Co-Expression Effect of SLC7A5/SLC3A2 to Predict Response to Endocrine Therapy in Oestrogen-Receptor-Positive Breast Cancer

 , , ,
, , , 

Abstract
:1. Introduction
2. Results
2.1. SLC7A5/SLC3A2 Co-Expression and Clinicopathological Characteristics
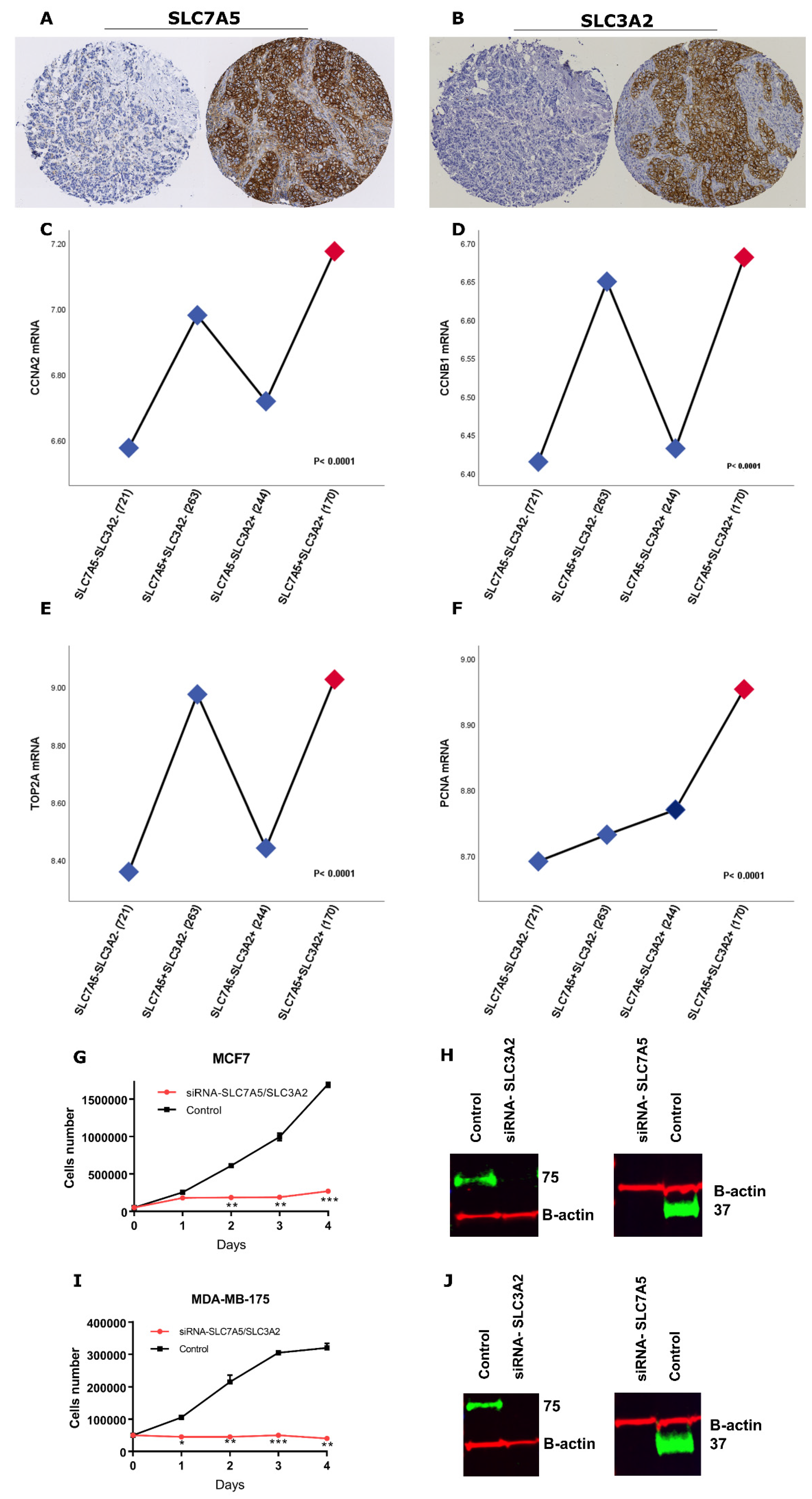
2.2. SLC7A5/SLC3A2 Co-Expression Associates with Proliferation in ER+ Breast Cancer Cells
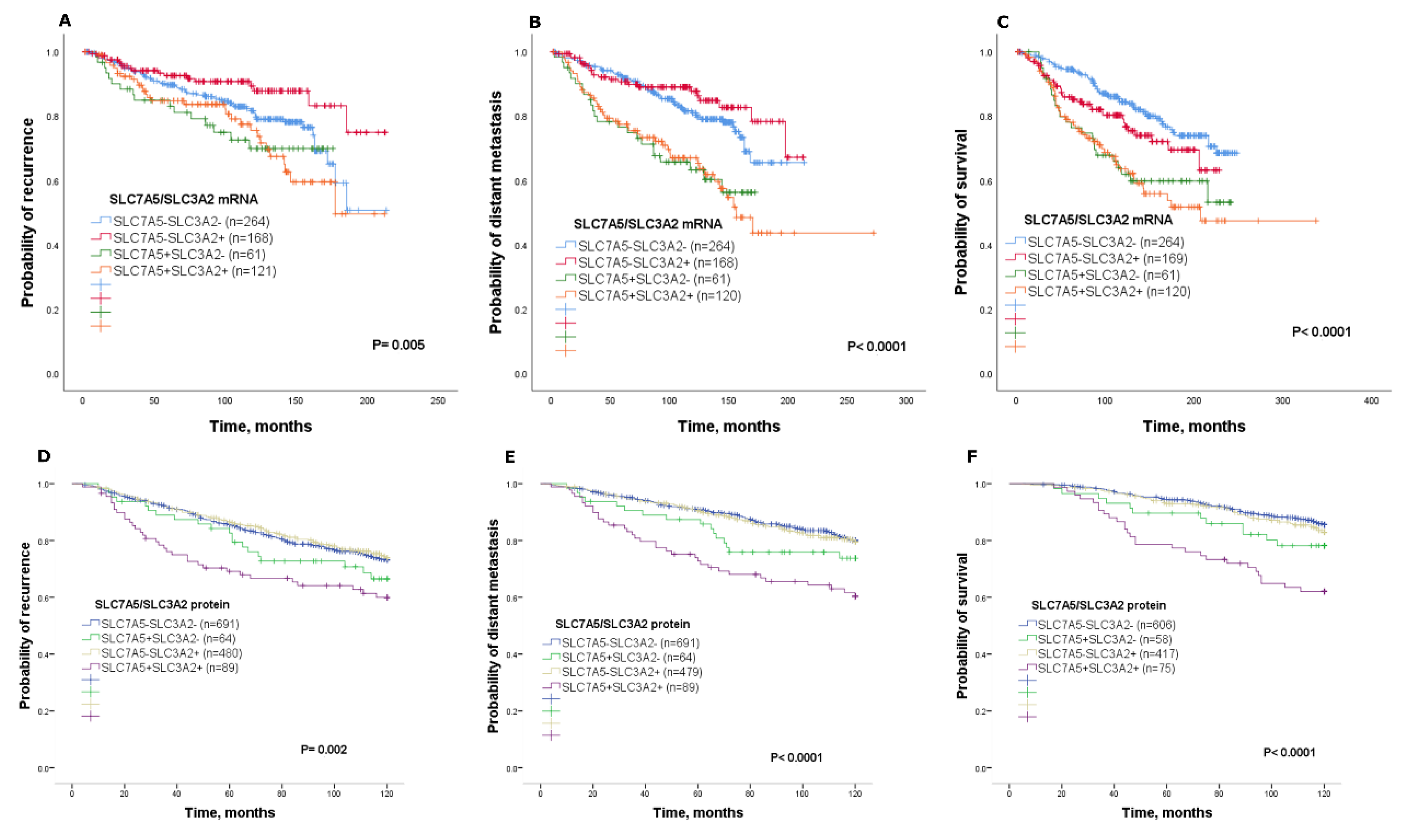
2.3. Prognostic Value of SLC7A5/SLC3A2 Co-Expression
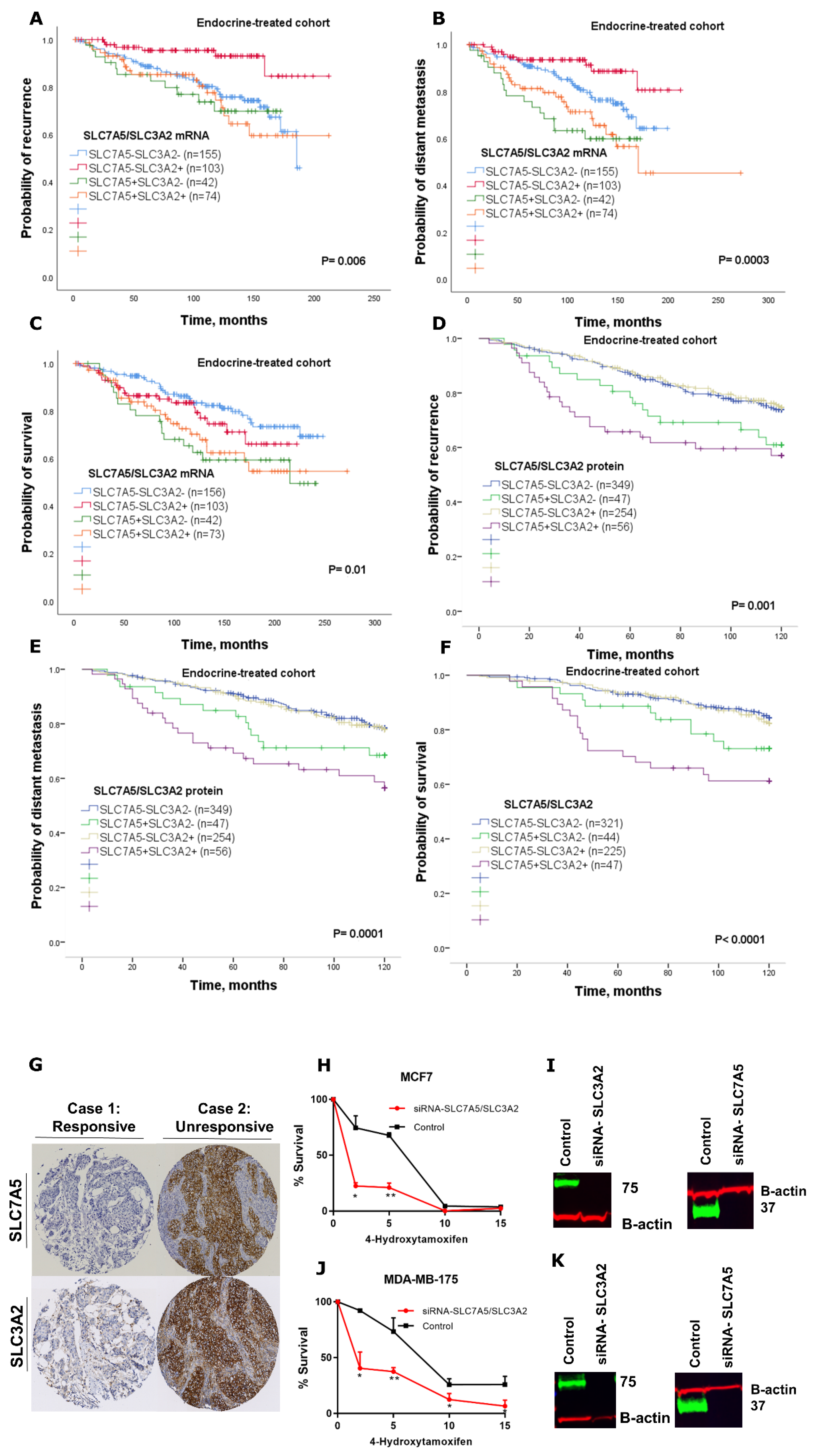
2.4. Predictive Value of SLC7A5/SLC3A2 Co-Expression for Endocrine Treatment Benefit
3. Discussion
4. Materials and Methods
4.1. Patients mRNA Expression Cohort
4.2. Patients Protein Expression Cohort
4.3. IHC Staining and Evaluation
4.4. Clinical Outcome and Events Definition
4.5. Cell Lines and Reagents
4.6. Transient siRNA Knockdown of SLC7A5 and SLC3A2
4.7. Proliferation Assay
4.8. Tamoxifen Sensitivity Assay
4.9. Western Blotting
4.10. Patient Data Analysis and Statistics
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| ER+ | Oestrogen Receptor Positive |
| NPI | Nottingham Prognostic Index |
| IHC | Immunohistochemistry |
| METABRIC | Molecular Taxonomy of Breast Cancer International Consortium |
| H-score | Histochemical score |
References
- Alfarsi, L.; Johnston, S.; Liu, D.X.; Rakha, E.; Green, A. Current issues with luminal subtype classification in terms of prediction of benefit from endocrine therapy in early breast cancer. Histopathology 2018, 73, 545–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Ansari, R.; McIntyre, A.; Craze, M.L.; Ellis, I.O.; Rakha, E.A.; Green, A.R. Altered glutamine metabolism in breast cancer; subtype dependencies and alternative adaptations. Histopathology 2018, 72, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Kandasamy, P.; Gyimesi, G.; Kanai, Y.; Hediger, M.A. Amino acid transporters revisited: New views in health and disease. Trends Biochem. Sci. 2018, 43, 752–789. [Google Scholar] [CrossRef] [PubMed]
