Abstract
Hepatic encephalopathy (HE) is a serious complication of cirrhosis that causes neuropsychiatric problems, such as cognitive dysfunction and movement disorders. The link between the microbiota and the host plays a key role in the pathogenesis of HE. The link between the gut microbiome and disease can be positively utilized not only in the diagnosis area of HE but also in the treatment area. Probiotics and prebiotics aim to resolve gut dysbiosis and increase beneficial microbial taxa, while fecal microbiota transplantation aims to address gut dysbiosis through transplantation (FMT) of the gut microbiome from healthy donors. Antibiotics, such as rifaximin, aim to improve cognitive function and hyperammonemia by targeting harmful taxa. Current treatment regimens for HE have achieved some success in treatment by targeting the gut microbiota, however, are still accompanied by limitations and problems. A focused approach should be placed on the establishment of personalized trial designs and therapies for the improvement of future care. This narrative review identifies factors negatively influencing the gut–hepatic–brain axis leading to HE in cirrhosis and explores their relationship with the gut microbiome. We also focused on the evaluation of reported clinical studies on the management and improvement of HE patients with a particular focus on microbiome-targeted therapy.
1. Introduction
Hepatic encephalopathy (HE) is a major complication occurring in the cirrhosis stage, accompanied by cognitive impairment. HE is a neurological or psychiatric abnormality with a broad spectrum from minimal to overt stage as a brain dysfunction, including cognitive alterations due to hepatic insufficiency or portal systemic shunt [1]. Mild cognitive impairment resulting from HE is estimated to affect 60–80% of the population of people with cirrhosis and causes significant deterioration in daily functioning and quality of life [2,3]. The prevention and early management of HE is crucial and can improve the prognosis of affected patients [4].
The factors related to the weakening of the gut environment, such as systemic inflammation and endotoxemia, act as major mechanisms in the pathogenesis of HE [5]. Changes in the gut microbiota are a key factor in the gut environment and are closely related to the progression of cirrhosis and its complications [6]. It is unclear whether disease progresses due to the gut microbiota alone in a vast complex system, such as the gut environment; however, the study of gut microbiota will be of great help in understanding cirrhosis and subsequent HE [7]. In particular, as the impaired gut–liver-brain axis plays a fundamental role in the pathogenesis of HE, exploration of the relationship will provide new options for HE therapy [8,9].
Current management of HE consists of intestinal-centered therapy with lactulose and lactitol and nonabsorbable antibiotics, such as rifaximin and neomycin [10]. Additionally, studies are underway to apply the modulating effect of intestinal microbes through probiotics and prebiotics to the therapeutic management of HE [11]. Through this, it is being considered as another alternative as it has confirmed the possibility of improving cognitive function while suppressing harmful gut bacteria and lowering ammonia absorption [12,13].
In addition, although the management of HE through pharmacological approaches and nutritional methods is being studied [14,15], the link with the intestinal microflora has not been clearly identified. We explore the association of HE with the gut microbiota based on the gut–liver-brain axis and evaluate the therapeutic management of HE with a focus on clinical research data. Through this, we review the future directions by identifying the link with the gut microbiota.
2. Gut Microbiota
The human digestive tract contains a microbial population that is approximately ten times the number of cells in the body and forms a complex ecosystem by forming a symbiotic relationship with the host [16]. The gut microbiota matures the host’s immune system and maintains homeostasis [17]. It also performs important functions related to metabolism, including vitamin synthesis, nutrient digestion, drug action and metabolism [18].
A major issue of study related to the gut microbiota has focused on its relationship to host health and disease. Existing studies have confirmed that the gut microbiota affects the improvement or exacerbation of liver disease. The evidence related to the deterioration of gut function in patients with cirrhosis and changes in the gut microbiota caused by dysbiosis was studied. Factors, such as decreased intestinal motility, small intestinal bacterial overgrowth and decreased bile acids caused by impaired enterohepatic circulation mainly affect the gut microbiota and alter the gut environment of patients [19,20]. Animal models and clinical studies have confirmed alterations in the gut microbiota in patients with cirrhosis and HE, resulting in increased production of ammonia and endotoxins [21,22].
A significant increase in Escherichia coli and Staphylococcus spp. was confirmed in the gut microbiome of cirrhotic patients with minimal HE (MHE), and evidence of a disruption of the gut microbiota was also reported [12]. A similar pattern has been observed for dysbiosis in these cirrhosis conditions, and some researchers have devised and used several indices for the diagnosis and prognosis of cirrhosis. One index that measures the degree of dysbiosis in cirrhosis is the Cirrhosis Dysbiosis Ratio (CDR) [23]. This index reported by Bajaj is calculated as the ratio of the abundance of Lachnospiraceae, Ruminococcaceae, Veillonellaceae and Clostridiales Incertae sedis XIV to that of Bacteroidaceae and Enterobacteriaceae.
This index also correlates with endotoxins and represents negative ecological and gut functional effects. Another index is the Gut Dysbiosis Index (GDI) reported by Wang [24]. The higher this index, the more severe dysbiosis appears. In addition, recently Bajaj et al. [25] reported that the addition of a microbiota index to an RNA or DNA model in the stool analysis of patients could be significantly added to the MELD score to predict the risk of hospitalization for liver cirrhosis.
Current HE therapies are based on modulation of this gut microbiota and are aimed at reducing blood ammonia and endotoxin and improving cognitive function. To improve and improve the effectiveness of treatment for HE, it is essential to understand the changes in the composition and functions of the gut microbiota. To this end, the resolution and management of dysbiosis can be key to the therapeutic approach of the disease. Utilization of the indices mentioned can help with this approach.
3. Hepatic Encephalopathy
HE is a reversible syndrome with impaired brain function observed in patients with advanced liver failure or decompensated cirrhosis stages. In addition, cases of HE have been reported in patients with extensive portosystemic shunting despite the absence of cirrhosis [26,27]. HE affects the brain due to the accumulation of neurotoxic substances in the bloodstream and presents a variety of neuropsychiatric abnormalities [28]. The patient develops personality changes, disorientation and depression, and severe disease progression can eventually lead to a coma and ultimately death [29]. Although the mechanism of brain dysfunction in liver failure has not been elucidated, it is clear that it is directly related to liver failure through reduced ammonia metabolism and loss of liver function [30,31].
The main triggers for HE are infection, alcohol consumption, drug noncompliance and kidney failure, which can occur in any situation present in chronic liver disease [32]. However, the pathogenesis of HE is still not well understood. There are clear limitations in directly studying the brains of HE patients, and the existing models representing HE are not perfect. Nevertheless, it is suggested that neurotoxic effects, neurological disorders due to metabolic changes induced by liver failure, systemic inflammatory responses, alterations in the brain barrier and changes in the brain energy metabolism may play a role [33,34]. The development of HE can be triggered or progressed through the interaction and simultaneous action of several complex factors.
Neurotoxic substances presumed to affect HE include short-chain fatty acids, manganese, γ-aminobutyric acid (GABA) and false neurotransmitters, such as tyramine and octopamine, among which ammonia is the most well-known [35]. Ammonia is continuously produced in human organs as a by-product of the catabolism of amino acids. In a healthy person, ammonia is produced by gut microbiota and is converted to glutamine by the liver, thus preventing the penetration of ammonia into the systemic circulation [36]. In the liver, ammonia is converted to urea through the urea cycle in periportal hepatocytes, which is then excreted or eliminated through the urine and colon [37].
The urea cycle undergoes five major steps and requires enzymes, including N-acetyl-glutamate synthase, carbamoyl phosphate synthetase, ornithine transcarbamylase, argininosuccinate synthetase, argininosuccinic acid lyase and arginase [38]. Among them, glutamine synthase is present in periportal hepatocytes and prevents the release of residual ammonia into the systemic circulation [39]. This enzyme synthesizes glutamic acid and ammonia and converts them to glutamine. However, in cirrhosis or equivalent liver failure, ammonia clearance decreases and progresses to hyperammonemia [40]. Additionally, when portal hypertension develops, various portal-systemic shunts occur as a complication, which is frequently observed in cirrhosis patients [41,42].
These portal-systemic shunts play a role in lowering portal pressure; however, through this, normal liver flow is bypasses, resulting in increased blood concentrations without detoxification or metabolization of various toxic substances, including ammonia [43,44]. When ammonia, which is excessively accumulated in the blood, passes through the blood–brain barrier, a neurotoxic effect is expressed, which results in the swelling of astrocytes [45,46]. As astrocytes metabolize the infiltrated ammonia and produce glutamine, the osmolarity increases, which can lead to brain edema [47]. Ammonia additionally inhibits excitatory and inhibitory postsynaptic potential generation, negatively affecting neuroelectric activity and leading to impaired energy and amino acid metabolism [48] (Figure 1).
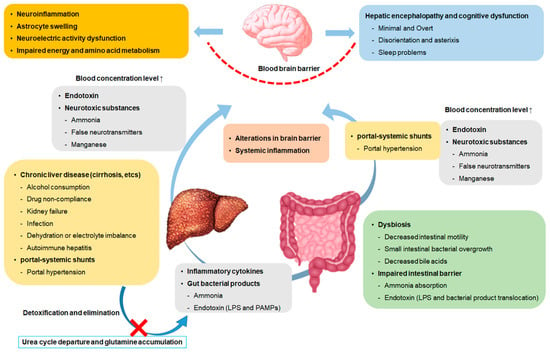
Figure 1.
Schema of brain dysfunction by the gut-liver-brain axis. LPS, Lipopolysaccharide; and PAMPs, pathogen-associated molecular patterns.
The gut microbiota is known as one of the factors that can trigger HE; however, the detailed mechanisms are not fully understood. However, intestinal changes due to dysbiosis contribute to MHE [49]. In the intestines of patients with cirrhosis and liver failure, changes occur in the abundance of pathogenic gut microbiota from overgrowth of small intestine bacteria [50]. An increase in gut microbiota taxa, such as Porphyromonadaceae, is positively correlated with cognitive impairment [23]. In this way, analysis of the gut microbiota from patients’ feces and saliva could be helpful in the diagnosis of HE [51].
4. Linkage of Gut Microbiota with Hepatic Encephalopathy
Recent cumulative data reveal a close correlation between HE and the gut microbiome [52,53]. Advances in gut microbiome analysis are providing new perspectives in the treatment of HE [54,55]. Newly developed analytical methods have moved beyond simply cataloging the composition of the gut microbiota to understanding their interrelationships with diseases. In this way, we influence our understanding of HE-targeted gut microbiota therapy, diagnosis and management. We focused on clinical data to illuminate the relationship between the gut microbiota and HE.
4.1. Gut Microbiota in Hepatic Encephalopathy Diagnosis
The diagnosis of HE ranges from clinical scales to psychometric and neurophysiological approaches. Testing and diagnosis options may vary depending on the severity of HE symptoms [56]. Representative symptoms of overt HE (OHE) include disorientation and asterixis [57]. In OHE, the diagnosis of cognitive impairment is not difficult to make through clinical observations and neurophysiological examinations, if other causes of mental status abnormalities, such as drug and alcohol abuse as well as hyponatremia are excluded [58]. MHE is frequently seen in patients with chronic liver disease, and brain dysfunction can be judged as test-dependent or clinical signs [58].
