; Orloff, M.M. Survival of Some Medically Important Fungi on Hospital Fabrics and Plastics. J. Clin. Microbiol. 2001, 39, 3360–3361. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, F.; Abolghasemi, S.; Parhizgari, N.; Moradpour, F. Effect of Silver Nanoparticles on Common Bacteria in Hospital Surfaces. Jundishapur J. Microbiol. 2013, 6, 209–214. [Google Scholar] [CrossRef] [Green Version]
- Rangel-Frausto, M.S.; Houston, A.K.; Bale, M.J.; Fu, C.; Wenzel, R.P. An experimental model for study ofCandida survival and transmission in human volunteers. Eur. J. Clin. Microbiol. Infect. Dis. 1994, 13, 590–595. [Google Scholar] [CrossRef]
- Weber, D.J.; Rutala, W.A.; Miller, M.B.; Huslage, K.; Sickbert-Bennett, E. Role of hospital surfaces in the transmission of emerging health care-associated pathogens: Norovirus, Clostridium difficile, and Acinetobacter species. Am. J. Infect. Control 2010, 38, S25–S33. [Google Scholar] [CrossRef]
- Tuson, H.H.; Weibel, D.B. Bacteria-surface interactions. Soft Matter 2013, 9, 4368–4380. [Google Scholar] [CrossRef] [Green Version]
- McDonnell, G.; Russell, A.D. Antiseptics and Disinfectants: Activity, Action, and Resistance. Clin. Microbiol. Rev. 1999, 12, 147–179. [Google Scholar] [CrossRef] [Green Version]
- Dettenkofer, M.; Block, C. Hospital disinfection: Efficacy and safety issues. Curr. Opin. Infect. Dis. 2005, 18, 320–325. [Google Scholar] [CrossRef]
- Dettenkofer, M.; Spencer, R. Importance of environmental decontamination—A critical view. J. Hosp. Infect. 2007, 65, 55–57. [Google Scholar] [CrossRef]
- Edwards, N.; Best, E.L.; Connell, S.D.; Goswami, P.; Carr, C.M.; Wilcox, M.H.; Russell, S.J. Role of surface energy and nano-roughness in the removal efficiency of bacterial contamination by nonwoven wipes from frequently touched surfaces. Sci. Technol. Adv. Mater. 2017, 18, 197–209. [Google Scholar] [CrossRef]
- Lee, J.; Lopes, J.; Pascall, M.A. Development of a Sanitizing Fabric Wipe for Use on Food Contact Surfaces. J. Food Sci. 2007, 72, M375–M381. [Google Scholar] [CrossRef]
- Williams, G.J.; Denyer, S.P.; Hosein, I.K.; Hill, D.W.; Maillard, J.-Y. Limitations of the Efficacy of Surface Disinfection in the Healthcare Setting. Infect. Control Hosp. Epidemiol. 2009, 30, 570–573. [Google Scholar] [CrossRef]
- Sattar, S.A.; Maillard, J.-Y. The crucial role of wiping in decontamination of high-touch environmental surfaces: Review of current status and directions for the future. Am. J. Infect. Control 2013, 41, S97–S104. [Google Scholar] [CrossRef] [PubMed]
- Maillard, J.Y. RCN Guidance on the Selection and Use of Disinfectant Wipes; Royal College of Nursing: London, UK, 2011. [Google Scholar]
- Dancer, S.J.; Kramer, A. Four steps to clean hospitals: LOOK, PLAN, CLEAN and DRY. J. Hosp. Infect. 2019, 103, e1–e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ASTM E2967. Test Method for Assessing the Ability of Pre-Wetted Towelettes to Remove and Transfer Bacterial Contamination on Hard, Non-Porous Environmental Surfaces Using the Wiperato; ASTM International: West Conshohocken, PA, USA, 2015. [Google Scholar]
