
Bone Tissue Response to Different Grown Crystal Batches of Octacalcium Phosphate in Rat Long Bone Intramedullary Canal Area



Abstract
:1. Introduction
2. Results
2.1. Crystal Morphology of F-OCP and C-OCP
2.2. Change of Crystal Structure of OCPs after Immersion in the Tris-HCl Buffer
2.3. Alteration of the DS in the Tris-HCl Buffer after Immersion of OCPs
2.4. Change of Crystal Structure of OCPs in Rat Abdominal Subcutaneous Pouches
2.5. Micro-CT Analysis of Rat Tibia Defects Implanted with Various Crystal Size of OCPs
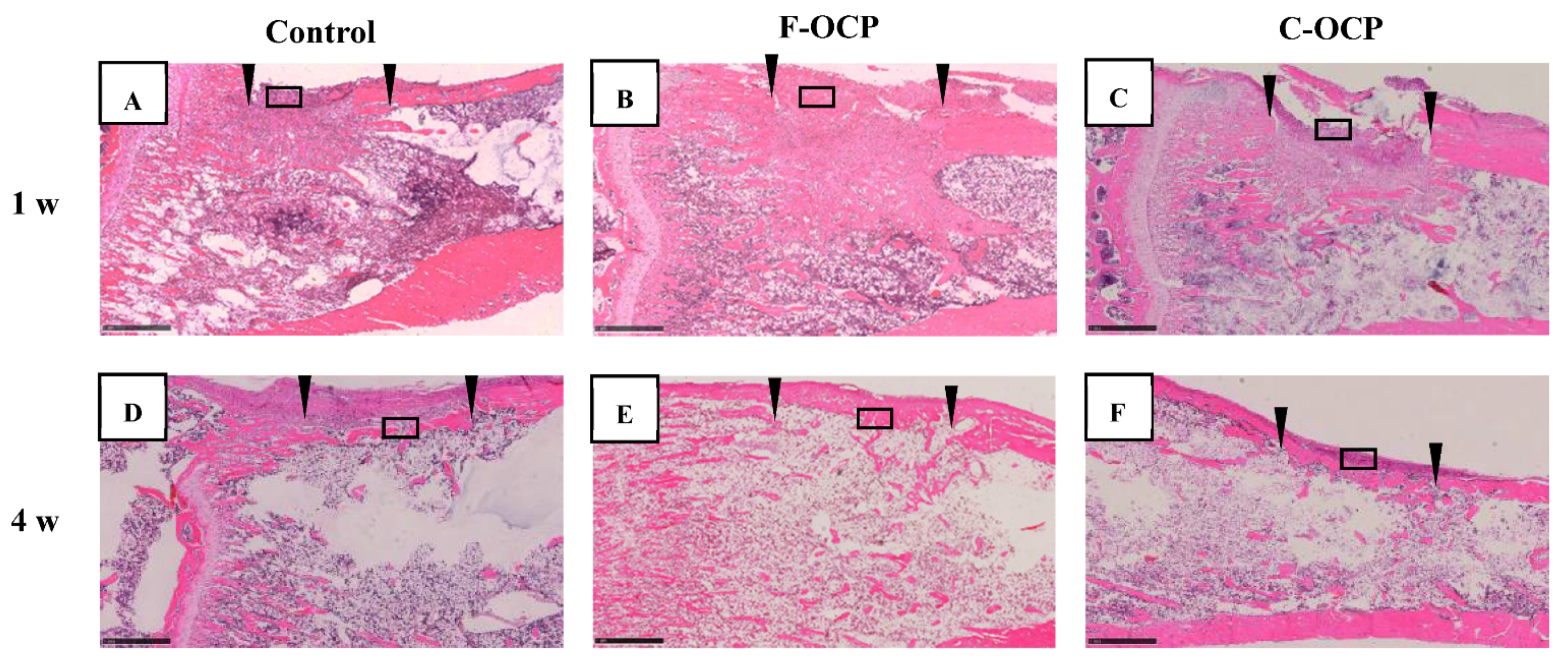
2.6. Histological and Histomorphometric Examinations
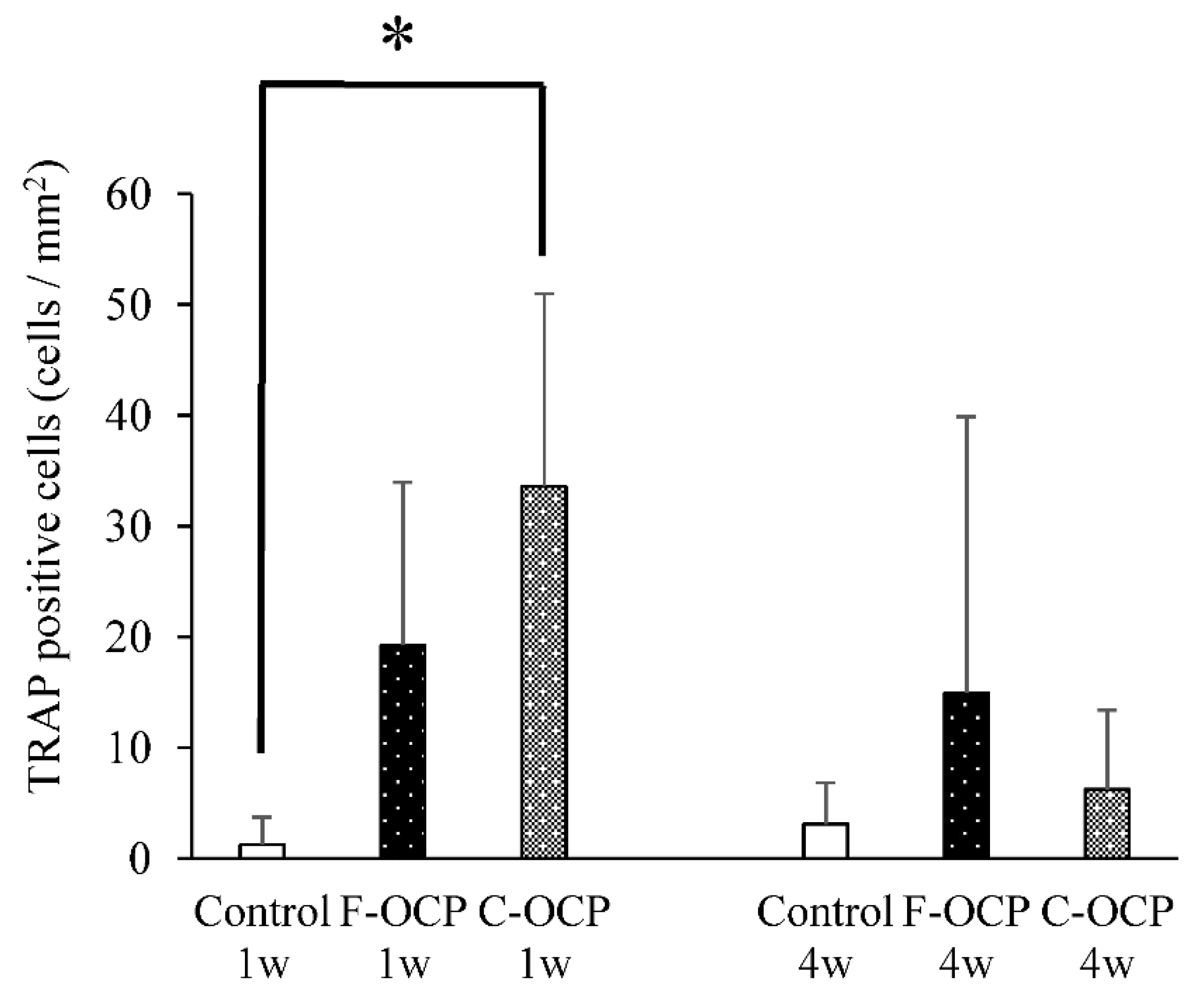
2.7. TRAP Staining
3. Discussion
4. Materials and Methods
4.1. Preparation of Various Crystal Sizes of OCPs
4.2. Characterization of OCPs and Supernatants after the Immersion in the Tris-HCl Buffer
4.3. Implantation of OCPs into Rat Tibia Defects or Subcutaneous Tissue
4.4. Characterization of OCPs Collected after Implantation of Rat Abdominal Regions
4.5. Determination of the DS in the Tris-HCl Buffer Immersed with F-OCP, C-OCP and Nano-OCP
4.6. Micro-CT Analysis
4.7. Tissue Preparation and Histomorphometric Analysis
4.8. Tartrate-Resistant Acid Phosphatase (TRAP) Staining
4.9. Imaging Techniques
4.10. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chou, L.; Marek, B.; Wagner, W.R. Effects of hydroxylapatite coating crystallinity on biosolubility, cell attachment efficiency and proliferation in vitro. Biomaterials 1999, 20, 977–985. [Google Scholar] [CrossRef]
- Murakami, Y.; Honda, Y.; Anada, T.; Shimauchi, H.; Suzuki, O. Comparative study on bone regeneration by synthetic octacalcium phosphate with various granule sizes. Acta Biomater. 2010, 6, 1542–1548. [Google Scholar] [CrossRef] [PubMed]
- Honda, Y.; Anada, T.; Kamakura, S.; Morimoto, S.; Kuriyagawa, T.; Suzuki, O. The effect of microstructure of octacalcium phosphate on the bone regenerative property. Tissue Eng. Part A 2009, 15, 1965–1973. [Google Scholar] [CrossRef] [PubMed]
