


Do Circulating Redox Biomarkers Have Diagnostic Significance in Alcohol-Intoxicated People?

 ,
,  ,
,  , , ,
, , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
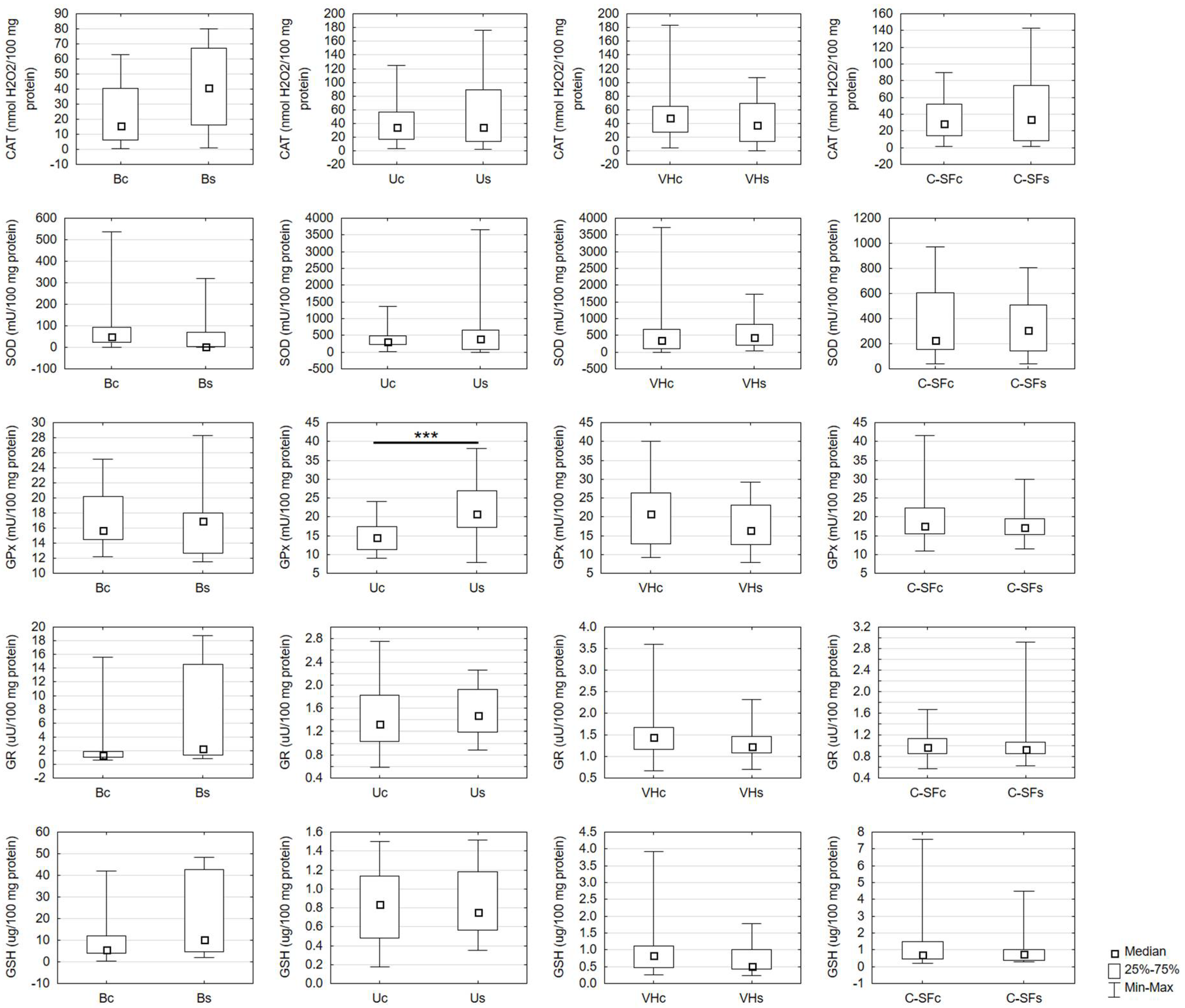
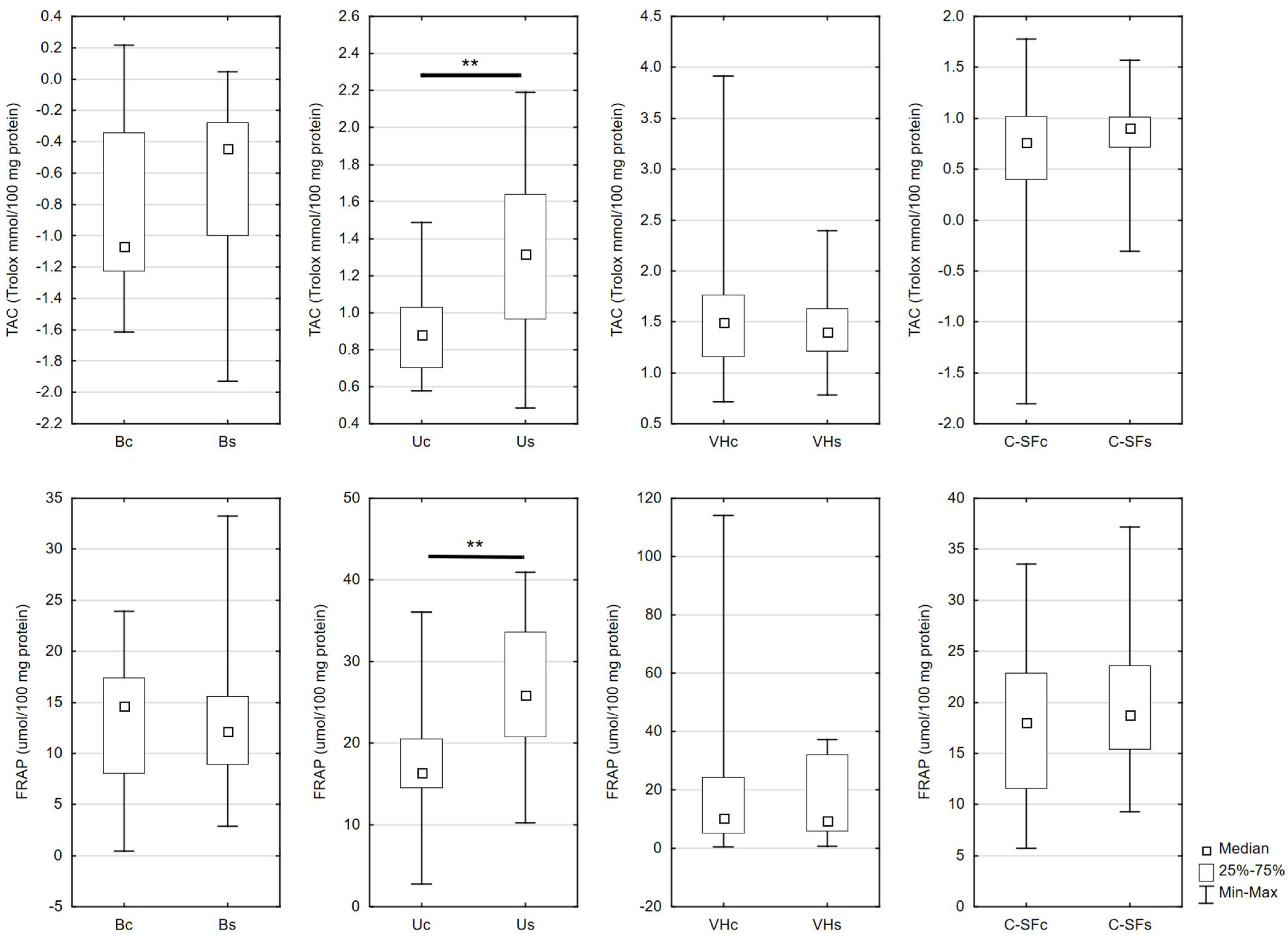
2.1. Antioxidant Assays
2.2. Redox Status Assays
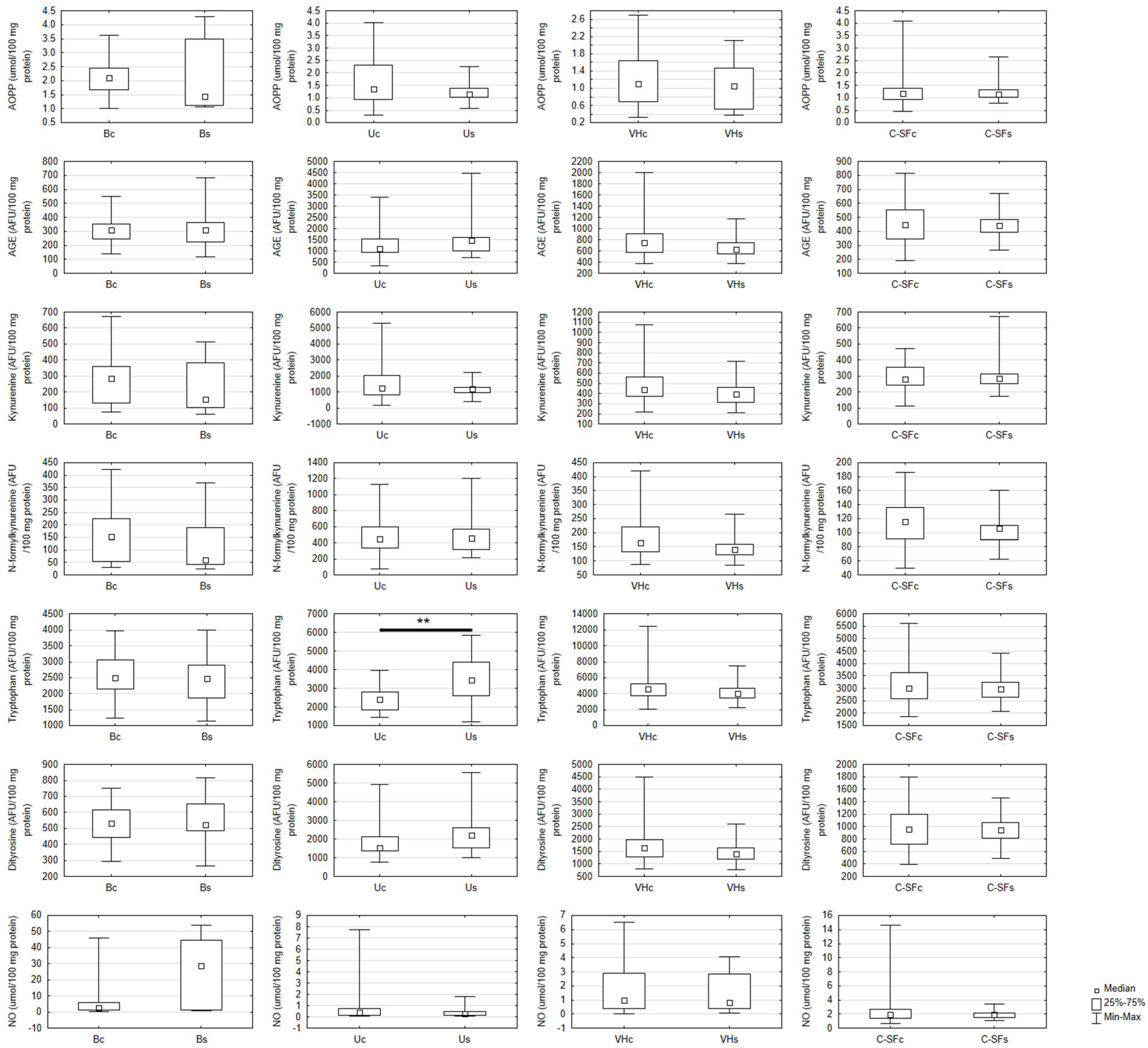
2.3. Oxidative Damage and Nitric Oxide Assays
2.4. Protein Assay
2.5. Correlations
2.6. Multifactorial Linear Regression
3. Discussion
4. Limitations, Strengths and Future Prospects
5. Materials and Methods
5.1. Redox Determinations
5.2. Antioxidant Assays
5.3. Redox Status Assays
5.4. Oxidative Damage Assays
5.5. Nitric Oxide Assay
5.6. Protein Assay
5.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Das, S.K.; Vasudevan, D.M. Alcohol-induced oxidative stress. Life Sci. 2007, 81, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, K.; Suwaki, H. Ethanol metabolism, toxicity and genetic polymorphism. Addict. Biol. 1998, 3, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Zięba, S.; Maciejczyk, M.; Zalewska, A. Ethanol- and Cigarette Smoke-Related Alternations in Oral Redox Homeostasis. Front. Physiol. 2022, 12, 793028. [Google Scholar] [CrossRef] [PubMed]
- Lieber, C.S. Metabolism of alcohol. Clin. Liver Dis. 2005, 9, 1–35. [Google Scholar] [CrossRef]
- Videla, L.A.; Valenzuela, A. Alcohol ingestion, liver glutathione and lipoperoxidation: Metabolic interrelations and pathological implications. Life Sci. 1982, 31, 2395–2407. [Google Scholar] [CrossRef]
- Chen, Y.; Han, M.; Matsumoto, A.; Wang, Y.; Thompson, D.C.; Vasiliou, V. Glutathione and Transsulfuration in Alcohol-Associated Tissue Injury and Carcinogenesis. Alcohol Cancer 2018, 37–53. [Google Scholar]
- Peterson, C.M.; Nguyen, L.B. Clinical implications of acetaldehyde adducts with hemoglobin. Prog. Clin. Biol. Res. 1985, 183, 19–30. [Google Scholar]
- Niemelä, O. Acetaldehyde adducts in circulation. Novartis Found. Symp. 2007, 285, 183–192; discussion 193–197. [Google Scholar] [CrossRef]