- Yanagida, O.; Kanai, Y.; Chairoungdua, A.; Kim, D.K.; Segawa, H.; Nii, T.; Cha, S.H.; Matsuo, H.; Fukushima, J.; Fukasawa, Y.; et al. Human L-type amino acid transporter 1 (LAT1): Characterization of function and expression in tumor cell lines. Biochim. Biophys. Acta 2001, 1514, 291–302. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, E.; Sato, M.; Yang, H.; Miyagawa, F.; Harasaki, M.; Tomita, K.; Matsuoka, S.; Noma, A.; Iwai, K.; Minato, N. 4F2 (CD98) heavy chain is associated covalently with an amino acid transporter and controls intracellular trafficking and membrane topology of 4F2 heterodimer. J. Biol. Chem. 1999, 274, 3009–3016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulter, E.; Estrach, S.; Tissot, F.S.; Hennrich, M.L.; Tosello, L.; Cailleteau, L.; de la Ballina, L.R.; Pisano, S.; Gavin, A.-C.; Féral, C.C. Cell metabolism regulates integrin mechanosensing via an SLC3A2-dependent sphingolipid biosynthesis pathway. Nat. Commun. 2018, 9, 4862. [Google Scholar] [CrossRef]
- Prager, G.W.; Feral, C.C.; Kim, C.; Han, J.; Ginsberg, M.H. CD98hc (SLC3A2) interaction with the integrin beta subunit cytoplasmic domain mediates adhesive signaling. J. Biol. Chem. 2007, 282, 24477–24484. [Google Scholar] [CrossRef] [Green Version]
- Yan, R.; Zhao, X.; Lei, J.; Zhou, Q. Structure of the human LAT1–4F2hc heteromeric amino acid transporter complex. Nature 2019, 568, 127–130. [Google Scholar] [CrossRef]
- Mastroberardino, L.; Spindler, B.; Pfeiffer, R.; Skelly, P.J.; Loffing, J.; Shoemaker, C.B.; Verrey, F. Amino-acid transport by heterodimers of 4F2hc/CD98 and members of a permease family. Nature 1998, 395, 288–291. [Google Scholar] [CrossRef]
- Nicklin, P.; Bergman, P.; Zhang, B.; Triantafellow, E.; Wang, H.; Nyfeler, B.; Yang, H.; Hild, M.; Kung, C.; Wilson, C.; et al. Bidirectional transport of amino acids regulates mTOR and autophagy. Cell 2009, 136, 521–534. [Google Scholar] [CrossRef] [Green Version]