- Li, X.M.; van Blitterswijk, C.A.; Feng, Q.L.; Cui, F.Z.; Watari, F.M. The effect of calcium phosphate microstructure on bone-related cells in vitro. Biomaterials 2008, 29, 3306–3316. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.D.; Zhang, H.J.; Fan, H.S.; Li, W.; Zhang, X.D. Effect of phase composition and microstructure of calcium phosphate ceramic particles on protein adsorption. Acta Biomater. 2010, 6, 1536–1541. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.W.; Luo, X.M.; Barbieri, D.; Barradas, A.M.C.; de Bruijn, J.D.; Van Blitterswijk, C.A.; Yuan, H.P. The size of surface microstructures as an osteogenic factor in calcium phosphate ceramics. Acta Biomater. 2014, 10, 3254–3263. [Google Scholar] [CrossRef] [PubMed]
- Davison, N.L.; Su, J.; Yuan, H.; van den Beucken, J.; de Bruijn, J.D.; Groot, F.B.D. Influence of surface microstructure and chemistry on osteoinduction and osteoclastogenesis by biphasic calcium phosphate discs. Eur. Cell. Mater. 2015, 29, 314–329. [Google Scholar] [CrossRef]
- Thamma, U.; Kowal, T.J.; Falk, M.M.; Jain, H. Nanostructure of bioactive glass affects bone cell attachment via protein restructuring upon adsorption. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Suzuki, O. Octacalcium phosphate (OCP)-based bone substitute materials. Jpn. Dent. Sci. Rev. 2013, 49, 58–71. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, O.; Shiwaku, Y.; Hamai, R. Octacalcium phosphate bone substitute materials: Comparison between properties of biomaterials and other calcium phosphate materials. Dent. Mater. J. 2020, 39, 187–199. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, O.; Kamakura, S.; Katagiri, T.; Nakamura, M.; Zhao, B.H.; Honda, Y.; Kamijo, R. Bone formation enhanced by implanted octacalcium phosphate involving conversion into Ca-deficient hydroxyapatite. Biomaterials 2006, 27, 2671–2681. [Google Scholar] [CrossRef]
- Anada, T.; Kumagai, T.; Honda, Y.; Masuda, T.; Kamijo, R.; Kamakura, S.; Yoshihara, N.; Kuriyagawa, T.; Shimauchi, H.; Suzuki, O. Dose-dependent osteogenic effect of octacalcium phosphate on mouse bone marrow stromal cells. Tissue Eng. Part A 2008, 14, 965–978. [Google Scholar] [CrossRef]
