
Cumulative Effects of Strontium Ranelate and Impact Exercise on Bone Mass in Ovariectomized Rats

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Effects of Ovariectomy on Bone
2.2. BMD, BMC, and Body Composition
2.3. Trabecular Bone Microarchitecture
2.4. Cortical Bone Microarchitecture
2.5. Biomechanics
2.6. Bone Turnover
2.7. Osteocyte Apoptosis and Lipid Cells
3. Discussion
4. Materials and Methods
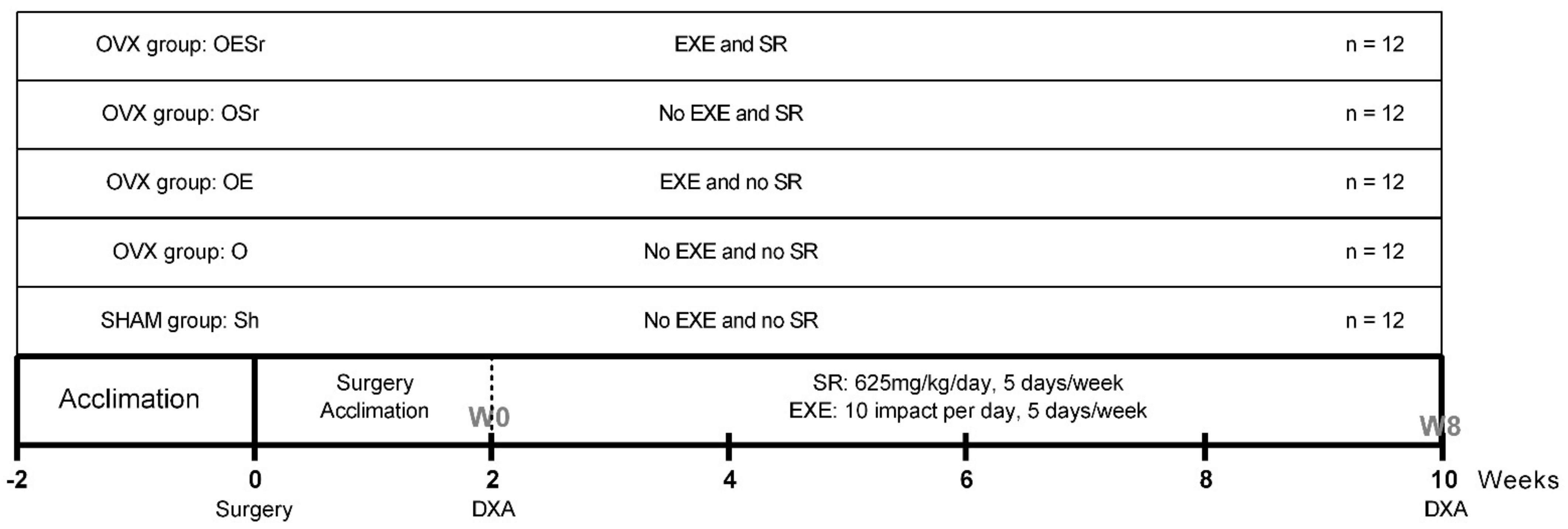
4.1. Animals and In Vivo Experimental Design
4.2. SR Administration
4.3. Exercise Protocol
4.4. Bone Densitometry Measurements
4.5. Morphological Characteristic of Trabecular Bone
4.6. Morphological Characteristic of Cortical Bone
4.7. Bone Mechanical Testing
4.8. Biochemical Analysis
4.9. Bone Immunostaining
4.9.1. Bone Preparation
4.9.2. Cleaved Caspase-3 Staining
4.9.3. Nile Red Staining
4.9.4. Image Acquisition
4.10. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ammann, P.; Shen, V.; Robin, B.; Mauras, Y.; Bonjour, J.-P.; Rizzoli, R. Strontium Ranelate Improves Bone Resistance by Increasing Bone Mass and Improving Architecture in Intact Female Rats. J. Bone Miner. Res. 2004, 19, 2012–2020. [Google Scholar] [CrossRef]
- Umemura, Y.; Ishiko, T.; Tsujimoto, H.; Miura, H.; Mokushi, N.; Suzuki, H. Effects of Jump Training on Bone Hypertrophy in Young and Old Rats. Int. J. Sports Med. 1995, 16, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Maurel, D.B.; Boisseau, N.; Ingrand, I.; Dolleans, E.; Benhamou, C.-L.; Jaffre, C. Combined effects of chronic alcohol consumption and physical activity on bone health: Study in a rat model. Eur. J. Appl. Physiol. 2011, 111, 2931–2940. [Google Scholar] [CrossRef]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Muller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef] [PubMed]
- Vatsa, A.; Semeins, C.; Smit, T.; Klein-Nulend, J. Paxillin localisation in osteocytes—Is it determined by the direction of loading? Biochem. Biophys. Res. Commun. 2008, 377, 1019–1024. [Google Scholar] [CrossRef]
- Maurel, D.; Jaffré, C.; Rochefort, G.Y.; Aveline, P.; Boisseau, N.; Uzbekov, R.; Gosset, D.; Pichon, C.; Fazzalari, N.; Pallu, S.; et al. Low bone accrual is associated with osteocyte apoptosis in alcohol-induced osteopenia. Bone 2011, 49, 543–552. [Google Scholar] [CrossRef]
- Fowler, S.D.; Greenspan, P. Application of Nile red, a fluorescent hydrophobic probe, for the detection of neutral lipid deposits in tissue sections: Comparison with oil red O. J. Histochem. Cytochem. 1985, 33, 833–836. [Google Scholar] [CrossRef]
- Lespessailles, E.; Prouteau, S. Is there a synergy between physical exercise and drug therapies for osteoporosis? Clin. Exp. Rheumatol. 2006, 24, 191–195. [Google Scholar]