- El Ansari, R.; Craze, M.L.; Miligy, I.; Diez-Rodriguez, M.; Nolan, C.C.; Ellis, I.O.; Rakha, E.A.; Green, A.R. The amino acid transporter SLC7A5 confers a poor prognosis in the highly proliferative breast cancer subtypes and is a key therapeutic target in luminal B tumours. Breast Cancer Res. 2018, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- El Ansari, R.; Craze, M.L.; Diez-Rodriguez, M.; Nolan, C.C.; Ellis, I.O.; Rakha, E.A.; Green, A.R. The multifunctional solute carrier 3A2 (SLC3A2) confers a poor prognosis in the highly proliferative breast cancer subtypes. Br. J. Cancer 2018, 118, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Shishido, T.; Uno, S.; Kamohara, M.; Tsuneoka-Suzuki, T.; Hashimoto, Y.; Enomoto, T.; Masuko, T. Transformation of BALB3T3 cells caused by over-expression of rat CD98 heavy chain (HC) requires its association with light chain: Mis-sense mutation in a cysteine residue of CD98HC eliminates its transforming activity. Int. J. Cancer 2000, 87, 311–316. [Google Scholar] [CrossRef]
- Elorza, A.; Soro-Arnaiz, I.; Melendez-Rodriguez, F.; Rodriguez-Vaello, V.; Marsboom, G.; de Carcer, G.; Acosta-Iborra, B.; Albacete-Albacete, L.; Ordonez, A.; Serrano-Oviedo, L.; et al. HIF2alpha acts as an mTORC1 activator through the amino acid carrier SLC7A5. Mol. Cell 2012, 48, 681–691. [Google Scholar] [CrossRef] [Green Version]
- Sakata, T.; Ferdous, G.; Tsuruta, T.; Satoh, T.; Baba, S.; Muto, T.; Ueno, A.; Kanai, Y.; Endou, H.; Okayasu, I. L-type amino-acid transporter 1 as a novel biomarker for high-grade malignancy in prostate cancer. Pathol. Int. 2009, 59, 7–18. [Google Scholar] [CrossRef]
- Kaira, K.; Oriuchi, N.; Imai, H.; Shimizu, K.; Yanagitani, N.; Sunaga, N.; Hisada, T.; Tanaka, S.; Ishizuka, T.; Kanai, Y.; et al. Prognostic significance of L-type amino acid transporter 1 expression in resectable stage I-III nonsmall cell lung cancer. Br. J. Cancer 2008, 98, 742–748. [Google Scholar] [CrossRef]
- Haining, Z.; Kawai, N.; Miyake, K.; Okada, M.; Okubo, S.; Zhang, X.; Fei, Z.; Tamiya, T. Relation of LAT1/4F2hc expression with pathological grade, proliferation and angiogenesis in human gliomas. BMC Clin. Pathol. 2012, 12, 4. [Google Scholar] [CrossRef] [Green Version]