- Sai, Y.; Shiwaku, Y.; Anada, T.; Tsuchiya, K.; Takahashi, T.; Suzuki, O. Capacity of octacalcium phosphate to promote osteoblastic differentiation toward osteocytes in vitro. Acta Biomater. 2018, 69, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Hamai, R.; Shiwaku, Y.; Hasegawa, T.; Sakai, S.; Tsuchiya, K.; Sai, Y.; Iwama, R.; Amizuka, N.; Takahashi, T.; et al. Involvement of distant octacalcium phosphate scaffolds in enhancing early differentiation of osteocytes during bone regeneration. Acta Biomater. 2021, 129, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Anada, T.; Handa, T.; Kanda, N.; Yoshinari, M.; Takahashi, T.; Suzuki, O. Osteoconductive property of a mechanical mixture of octacalcium phosphate and amorphous calcium phosphate. ACS Appl. Mater. Interfaces 2014, 6, 22602–22611. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, B.; Anada, T.; Shiwaku, Y.; Miyatake, N.; Tsuchiya, K.; Nakamura, M.; Takahashi, T.; Suzuki, O. Immune cell response and subsequent bone formation induced by implantation of octacalcium phosphate in a rat tibia defect. RSC Adv. 2016, 6, S7475–S7484. [Google Scholar] [CrossRef]
- Takami, M.; Mochizuki, A.; Yamada, A.; Tachi, K.; Zhao, B.; Miyamoto, Y.; Anada, T.; Honda, Y.; Inoue, T.; Nakamura, M.; et al. Osteoclast differentiation induced by synthetic octacalcium phosphate through receptor activator of NF-κB ligand expression in osteoblasts. Tissue Eng. Part A 2009, 15, 3991–4000. [Google Scholar] [CrossRef]
- Shiwaku, Y.; Tsuchiya, K.; Xiao, L.; Suzuki, O. Effect of calcium phosphate phases affecting the crosstalk between osteoblasts and osteoclasts in vitro. J. Biomed. Mater. Res. A 2019, 107A, 1001–1013. [Google Scholar] [CrossRef]
- Miyatake, N.; Kishimoto, K.N.; Anada, T.; Imaizumi, H.; Itoi, E.; Suzuki, O. Effect of partial hydrolysis of octacalcium phosphate on its osteoconductive characteristics. Biomaterials 2009, 30, 1005–1014. [Google Scholar] [CrossRef]
- Baba, K.; Shiwaku, Y.; Hamai, R.; Mori, Y.; Anada, T.; Tsuchiya, K.; Oizumi, I.; Miyatake, N.; Itoi, E.; Suzuki, O. Chemical stability-sensitive osteoconductive performance of octacalcium phosphate bone substitute in an ovariectomized rat tibia defect. ACS Appl. Bio Mater. 2020, 3, 1444–1458. [Google Scholar] [CrossRef]