- Bondy, S.C. Ethanol toxicity and oxidative stress. Toxicol. Lett. 1992, 63, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Teschke, R. Microsomal Ethanol-Oxidizing System: Success Over 50 Years and an Encouraging Future. Alcohol. Clin. Exp. Res. 2019, 43, 386–400. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhang, T.; Kusumanchi, P.; Han, S.; Yang, Z.; Liangpunsakul, S. Alcohol Metabolizing Enzymes, Microsomal Ethanol Oxidizing System, Cytochrome P450 2E1, Catalase, and Aldehyde Dehydrogenase in Alcohol-Associated Liver Disease. Biomedicines 2020, 8, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albano, E.; French, S.W.; Ingelman-Sundberg, M. Hydroxyethyl radicals in ethanol hepatotoxicity. Front. Biosci. 1999, 4, D533–D540. [Google Scholar] [CrossRef] [PubMed]
- Holford, N.H. Clinical pharmacokinetics of ethanol. Clin. Pharmacokinet. 1987, 13, 273–292. [Google Scholar] [CrossRef] [PubMed]
- Plapp, B.V. Control of alcohol metabolism. EXS 1994, 71, 311–322. [Google Scholar] [CrossRef]
- Wu, D.; Zhai, Q.; Shi, X. Alcohol-induced oxidative stress and cell responses. J. Gastroenterol. Hepatol. 2006, 21, S26–S29. [Google Scholar] [CrossRef]
- Wu, D.; Cederbaum, A.I. Alcohol, oxidative stress, and free radical damage. Alcohol Res. Health 2003, 27, 277–284. [Google Scholar]
- Albano, E. Alcohol, oxidative stress and free radical damage. Proc. Nutr. Soc. 2006, 65, 278–290. [Google Scholar] [CrossRef] [Green Version]
- Halliwell, B. Biochemistry of oxidative stress. Biochem. Soc. Trans. 2007, 35, 1147–1150. [Google Scholar] [CrossRef]
- Yang, H.-Y.; Lee, T.-H. Antioxidant enzymes as redox-based biomarkers: A brief review. BMB Rep. 2015, 48, 200–208. [Google Scholar] [CrossRef] [Green Version]
- Korac, B.; Kalezic, A.; Pekovic-Vaughan, V.; Korac, A.; Jankovic, A. Redox changes in obesity, metabolic syndrome, and diabetes. Redox Biol. 2021, 42, 101887. [Google Scholar] [CrossRef]
