
Reduced Percentage of CD14dimCD16+SLAN+ Monocytes Producing TNF and IL-12 as an Immunological Sign of CLL Progression

 , , and
, , and
Abstract
:1. Introduction
2. Results
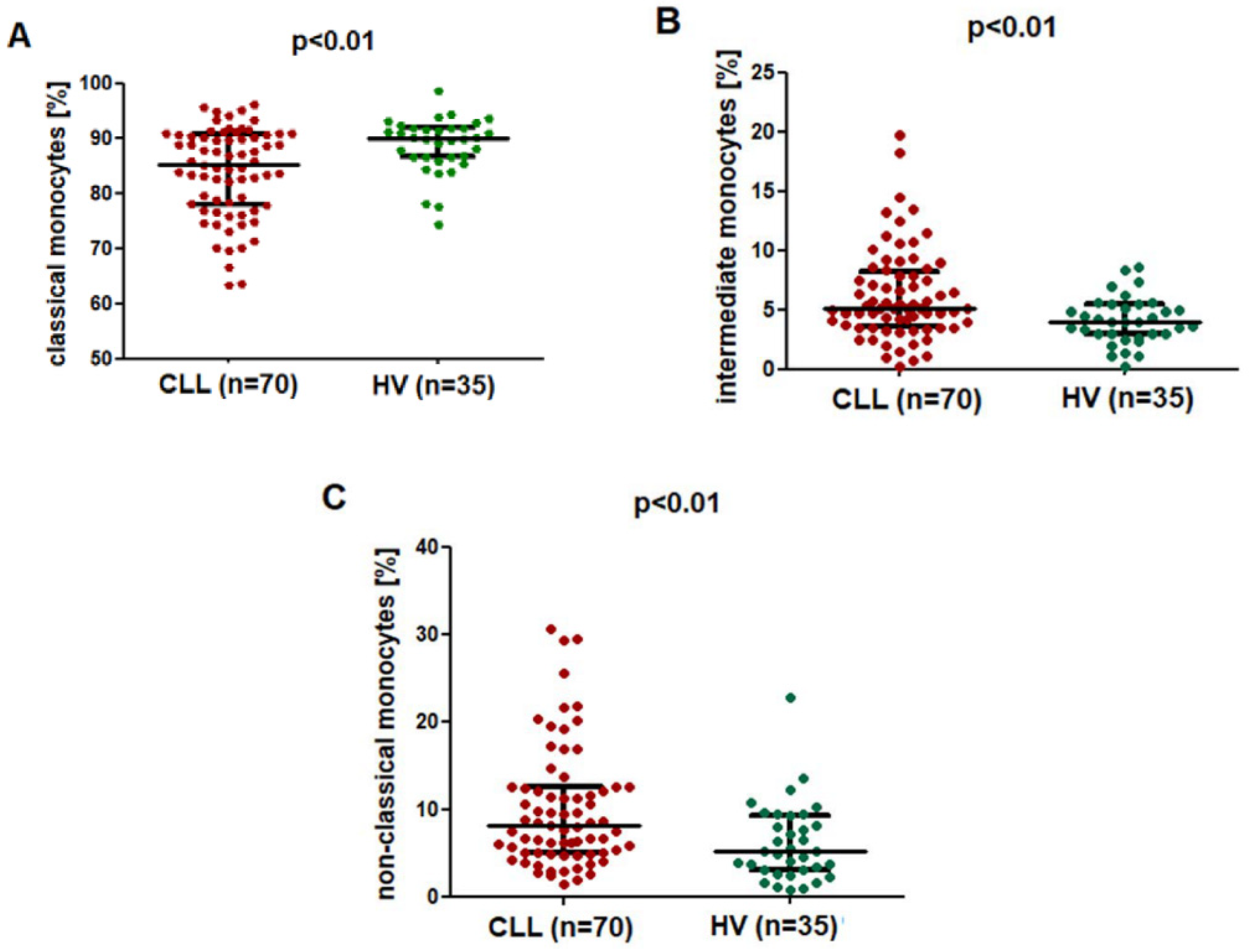
2.1. The Percentage of the SLAN-Positive and SLAN-Negative CD16+ Monocytes Is Increased in CLL
2.2. SLAN-Positive Monocytes Percentage Decreases with Disease Progression