- Oizumi, I.; Hamai, R.; Shiwaku, Y.; Mori, Y.; Anada, T.; Baba, K.; Miyatake, N.; Hamada, S.; Tsuchiya, K.; Nishimura, S.; et al. Impact of simultaneous hydrolysis of OCP and PLGA on bone induction of a PLGA-OCP composite scaffold in a rat femoral defect. Acta Biomater. 2021, 124, 358–373. [Google Scholar] [CrossRef]
- Dwek, J.R. The periosteum: What is it, where is it, and what mimics it in its absence? Skelet. Radiol. 2010, 39, 319–323. [Google Scholar] [CrossRef] [Green Version]
- Scotti, C.; Piccinini, E.; Takizawa, H.; Todorov, A.; Bourgine, P.; Papadimitropoulos, A.; Barbero, A.; Manz, M.G.; Martin, I. Engineering of a functional bone organ through endochondral ossification. Proc. Natl. Acad. Sci. USA 2013, 110, 3997–4002. [Google Scholar] [CrossRef] [Green Version]
- LeGeros, R.Z. Properties of osteoconductive biomaterials: Calcium phosphates. Clin. Orthop. Relat. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef]
- Okuda, T.; Ioku, K.; Yonezawa, I.; Minagi, H.; Kawachi, G.; Gonda, Y.; Murayama, H.; Shibata, Y.; Minami, S.; Kamihira, S.; et al. The effect of the microstructure of β-tricalcium phosphate on the metabolism of subsequently formed bone tissue. Biomaterials 2007, 28, 2612–2621. [Google Scholar] [CrossRef] [PubMed]
- Okuda, T.; Ioku, K.; Yonezawa, I.; Minagi, H.; Gonda, Y.; Kawachi, G.; Kamitakahara, M.; Shibata, Y.; Murayama, H.; Kurosawa, H.; et al. The slow resorption with replacement by bone of a hydrothermally synthesized pure calcium-deficient hydroxyapatite. Biomaterials 2008, 29, 2719–2728. [Google Scholar] [CrossRef] [PubMed]
- Bonfield, W. Designing porous scaffolds for tissue engineering. Philos. Trans. A Math. Phys. Eng. Sci. 2006, 364, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.R.; Lee, P.D.; Hench, L.L. Hierarchical porous materials for tissue engineering. Philos. Trans. A Math. Phys. Eng. Sci. 2006, 364, 263–281. [Google Scholar] [CrossRef] [PubMed]