MHE does not show cognitive signs or other clinical signs and should be tested with psychometric and neurophysiological approaches [59]. MHE may cause socioeconomic difficulties due to a decrease in the patient’s quality of life [60,61]. Examination of patients with all potential risks is required for the diagnosis of MHE; however, it may cause economic difficulties due to the cost of the examination [62]. Since the tests and clinical measures currently applied to diagnose HE are not valid for the overall HE spectrum [46], adding additional diagnostic strategies should increase the reliability and determine the severity of cognitive impairment.
The close correlation between disease and the gut microbiome was the main focus of chronic liver disease study [63]. In the early days of the study of the gut microbiome of liver cirrhosis patients, the definition of changes in the gut microbiome by culture-based study was the main focus; however, after the metagenomic revolution [64], the progress of culture-independent technology made it possible to analyze the overall changes in the com-position and function of the microbiome in detail [7]. These changes in analysis technology are gradually enabling the expansion of the diagnostic field of liver diseases through the gut microbiome. Table 1 provides a summary of studies evaluating the gut microbiome in cirrhosis and HE patients as examples that can be used for diagnostic application.
Certain changes in the gut microbiome have been clearly identified between cirrhosis patients without cognitive impairment and cirrhosis patients with MHE or OHE [65]. Sung and colleagues profiled dynamic changes in the gut microbiome of cirrhotic patients with OHE compared to healthy individuals and cirrhosis patients. In patients with acute HE, the relative abundance of Bacteroidetes decreased while the relative abundance of Firmicutes, Proteobacteria, Actinobacteria and Veillonella parvula increased. In addition, the association between HE recurrence and survival time of specific taxa was confirmed [66].
Zhang et al. reported that Streptococcus salivarius showed a higher relative abundance in cirrhotic patients with MHE than in non-MHE cirrhotic patients. Streptococcus salivarius showed a positive correlation with ammonia accumulation and could be a potential biomarker targeting MHE cirrhotic patients [67]. Bajaj et al. confirmed the difference in the composition of fecal microbiota between healthy controls and cirrhosis patients and analyzed the change in the fecal microbiota of cirrhosis patients according to the presence or absence of HE [68].
The fecal microbiota of cirrhotic patients were significantly different from those of healthy controls. The relative abundances of Enterobacteriaceae, Alcaligeneceae and Fusobacteriaceae were high but lower for Ruminococcaceae and Lachnospiraceae. High levels of Veillonellaceae and endotoxemia were found between cirrhosis patients without HE and HE patients, and in particular Alcaligeneceae and Porphyromonadaceae were reported to have a positive correlation with cognitive impairment. In addition, since Alcaligenaceae can produce ammonia through urea decomposition, the association of HE with cognitive impairment was confirmed.
Subsequently, the same researchers successively analyzed the microbiome of the feces and colonic mucosa of cirrhosis patients [49]. The control group had lower pathogenic bacterial genera than cirrhotic patients, including HE in the microbiome, and HE patients had a poorer model for end-stage liver disease (MELD) score and higher endotoxin levels than no-HE patients. Although the microbiome analyzed in the stool was not prominent, the sigmoid mucosal microbiome showed a significant difference, further confirming the difference with or without HE.
In the mucosal microbiota of HE patients, Enterococcus, Veillonella, Megasphaera and Burkholderia predominated at high levels, whereas Roseburia showed low levels compared to the control group. Blautia, Fecalibacterium, Roseburia and Dorea were associated with good cognition and reduced inflammation in both HE and no-HE patients, whereas Enterococcus, Megasphaera and Burkholderia, prominent in HE patients, were strongly associated with cognitive impairment.
A clear difference in the gut microbiome between the healthy control group and cirrhosis patients with liver cirrhosis and HE was revealed through various lines of evidence, and it was confirmed that these differences were strongly related to symptoms, such as cognitive impairment and inflammation. This difference is expected to bring accuracy to the diagnosis of the disease and will act as a clue in the therapeutic stage.

Table 1.
Human study of microbiome change in cirrhosis with hepatic encephalopathy.
Table 1.
Human study of microbiome change in cirrhosis with hepatic encephalopathy.
| Author | Scheme | Group | Result | Ref. |
|---|---|---|---|---|
| Sung et al., 2019 | Profiled fecal microbiome changes for a cohort patients | Control/compensated cirrhosis/decompensated cirrhosis/Acute HE | Higher Firmicute, Proteobacteria, Actinobacteria and Veillonella parvula and lower Bacteroidetes phylum in AHE patients compared compensated cirrhosis. | [66] |
| Zhang et al., 2013 | Gut microbiome analysis of MHE patients with cirrhosis | MHE/cirrhotic patients without MHE | Higher Streptococcus salivarius in MHE cirrhotic patients compared no-MHE cirrhotic patients. Gut ammonia-increasing bacteria Streptococcus salivarius can be a potential biomarker in MHE cirrhotic patients. | [67] |
| Bajaj et al., 2012 | Stool analysis of cirrhosis patients and age-matched controls | Cirrhotic patients with or without HE/control | Higher Veillonellaceae in HE cirrhotic patients. Alcaligenaceae and Porphyromonadaceae were positively correlated with cognitive impairment in cirrhotic patients | [68] |
| Bajaj et al., 2012 | Sigmoid mucosal and fecal microbiome analysis to study linkage with cognition and inflammation | OHE patients/no-OHE patients/control | Higher Enterococcus, Veillonella, Megasphaera and Burkholderia in mucosal microbiota of HE patients. Lower Roseburia in mucosal microbiota of HE patients. Blautia, Fecalibacterium, Roseburia and Dorea are associated with a positive cognition state and Enterococcus, Megasphaera and Burkholderia are associated with a poor cognition state. | [49] |
AHE, acute episode of overt hepatic encephalopathy; HE, hepatic encephalopathy; MHE, minimal hepatic encephalopathy; and OHE, overt hepatic encephalopathy.
4.2. Gut Microbiota in HE Treatment
Given the impact and key role of the microbiota and host interaction on HE, it is only natural that the direction of the investigation of HE therapy targets the gut microbiota. Several treatments have been studied, ranging from direct approaches aimed at relieving dysbiosis observed in cirrhosis patients or reducing harmful taxa, to targeting metabolites by microbiota. Here, we refer to several therapeutic approaches and summarize the cases.
4.2.1. Probiotics and Prebiotics
The various effects of probiotics are being proven or tested in a number of diseases. Likewise, probiotics are being considered as one of the treatments that can improve HE and have been applied and studied in several studies. The expected effects of probiotics include improvement of intestinal barrier function by modulating gut microbiota, immune regulation and HE treatment effects by reducing portal hypertension. In addition, synbiotics are being studied as potential therapeutics for HE and lactulose, a representative nonabsorbable disaccharide and prebiotic, is being used as an effective treatment for HE (Table 2).
A previous study evaluated the effectiveness of Lactobacillus rhamnosus GG (LGG) in patients with MHE in a phase 1 randomized controlled trial [52]. Patients were treated with LGG or placebo for 8 weeks, and the fecal microbiota, inflammation and endotoxin levels were analyzed. As a result, Enterobacteriaceae decreased in the LGG group, the relative abundance of Clostridiales Incertae Sedis XIV and Lachnospiraceae increased, and endotoxemia and TNF-α decreased. However, as the efficacy of the study was not proven, no cognitive changes were observed between patients.
Xia et al. conducted a probiotic-based treatment for HBV cirrhosis patients with MHE [69]. Probiotics were given to patients in combination with Clostridium butyricum and Bifidobacterium infantis. In the intestinal microflora of the patients, Clostridium cluster I and Bifidobacterium were increased and Enterococcus and Enterobacteriaceae were decreased, which also decreased the level of venous ammonia and had an effect on cognitive improvement. In another study, a mixture of VSL#3 probiotics was administered to cirrhotic patients without HE and their effectiveness was confirmed [70]. Reductions in arterial ammonia levels, small intestinal bacterial overgrowth (SIBO) and orocecal transit time (OCTT) were observed after 3 months of probiotic treatment.
As a result, it was possible to confirm the primary prevention effect in OHE through the administration of probiotics. Another study confirmed the effect of synbiotics in MHE patients without OHE through an additional combination [12]. The synbiotics used in the study were provided to patients by combining urease-free bacteria and fermentable fibers. As a result, the content of Lactobacillus, which does not produce urease, was increased in the patient’s feces, and endotoxemia was reduced.
In addition, improvement in the Child–Turcotte–Pugh functional class, reduction in blood ammonia levels and reversal of MHE were observed in 50% of patients receiving synbiotics. Other researchers who provided patients with a combination of Bifidobacterium and fructooligosaccharides reported improvements in psychometric tests compared to the lactulose-treated group, with improvements in blood ammonia levels and psychometric tests after 60 days.
Lactulose is a synthetic, nonabsorbable disaccharide used as one of the treatments for HE that affects the gut microbiota and reduces the absorption of ammonia. In a study evaluating the effect of lactulose on MHE patients, a reduction in bacterial DNA translocation and improvement in neurocognitive test scores were observed [71]. This is likely due to the effect of lactulose in changing the gut microbiota and improving intestinal permeability. In a randomized controlled trial in HE patients, positive alterations in the gut microbiota were observed in patients responding to lactulose treatment [72]. Significant differences were observed between lactulose responders and nonresponders in Bacteroidetes, Firmicutes, Actinobacteria and Proteobacteria.
However, the limitations as therapeutic agents for the abovementioned probiotics and prebiotics are still clear. Accurate comparative analysis is difficult due to differences in research design and delivery methods of probiotics used in each clinical study. In addition, the question remains as to whether the intestine of cirrhosis patients can be reconstituted into a healthy complex microbiome through probiotics or prebiotics as an environment in which dysbiosis occurs [73].
Probiotics, prebiotics and synbiotics may not reach the vulnerable intestine of cirrhotic patients correctly or may be eliminated by antibiotic treatment and may not induce changes in the intestinal environment. Lactulose, which is widely used as a treatment for HE, was also reported to have increased bacterial imbalance despite lactulose treatment in HE patients, unlike the previously reported effects of inducing changes in the gut microbiota [23].
In addition, the evaluation of the therapeutic effect of HE on nonabsorbable disaccharides remains controversial. A meta-analysis reported in the Cochrane Review in 2004 found that nonabsorbable disaccharides had a beneficial effect on HE but not on mortality. However, in the review at the time, the argument of the conclusion about nonabsorbable disaccharide showed weakness due to the lack of statistical power and methodological problems, such as bias area reporting.
Subsequently, an updated 2016 Cochrane Review found evidence for the efficacy and safety of nonabsorbable disaccharides for the treatment and prevention of HE in cirrhosis patients and reached conclusions. The use of nonabsorbable disaccharides has significantly confirmed minimal and overt therapeutic effects for HE and has an overall beneficial effect on liver-related morbidity and all-cause mortality.