- Betsunoh, H.; Fukuda, T.; Anzai, N.; Nishihara, D.; Mizuno, T.; Yuki, H.; Masuda, A.; Yamaguchi, Y.; Abe, H.; Yashi, M.; et al. Increased expression of system large amino acid transporter (LAT)-1 mRNA is associated with invasive potential and unfavorable prognosis of human clear cell renal cell carcinoma. BMC Cancer 2013, 13, 509. [Google Scholar] [CrossRef] [Green Version]
- Jewell, J.L.; Kim, Y.C.; Russell, R.C.; Yu, F.X.; Park, H.W.; Plouffe, S.W.; Tagliabracci, V.S.; Guan, K.L. Metabolism. Differential regulation of mTORC1 by leucine and glutamine. Science 2015, 347, 194–198. [Google Scholar] [CrossRef] [Green Version]
- Kimball, S.R. Regulation of translation initiation by amino acids in eukaryotic cells. Prog. Mol. Subcell. Biol. 2001, 26, 155–184. [Google Scholar]
- Furuya, M.; Horiguchi, J.; Nakajima, H.; Kanai, Y.; Oyama, T. Correlation of L-type amino acid transporter 1 and CD98 expression with triple negative breast cancer prognosis. Cancer Sci. 2012, 103, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, M.L.; George, L.K.; Grant, G.D.; Perou, C.M. Common markers of proliferation. Nat. Rev. Cancer 2006, 6, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Curtis, C.; Shah, S.P.; Chin, S.F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The genomic and transcriptomic architecture of 2,000 breast tumours reveals novel subgroups. Nature 2012, 486, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Sauerbrei, W.; Taube, S.E.; McShane, L.M.; Cavenagh, M.M.; Altman, D.G. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): An Abridged Explanation and Elaboration. J. Natl. Cancer Inst. 2018, 110, 803–811. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| METABRIC Cohort | SLC7A5/SLC3A2 mRNA | |||||
|---|---|---|---|---|---|---|
| Parameters | SLC7A5− | SLC7A5+ | SLC7A5− | SLC7A5+ | p | p * |
| SLC3A2− | SLC3A2− | SLC3A2+ | SLC3A2+ | |||
| No. (%) | No. (%) | No. (%) | No. (%) | |||
| Size | 0.039 | 0.06 | ||||
| <2 cm | 67 (72.8) | 9 (9.8) | 9 (9.8) | 7 (7.6) | ||
| ≥2 cm | 48 (52.7) | 17 (18.7) | 12 (13.2) | 14 (15.4) | ||
| Grade | 3.8 × 10−12 | <0.0001 | ||||
| 1 | 52 (67.5) | 2 (2.6) | 17 (22.1) | 6 (7.8) | ||
| 2 | 132 (51.8) | 20 (7.8) | 78 (30.6) | 28 (9.8) | ||