- Benedetti, M.G.; Furlini, G.; Zati, A.; Mauro, G.L. The Effectiveness of Physical Exercise on Bone Density in Osteoporotic Patients. BioMed Res. Int. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; March, L. Treating osteoporosis. Aust. Prescr. 2016, 39, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aerssens, J.; Van Audekercke, R.; Geusens, P.; Schot, L.P.C.; Osman, A.A.-H.; Dequeker, J. Mechanical properties, bone mineral content, and bone composition (collagen, osteocalcin, IGF-I) of the rat femur: Influence of ovariectomy and nandrolone decanoate (anabolic steroid) treatment. Calcif. Tissue Int. 1993, 53, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Hara, K.; Kobayashi, M.; Akiyama, Y. Influence of bone osteocalcin levels on bone loss induced by ovariectomy in rats. J. Bone Miner. Metab. 2007, 25, 345–353. [Google Scholar] [CrossRef] [PubMed]
- McElroy, J.F.; Wade, G.N. Short- and long-term effects of ovariectomy on food intake, body weight, carcass composition, and brown adipose tissue in rats. Physiol. Behav. 1987, 39, 361–365. [Google Scholar] [CrossRef]
- Wu, Z.-X.; Lei, W.; Hu, Y.-Y.; Wang, H.-Q.; Wan, S.-Y.; Ma, Z.-S.; Sang, H.-X.; Fu, S.-C.; Han, Y.-S. Effect of ovariectomy on BMD, micro-architecture and biomechanics of cortical and cancellous bones in a sheep model. Med. Eng. Phys. 2008, 30, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Komrakova, M.; Hoffmann, D.B.; Nuehnen, V.; Stueber, H.; Wassmann, M.; Wicke, M.; Tezval, M.; Stuermer, K.M.; Sehmisch, S. The Effect of Vibration Treatments Combined with Teriparatide or Strontium Ranelate on Bone Healing and Muscle in Ovariectomized Rats. Calcif. Tissue Int. 2016, 99, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Honda, A.; Sogo, N.; Nagasawa, S.; Shimizu, T.; Umemura, Y. High-impact exercise strengthens bone in osteopenic ovariectomized rats with the same outcome as Sham rats. J. Appl. Physiol. 2003, 95, 1032–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, M.; Gleeson, J.; O’Brien, F.; McNamara, L. Effects of ageing, prolonged estrogen deficiency and zoledronate on bone tissue mineral distribution. J. Mech. Behav. Biomed. Mater. 2014, 29, 161–170. [Google Scholar] [CrossRef]
- Klein-Nulend, J.; Bacabac, R.G.; Bakker, A.D. Mechanical loading and how it affects bone cells: The role of the osteocyte cytoskeleton in maintaining our skeleton. Eur. Cells Mater. 2012, 24, 278–291. [Google Scholar] [CrossRef] [PubMed]
- Klein-Nulend, J.; Bacabac, R.; Mullender, M. Mechanobiology of bone tissue. Pathol. Biol. 2005, 53, 576–580. [Google Scholar] [CrossRef]