- Ryan, B.J.; Nissim, A.; Winyard, P.G. Oxidative post-translational modifications and their involvement in the pathogenesis of autoimmune diseases. Redox Biol. 2014, 2, 715–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejczyk, M.; Zalewska, A.; Gerreth, K. Salivary Redox Biomarkers in Selected Neurodegenerative Diseases. J. Clin. Med. 2020, 9, 497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastore, A.; Petrillo, S.; Piermarini, E.; Piemonte, F. Systemic Redox Biomarkers in Neurodegenerative Diseases. Curr. Drug Metab. 2015, 16, 46–70. [Google Scholar] [CrossRef] [PubMed]
- Raman, D.; Foo, C.H.J.; Clement, M.-V.; Pervaiz, S. Breast Cancer: A Molecular and Redox Snapshot. Antioxid. Redox Signal. 2016, 25, 337–370. [Google Scholar] [CrossRef] [PubMed]
- Tasdogan, A.; Ubellacker, J.M.; Morrison, S.J. Redox Regulation in Cancer Cells during Metastasis. Cancer Discov. 2021, 11, 2682–2692. [Google Scholar] [CrossRef]
- Niki, E. Oxidant-specific biomarkers of oxidative stress. Association with atherosclerosis and implication for antioxidant effects. Free Radic. Biol. Med. 2018, 120, 425–440. [Google Scholar] [CrossRef]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxid. Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef]
- Frijhoff, J.; Winyard, P.G.; Zarkovic, N.; Davies, S.S.; Stocker, R.; Cheng, D.; Knight, A.R.; Taylor, E.L.; Oettrich, J.; Ruskovska, T.; et al. Clinical Relevance of Biomarkers of Oxidative Stress. Antioxid. Redox Signal. 2015, 23, 1144–1170. [Google Scholar] [CrossRef] [Green Version]
- Majno, G.; Joris, I. Apoptosis, oncosis, and necrosis. An overview of cell death. Am. J. Pathol. 1995, 146, 3–15. [Google Scholar]
- Pigaiani, N.; Bertaso, A.; De Palo, E.F.; Bortolotti, F.; Tagliaro, F. Vitreous humor endogenous compounds analysis for post-mortem forensic investigation. Forensic Sci. Int. 2020, 310, 110235. [Google Scholar] [CrossRef]
- Atkin, L.; Rippon, M. Autolysis: Mechanisms of action in the removal of devitalised tissue. Br. J. Nurs. 2016, 25, S40–S47. [Google Scholar] [CrossRef] [PubMed]