| 3 | 59 (28.5) | 23 (11.1) | 60 (29) | 65 (31.4) | ||
| Nodal Stage | 0.2 | 0.23 | ||||
| 1 | 77 (67.5) | 13 (11.4) | 14 (12.3) | 10 (8.8) | ||
| 2 | 34 (59.6) | 10 (17.5) | 4 (7) | 9 (15.8) | ||
| 3 | 4 (36.4) | 2 (18.2) | 3 (27.3) | 2 (18.2) | ||
| NPI | 8.3 × 10−8 | <0.0001 | ||||
| GPG | 111 (55.8) | 11 (5.5) | 63 (31.7) | 14 (7) | ||
| MPG | 121 (42.3) | 23 (8) | 79 (27.6) | 63 (22) | ||
| PPG | 15 (22.4) | 12 (17.9) | 21 (31.3) | 19 (28.4) | ||
| Vascular invasion | 0.01 | 0.02 | ||||
| Negative | 82 (71.3) | 12 (10.4) | 12 (10.4) | 9 (7.8) | ||
| Definite | 33 (48.5) | 14 (20.6) | 9 (13.2) | 12 (17.6) | ||
| PR | 0.1 | 0.14 | ||||
| Negative | 60 (40.5) | 8 (5.4) | 48 (32.4) | 32 (21.6) | ||
| Positive | 184 (45.9) | 38 (9.5) | 115 (28.7) | 64 (16) | ||
| Nottingham Cohort | SLC7A5/SLC3A2 protein | |||||
| Size | 0.002 | 0.003 | ||||
| <2 cm | 432 (54.8) | 27 (3.4) | 288 (36.5) | 42 (5.3) | ||
| ≥2 cm | 266 (48.6) | 37 (6.8) | 197 (36) | 47 (8.6) | ||
| Grade | 2.6 × 10−35 | <0.0001 | ||||
| 1 | 184 (65.2) | 0 (0) | 96 (34) | 2 (0.8) | ||
| 2 | 356 (56) | 20 (3.1) | 245 (38.5) | 15 (2.4) | ||
| 3 | 158 (37.9) | 44 (10.6) | 144 (34.5) | 71 (17) | ||
| Mitosis | 1.1 × 10−32 | <0.0001 | ||||
| 1 | 436 (59.4) | 10 (1.4) | 279 (38) | 9 (1.2) | ||
| 2 | 133 (49.8) | 21 (7.9) | 90 (33.7) | 23 (8.6) | ||
| 3 | 109 (35.5) | 32 (10.4) | 110 (35.8) | 56 (18.2) | ||
| Nodal Stage | 0.136 | 0.15 | ||||
| 1 | 450 (52.7) | 34 (4) | 316 (37) | 54 (6.3) | ||
| 2 | 204 (52.7) | 20 (5.2) | 137 (35.4) | 26 (6.7) | ||
| 3 | 44 (47.3) | 10 (10.8) | 31 (33.3) | 8 (8.6) | ||
| NPI | 1.1 × 10−16 | <0.0001 | ||||
| GPG | 339 (60) | 9 (1.6) | 209 (37) | 8 (1.4) | ||
| MPG | 297 (49) | 36 (5.9) | 214 (35.3) | 59 (9.7) | ||
| PPG | 62 (38) | 19 (11.7) | 60 (36.8) | 22 (13.5) | ||
| Vascular invasion | 0.0004 | 0.0009 | ||||
| Negative | 500 (54.6) | 30 (3.3) | 329 (35.9) | 57 (6.2) | ||
| Definite | 197 (47.1) | 34 (8.1) | 156 (37.3) | 31 (7.4) | ||
| PR | 0.116 | 0.13 | ||||
| Negative | 147 (47.7) | 20 (6.5) | 115 (37.3) | 26 (8.4) | ||