- Bonnelye, E.; Chabadel, A.; Saltel, F.; Jurdic, P. Dual effect of strontium ranelate: Stimulation of osteoblast differentiation and inhibition of osteoclast formation and resorption in vitro. Bone 2008, 42, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Atkins, G.J.; Welldon, K.J.; Halbout, P.; Findlay, D.M. Strontium ranelate treatment of human primary osteoblasts promotes an osteocyte-like phenotype while eliciting an osteoprotegerin response. Osteoporos. Int. 2008, 20, 653–664. [Google Scholar] [CrossRef]
- Chattopadhyay, N.; Quinn, S.J.; Kifor, O.; Ye, C.; Brown, E.M. The calcium-sensing receptor (CaR) is involved in strontium ranelate-induced osteoblast proliferation. Biochem. Pharmacol. 2007, 74, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Fromigué, O.; Haÿ, E.; Barbara, A.; Marie, P.J. Essential Role of Nuclear Factor of Activated T Cells (NFAT)-mediated Wnt Signaling in Osteoblast Differentiation Induced by Strontium Ranelate. J. Biol. Chem. 2010, 285, 25251–25258. [Google Scholar] [CrossRef] [Green Version]
- Welch, J.; Turner, C.; Devareddy, L.; Arjmandi, B.; Weaver, C. High impact exercise is more beneficial than dietary calcium for building bone strength in the growing rat skeleton. Bone 2008, 42, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.K.; Aloia, J.F.; Tierney, J.M.; Sprintz, S. Effect of treadmill exercise on vertebral and tibial bone mineral content and bone mineral density in the aged adult rat: Determined by dual energy X-ray absorptiometry. Calcif. Tissue Int. 1993, 52, 234–238. [Google Scholar] [CrossRef]
- Kontulainen, S.; Kannus, P.; Haapasalo, H.; Sievänen, H.; Pasanen, M.; Heinonen, A.; Oja, P.; Vuori, I. Good Maintenance of Exercise-Induced Bone Gain with Decreased Training of Female Tennis and Squash Players: A Prospective 5-Year Follow-Up Study of Young and Old Starters and Controls. J. Bone Miner. Res. 2001, 16, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Moreira, L.D.F.; De Oliveira, M.L.; Lirani-Galvão, A.P.; Marin-Mio, R.V.; Dos Santos, R.N.; Lazaretti-Castro, M. Physical exercise and osteoporosis: Effects of different types of exercises on bone and physical function of postmenopausal women. Arq. Bras. Endocrinol. Metabol. 2014, 58, 514–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westbroek, I.; Ajubi, N.; Alblas, M.; Semeins, C.; Klein-Nulend, J.; Burger, E.; Nijweide, P. Differential Stimulation of Prostaglandin G/H Synthase-2 in Osteocytes and Other Osteogenic Cells by Pulsating Fluid Flow. Biochem. Biophys. Res. Commun. 2000, 268, 414–419. [Google Scholar] [CrossRef]
- Joukar, A.; Niroomand-Oscuii, H.; Ghalichi, F. Numerical simulation of osteocyte cell in response to directional mechanical loadings and mechanotransduction analysis: Considering lacunar–canalicular interstitial fluid flow. Comput. Methods Programs Biomed. 2016, 133, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Bonewald, L.F.; Johnson, M.L. Osteocytes, mechanosensing and Wnt signaling. Bone 2008, 42, 606–615. [Google Scholar] [CrossRef] [Green Version]