The evaluation of nonabsorbable disaccharides has been revisited with the ongoing development of new randomized clinical trials and updates to the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD) practice guidelines. In order to evaluate the controversies of these microbial-targeted therapies, improve the limitations and increase the therapeutic effects, alternatives, such as data accumulation through large-scale studies and establishment of standards should be prepared.
Table 2.
Probiotics and prebiotics therapies for hepatic encephalopathy.
Table 2.
Probiotics and prebiotics therapies for hepatic encephalopathy.
| Author | Scheme | Group | Result | Ref. |
|---|---|---|---|---|
| Bajaj et al., 2014 | A randomized clinical phase 1, placebo-controlled trial | LGG or placebo in cirrhotic patients with MHE | In the LGG group, Enterobacteriaceae decreased and the relative abundance of Clostridiales Incertae Sedis XIV and Lachnospiraceae increased. Endotoxemia and TNF-α were decreased in the LGG group but there was no change in cognitive function. | [52] |
| Xia et al., 2018 | A randomized clinical trial | Probiotics (Clostridium butyricum combined with Bifidobacterium infantis) or no probiotics | Clostridium cluster I and Bifidobacterium increased and Enterococcus and Enterobacteriaceae decreased in the group treated with probiotics in HBV cirrhosis patients with MHE. There was also a reduction in venous ammonia and cognitive improvement. | [69] |
| Lunia et al., 2014 | A prospective, randomized controlled trial | Cirrhosis patients without OHE given probiotics (VSL#3)/cirrhosis patients without OHE not given probiotics (VSL#3) | Treatment with probiotics for 3 months significantly reduced arterial ammonia, SIBO and OCTT levels. Probiotics have shown a preventing effect on HE. | [70] |
| Liu et al., 2004 | A randomized clinical trial | Synbiotic preparation/fermentable fiber alone/placebo | Synbiotic treatment increased the fecal content of Lactobacillus species that do not produce urease. Modulation of the gut microbiota showed a reduction in blood ammonia levels and reversal of MHE in 50% of patients. | [12] |
| Malaguarnera et al., 2010 | A randomized controlled trial | Bifidobacterium + fructooligosaccharides or lactulose in HE patients | The combination of Bifidobacterium and fructooligosaccharide at 30 days of treatment showed improvement in psychometric tests compared to the lactulose group. Treatment for 60 days showed significant improvement in psychometric tests and blood ammonia levels. | [74] |
| Moratalla et al., 2017 | Observational cohort study of cirrhosis patients with MHE | First cohort: MHE patients with or without lactulose Second cohort: Non-lactulose MHE patients going to initiate lactulose therapy | Lactulose reduces bacterial DNA translocation and improves neurocognitive test scores in MHE patients. | [71] |
| Wang et al., 2019 | A multicenter, open-label randomized controlled trial | Lactulose or control in cirrhotic patients | Treatment with lactulose significantly improved MHE recovery. Significant differences were found between lactulose responders and non-responders in Bacteroidetes, Firmicutes, Actinobacteria and Proteobacteria. | [72] |
HE, hepatic encephalopathy; LGG, Lactobacillus rhamnosus GG; MHE, minimal hepatic encephalopathy; OCTT, orocecal transit time; OHE, overt hepatic encephalopathy; and SIBO, small intestinal bacterial overgrowth.
4.2.2. Fecal Microbiota Transplantation
Fecal microbiota transplantation (FMT) is the transfer of stool from a ‘healthy’ donor to a patient with an imbalanced gut microbiota for recovery purposes [75]. When FMT is performed in HE patients, it can be expected to change the composition of the gut microbiota to rebuild intestinal barrier integrity and reduce ammonia absorption (Table 3). In several animal models, FMT had confirmed effects in reducing intestinal ammonia production in the gut and decreasing the reduced risk of encephalopathy [76].
Table 3.
Fecal microbiota transplantation therapies for hepatic encephalopathy.
In a case report, Kao et al. demonstrated for the first time that continuous FMT in patients with mild HE improved cognitive function as assessed by the Stroop test and inhibitory control test [77]. However, the beneficial effects did not persist after FMT was discontinued, and there were reports of results suggesting that it is unclear whether FMT is effective for severe HE. Bajaj et al. performed FMT in patients with recurrent HE and compared it with the standard of care [54]. For rational donor selection, feces from donors with the highest relative abundance of Lachnospiraceae and Ruminococcaceae were selected using machine-learning techniques.
At the 5-month follow-up, compared with standard of care, improvement of dysbiosis and improvement of cognitive function were confirmed through an increase in beneficial taxa and diversity. Afterward, similar results were reported in phase 1 clinical trials using FMT oral capsules in patients with recurrent HE [78]. Oral FMT capsules were prepared from the feces of the same donor as above. The patients who received the FMT capsule showed improvement in the cognitive cognition test using EncephalApp but not in the test using the psychometric HE score. However, the microbiome diversity and intestinal microbiome imbalance of the duodenal mucosa were improved, and the expression of antimicrobial peptides and reduction in lipopolysaccharide-binding proteins were confirmed.
One of the key factors to consider first in FMT is the optimization of donors and recipients. Bloom et al. [79] evaluated the safety and efficacy of FMT in patients with overt HE through donor diversity. A total of five FMT donors were screened and administered fivefive FMT capsules over 3 weeks. After 6 months of follow-up of 10 patients, no change in the Model for End-Stage Liver Disease (MELD) score was observed. In the evaluation of serious adverse events in this study, 13 minor adverse events and one extended-spectrum beta-lactamase Escherichia coli bacteremia were reported.
After FMT, the psychometric HE score improved, and the range of change varied among donors. In addition, high levels of Bifidobacterium and other known beneficial taxa were identified in stool analysis of FMT responders. In conclusion, cognitive improvement in HE was confirmed; however, the effect varied widely between donors and recipients. The study reported by Bloom et al. [79] is an important reminder of the importance of donor and recipient factors and the importance of selection.
Overall, studies evaluating the effects of FMT on HE have been designed with safety-first objectives, and definitive efficacy evaluations are lacking. In addition, there are risk factors for infection and safety due to the lack of standards and tests for donor selection. The potential benefits of FMT are clear; however, large-scale studies are needed to establish additional dosing strategies.
4.2.3. Antibiotics
Antibiotics in the treatment of HE are suggested as a way to deplete certain taxa in the gut that produce urease-producing bacteria or neurotoxins and reduce the systemic immune response [80]. It is known that certain antibiotics can potentially survive beneficial taxa and selectively inhibit harmful taxa [81]. The current mainstream treatment for HE is a combination of antibiotics and lactulose (Table 4). Rifaximin, recently used to treat HE, is an antibiotic with broad-spectrum activity against both Gram-positive and Gram-negative, aerobic and anaerobic bacteria [82].
Rifaximin is an antibiotic approved in the United States and Europe to reduce the risk of recurrent OHE [1]. Administration of rifaximin to HE patients reduced hyperammonemia and endotoxemia and showed cognitive improvement [83]. In current clinical practice, rifaximin is recommended as an additional therapy to prevent OHE recurrence and is prescribed in combination with lactulose for OHE patients [83]. Several clinically controlled trials have reported that rifaximin significantly reduces the risk of recurrent OHE and improves the cognition and quality of life in MHE patients [84].
The effectiveness of rifaximin was also confirmed in a study that determined whether rifaximin was associated with the risk of death and cirrhosis complications. Kang et al. [85] reported that the risk of death and the reduced risk of recurrent HE were significantly related in the group of patients receiving rifaximin and lactulose compared to the control group receiving only lactulose in non-hepatocellular carcinoma (HCC) cohort. In this way, rifaximin treatment significantly affects the prolongation of overall survival and reduced risk of complications, such as spontaneous bacterial peritonitis, varicose bleeding and recurrent hepatic encephalopathy [85].
A decrease in endotoxin activity and serum ammonia levels was reported in 20 patients with decompensated cirrhosis after 4 weeks of rifaximin administration [86]. In addition, it was confirmed that cognitive improvement was significantly achieved through this. A decrease in the genera Veillonella and Streptococcus was observed; however, the effect of rifaximin on the diversity of the gut microbiome was not confirmed. Another clinical study in which rifaximin was administered to 20 MHE patients also confirmed a significant improvement in endotoxemia [87].
After rifaximin was administered, cognitive improvement was confirmed, and an increase in serum saturated and unsaturated fatty acids was observed. There was a decrease in Veillonellaceae and an increase in Eubacteriaceae; however, there was no significant change in the overall intestinal microflora. However, a change was confirmed in the correlation network analysis with rifaximin. In networks centered on Enterobacteriaceae, Porphyromonadaceae and Bacteroidaceae, transfer changes associated with association with beneficial metabolites and cognitive improvement were observed.
Other researchers have confirmed the gut microbiota and therapeutic effects of rifaximin alone or rifaximin plus probiotics administered to MHE patients [88]. In both treatment groups, a decrease in the diversity of the gut microbiota was observed, and a decrease in certain ammonia-producing taxa, such as Clostridium was observed. Rifaximin showed a decrease in Streptococcus, Veillonella and Lactobacillus with hyperammonemia and cognitive improvement, however, still showed no significant effect or change on the overall relative abundance of bacteria [89,90]. In patients with cirrhosis and MHE, rifaximin alone or rifaximin plus lactulose consecutively for 3 months did not show any significant changes in the microbiome [91]. The microbiota analyzed in duodenal samples and feces showed clear differences; however, no changes were observed before versus after treatment.
Combining the reported clinical results, the effect of rifaximin on the overall gut mi-crobiota composition has not been observed and no conclusion has been reached either. Detailed changes in species or subgroups have not been measured and may not have confirmed the effect of such rifaximin. The effect of rifaximin on changes in the composition of the gut microbiome has been demonstrated in animal studies and in changes in microbial metabolites, such as bile acids [92,93]. Changes in beneficial taxa in irritable bowel syndrome or Crohn’s disease are clearly observed [94]. To analyze the effects and mechanisms of rifaximin on the intestinal microflora for the treatment of HE in the future, it is necessary to identify changes at the species and subtaxa levels.
Table 4.
Antibiotics therapies for hepatic encephalopathy.
Table 4.