| Positive | 548 (53.7) | 44 (4.3) | 366 (35.8) | 63 (6.2) | ||
| SLC7A5−SLC3A2− vs | Outcome | Hazard Ratio | 95% Confidence Interval | p | p * |
|---|---|---|---|---|---|
| SLC7A5+SLC3A2− | Recurrence | 1.3 | 0.8–2.0 | 0.239 | 0.4 |
| Distant metastasis | 1.4 | 0.8–2.4 | 0.147 | 0.2 | |
| Survival | 1.6 | 0.9–3.0 | 0.106 | 0.2 | |
| SLC7A5−SLC3A2+ | Recurrence | 0.9 | 0.7–1.2 | 0.720 | 0.9 |
| Distant metastasis | 1.0 | 0.7–1.3 | 0.821 | 1.0 | |
| Survival | 1.1 | 0.8–1.6 | 0.289 | 0.3 | |
| SLC7A5+SLC3A2+ | Recurrence | 1.7 | 1.2–2.5 | 0.002 | 0.008 |
| Distant metastasis | 2.4 | 1.6–3.5 | 0.000004 | <0.0001 | |
| Survival | 3.2 | 2.0–4.9 | 1.0 × 10−7 | <0.0001 |
| mRNA Expression | |||
| Recurrence-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 2.0 (1.1–3.7) | 0.01 | 0.05 |
| Tumour size | 1.2 (0.8–2.0) | 0.2 | 0.3 |
| Tumour grade | 1.3 (0.9–1.9) | 0.09 | 0.2 |
| Nodal stage | 1.1 (0.7–1.5) | 0.6 | 0.7 |
| Distant metastasis-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 2.1 (1.1–3.9) | 0.01 | 0.05 |
| Tumour size | 1.8 (1.0–3.1) | 0.02 | 0.05 |
| Tumour grade | 1.5 (1.0–2.2) | 0.03 | 0.5 |
| Nodal stage | 1.3 (0.9–1.9) | 0.1 | 0.12 |
| Breast-cancer-specific survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 2.2 (1.1–4.3) | 0.02 | 0.05 |
| Tumour size | 1.8 (1.0–3.2) | 0.04 | 0.06 |
| Tumour grade | 2.0 (1.2–3.2) | 0.002 | 0.01 |
| Nodal stage | 1.3 (0.8–2.0) | 0.1 | 0.12 |
| Protein expression | |||
| Recurrence-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 1.5 (1.0–2.4) | 0.2 | 0.25 |
| Tumour size | 1.5 (1.1–2.0) | 0.006 | 0.01 |
| Tumour grade | 1.4 (1.1–1.8) | 0.001 | 0.002 |
| Nodal stage | 1.6 (1.3–1.9) | 0.000008 | <0.0001 |
| Distant metastasis-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 1.5 (1.0–2.3) | 0.03 | 0.037 |
| Tumour size | 1.6 (1.1–2.3) | 0.004 | 0.006 |
| Tumour grade | 1.7 (1.3–2.3) | 0.00001 | <0.0001 |
| Nodal stage | 1.8 (1.4–2.2) | 3.5 × 10−7 | <0.0001 |
| Breast-cancer-specific survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 1.7 (1.0–2.7) | 0.02 | 0.03 |
| Tumour size | 1.3 (0.8–2.0) | 0.16 | 0.2 |