- Grigorie, D.; Lerner, U. The Crucial Role of the WNT System in Bone Remodelling. Acta Endocrinol. 2018, 14, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Sawakami, K.; Robling, A.G.; Ai, M.; Pitner, N.D.; Liu, D.; Warden, S.J.; Li, J.; Maye, P.; Rowe, D.W.; Duncan, R.L.; et al. The Wnt Co-receptor LRP5 Is Essential for Skeletal Mechanotransduction but Not for the Anabolic Bone Response to Parathyroid Hormone Treatment. J. Biol. Chem. 2006, 281, 23698–23711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Zhang, Y.; Kang, H.; Liu, W.; Liu, P.; Zhang, J.; Harris, S.E.; Wu, D. Sclerostin binds to LRP5/6 and antagonizes canonical Wnt signaling. J. Biol. Chem. 2005, 280, 19883–19887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tu, X.; Rhee, Y.; Condon, K.W.; Bivi, N.; Allen, M.R.; Dwyer, D.; Stolina, M.; Turner, C.H.; Robling, A.G.; Plotkin, L.I.; et al. Sost downregulation and local Wnt signaling are required for the osteogenic response to mechanical loading. Bone 2012, 50, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Liu, D.; Ke, H.Z.; Duncan, R.L.; Turner, C.H. The P2X7 Nucleotide Receptor Mediates Skeletal Mechanotransduction. J. Biol. Chem. 2005, 280, 42952–42959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimston, S.K.; Brodt, M.D.; Silva, M.J.; Civitelli, R. Attenuated Response to In Vivo Mechanical Loading in Mice With Conditional Osteoblast Ablation of the Connexin43 Gene (Gja1). J. Bone Miner. Res. 2008, 23, 879–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Variables | Sh | O | OE | OSr | OESr |
|---|---|---|---|---|---|
| Whole body BMC (g) | 3.47 ± 0,66 c d e | 2.48 ± 0.63 c d e | 4.16 ± 0.57 a b | 4.22 ± 0.32 a b | 4.49 ± 0.99 a b |
| Whole body BMD (g/cm2) | 0.039 ± 0.009 b | 0.029 ± 0.012 vs. all | 0.043 ± 0.009 b | 0.044 ± 0.016 b | 0.047 ± 0.012 b |
| Weight (g) | 78.89 ± 27.56 b c | 114.63 ± 16.44 E e | 101.55 ± 12.20 a e | 94.38 ± 24.79 e | 64.53 ± 6.95 vs. all |
| Lean Mass (g) (%of weight) | 37.48 ± 19.57 46.91% vs. all | 59.21 ± 17.23 51.65% a | 52.13 ± 7.97 51.33% a | 50.47 ± 18.97 53.48% a | 43.65 ± 9.54 67.64% a |
| Fat Mass (g) (% of weight) | 38.95 ± 11.47 48.75% b e | 51.28 ± 11.48 44.74% a d e | 44.90 ± 7.28 44.21% e | 39.72 ± 10.86 42.09% b e | 18.02 ± 7.06 27.92% vs. all |
| Zones | Variables |  |  |  |  |  |
|---|---|---|---|---|---|---|
| Trabecular Bone | BV/TV (%) | 22.002 ± 1.647 b c e | 6;287 ± 0.866 vs. all | 19.017 ± 3.074 vs. all | 22.227 ± 0.631 b c e | 26.675 ± 0.534 vs. all |