Antibiotics therapies for hepatic encephalopathy.
| Author | Scheme | Group | Result | Ref. |
|---|---|---|---|---|
| Kang et al., 2017 | A retrospective cohort study | Rifaximin + lactulose or lactulose in non-HCC cohort or HCC cohort | In the non-HCC cohort, rifaximin was significantly associated with a lower risk of death and reduced the risk of recurrent HE, spontaneous bacterial peritonitis. In the HCC cohort, rifaximin was not associated with a risk of death. It was associated with a lower risk of spontaneous bacterial peritonitis but not with varicose bleeding or recurrent HE. The risk of Clostridium difficile-associated diarrhea was not different between the two groups. | [85] |
| Kaji et al., 2017 | A clinical trial | 20 patients with decompensated cirrhosis (Child–Pugh score > 7) | Treatment with rifaximin for 4 weeks resulted in a decrease in endotoxin activity and serum ammonia levels. Treatment with rifaximin for 4 weeks resulted in a decrease in endotoxin activity and serum ammonia levels. There was no significant difference in the diversity and composition of gut microbiota at baseline and after 4 weeks of treatment but the relative abundance of genus Veillonella and Streptococcus was lowered. | [86] |
| Bajaj et al., 2013 | A clinical trial | 20 patients with cirrhosis who had been diagnosed with MHE | There was a significant cognitive improvement and a decrease in endotoxemia after rifaximin treatment. Serum saturated and unsaturated fatty acids were significantly increased after rifaximin treatment. No significant changes in gut microbiota were observed except for the decrease of Veillonellaceae and the increase of Eubacteriaceae. | [87] |
| Zuo et al., 2017 | A randomized clinical trial | Rifaximin or rifaximin and probiotics in cirrhotic patients with MHE | Both treatments reduced overall microbiome diversity and decreased abundance of specific ammonia-producing bacteria. The treatment with rifaximin + probiotics showed a more definite effect. Patients with nonalcoholic MHE were more responsive to microbiota alteration therapy. | [88] |
| Suzuki et al., 2018 Kawaguchi et al., 2019 | A prospective, randomized studies (a phase II/III study and a phase III study) | Rifaximin or lactitol with grade I or II HE and hyperammonemia patients | Blood ammonia concentrations were significantly improved in the rifaximin group. The portal systemic encephalopathy index was significantly improved in both groups. As a result of fecal microbiome analysis of 17 participants in the clinical trial, the number of Streptococcus, Veillonella and Lactobacillus decreased after rifaximin treatment. Rifaximin alters the composition of microbial taxa linked to hepatic/neuropsychological function. | [89,90] |
| Schulz et al., 2019 | A randomized clinical trial | Rifaximin or rifaximin and lactulose in cirrhotic patients with MHE | An improvement in MHE was confirmed after treatment. Microbiological analysis was performed on duodenum and stool samples and no statistically significant changes were found in the bacterial profile. Rifaximin therapy with or without lactulose for 3 months has no effect on microbiome composition. HE improvement with rifaximin persisted after termination. | [91] |
HCC, hepatocellular carcinoma; and MHE, minimal hepatic encephalopathy.
4.2.4. Dietary
Therapeutic strategies for HE have been to modulate the systemic inflammation, neurotoxic substances, such as ammonia, and changes in the composition and environment of the gut microbiota [95]. Additionally, implementing these strategies in conjunction with a diet at the same time can play an important role in treatment and management [96]. It has been known through many reports that changes in eating habits are closely related to the gut microbiota [97]. These dietary adjustments and changes have beneficial effects on the gut microbiome and affect disease improvement. Likewise, it can alter the cascades that lead to cognitive impairment by regulating the gut nitrogen metabolism and improving inflammation [98].
For the management of HE, recommendations for dietary changes are presented as key clinical guidelines, which can make a significant contribution to treatment and prevention. The American Association for the Study of Liver Diseases (AASLD), in its 2014 guidelines [1], recommended a calorie intake of 35–40 kcal/kg/day for patients with cirrhosis and HE.
The International Society for Hepatic Encephalopathy (ISHEN) also recommends a calorie intake of 35–40 kcal/kg/day [11], and the European Association for the Study of the Liver (EASL), in its latest guidelines published in 2019 [99], recommends at least 35 kcal/kg/day. Additionally, the European Society for Clinical Nutrition and Metabolism (ESPEN) recommends a calorie intake of 30–35 kcal/kg/day [99]. The four organizations recommend a protein intake of 1.2–1.5 g/kg/day. In particular, lipids in the diet are beneficial to patients with HE, as they have been shown to have beneficial effects on gut microbiota and bowel transit time [15].
As abnormal nitrogen metabolism plays an important role in the pathogenesis of HE, and early studies suggested that protein intake should be reduced [100]. However, further studies have reported that it has no beneficial effect on the progression of HE and worsens the nutritional status of patients by exacerbating protein breakdown in muscle [101]. Rather, it has been found that normal protein intake is well tolerated in HE and is useful in ensuring sufficient substrates for energy synthesis and hepatocyte function [102].
As additional nutrients, branched-chain amino acids, such as valine, leucine and isoleucine, have been shown to prevent excessive protein catabolism and reduce ammonia levels in patients with HE [103]. There are still obstacles and limitations in the application of these dietary and nutritional treatment modalities for HE, and high-quality randomized controlled trials are required [104]. In addition, there is still little research on the effect of diet and nutrition on the relationship between HE and the gut microbiota we are dealing with. If the positive factors of diet on this relationship are identified or proven in the future, this could be another option for HE treatment strategies.
5. Challenges and Limitations
The human gut microbiome is constantly exposed to external factors, such as diet, drugs and pathogens but has the ability to restore equilibrium after perturbation [105]. However, in diseases, such as cirrhosis, dysbiosis occurs in which the overgrowth of harmful taxa is promoted and beneficial taxa is suppressed [106]. Therefore, the effect of HE-related gut microbiota therapy should be confirmed through continuous iterations rather than single short-term therapy. Treatment with the gut microbiome occurs through an ecosystem connected by the gut–liver axis [107]. Due to the interconnected components of these complex ecosystems, a change in the composition of a single microbial community can have unexpected ramifications or no impact or effect at all [108].
FMT, which is being studied as one of the treatments for HE, has its own challenges and limitations [109]. As it is donated from the feces of healthy individuals, it will change over time. There are also difficulties in identifying pathogens from FMT materials. Due to this problem, there has recently been a case of infection by ESBL-producing Escherichia coli [110,111]. Clinical trials of FMT for HE used different routes, doses and timing of administration. Due to these differences, there is still a lack of understanding of the best FMT dosing regimen [109,112]. Criteria for an ideal FMT donor are also lacking. This optimal donor selection may require detailed analysis of microbiome composition as well as function. Additionally, there are restrictions on the preparation of FMT. When prepared aerobically, the benefits of anaerobicity are lost because of the lack of supplementation for anaerobic microorganisms.
The use of antibiotics, the main treatment for HE, also poses an important problem, as it can lead to multidrug resistance. Although the prevalence of resistant bacteria continues to rise [113,114], the use of antibiotics for the treatment of HE has no choice but to be used in a balanced way with the problem of resistance in mind.
Our review of HE addressed only a narrow category of links with the gut microbiota. Currently, pharmacological approaches to the treatment of HE are also being actively studied. L-ornithine-L-aspartate increases ammonia metabolism in the liver and muscle, thereby lowering blood ammonia levels [115,116]. Although it has been effective in improving the mental state and psychometric performance of patients in clinical studies [117], there are still problems and hurdles that are not approved in many countries.
Sodium benzoate may be used in patients with congenital urea circulation defects and is an FDA-approved drug for the treatment of acute hyperammonemia and related encephalopathy [118,119]. However, there are problems, including the management of ascites in cirrhosis patients. This pharmacological approach could be proposed as an effective way for the treatment of HE. However, there are no studies on the relationship between these pharmacological treatments and the gut microbiome. Therefore, it is not within the scope of this review, as it departs from the solution we address in this review through modulation of the gut microbiome.
6. Future Directions
The treatment of HE through the gut microbiome is being achieved through major therapies, such as lactulose and rifaximin, as well as some applied therapies, such as probiotics, prebiotics and FMT. However, many HE patients still suffer from persistent symptoms. The future directions of therapeutic studies targeting the gut microbiome should be aimed at personalized treatment approaches, therapy selection and clinical trial design.
Since therapy using the gut microbiome affects the gastrointestinal tract as a whole, it is necessary to check the effects on each part of the intestine and the effects on intestinal permeability. Further studies, including larger trials, are needed to determine the ideal dosing regimen for FMT, donor selection and the benefits of anaerobic conditions. Research into the unique gut microbiome of HE patients and therapies designed for their gut type should also be pursued. A personalized approach will be an important issue in future directions for treatment success as it can maximize the effectiveness of therapies.
For the treatment and management of HE, the scope is expanding with convergence [120] with new areas: First, as dysbiosis is induced in cirrhosis and it has been confirmed that this gut microbiota imbalance affects bacterial products and metabolites [68,121], related multiomics studies are being conducted. Researchers are focusing on the gut microbiota of metabolic potential comparable to the liver and are studying the treatment of liver disease and related complications based on the gut–liver axis [122,123].
In introducing the concept of ‘functional metagenomics’, Li et al. [124] demonstrated that functional key members of the gut microbiome have a significant impact on the metabolism and health of the host. Other researchers have discovered altered immune pathways through a multiplex approach to profiling of transcripts, metabolites and cytokines in blood samples from cirrhosis patients [125]. Going forward, we will go beyond generally focusing on single or target components, such as short-chain fatty acids [126] to deepen our understanding of gut microbiota dynamics in relation to host physiology and pathology [127], exploring the broad and complex host-microorganism metabolic interactions in the superorganism.
This may provide new inspiration for the treatment of cirrhosis and HE. The second approach to new territory is AI. Recently, methods utilizing artificial intelligence and machine-learning algorithms are being applied to hepatology [120]. Machine learning is the use of artificial intelligence to create and utilize predictive models on large data sets more efficiently and effectively than traditional methods [120]. MHE can be detected by special, time-consuming psychometric tests. Recently, as the diagnostic approach of MHE through artificial intelligence and machine learning is progressing, uncertainty resolution is being studied [128].
Artificial intelligence and machine learning are being applied in a variety of ways, from analysis using magnetic resonance imaging data [129,130] to methods of distinguishing patients with different cirrhosis severities by the microbiome of saliva and feces [65]. In particular, the use of artificial intelligence (AI) could become a necessity in the near future, especially for the utilization of large data sets, such as linking gut microbiome data and human biometric data.
Artificial intelligence and machine learning will help classify disproportionate medical data and build risk prediction and diagnostic evaluation systems for liver cirrhosis with HE [131]. The third is a personalized therapeutic approach. The gut microbiome has the potential to uniquely identify an individual like a fingerprint [132]. Therefore, even the same treatment may have different responses [133]. A method for determining baseline microbiome characteristics has been proposed to be consistent with an appropriate microbiome therapy. They also reported that a personalized approach to microbiome treatment based on baseline community structure and function may achieve the most clinical success [133].
The future direction of the treatment and management of cirrhosis and HE will be the link between the gut microbiota and the host based on the gut–liver axis.