- Levine, B.S.; Smith, M.L.; Froede, R.C. Postmortem forensic toxicology. Clin. Lab. Med. 1990, 10, 571–589. [Google Scholar] [PubMed]
- Virkler, K.; Lednev, I.K. Analysis of body fluids for forensic purposes: From laboratory testing to non-destructive rapid confirmatory identification at a crime scene. Forensic Sci. Int. 2009, 188, 1–17. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Han, N.; Ji, C.; Zhao, Y.; Hu, S.; Kong, Q.; Ye, J.; Ji, A.; Sun, Q. Identification of five types of forensic body fluids based on stepwise discriminant analysis. Forensic Sci. Int. Genet. 2020, 48, 102337. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.S.; Lopes, C.; Teixeira, A.L.; Carneiro de Sousa, M.J.; Medeiros, R. Forensic miRNA: Potential biomarker for body fluids? Forensic Sci. Int. Genet. 2015, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- de Beijer, R.P.; de Graaf, C.; van Weert, A.; van Leeuwen, T.G.; Aalders, M.C.G.; van Dam, A. Identification and detection of protein markers to differentiate between forensically relevant body fluids. Forensic Sci. Int. 2018, 290, 196–206. [Google Scholar] [CrossRef]
- Sapan, C.V.; Lundblad, R.L. Review of methods for determination of total protein and peptide concentration in biological samples. PROTEOMICS-Clin. Appl. 2015, 9, 268–276. [Google Scholar] [CrossRef]
- Küting, T.; Madea, B.; Hess, C.; Krämer, M. Comparative Study: Postmortem Long-Term Stability of Endogenous GHB in Cardiac Blood, Femoral Blood, Vitreous Humor, Cerebrospinal Fluid and Urine with and without Sodium Fluoride Stabilization. J. Anal. Toxicol. 2022, 46, 519–527. [Google Scholar] [CrossRef]
- Wallace, M.A. Anatomy and Physiology of the Kidney. AORN J. 1998, 68, 799–820. [Google Scholar] [CrossRef]
- Choromańska, B.; Myśliwiec, P.; Kozłowski, T.; Łuba, M.; Wojskowicz, P.; Dadan, J.; Myśliwiec, H.; Choromańska, K.; Gibała, A.; Starzyńska, A.; et al. Antioxidant Barrier and Oxidative Damage to Proteins, Lipids, and DNA/RNA in Adrenal Tumor Patients. Oxid. Med. Cell. Longev. 2021, 2021, 5543531. [Google Scholar] [CrossRef]