- Edwards, N.; Best, E.; Goswami, P.; Wilcox, M.; Russell, S. Factors affecting removal of bacterial pathogens from healthcare surfaces during dynamic wiping. Text. Res. J. 2019, 89, 580–589. [Google Scholar] [CrossRef]
- Taylor, J.H.; Rogers, S.J.; Holah, J. A comparison of the bactericidal efficacy of 18 disinfectants used in the food industry against Escherichia coli O157:H7 and Pseudomonas aeruginosa at 10 and 20 °C. J. Appl. Microbiol. 1999, 87, 718–725. [Google Scholar] [CrossRef]
- Knapp, L.; Rushton, L.; Stapleton, H.; Sass, A.; Stewart, S.; Amezquita, A.; McClure, P.; Mahenthiralingam, E.; Maillard, J.-Y. The effect of cationic microbicide exposure against Burkholderia cepacia complex (Bcc); the use of Burkholderia lata strain 383 as a model bacterium. J. Appl. Microbiol. 2013, 115, 1117–1126. [Google Scholar] [CrossRef]
- Berendt, A.E.; Turnbull, L.; Spady, D.; Rennie, R.P.; Forgie, S.E. Three swipes and you’re out: How many swipes are needed to decontaminate plastic with disposable wipes? Am. J. Infect. Control 2011, 39, 442–443. [Google Scholar] [CrossRef]
- Tomasino, S.F.; Fiumara, R.M.; Cottrill, M.P. Enumeration Procedure for Monitoring Test Microbe Populations on Inoculated Carriers in AOAC Use-Dilution Methods. J. AOAC Int. 2006, 89, 1629–1634. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PMMA | Weight % | Steel (R) | Weight % | Ceramic | Weight % | |||
|---|---|---|---|---|---|---|---|---|
| Element | Biocide | Control | Element | Biocide | Control | Element | Biocide | Control |
| Carbon (C) | 35.71 | 61.88 | C | 32.64 | 7.48 | C | 32.47 | - |
| Oxygen (O) | 42.38 | 38.12 | O | 8.05 | - | O | 29.53 | 43.95 |
| Sodium (Na) | 14.20 | - | Na | 3.07 | - | Na | 4.59 | - |
| Phosphorus (P) | 6.34 | - | P | 0.98 | - | Aluminium (Al) | 2.70 | 4.26 |
| Chlorine (Cl) | 1.37 | - | Cl | 0.39 | - | Silicon (Si) | 17.34 | 31.97 |
| Chromium (Cr) | 10.32 | 18.42 | Cl | 0.48 | - | |||
| Manganese (Mn) | 1.3 | 1.65 | Potassium (K) | 2.48 | 3.84 | |||
| Iron (Fe) | 39.55 | 65.07 | Calcium (Ca) | 4.36 | 6.74 | |||
| Nickel (Ni) | 3.69 | 7.56 | Zinc (Zn) | 6.05 | 9.23 | |||
| Bacteria | Surface | Mean Recovery (%) | SE |
|---|---|---|---|
| E. coli | Ceramic | +8 | 11 |
| S. aureus | Ceramic | −8 | 3 |
| E. faecalis | Ceramic | +7 | 13 |
| E. coli | Steel (R) | −3 | 8 |
| S. aureus | Steel (R) | −5 | 3 |
| E. faecalis | Steel (R) | −12 | 9 |
| E. coli | PMMA | −3 | 15 |
| S. aureus | PMMA | −4 | 14 |
| E. faecalis | PMMA | −16 | 27 |
| Surface | Organic Load | Contact Angle | Wetting Tension | Roughness (Ra) | Tukey-Roughness |
|---|---|---|---|---|---|
| PMMA | Clean | 29.22° | 63.54 mJ·m−2 | 3.8 nm | A |
| 0.015 g·m−2 BSA | 62.30° | 33.84 mJ·m−2 | n/a | ||
| Ceramic | Clean | 18.43° | 69.06 mJ·m−2 | 14.8 nm | A |
| 0.015 g·m−2 BSA | 38.37° | 57.08 mJ·m−2 | n/a | ||
| Steel (S) | Clean | 38.61° | 65.95 mJ·m−2 | 128 nm | B |
| 0.015 g·m−2 BSA | 64.20° | 32.67 mJ·m−2 | n/a | ||
| Steel (R) | Clean | 60.49° | 72.80 mJ·m−2 | 583 nm | C |
| 0.015 g·m−2 BSA | 63.90° | 32.03 mJ·m−2 | n/a | ||
| Bacteria | Surface | Removal (%) | SE | CFU on Wipe * | T 1 (%) | T 2 (%) | T 3 (%) | Total (%) |
|---|---|---|---|---|---|---|---|---|