Author Contributions
Conceptualization and drafting, S.-M.W.; resources, S.-M.W., J.-J.J., R.G., H.G., K.K.O., S.P.S., S.J.Y., J.Y.H., M.K.J., H.J.P., B.H.M., S.B.L., M.G.C. and M.R.C.; writing and editing, J.A.E., G.H.K. and D.J.K.; revisions and reviews, K.T.S. and S.-M.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Hallym University Research Fund and the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (NRF-2020R1I1A3073530 and NRF-2020R1A6A1A03043026).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AASLD | American Association for the Study of Liver Diseases |
| AMP | Antimicrobial peptide |
| AHE | Acute episode of overt hepatic encephalopathy |
| EASL | European Association for the Study of the Liver |
| FMT | Fecal microbiota transplantation |
| GABA | γ-aminobutyric acid |
| HCC | hepatocellular carcinoma |
| HE | Hepatic encephalopathy |
| LBP | Lipopolysaccharide-binding protein |
| LGG | Lactobacillus rhamnosus GG |
| LPS | Lipopolysaccharide |
| MELD | Model for End-Stage Liver Disease |
| MHE | Minimal hepatic encephalopathy |
| OCTT | Orocecal transit time |
| OHE | Overt hepatic encephalopathy |
| PAMPs | Pathogen-associated molecular patterns |
| SIBO | Small intestinal bacterial overgrowth |
| SOC | Standard of care |
References
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Saraswat, V.A.; Sharma, B.K.; Sarin, S.K.; Chawla, Y.K.; Butterworth, R.; Duseja, A.; Aggarwal, R.; Amarapurkar, D.; Sharma, P.; et al. Minimal hepatic encephalopathy: Consensus statement of a working party of the Indian National Association for Study of the Liver. J. Gastroenterol. Hepatol. 2010, 25, 1029–1041. [Google Scholar] [CrossRef]
- Prasad, S.; Dhiman, R.K.; Duseja, A.; Chawla, Y.K.; Sharma, A.; Agarwal, R. Lactulose improves cognitive functions and health-related quality of life in patients with cirrhosis who have minimal hepatic encephalopathy. Hepatology 2007, 45, 549–559. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Gillevet, P.M.; Patel, N.R.; Ahluwalia, V.; Ridlon, J.M.; Kettenmann, B.; Schubert, C.M.; Sikaroodi, M.; Heuman, D.M.; Crossey, M.M.; et al. A longitudinal systems biology analysis of lactulose withdrawal in hepatic encephalopathy. Metab. Brain Dis. 2012, 27, 205–215. [Google Scholar] [CrossRef]
- Dhiman, R.K. Gut microbiota, inflammation and hepatic encephalopathy: A puzzle with a solution in sight. J. Clin. Exp. Hepatol. 2012, 2, 207–210. [Google Scholar] [CrossRef]
- Quigley, E.M.; Stanton, C.; Murphy, E.F. The gut microbiota and the liver. Pathophysiological and clinical implications. J. Hepatol. 2013, 58, 1020–1027. [Google Scholar] [CrossRef]
- Bajaj, J.S. The role of microbiota in hepatic encephalopathy. Gut Microbes 2014, 5, 397–403. [Google Scholar] [CrossRef]
- Sturgeon, J.A.; Darnall, B.D.; Kao, M.C.; Mackey, S.C. Physical and psychological correlates of fatigue and physical function: A Collaborative Health Outcomes Information Registry (CHOIR) study. J. Pain 2015, 16, 291–298.e1. [Google Scholar] [CrossRef]
- Guarner, F.; Malagelada, J.R. Gut flora in health and disease. Lancet 2003, 361, 512–519. [Google Scholar] [CrossRef]
- Bajaj, J.S. Review article: The modern management of hepatic encephalopathy. Aliment. Pharmacol. Ther. 2010, 31, 537–547. [Google Scholar] [CrossRef]
- Amodio, P.; Bemeur, C.; Butterworth, R.; Cordoba, J.; Kato, A.; Montagnese, S.; Uribe, M.; Vilstrup, H.; Morgan, M.Y. The nutritional management of hepatic encephalopathy in patients with cirrhosis: International Society for Hepatic Encephalopathy and Nitrogen Metabolism Consensus. Hepatology 2013, 58, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Duan, Z.P.; Ha, D.K.; Bengmark, S.; Kurtovic, J.; Riordan, S.M. Synbiotic modulation of gut flora: Effect on minimal hepatic encephalopathy in patients with cirrhosis. Hepatology 2004, 39, 1441–1449. [Google Scholar] [CrossRef] [PubMed]
- Marlicz, W.; Wunsch, E.; Mydlowska, M.; Milkiewicz, M.; Serwin, K.; Mularczyk, M.; Milkiewicz, P.; Raszeja-Wyszomirska, J. The effect of short term treatment with probiotic VSL#3 on various clinical and biochemical parameters in patients with liver cirrhosis. J. Physiol. Pharmacol. 2016, 67, 867–877. [Google Scholar] [PubMed]
- Hassanein, T.I.; Tofteng, F.; Brown, R.S., Jr.; McGuire, B.; Lynch, P.; Mehta, R.; Larsen, F.S.; Gornbein, J.; Stange, J.; Blei, A.T. Randomized controlled study of extracorporeal albumin dialysis for hepatic encephalopathy in advanced cirrhosis. Hepatology 2007, 46, 1853–1862. [Google Scholar] [CrossRef] [PubMed]
- Pazgan-Simon, M.; Zuwala-Jagiello, J.; Serafinska, S.; Simon, K. Nutrition principles and recommendations in different types of hepatic encephalopathy. Clin. Exp. Hepatol. 2016, 1, 121–126. [Google Scholar] [CrossRef]
- Cho, I.; Blaser, M.J. The human microbiome: At the interface of health and disease. Nat. Rev. Genet. 2012, 13, 260–270. [Google Scholar] [CrossRef]
- Backhed, F.; Ding, H.; Wang, T.; Hooper, L.V.; Koh, G.Y.; Nagy, A.; Semenkovich, C.F.; Gordon, J.I. The gut microbiota as an environmental factor that regulates fat storage. Proc. Natl. Acad. Sci. USA 2004, 101, 15718–15723. [Google Scholar] [CrossRef]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef]
- Zeuzem, S. Gut-liver axis. Int. J. Colorectal. Dis. 2000, 15, 59–82. [Google Scholar] [CrossRef]
- Ridlon, J.M.; Alves, J.M.; Hylemon, P.B.; Bajaj, J.S. Cirrhosis, bile acids and gut microbiota: Unraveling a complex relationship. Gut Microbes 2013, 4, 382–387. [Google Scholar] [CrossRef]
- Butterworth, R.F. Hepatic encephalopathy: A central neuroinflammatory disorder? Hepatology 2011, 53, 1372–1376. [Google Scholar] [CrossRef] [PubMed]
- Shawcross, D.L.; Wright, G.; Olde Damink, S.W.; Jalan, R. Role of ammonia and inflammation in minimal hepatic encephalopathy. Metab. Brain Dis. 2007, 22, 125–138. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Hylemon, P.B.; Sanyal, A.J.; White, M.B.; Monteith, P.; Noble, N.A.; Unser, A.B.; Daita, K.; Fisher, A.R.; et al. Altered profile of human gut microbiome is associated with cirrhosis and its complications. J. Hepatol. 2014, 60, 940–947. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Zhang, X.; Liu, J.; Zhang, Q.; Zhao, Y.; Peng, J.; Feng, Q.; Dai, J.; Sun, S.; et al. Gut Microbial Dysbiosis Is Associated with Altered Hepatic Functions and Serum Metabolites in Chronic Hepatitis B Patients. Front. Microbiol. 2017, 8, 2222. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Thacker, L.R.; Fagan, A.; White, M.B.; Gavis, E.A.; Hylemon, P.B.; Brown, R.; Acharya, C.; Heuman, D.M.; Fuchs, M.; et al. Gut microbial RNA and DNA analysis predicts hospitalizations in cirrhosis. JCI Insight 2018, 3, e98019. [Google Scholar] [CrossRef]
- D’Amico, G.; Morabito, A.; Pagliaro, L.; Marubini, E. Survival and prognostic indicators in compensated and decompensated cirrhosis. Dig. Dis. Sci. 1986, 31, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Ding, A.; Lee, A.; Callender, M.; Loughrey, M.; Quah, S.P.; Dinsmore, W.W. Hepatic encephalopathy as an unusual late complication of transjugular intrahepatic portosystemic shunt insertion for non-cirrhotic portal hypertension caused by nodular regenerative hyperplasia in an HIV-positive patient on highly active antiretroviral therapy. Int. J. STD AIDS 2010, 21, 71–72. [Google Scholar] [CrossRef]
- Butterworth, R.F. Role of circulating neurotoxins in the pathogenesis of hepatic encephalopathy: Potential for improvement following their removal by liver assist devices. Liver Int. 2003, 23 (Suppl. 3), 5–9. [Google Scholar] [CrossRef]
- Cornberg, M.; Tacke, F.; Karlsen, T.H.; European Association for the Study of the Liver. Clinical Practice Guidelines of the European Association for the study of the Liver—Advancing methodology but preserving practicability. J. Hepatol. 2019, 70, 5–7. [Google Scholar] [CrossRef]
- Tajiri, K.; Shimizu, Y. Branched-chain amino acids in liver diseases. Transl. Gastroenterol. Hepatol. 2018, 3, 47. [Google Scholar] [CrossRef]
- Acharya, C.; Bajaj, J.S. Altered Microbiome in Patients with Cirrhosis and Complications. Clin. Gastroenterol. Hepatol. 2019, 17, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Fiati Kenston, S.S.; Song, X.; Li, Z.; Zhao, J. Mechanistic insight, diagnosis, and treatment of ammonia-induced hepatic encephalopathy. J. Gastroenterol. Hepatol. 2019, 34, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, D.R.; Tranah, E.J.; Shawcross, D.L. Pathogenesis of hepatic encephalopathy: Role of ammonia and systemic inflammation. J. Clin. Exp. Hepatol. 2015, 5, S7–S20. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F. Hepatic Encephalopathy. N. Engl. J. Med. 2016, 375, 1660–1670. [Google Scholar] [CrossRef]