- Gupta, S.; Finelli, R.; Agarwal, A.; Henkel, R. Total antioxidant capacity-Relevance, methods and clinical implications. Andrologia 2021, 53, e13624. [Google Scholar] [CrossRef] [PubMed]
- Benzie, I.F.; Strain, J.J. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: The FRAP assay. Anal. Biochem. 1996, 239, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glantzounis, G.; Tsimoyiannis, E.; Kappas, A.; Galaris, D. Uric Acid and Oxidative Stress. Curr. Pharm. Des. 2005. [Google Scholar] [CrossRef]
- Li, L.; Zhang, Y.; Zeng, C. Update on the epidemiology, genetics, and therapeutic options of hyperuricemia. Am. J. Transl. Res. 2020, 12, 3167–3181. [Google Scholar] [PubMed]
- Danve, A.; Sehra, S.T.; Neogi, T. Role of diet in hyperuricemia and gout. Best Pract. Res. Clin. Rheumatol. 2021, 35, 101723. [Google Scholar] [CrossRef] [PubMed]
- Nieradko-Iwanicka, B. The role of alcohol consumption in pathogenesis of gout. Crit. Rev. Food Sci. Nutr. 2022, 62, 7129–7137. [Google Scholar] [CrossRef]
- Demirci-Çekiç, S.; Özkan, G.; Avan, A.N.; Uzunboy, S.; Çapanoğlu, E.; Apak, R. Biomarkers of Oxidative Stress and Antioxidant Defense. J. Pharm. Biomed. Anal. 2022, 209, 114477. [Google Scholar] [CrossRef]
- Sautin, Y.Y.; Johnson, R.J. Uric Acid: The Oxidant-Antioxidant Paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Maciejczyk, M.; Taranta-Janusz, K.; Wasilewska, A.; Kossakowska, A.; Zalewska, A. A Case-Control Study of Salivary Redox Homeostasis in Hypertensive Children. Can Salivary Uric Acid be a Marker of Hypertension? J. Clin. Med. 2020, 9, 837. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.-H.; Ha, S.-K. Uric Acid Puzzle: Dual Role as Anti-oxidantand Pro-oxidant. Electrolyte Blood Press. 2014, 12, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ponticelli, C.; Podestà, M.A.; Moroni, G. Hyperuricemia as a trigger of immune response in hypertension and chronic kidney disease. Kidney Int. 2020, 98, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.W.; Kim, S.-M.; Kim, Y.G.; Lee, S.-H.; Moon, J.-Y. Uric acid and inflammation in kidney disease. Am. J. Physiol. Renal Physiol. 2020, 318, F1327–F1340. [Google Scholar] [CrossRef] [PubMed]