| Tb.Th (mm) | 0.103 ± 0;115 vs. all | 0.092 ± 0.004 vs. all | 0.124 ± 0.008 vs. all | 0.141 ± 0.006 vs. all | 0.154 ± 0.009 vs. all | |
| Tb.N (1/mm) | 2.143 ± 0.115 vs. all | 0.683 ± 0.099 vs. all | 1.522 ± 0.195 a b e | 1.577 ± 0.083 a b e | 1.739 ± 0.092 vs. all | |
| Cortical Bone | Ct.Po(%) | 0.038 ± 0.015 e | 0.026 ± 0.012 e | 0.031 ± 0.017 e | 0.026 ± 0.016 e | 0.010 ± 0.007 vs. all |
| Ct.Th (mm) | 0.475 ± 0.038 vs. all | 0.413 ± 0.026 a d e | 0.398 ± 0.032 a | 0.503 ± 0.044 a b | 0.512 ± 0.035 a b | |
| Po.N (1/mm) | 0.011 ± 0.004 b d e | 0.007 ± 0.003 a e | 0.008 ± 0.004 a e | 0.006 ± 0.003 a e | 0.003 ± 0.002 Vs. |
| Variables | Sh | O | OE | OSr | OESr |
|---|---|---|---|---|---|
| Ultimate strength (N) | 134.193 ± 11.313 d e | 144.433 ± 11.040 e | 145.163 ± 13.110 e | 153.405 ± 11.234 a | 157.778 ± 13.046 a b c |
| Cross-sectional area (mm2) | 3.944 ± 0.258 vs. all | 4.556 ± 0.176 vs. all | 4.996 ± 0.0440 a b | 4.941 ± 0.368 a b | 5.274 ± 0.528 a b |
| Yield point stress (N) | 269.313 ± 34.599 c e | 256.185 ± 20.202 NS | 232.273 ± 18.045 a d | 264.452 ± 21.385 c | 243.035 ± 34.0,857 a b |
| Moment of inertia (mm4) | 4.207 ± 4.459 c e | 4.818 ± 0.435 c e | 5.555 ± 0.751 a b | 4.872 ± 0.585 ns | 5.776 ± 0.857 a b |
| Stiffness (N/mm) | 221.410 ± 25.469 d e | 223.143 ± 25.247 d e | 227.152 ± 25.271 d e | 241.152 ± 25.082 vs. all | 256.580 ± 25.469 vs. all |
| Variables | Sh | O | OD | OSr | OESr |
|---|---|---|---|---|---|
| ALP (U/L) | 1.686 ± 0.694 d e | 2.314 ± 0.844 d e | 1.808 ± 0.465 d e | 4.189 ± 0.839 vs. all | 3.110 ± 0.731 vs. all |
| OCN (pg/ml) | 1.577 ± 0.364 b e | 1.222 ± 0.346 vs. all | 1.538 ± 0.622 b e | 1.658 ± 0.466 b e | 1.879 ± 0.698 vs. all |
| NTX (nm) | 0.781 ± 0.152 d e | 0.857 ± 0.076 d e | 0.745 ± 0.103 d e | 0.585 ± 0.086 a b c | 0.622 ± 0.083 a b c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aveline, P.; Cesaro, A.; Mazor, M.; Best, T.M.; Lespessailles, E.; Toumi, H. Cumulative Effects of Strontium Ranelate and Impact Exercise on Bone Mass in Ovariectomized Rats. Int. J. Mol. Sci. 2021, 22, 3040. https://doi.org/10.3390/ijms22063040
Aveline P, Cesaro A, Mazor M, Best TM, Lespessailles E, Toumi H. Cumulative Effects of Strontium Ranelate and Impact Exercise on Bone Mass in Ovariectomized Rats. International Journal of Molecular Sciences. 2021; 22(6):3040. https://doi.org/10.3390/ijms22063040
Chicago/Turabian StyleAveline, Priscilla, Annabelle Cesaro, Marija Mazor, Thomas M. Best, Eric Lespessailles, and Hechmi Toumi. 2021. "Cumulative Effects of Strontium Ranelate and Impact Exercise on Bone Mass in Ovariectomized Rats" International Journal of Molecular Sciences 22, no. 6: 3040. https://doi.org/10.3390/ijms22063040