| E. coli | Ceramic | 83 | 5 | 4,900,000 | 12 | 6 | 6 | 24 |
| S. aureus | Ceramic | 81 | 4 | 10,250,000 | 7 | 2 | 2 | 11 |
| E. faecalis | Ceramic | 73 | 7 | 2,016,667 | 12 | 3 | 2 | 17 |
| E. coli | PMMA | 85 | 7 | 7,700,000 | 8 | 1 | 1 | 10 |
| S. aureus | PMMA | 82 | 1 | 4,116,667 | 2 | 6 | 2 | 10 |
| E. faecalis | PMMA | 84 | 1 | 5,133,333 | 3 | 4 | 1 | 8 |
| E. coli | Steel (S) | 80 | 6 | 4,916,667 | 9 | 5 | 1 | 15 |
| S. aureus | Steel (S) | 84 | 4 | 8,350,000 | 8 | 6 | 2 | 16 |
| E. faecalis | Steel (S) | 87 | 2 | 3,666,667 | 11 | 9 | 1 | 21 |
| E. coli | Steel (R) | 83 | 5 | 4,600,000 | 22 | 2 | 3 | 27 |
| S. aureus | Steel (R) | 89 | 1 | 9,800,000 | 7 | 7 | 3 | 17 |
| E. faecalis | Steel (R) | 84 | 2 | 3,800,000 | 20 | 14 | 3 | 37 |
| Bacteria | Surface | Removal (%) | SE | CFU on Wipe * | T 1 (%) | T 2 (%) | T 3 (%) | Total (%) |
|---|---|---|---|---|---|---|---|---|
| E. coli | Ceramic | 85 | 6 | 3,383,333 | 12 | 4 | 1 | 17 |
| S. aureus | Ceramic | 89 | 5 | 12,483,333 | 16 | 1 | 2 | 19 |
| E. faecalis | Ceramic | 80 | 2 | 2,483,333 | 11 | 3 | 1 | 15 |
| E. coli | PMMA | 79 | 3 | 9,866,667 | 7 | 2 | 1 | 10 |
| S. aureus | PMMA | 80 | 3 | 7,633,333 | 5 | 4 | 3 | 12 |
| E. faecalis | PMMA | 78 | 6 | 4,300,000 | 3 | 3 | 5 | 11 |
| E. coli | Steel (S) | 83 | 3 | 4,550,000 | 9 | 5 | 2 | 16 |
| S. aureus | Steel (S) | 83 | 3 | 8,250,000 | 6 | 4 | 1 | 11 |
| E. faecalis | Steel (S) | 83 | 6 | 4,700,000 | 10 | 6 | 1 | 17 |
| E. coli | Steel (R) | 88 | 1 | 6,600,000 | 11 | 8 | 7 | 26 |
| S. aureus | Steel (R) | 70 | 6 | 6,283,333 | 16 | 14 | 4 | 34 |
| E. faecalis | Steel (R) | 80 | 2 | 3,900,000 | 17 | 9 | 5 | 31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edwards, N.W.M.; Best, E.L.; Goswami, P.; Wilcox, M.H.; Russell, S.J. Recontamination of Healthcare Surfaces by Repeated Wiping with Biocide-Loaded Wipes: “One Wipe, One Surface, One Direction, Dispose” as Best Practice in the Clinical Environment. Int. J. Mol. Sci. 2020, 21, 9659. https://doi.org/10.3390/ijms21249659
Edwards NWM, Best EL, Goswami P, Wilcox MH, Russell SJ. Recontamination of Healthcare Surfaces by Repeated Wiping with Biocide-Loaded Wipes: “One Wipe, One Surface, One Direction, Dispose” as Best Practice in the Clinical Environment. International Journal of Molecular Sciences. 2020; 21(24):9659. https://doi.org/10.3390/ijms21249659
Chicago/Turabian StyleEdwards, Nicholas W. M., Emma L. Best, Parikshit Goswami, Mark H. Wilcox, and Stephen J. Russell. 2020. "Recontamination of Healthcare Surfaces by Repeated Wiping with Biocide-Loaded Wipes: “One Wipe, One Surface, One Direction, Dispose” as Best Practice in the Clinical Environment" International Journal of Molecular Sciences 21, no. 24: 9659. https://doi.org/10.3390/ijms21249659
APA StyleEdwards, N. W. M., Best, E. L., Goswami, P., Wilcox, M. H., & Russell, S. J. (2020). Recontamination of Healthcare Surfaces by Repeated Wiping with Biocide-Loaded Wipes: “One Wipe, One Surface, One Direction, Dispose” as Best Practice in the Clinical Environment. International Journal of Molecular Sciences, 21(24), 9659. https://doi.org/10.3390/ijms21249659