- Fathallah-Shaykh, S.A.; Cramer, M.T. Uric acid and the kidney. Pediatr. Nephrol. 2014, 29, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Berndt, C.; Jones, D.P. Oxidative Stress. Annu. Rev. Biochem. 2017, 86, 715–748. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Jones, D.P. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat. Rev. Mol. Cell Biol. 2020, 21, 363–383. [Google Scholar] [CrossRef]
- Lushchak, V.I. Free radicals, reactive oxygen species, oxidative stress and its classification. Chem. Biol. Interact. 2014, 12, 1. [Google Scholar] [CrossRef]
- Valacchi, G.; Caccamo, D.; Pelle, E.; De Luca, C. Innovative Approaches in Environmental Medicine: Redox/Detoxification Biomarkers in Environmental Intolerances. Oxid. Med. Cell. Longev. 2013, 2013, 691624. [Google Scholar] [CrossRef]
- Ramezani, A.; Goudarzi, I.; Lashkarboluki, T.; Ghorbanian, M.T.; Abrari, K.; Elahdadi Salmani, M. Role of Oxidative Stress in Ethanol-induced Neurotoxicity in the Developing Cerebellum. Iran. J. Basic Med. Sci. 2012, 15, 965–974. [Google Scholar] [CrossRef]
- Comporti, M.; Signorini, C.; Leoncini, S.; Gardi, C.; Ciccoli, L.; Giardini, A.; Vecchio, D.; Arezzini, B. Ethanol-induced oxidative stress: Basic knowledge. Genes Nutr. 2010, 5, 101–109. [Google Scholar] [CrossRef] [Green Version]
- Juszka, K.; Juszka, K. A researcher’s review of adherence to forensic examination principles in homicide cases in Poland. Arch. Forensic Med. Criminol. 2015, 4, 214–224. [Google Scholar] [CrossRef]
- Aebi, H. Catalase in vitro. In Methods in Enzymology; Elsevier: Amsterdam, The Netherlands, 1984; Volume 105, pp. 121–126. ISBN 9780121820053. [Google Scholar]
- Misra, H.P.; Fridovich, I. The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J. Biol. Chem. 1972, 247, 3170–3175. [Google Scholar] [CrossRef]