- Levitt, D.G.; Levitt, M.D. A model of blood-ammonia homeostasis based on a quantitative analysis of nitrogen metabolism in the multiple organs involved in the production, catabolism, and excretion of ammonia in humans. Clin. Exp. Gastroenterol. 2018, 11, 193–215. [Google Scholar] [CrossRef]
- Sawhney, R.; Jalan, R. Liver: The gut is a key target of therapy in hepatic encephalopathy. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 7–8. [Google Scholar] [CrossRef]
- Wierling, C. Bridging the gap between metabolic liver processes and functional tissue structure by integrated spatiotemporal modeling applied to hepatic ammonia detoxification. Hepatology 2014, 60, 1823–1825. [Google Scholar] [CrossRef]
- Mitchell, S.; Ellingson, C.; Coyne, T.; Hall, L.; Neill, M.; Christian, N.; Higham, C.; Dobrowolski, S.F.; Tuchman, M.; Summar, M.; et al. Genetic variation in the urea cycle: A model resource for investigating key candidate genes for common diseases. Hum. Mutat. 2009, 30, 56–60. [Google Scholar] [CrossRef]
- Fleming, K.E.; Wanless, I.R. Glutamine synthetase expression in activated hepatocyte progenitor cells and loss of hepatocellular expression in congestion and cirrhosis. Liver Int. 2013, 33, 525–534. [Google Scholar] [CrossRef]
- Hansen, B.A.; Vilstrup, H. Increased intestinal hydrolysis of urea in patients with alcoholic cirrhosis. Scand. J. Gastroenterol. 1985, 20, 346–350. [Google Scholar] [CrossRef]
- Blei, A.T. Portal hypertension and its complications. Curr. Opin. Gastroenterol. 2007, 23, 275–282. [Google Scholar] [CrossRef] [PubMed]
- De Franchis, R.; Baveno, V.I.F. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J. Hepatol. 2015, 63, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Takefuta, K.; Senzaki, H.; Shimabukuro, A.; Nishibata, M.; Sato, S.; Nakayashiro, M. Portosystemic shunt with hyperammonemia and high cardiac output as a complication after Fontan surgery. J. Cardiol. Cases 2021, 23, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, K.; Sato, S.; Saito, M.; Terabayashi, H.; Nakayama, T.; Saito, M.; Chin, N.; Iida, S.; Nomura, F.; Okuda, K. Clinical and portal hemodynamic features in cirrhotic patients having a large spontaneous splenorenal and/or gastrorenal shunt. Am. J. Gastroenterol. 1986, 81, 450–455. [Google Scholar]
- Haussinger, D.; Kircheis, G.; Fischer, R.; Schliess, F.; Vom Dahl, S. Hepatic encephalopathy in chronic liver disease: A clinical manifestation of astrocyte swelling and low-grade cerebral edema? J. Hepatol. 2000, 32, 1035–1038. [Google Scholar] [CrossRef]
- Jover, R.; Rodrigo, R.; Felipo, V.; Insausti, R.; Saez-Valero, J.; Garcia-Ayllon, M.S.; Suarez, I.; Candela, A.; Compan, A.; Esteban, A.; et al. Brain edema and inflammatory activation in bile duct ligated rats with diet-induced hyperammonemia: A model of hepatic encephalopathy in cirrhosis. Hepatology 2006, 43, 1257–1266. [Google Scholar] [CrossRef]
- Gorg, B.; Schliess, F.; Haussinger, D. Osmotic and oxidative/nitrosative stress in ammonia toxicity and hepatic encephalopathy. Arch. Biochem. Biophys. 2013, 536, 158–163. [Google Scholar] [CrossRef]
- Raabe, W. Effects of hyperammonemia on neuronal function: NH4+, IPSP and Cl(−)-extrusion. Adv. Exp. Med. Biol. 1993, 341, 71–82. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Hylemon, P.B.; Ridlon, J.M.; Heuman, D.M.; Daita, K.; White, M.B.; Monteith, P.; Noble, N.A.; Sikaroodi, M.; Gillevet, P.M. Colonic mucosal microbiome differs from stool microbiome in cirrhosis and hepatic encephalopathy and is linked to cognition and inflammation. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 303, G675–G685. [Google Scholar] [CrossRef]
- Gupta, A.; Dhiman, R.K.; Kumari, S.; Rana, S.; Agarwal, R.; Duseja, A.; Chawla, Y. Role of small intestinal bacterial overgrowth and delayed gastrointestinal transit time in cirrhotic patients with minimal hepatic encephalopathy. J. Hepatol. 2010, 53, 849–855. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Betrapally, N.S.; Hylemon, P.B.; Heuman, D.M.; Daita, K.; White, M.B.; Unser, A.; Thacker, L.R.; Sanyal, A.J.; Kang, D.J.; et al. Salivary microbiota reflects changes in gut microbiota in cirrhosis with hepatic encephalopathy. Hepatology 2015, 62, 1260–1271. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Heuman, D.M.; Hylemon, P.B.; Sanyal, A.J.; Puri, P.; Sterling, R.K.; Luketic, V.; Stravitz, R.T.; Siddiqui, M.S.; Fuchs, M.; et al. Randomised clinical trial: Lactobacillus GG modulates gut microbiome, metabolome and endotoxemia in patients with cirrhosis. Aliment. Pharmacol. Ther. 2014, 39, 1113–1125. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, R.K.; Rana, B.; Agrawal, S.; Garg, A.; Chopra, M.; Thumburu, K.K.; Khattri, A.; Malhotra, S.; Duseja, A.; Chawla, Y.K. Probiotic VSL#3 reduces liver disease severity and hospitalization in patients with cirrhosis: A randomized, controlled trial. Gastroenterology 2014, 147, 1327–1337.e3. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Kassam, Z.; Fagan, A.; Gavis, E.A.; Liu, E.; Cox, I.J.; Kheradman, R.; Heuman, D.; Wang, J.; Gurry, T.; et al. Fecal microbiota transplant from a rational stool donor improves hepatic encephalopathy: A randomized clinical trial. Hepatology 2017, 66, 1727–1738. [Google Scholar] [CrossRef] [PubMed]
- Gluud, L.L.; Vilstrup, H.; Morgan, M.Y. Non-absorbable disaccharides versus placebo/no intervention and lactulose versus lactitol for the prevention and treatment of hepatic encephalopathy in people with cirrhosis. Cochrane Database Syst. Rev. 2016, 4, CD003044. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Wade, J.B.; Sanyal, A.J. Spectrum of neurocognitive impairment in cirrhosis: Implications for the assessment of hepatic encephalopathy. Hepatology 2009, 50, 2014–2021. [Google Scholar] [CrossRef]
- Montagnese, S.; Amodio, P.; Morgan, M.Y. Methods for diagnosing hepatic encephalopathy in patients with cirrhosis: A multidimensional approach. Metab. Brain Dis. 2004, 19, 281–312. [Google Scholar] [CrossRef]
- Ferenci, P. Hepatic encephalopathy. Gastroenterol. Rep. 2017, 5, 138–147. [Google Scholar] [CrossRef]
- Guerit, J.M.; Amantini, A.; Fischer, C.; Kaplan, P.W.; Mecarelli, O.; Schnitzler, A.; Ubiali, E.; Amodio, P.; members of the I.c.N.I. Neurophysiological investigations of hepatic encephalopathy: ISHEN practice guidelines. Liver Int. 2009, 29, 789–796. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Riggio, O.; Allampati, S.; Prakash, R.; Gioia, S.; Onori, E.; Piazza, N.; Noble, N.A.; White, M.B.; Mullen, K.D. Cognitive dysfunction is associated with poor socioeconomic status in patients with cirrhosis: An international multicenter study. Clin. Gastroenterol. Hepatol. 2013, 11, 1511–1516. [Google Scholar] [CrossRef]
- Ridola, L.; Nardelli, S.; Gioia, S.; Riggio, O. Quality of life in patients with minimal hepatic encephalopathy. World J. Gastroenterol. 2018, 24, 5446–5453. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Pinkerton, S.D.; Sanyal, A.J.; Heuman, D.M. Diagnosis and treatment of minimal hepatic encephalopathy to prevent motor vehicle accidents: A cost-effectiveness analysis. Hepatology 2012, 55, 1164–1171. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C.; Guarner, F.; Madsen, K.; Cabana, M.D.; Gibson, G.; Hentges, E.; Sanders, M.E. Human gut microbiota and its relationship to health and disease. Nutr. Rev. 2011, 69, 392–403. [Google Scholar] [CrossRef]
- Goodrich, J.K.; Di Rienzi, S.C.; Poole, A.C.; Koren, O.; Walters, W.A.; Caporaso, J.G.; Knight, R.; Ley, R.E. Conducting a microbiome study. Cell 2014, 158, 250–262. [Google Scholar] [CrossRef] [PubMed]