- Tamai, N.; Myoui, A.; Tomita, T.; Nakase, T.; Tanaka, J.; Ochi, T.; Yoshikawa, H. Novel hydroxyapatite ceramics with an interconnective porous structure exhibit superior osteoconduction in vivo. J. Biomed. Mater. Res. 2002, 59, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Isaac, J.; Hornez, J.C.; Jian, D.; Descamps, M.; Hardouin, P.; Magne, D. β-TCP microporosity decreases the viability and osteoblast differentiation of human bone marrow stromal cells. J. Biomed. Mater. Res. A 2008, 86A, 386–393. [Google Scholar] [CrossRef]
- Liu, Y.; Shelton, R.M.; Gbureck, U.; Barralet, J.E. Influence of calcium phosphate crystal morphology on the adhesion, spreading, and growth of bone derived cells. J. Biomed. Mater. Res. A 2009, 90A, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.T.; Klein, T.; Murray, R.Z.; Crawford, R.; Chang, J.; Wu, C.T.; Xiao, Y. Osteoimmunomodulation for the development of advanced bone biomaterials. Mater. Today 2016, 19, 304–321. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, O.; Nakamura, M.; Miyasaka, Y.; Kagayama, M.; Sakurai, M. Bone formation on synthetic precursors of hydroxyapatite. Tohoku J. Exp. Med. 1991, 164, 37–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miura, K.; Anada, T.; Honda, Y.; Shiwaku, Y.; Kawai, T.; Echigo, S.; Takahashi, T.; Suzuki, O. Characterization and bioactivity of nano-submicro octacalcium phosphate/gelatin composite. Appl. Surf. Sci. 2013, 282, 138–145. [Google Scholar] [CrossRef]
- Aoba, T.; Fukae, M.; Tanabe, T.; Shimizu, M.; Moreno, E.C. Selective adsorption of porcine-amelogenins onto hydroxyapatite and their inhibitory activity on hydroxyapatite growth in supersaturated solutions. Calcif. Tissue Int. 1987, 41, 281–289. [Google Scholar] [CrossRef]
- Moreno, E.C.; Aoba, T. Calcium bonding in enamel fluid and driving force for enamel mineralization in the secretory stage of amelogenesis. Adv. Dent. Res. 1987, 1, 245–251. [Google Scholar] [CrossRef]
- Moreno, E.C.; Aoba, T. Comparative solubility study of human dental enamel, dentin, and hydroxyapatite. Calcif. Tissue Int. 1991, 49, 6–13. [Google Scholar] [CrossRef]
- Moreno, E.C.; Kresak, M.; Zahradnik, R.T. Fluoridated hydroxyapatite solubility and caries formation. Nature 1974, 247, 64–65. [Google Scholar] [CrossRef]