- Paglia, D.E.; Valentine, W.N. Studies on the quantitative and qualitative characterization of erythrocyte glutathione peroxidase. J. Lab. Clin. Med. 1967, 70, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Moron, M.; Depierre, J.; Mannervik, B. Levels of glutathione, glutathione reductase and glutathione S-transferase activities in rat lung and liver. Biochim. Biophys. Acta-Gen. Subj. 1979, 582, 67–78. [Google Scholar] [CrossRef]
- Erel, O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin. Biochem. 2004, 37, 277–285. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Szulimowska, J.; Taranta-Janusz, K.; Werbel, K.; Wasilewska, A.; Zalewska, A. Salivary FRAP as A Marker of Chronic Kidney Disease Progression in Children. Antioxidants 2019, 8, 409. [Google Scholar] [CrossRef] [Green Version]
- Kalousová, M.; Skrha, J.; Zima, T. Advanced glycation end-products and advanced oxidation protein products in patients with diabetes mellitus. Physiol. Res. 2002, 51, 597–604. [Google Scholar]
- Maciejczyk, M.; Zalewska, A.; Gryciuk, M.; Hodun, K.; Czuba, M.; Płoszczyca, K.; Charmas, M.; Sadowski, J.; Baranowski, M. Effect of Normobaric Hypoxia on Alterations in Redox Homeostasis, Nitrosative Stress, Inflammation, and Lysosomal Function following Acute Physical Exercise. Oxid. Med. Cell. Longev. 2022, 2022, 4048543. [Google Scholar] [CrossRef]
- Drygalski, K.; Fereniec, E.; Zalewska, A.; Krętowski, A.; Żendzian-Piotrowska, M.; Maciejczyk, M. Phloroglucinol prevents albumin glycation as well as diminishes ROS production, glycooxidative damage, nitrosative stress and inflammation in hepatocytes treated with high glucose. Biomed. Pharmacother. 2021, 142, 111958. [Google Scholar] [CrossRef]
- Zińczuk, J.; Zaręba, K.; Kamińska, J.; Koper-Lenkiewicz, O.M.; Dymicka-Piekarska, V.; Pryczynicz, A.; Guzińska-Ustymowicz, K.; Kędra, B.; Matowicka-Karna, J.; Żendzian-Piotrowska, M.; et al. Association of Tumour Microenvironment with Protein Glycooxidation, DNA Damage, and Nitrosative Stress in Colorectal Cancer. Cancer Manag. Res. 2021, 13, 6329–6348. [Google Scholar] [CrossRef]