- Saboo, K.; Petrakov, N.V.; Shamsaddini, A.; Fagan, A.; Gavis, E.A.; Sikaroodi, M.; McGeorge, S.; Gillevet, P.M.; Iyer, R.K.; Bajaj, J.S. Stool microbiota are superior to saliva in distinguishing cirrhosis and hepatic encephalopathy using machine learning. J. Hepatol. 2022, 76, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Sung, C.M.; Lin, Y.F.; Chen, K.F.; Ke, H.M.; Huang, H.Y.; Gong, Y.N.; Tsai, W.S.; You, J.F.; Lu, M.J.; Cheng, H.T.; et al. Predicting Clinical Outcomes of Cirrhosis Patients with Hepatic Encephalopathy from the Fecal Microbiome. Cell Mol. Gastroenterol. Hepatol. 2019, 8, 301–318.E2. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhai, H.; Geng, J.; Yu, R.; Ren, H.; Fan, H.; Shi, P. Large-scale survey of gut microbiota associated with MHE Via 16S rRNA-based pyrosequencing. Am. J. Gastroenterol. 2013, 108, 1601–1611. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Ridlon, J.M.; Hylemon, P.B.; Thacker, L.R.; Heuman, D.M.; Smith, S.; Sikaroodi, M.; Gillevet, P.M. Linkage of gut microbiome with cognition in hepatic encephalopathy. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 302, G168–G175. [Google Scholar] [CrossRef]
- Xia, X.; Chen, J.; Xia, J.; Wang, B.; Liu, H.; Yang, L.; Wang, Y.; Ling, Z. Role of probiotics in the treatment of minimal hepatic encephalopathy in patients with HBV-induced liver cirrhosis. J. Int. Med. Res. 2018, 46, 3596–3604. [Google Scholar] [CrossRef]
- Lunia, M.K.; Sharma, B.C.; Sharma, P.; Sachdeva, S.; Srivastava, S. Probiotics prevent hepatic encephalopathy in patients with cirrhosis: A randomized controlled trial. Clin. Gastroenterol. Hepatol. 2014, 12, 1003–1008.E1. [Google Scholar] [CrossRef]
- Moratalla, A.; Ampuero, J.; Bellot, P.; Gallego-Duran, R.; Zapater, P.; Roger, M.; Figueruela, B.; Martinez-Moreno, B.; Gonzalez-Navajas, J.M.; Such, J.; et al. Lactulose reduces bacterial DNA translocation, which worsens neurocognitive shape in cirrhotic patients with minimal hepatic encephalopathy. Liver Int. 2017, 37, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Bajaj, J.S.; Wang, J.B.; Shang, J.; Zhou, X.M.; Guo, X.L.; Zhu, X.; Meng, L.N.; Jiang, H.X.; Mi, Y.Q.; et al. Lactulose improves cognition, quality of life, and gut microbiota in minimal hepatic encephalopathy: A multicenter, randomized controlled trial. J. Dig. Dis. 2019, 20, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Woodhouse, C.A.; Patel, V.C.; Singanayagam, A.; Shawcross, D.L. Review article: The gut microbiome as a therapeutic target in the pathogenesis and treatment of chronic liver disease. Aliment. Pharmacol. Ther. 2018, 47, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, M.; Gargante, M.P.; Malaguarnera, G.; Salmeri, M.; Mastrojeni, S.; Rampello, L.; Pennisi, G.; Li Volti, G.; Galvano, F. Bifidobacterium combined with fructo-oligosaccharide versus lactulose in the treatment of patients with hepatic encephalopathy. Eur. J. Gastroenterol. Hepatol. 2010, 22, 199–206. [Google Scholar] [CrossRef]
- Vindigni, S.M.; Surawicz, C.M. Fecal Microbiota Transplantation. Gastroenterol. Clin. N. Am. 2017, 46, 171–185. [Google Scholar] [CrossRef]
- Wang, W.W.; Zhang, Y.; Huang, X.B.; You, N.; Zheng, L.; Li, J. Fecal microbiota transplantation prevents hepatic encephalopathy in rats with carbon tetrachloride-induced acute hepatic dysfunction. World J. Gastroenterol. 2017, 23, 6983–6994. [Google Scholar] [CrossRef]
- Kao, D.; Roach, B.; Park, H.; Hotte, N.; Madsen, K.; Bain, V.; Tandon, P. Fecal microbiota transplantation in the management of hepatic encephalopathy. Hepatology 2016, 63, 339–340. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Salzman, N.H.; Acharya, C.; Sterling, R.K.; White, M.B.; Gavis, E.A.; Fagan, A.; Hayward, M.; Holtz, M.L.; Matherly, S.; et al. Fecal Microbial Transplant Capsules Are Safe in Hepatic Encephalopathy: A Phase 1, Randomized, Placebo-Controlled Trial. Hepatology 2019, 70, 1690–1703. [Google Scholar] [CrossRef]
- Bloom, P.P.; Donlan, J.; Torres Soto, M.; Daidone, M.; Hohmann, E.; Chung, R.T. Fecal microbiota transplant improves cognition in hepatic encephalopathy and its effect varies by donor and recipient. Hepatol. Commun. 2022, 6, 2079–2089. [Google Scholar] [CrossRef]
- Patidar, K.R.; Bajaj, J.S. Antibiotics for the treatment of hepatic encephalopathy. Metab. Brain Dis. 2013, 28, 307–312. [Google Scholar] [CrossRef]
- Zhang, S.; Chen, D.C. Facing a new challenge: The adverse effects of antibiotics on gut microbiota and host immunity. Chin. Med. J. 2019, 132, 1135–1138. [Google Scholar] [CrossRef] [PubMed]
- Rose, C.F.; Amodio, P.; Bajaj, J.S.; Dhiman, R.K.; Montagnese, S.; Taylor-Robinson, S.D.; Vilstrup, H.; Jalan, R. Hepatic encephalopathy: Novel insights into classification, pathophysiology and therapy. J. Hepatol. 2020, 73, 1526–1547. [Google Scholar] [CrossRef] [PubMed]
- Bass, N.M.; Mullen, K.D.; Sanyal, A.; Poordad, F.; Neff, G.; Leevy, C.B.; Sigal, S.; Sheikh, M.Y.; Beavers, K.; Frederick, T.; et al. Rifaximin treatment in hepatic encephalopathy. N. Engl. J. Med. 2010, 362, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Kimer, N.; Krag, A.; Moller, S.; Bendtsen, F.; Gluud, L.L. Systematic review with meta-analysis: The effects of rifaximin in hepatic encephalopathy. Aliment. Pharmacol. Ther. 2014, 40, 123–132. [Google Scholar] [CrossRef]
- Kang, S.H.; Lee, Y.B.; Lee, J.H.; Nam, J.Y.; Chang, Y.; Cho, H.; Yoo, J.J.; Cho, Y.Y.; Cho, E.J.; Yu, S.J.; et al. Rifaximin treatment is associated with reduced risk of cirrhotic complications and prolonged overall survival in patients experiencing hepatic encephalopathy. Aliment. Pharmacol. Ther. 2017, 46, 845–855. [Google Scholar] [CrossRef]
- Kaji, K.; Takaya, H.; Saikawa, S.; Furukawa, M.; Sato, S.; Kawaratani, H.; Kitade, M.; Moriya, K.; Namisaki, T.; Akahane, T.; et al. Rifaximin ameliorates hepatic encephalopathy and endotoxemia without affecting the gut microbiome diversity. World J. Gastroenterol. 2017, 23, 8355–8366. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Sanyal, A.J.; Hylemon, P.B.; Sterling, R.K.; Stravitz, R.T.; Fuchs, M.; Ridlon, J.M.; Daita, K.; Monteith, P.; et al. Modulation of the metabiome by rifaximin in patients with cirrhosis and minimal hepatic encephalopathy. PLoS ONE 2013, 8, e60042. [Google Scholar] [CrossRef]
- Zuo, Z.; Fan, H.; Tang, X.D.; Chen, Y.M.; Xun, L.T.; Li, Y.; Song, Z.J.; Zhai, H.Q. Effect of different treatments and alcohol addiction on gut microbiota in minimal hepatic encephalopathy patients. Exp. Ther. Med. 2017, 14, 4887–4895. [Google Scholar] [CrossRef]
- Suzuki, K.; Endo, R.; Takikawa, Y.; Moriyasu, F.; Aoyagi, Y.; Moriwaki, H.; Terai, S.; Sakaida, I.; Sakai, Y.; Nishiguchi, S.; et al. Efficacy and safety of rifaximin in Japanese patients with hepatic encephalopathy: A phase II/III, multicenter, randomized, evaluator-blinded, active-controlled trial and a phase III, multicenter, open trial. Hepatol. Res. 2018, 48, 411–423. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Suzuki, F.; Imamura, M.; Murashima, N.; Yanase, M.; Mine, T.; Fujisawa, M.; Sato, I.; Yoshiji, H.; Okita, K.; et al. Rifaximin-altered gut microbiota components associated with liver/neuropsychological functions in patients with hepatic encephalopathy: An exploratory data analysis of phase II/III clinical trials. Hepatol. Res. 2019, 49, 404–418. [Google Scholar] [CrossRef]
- Schulz, C.; Schutte, K.; Vilchez-Vargas, R.; Vasapolli, R.; Malfertheiner, P. Long-Term Effect of Rifaximin with and without Lactulose on the Active Bacterial Assemblages in the Proximal Small Bowel and Faeces in Patients with Minimal Hepatic Encephalopathy. Dig. Dis. 2019, 37, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.J.; Kakiyama, G.; Betrapally, N.S.; Herzog, J.; Nittono, H.; Hylemon, P.B.; Zhou, H.; Carroll, I.; Yang, J.; Gillevet, P.M.; et al. Rifaximin Exerts Beneficial Effects Independent of its Ability to Alter Microbiota Composition. Clin. Transl. Gastroenterol. 2016, 7, e187. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Gao, J.; Gillilland, M., 3rd; Wu, X.; Song, I.; Kao, J.Y.; Owyang, C. Rifaximin alters intestinal bacteria and prevents stress-induced gut inflammation and visceral hyperalgesia in rats. Gastroenterology 2014, 146, 484–496.E4. [Google Scholar] [CrossRef] [PubMed]
- Maccaferri, S.; Vitali, B.; Klinder, A.; Kolida, S.; Ndagijimana, M.; Laghi, L.; Calanni, F.; Brigidi, P.; Gibson, G.R.; Costabile, A. Rifaximin modulates the colonic microbiota of patients with Crohn’s disease: An in vitro approach using a continuous culture colonic model system. J. Antimicrob. Chemother. 2010, 65, 2556–2565. [Google Scholar] [CrossRef]
- Riggio, O.; Ridola, L.; Pasquale, C. Hepatic encephalopathy therapy: An overview. World J. Gastrointest. Pharmacol. Ther. 2010, 1, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Campion, D.; Giovo, I.; Ponzo, P.; Saracco, G.M.; Balzola, F.; Alessandria, C. Dietary approach and gut microbiota modulation for chronic hepatic encephalopathy in cirrhosis. World J. Hepatol. 2019, 11, 489–512. [Google Scholar] [CrossRef]