| Tumour grade | 2.3 (1.7–3.3) | 3.7 × 10−7 | <0.0001 |
| Nodal stage | 1.8 (1.3–2.3) | 0.00002 | 0.0001 |
| mRNA Expression | |||
| Recurrence-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 1.7 (1.0–2.8) | 0.02 | 0.03 |
| Tumour size | 1.3 (0.8–2.0) | 0.17 | 0.2 |
| Tumour grade | 2.1 (1.4–3.0) | 0.00004 | 0.0001 |
| Nodal stage | 1.9 (1.4–2.5) | 0.000003 | <0.0001 |
| Distant metastasis-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 1.9 (1.1–3.2) | 0.008 | 0.01 |
| Tumour size | 1.2 (0.8–2.0) | 0.2 | 0.25 |
| Tumour grade | 2.6 (1.7–4.0) | 0.000002 | <0.0001 |
| Nodal stage | 2.1 (1.6–2.9) | 4.7 × 10−7 | <0.0001 |
| Breast-cancer-specific survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 2.0 (1.1–3.6) | 0.01 | 0.016 |
| Tumour size | 0.9 (0.5–1.6) | 0.8 | 1 |
| Tumour grade | 3.6 (2.1–6.2) | 0.000002 | <0.0001 |
| Nodal stage | 2.1 (1.5–3.0) | 0.00002 | 0.0001 |
| Protein Expression | |||
| Recurrence-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 1.7 (1.0–2.8) | 0.02 | 0.03 |
| Tumour size | 1.3 (0.8–2.0) | 0.17 | 0.2 |
| Tumour grade | 2.1 (1.4–3.0) | 0.00004 | 0.0001 |
| Nodal stage | 1.9 (1.4–2.5) | 0.000003 | <0.0001 |
| Distant metastasis-free survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 1.9 (1.1–3.2) | 0.008 | 0.01 |
| Tumour size | 1.2 (0.8–2.0) | 0.2 | 0.25 |
| Tumour grade | 2.6 (1.7–4.0) | 0.000002 | <0.0001 |
| Nodal stage | 2.1 (1.6–2.9) | 4.7 × 10−7 | <0.0001 |
| Breast-cancer-specific survival | |||
| HR (95% CI) | p | p * | |
| SLC7A5−SLC3A2− vs. SLC7A5+SLC3A2+ | 2.0 (1.1–3.6) | 0.01 | 0.016 |
| Tumour size | 0.9 (0.5–1.6) | 0.8 | 1 |
| Tumour grade | 3.6 (2.1–6.2) | 0.000002 | <0.0001 |
| Nodal stage | 2.1 (1.5–3.0) | 0.00002 | 0.0001 |
| Parameters | METABRIC Cohort | Nottingham Cohort |
|---|---|---|
| mRNA | Protein | |
| No. (%) | No. (%) | |
| Age | ||
| <50 | 228 (15) | 370 (27.7) |
| ≥50 | 1278 (85) | 967 (72.3) |
| Tumour size (cm) | ||
| <2 cm | 475 (31.5) | 789 (59.1) |
| ≥2 cm | 1031 (68.5) | 547 (40.9) |
| Grade | ||
| 1 | 166 (11.5) | 110 (8.4) |
| 2 | 707 (49.1) | 493 (37.6) |
| 3 | 565 (38.4) | 707 (54.0) |