- Tung, M.S.; Eidelman, N.; Sieck, B.; Brown, W.E. Octacalcium phosphate solubility product from 4 to 37 °C. J. Res. Natl. Bur. Stand. 1988, 93, 613–624. [Google Scholar] [CrossRef]
- Moreno, E.C.; Brown, W.E.; Osborn, G. Solubility of dicalcium phosphate dihydrate in aqueous systems. Soil. Sci. Soc. Am. J. 1960, 24, 94–98. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Periods (day) | Calcium (mM) | Phosphate (mM) | pH | DS at pH (Each) and 37 °C | |||
|---|---|---|---|---|---|---|---|
| HA | OCP | DCPD | |||||
| control | 7 | 0.056 | 0.010 | 7.470 | Not calc. | Not calc. | Not calc. |
| Nano-OCP | 7 | 0.331 | 1.610 | 7.475 | 7.781 × 108 | 9.406 × 10 | 1.763 × 10−1 |
| F-OCP | 7 | 0.363 | 1.576 | 7.486 | 1.298 × 109 | 1.359 × 101 | 1.900 × 10−1 |
| C-OCP | 7 | 0.642 | 0.669 | 7.522 | 2.807 × 109 | 1.367 × 101 | 1.475 × 10−1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiwaku, Y.; Hamai, R.; Sato, S.; Sakai, S.; Tsuchiya, K.; Baba, K.; Takahashi, T.; Suzuki, O. Bone Tissue Response to Different Grown Crystal Batches of Octacalcium Phosphate in Rat Long Bone Intramedullary Canal Area. Int. J. Mol. Sci. 2021, 22, 9770. https://doi.org/10.3390/ijms22189770
Shiwaku Y, Hamai R, Sato S, Sakai S, Tsuchiya K, Baba K, Takahashi T, Suzuki O. Bone Tissue Response to Different Grown Crystal Batches of Octacalcium Phosphate in Rat Long Bone Intramedullary Canal Area. International Journal of Molecular Sciences. 2021; 22(18):9770. https://doi.org/10.3390/ijms22189770
Chicago/Turabian StyleShiwaku, Yukari, Ryo Hamai, Shinichi Sato, Susumu Sakai, Kaori Tsuchiya, Kazuyoshi Baba, Tetsu Takahashi, and Osamu Suzuki. 2021. "Bone Tissue Response to Different Grown Crystal Batches of Octacalcium Phosphate in Rat Long Bone Intramedullary Canal Area" International Journal of Molecular Sciences 22, no. 18: 9770. https://doi.org/10.3390/ijms22189770
APA StyleShiwaku, Y., Hamai, R., Sato, S., Sakai, S., Tsuchiya, K., Baba, K., Takahashi, T., & Suzuki, O. (2021). Bone Tissue Response to Different Grown Crystal Batches of Octacalcium Phosphate in Rat Long Bone Intramedullary Canal Area. International Journal of Molecular Sciences, 22(18), 9770. https://doi.org/10.3390/ijms22189770