- Fan, Y.; Pedersen, O. Gut microbiota in human metabolic health and disease. Nat. Rev. Microbiol. 2021, 19, 55–71. [Google Scholar] [CrossRef]
- Merli, M.; Iebba, V.; Giusto, M. What is new about diet in hepatic encephalopathy. Metab. Brain Dis. 2016, 31, 1289–1294. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef]
- Summerskill, W.H.; Wolfe, S.J.; Davidson, C.S. The management of hepatic coma in relation to protein withdrawal and certain specific measures. Am. J. Med. 1957, 23, 59–76. [Google Scholar] [CrossRef]
- Cordoba, J.; Lopez-Hellin, J.; Planas, M.; Sabin, P.; Sanpedro, F.; Castro, F.; Esteban, R.; Guardia, J. Normal protein diet for episodic hepatic encephalopathy: Results of a randomized study. J. Hepatol. 2004, 41, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Campollo, O.; Sprengers, D.; Dam, G.; Vilstrup, H.; McIntyre, N. Protein tolerance to standard and high protein meals in patients with liver cirrhosis. World J. Hepatol. 2017, 9, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, T.; Taniguchi, E.; Sata, M. Effects of oral branched-chain amino acids on hepatic encephalopathy and outcome in patients with liver cirrhosis. Nutr. Clin. Pract. 2013, 28, 580–588. [Google Scholar] [CrossRef]
- Plauth, M.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schutz, T.; Bischoff, S.C. ESPEN guideline on clinical nutrition in liver disease. Clin. Nutr. 2019, 38, 485–521. [Google Scholar] [CrossRef] [PubMed]
- Fassarella, M.; Blaak, E.E.; Penders, J.; Nauta, A.; Smidt, H.; Zoetendal, E.G. Gut microbiome stability and resilience: Elucidating the response to perturbations in order to modulate gut health. Gut 2021, 70, 595–605. [Google Scholar] [CrossRef]
- Fukui, H. Role of Gut Dysbiosis in Liver Diseases: What Have We Learned So Far? Diseases 2019, 7, 58. [Google Scholar] [CrossRef]
- Ohtani, N.; Kawada, N. Role of the Gut-Liver Axis in Liver Inflammation, Fibrosis, and Cancer: A Special Focus on the Gut Microbiota Relationship. Hepatol. Commun. 2019, 3, 456–470. [Google Scholar] [CrossRef]
- Mohajeri, M.H.; Brummer, R.J.M.; Rastall, R.A.; Weersma, R.K.; Harmsen, H.J.M.; Faas, M.; Eggersdorfer, M. The role of the microbiome for human health: From basic science to clinical applications. Eur. J. Nutr. 2018, 57, 1–14. [Google Scholar] [CrossRef]
- Sbahi, H.; Di Palma, J.A. Faecal microbiota transplantation: Applications and limitations in treating gastrointestinal disorders. BMJ Open Gastroenterol. 2016, 3, e000087. [Google Scholar] [CrossRef]
- Zellmer, C.; Sater, M.R.A.; Huntley, M.H.; Osman, M.; Olesen, S.W.; Ramakrishna, B. Shiga Toxin-Producing Escherichia coli Transmission via Fecal Microbiota Transplant. Clin. Infect. Dis. 2021, 72, e876–e880. [Google Scholar] [CrossRef]
- DeFilipp, Z.; Bloom, P.P.; Torres Soto, M.; Mansour, M.K.; Sater, M.R.A.; Huntley, M.H.; Turbett, S.; Chung, R.T.; Chen, Y.B.; Hohmann, E.L. Drug-Resistant E. coli Bacteremia Transmitted by Fecal Microbiota Transplant. N. Engl. J. Med. 2019, 381, 2043–2050. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.C.; Yang, Y.S. Fecal microbiota transplantation: Current status and challenges in China. JGH Open 2018, 2, 114–116. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, J.; Prado, V.; Trebicka, J.; Amoros, A.; Gustot, T.; Wiest, R.; Deulofeu, C.; Garcia, E.; Acevedo, J.; Fuhrmann, V.; et al. Multidrug-resistant bacterial infections in patients with decompensated cirrhosis and with acute-on-chronic liver failure in Europe. J. Hepatol. 2019, 70, 398–411. [Google Scholar] [CrossRef] [PubMed]
- Caraceni, P.; Vargas, V.; Sola, E.; Alessandria, C.; De Wit, K.; Trebicka, J.; Angeli, P.; Mookerjee, R.P.; Durand, F.; Pose, E.; et al. The Use of Rifaximin in Patients with Cirrhosis. Hepatology 2021, 74, 1660–1673. [Google Scholar] [CrossRef]
- Kircheis, G.; Nilius, R.; Held, C.; Berndt, H.; Buchner, M.; Gortelmeyer, R.; Hendricks, R.; Kruger, B.; Kuklinski, B.; Meister, H.; et al. Therapeutic efficacy of L-ornithine-L-aspartate infusions in patients with cirrhosis and hepatic encephalopathy: Results of a placebo-controlled, double-blind study. Hepatology 1997, 25, 1351–1360. [Google Scholar] [CrossRef]
- Stauch, S.; Kircheis, G.; Adler, G.; Beckh, K.; Ditschuneit, H.; Gortelmeyer, R.; Hendricks, R.; Heuser, A.; Karoff, C.; Malfertheiner, P.; et al. Oral L-ornithine-L-aspartate therapy of chronic hepatic encephalopathy: Results of a placebo-controlled double-blind study. J. Hepatol. 1998, 28, 856–864. [Google Scholar] [CrossRef]
- Poo, J.L.; Gongora, J.; Sanchez-Avila, F.; Aguilar-Castillo, S.; Garcia-Ramos, G.; Fernandez-Zertuche, M.; Rodriguez-Fragoso, L.; Uribe, M. Efficacy of oral L-ornithine-L-aspartate in cirrhotic patients with hyperammonemic hepatic encephalopathy. Results of a randomized, lactulose-controlled study. Ann. Hepatol. 2006, 5, 281–288. [Google Scholar] [CrossRef]
- Jalan, R.; Wright, G.; Davies, N.A.; Hodges, S.J. L-Ornithine phenylacetate (OP): A novel treatment for hyperammonemia and hepatic encephalopathy. Med. Hypotheses 2007, 69, 1064–1069. [Google Scholar] [CrossRef]
- Efrati, C.; Masini, A.; Merli, M.; Valeriano, V.; Riggio, O. Effect of sodium benzoate on blood ammonia response to oral glutamine challenge in cirrhotic patients: A note of caution. Am. J. Gastroenterol. 2000, 95, 3574–3578. [Google Scholar] [CrossRef]
- Spann, A.; Yasodhara, A.; Kang, J.; Watt, K.; Wang, B.; Goldenberg, A.; Bhat, M. Applying Machine Learning in Liver Disease and Transplantation: A Comprehensive Review. Hepatology 2020, 71, 1093–1105. [Google Scholar] [CrossRef]
- Guarner, C.; Soriano, G. Bacterial translocation and its consequences in patients with cirrhosis. Eur. J. Gastroenterol. Hepatol. 2005, 17, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Scheline, R.R. Metabolism of foreign compounds by gastrointestinal microorganisms. Pharmacol. Rev. 1973, 25, 451–523. [Google Scholar] [PubMed]
- Scheline, R.R. Drug metabolism by intestinal microorganisms. J. Pharm. Sci. 1968, 57, 2021–2037. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, B.; Zhang, M.; Rantalainen, M.; Wang, S.; Zhou, H.; Zhang, Y.; Shen, J.; Pang, X.; Zhang, M.; et al. Symbiotic gut microbes modulate human metabolic phenotypes. Proc. Natl. Acad. Sci. USA 2008, 105, 2117–2122. [Google Scholar] [CrossRef] [PubMed]
- Rubio, T.; Felipo, V.; Tarazona, S.; Pastorelli, R.; Escudero-Garcia, D.; Tosca, J.; Urios, A.; Conesa, A.; Montoliu, C. Multi-omic analysis unveils biological pathways in peripheral immune system associated to minimal hepatic encephalopathy appearance in cirrhotic patients. Sci. Rep. 2021, 11, 1907. [Google Scholar] [CrossRef]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef]
- Nicholson, J.K. Global systems biology, personalized medicine and molecular epidemiology. Mol. Syst. Biol. 2006, 2, 52. [Google Scholar] [CrossRef]
- Gazda, J.; Drotar, P.; Drazilova, S.; Gazda, J.; Gazda, M.; Janicko, M.; Jarcuska, P. Artificial Intelligence and Its Application to Minimal Hepatic Encephalopathy Diagnosis. J. Pers. Med. 2021, 11, 1090. [Google Scholar] [CrossRef]
- Chen, H.J.; Chen, R.; Yang, M.; Teng, G.J.; Herskovits, E.H. Identification of minimal hepatic encephalopathy in patients with cirrhosis based on white matter imaging and Bayesian data mining. AJNR Am. J. Neuroradiol. 2015, 36, 481–487. [Google Scholar] [CrossRef]
- Chen, Q.F.; Zou, T.X.; Yang, Z.T.; Chen, H.J. Identification of patients with and without minimal hepatic encephalopathy based on gray matter volumetry using a support vector machine learning algorithm. Sci. Rep. 2020, 10, 2490. [Google Scholar] [CrossRef]
- Yang, H.; Li, X.; Cao, H.; Cui, Y.; Luo, Y.; Liu, J.; Zhang, Y. Using machine learning methods to predict hepatic encephalopathy in cirrhotic patients with unbalanced data. Comput. Methods Programs Biomed. 2021, 211, 106420. [Google Scholar] [CrossRef] [PubMed]
- Franzosa, E.A.; Huang, K.; Meadow, J.F.; Gevers, D.; Lemon, K.P.; Bohannan, B.J.; Huttenhower, C. Identifying personal microbiomes using metagenomic codes. Proc. Natl. Acad. Sci. USA 2015, 112, E2930–E2938. [Google Scholar] [CrossRef] [PubMed]
- Bloom, P.P.; Tapper, E.B.; Young, V.B.; Lok, A.S. Microbiome therapeutics for hepatic encephalopathy. J. Hepatol. 2021, 75, 1452–1464. [Google Scholar] [CrossRef] [PubMed]
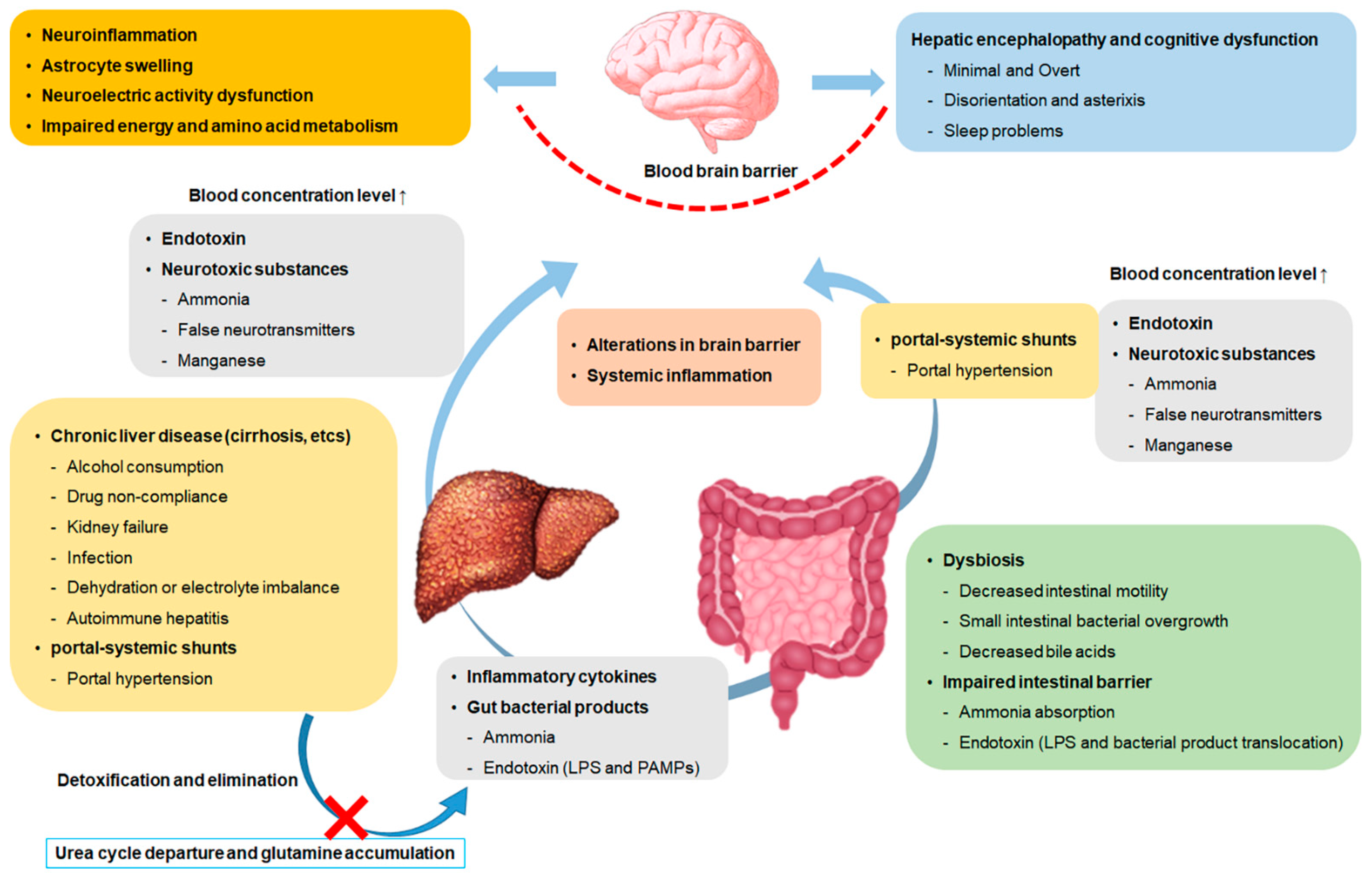
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).