- Grisham, M.B.; Johnson, G.G.; Lancaster, J.R. Quantitation of nitrate and nitrite in extracellular fluids. Methods Enzymol. 1996, 268, 237–246. [Google Scholar] [CrossRef]
- Choromańska, B.; Myśliwiec, P.; Kozłowski, T.; Łuba, M.; Wojskowicz, P.; Dadan, J.; Myśliwiec, H.; Choromańska, K.; Makarewicz, K.; Zalewska, A.; et al. Cross-Talk Between Nitrosative Stress, Inflammation and Hypoxia-Inducible Factor in Patients with Adrenal Masses. J. Inflamm. Res. 2021, 14, 6317–6330. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maciejczyk, M.; Ptaszyńska-Sarosiek, I.; Niemcunowicz-Janica, A.; Szeremeta, M.; Waszkiewicz, N.; Kułak-Bejda, A.; Cwalina, U.; Nesterowicz, M.; Zalewska, A. Do Circulating Redox Biomarkers Have Diagnostic Significance in Alcohol-Intoxicated People? Int. J. Mol. Sci. 2022, 23, 11808. https://doi.org/10.3390/ijms231911808
Maciejczyk M, Ptaszyńska-Sarosiek I, Niemcunowicz-Janica A, Szeremeta M, Waszkiewicz N, Kułak-Bejda A, Cwalina U, Nesterowicz M, Zalewska A. Do Circulating Redox Biomarkers Have Diagnostic Significance in Alcohol-Intoxicated People? International Journal of Molecular Sciences. 2022; 23(19):11808. https://doi.org/10.3390/ijms231911808
Chicago/Turabian StyleMaciejczyk, Mateusz, Iwona Ptaszyńska-Sarosiek, Anna Niemcunowicz-Janica, Michał Szeremeta, Napoleon Waszkiewicz, Agnieszka Kułak-Bejda, Urszula Cwalina, Miłosz Nesterowicz, and Anna Zalewska. 2022. "Do Circulating Redox Biomarkers Have Diagnostic Significance in Alcohol-Intoxicated People?" International Journal of Molecular Sciences 23, no. 19: 11808. https://doi.org/10.3390/ijms231911808
APA StyleMaciejczyk, M., Ptaszyńska-Sarosiek, I., Niemcunowicz-Janica, A., Szeremeta, M., Waszkiewicz, N., Kułak-Bejda, A., Cwalina, U., Nesterowicz, M., & Zalewska, A. (2022). Do Circulating Redox Biomarkers Have Diagnostic Significance in Alcohol-Intoxicated People? International Journal of Molecular Sciences, 23(19), 11808. https://doi.org/10.3390/ijms231911808