| Nottingham Prognostic Index | ||
| GPG | 623 (41.3) | 565 (42.4) |
| MPG | 772 (51.2) | 606 (45.4) |
| PPG | 111 (7.5) | 163 (12.2) |
| Nodal stage | ||
| 1 | 404 (36.2) | 854 (64.0) |
| 2 | 634 (56.8) | 387 (29.0) |
| 3 | 78 (7) | 93 (7.0) |
| Mitosis | ||
| 1 | 734 (56.1) | |
| 2 | N/A | 267 (20.4) |
| 3 | 307 (23.5) | |
| Vascular invasion | ||
| Negative | 115 (62.8) | 916 (68.5) |
| Positive | 68 (37.2) | 418 (31.2) |
| Endocrine therapy alone | ||
| No | 234 (15.5) | 505 (37.7) |
| Yes | 384 (25.5) | 716 (53.5) |
| Other * | 888 (59) | 117 (8.8) |
| Progesterone receptor | ||
| Negative | 486 (23.2) | 308 (23.2) |
| Positive | 1020 (76.8) | 1021 (76.8) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alfarsi, L.H.; El-Ansari, R.; Craze, M.L.; Masisi, B.K.; Mohammed, O.J.; Ellis, I.O.; Rakha, E.A.; Green, A.R. Co-Expression Effect of SLC7A5/SLC3A2 to Predict Response to Endocrine Therapy in Oestrogen-Receptor-Positive Breast Cancer. Int. J. Mol. Sci. 2020, 21, 1407. https://doi.org/10.3390/ijms21041407
Alfarsi LH, El-Ansari R, Craze ML, Masisi BK, Mohammed OJ, Ellis IO, Rakha EA, Green AR. Co-Expression Effect of SLC7A5/SLC3A2 to Predict Response to Endocrine Therapy in Oestrogen-Receptor-Positive Breast Cancer. International Journal of Molecular Sciences. 2020; 21(4):1407. https://doi.org/10.3390/ijms21041407
Chicago/Turabian StyleAlfarsi, Lutfi H., Rokaya El-Ansari, Madeleine L. Craze, Brendah K. Masisi, Omar J. Mohammed, Ian O. Ellis, Emad A. Rakha, and Andrew R. Green. 2020. "Co-Expression Effect of SLC7A5/SLC3A2 to Predict Response to Endocrine Therapy in Oestrogen-Receptor-Positive Breast Cancer" International Journal of Molecular Sciences 21, no. 4: 1407. https://doi.org/10.3390/ijms21041407
APA StyleAlfarsi, L. H., El-Ansari, R., Craze, M. L., Masisi, B. K., Mohammed, O. J., Ellis, I. O., Rakha, E. A., & Green, A. R. (2020). Co-Expression Effect of SLC7A5/SLC3A2 to Predict Response to Endocrine Therapy in Oestrogen-Receptor-Positive Breast Cancer. International Journal of Molecular Sciences, 21(4), 1407. https://doi.org/10.3390/ijms21041407