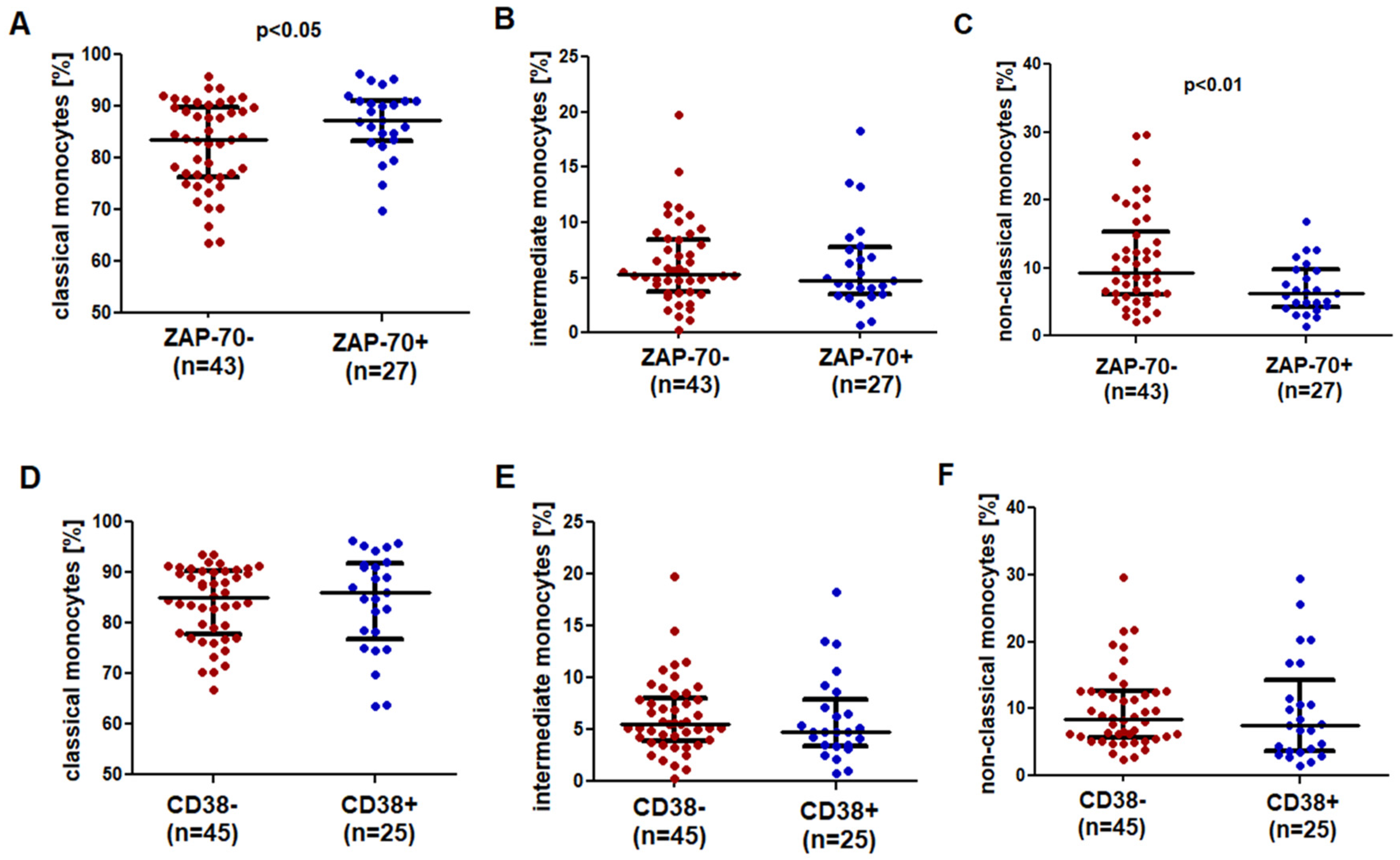
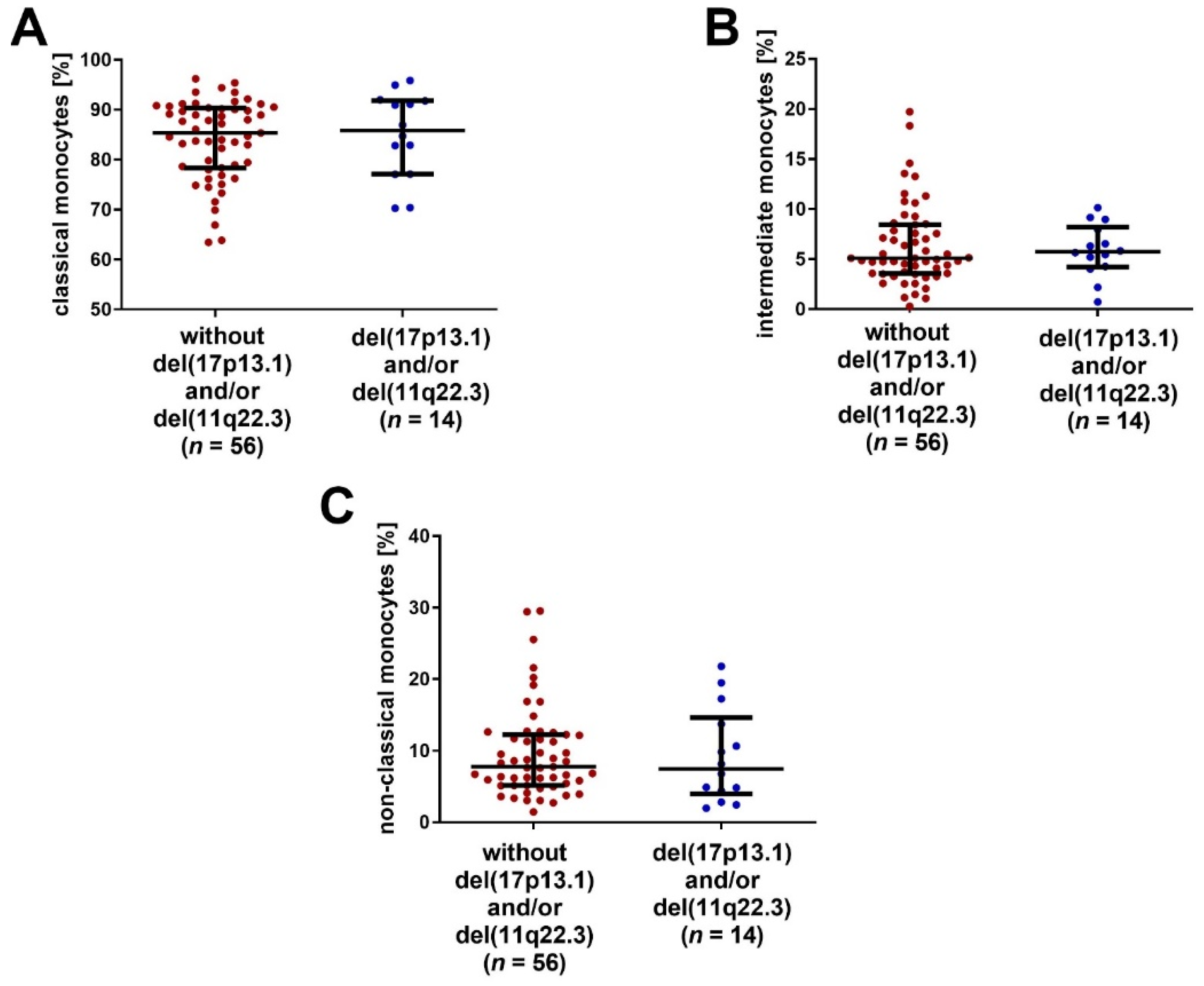
2.3. SLAN-Positive Monocytes Are Less Numerous in CLL Patients with Negative Prognostic Factors
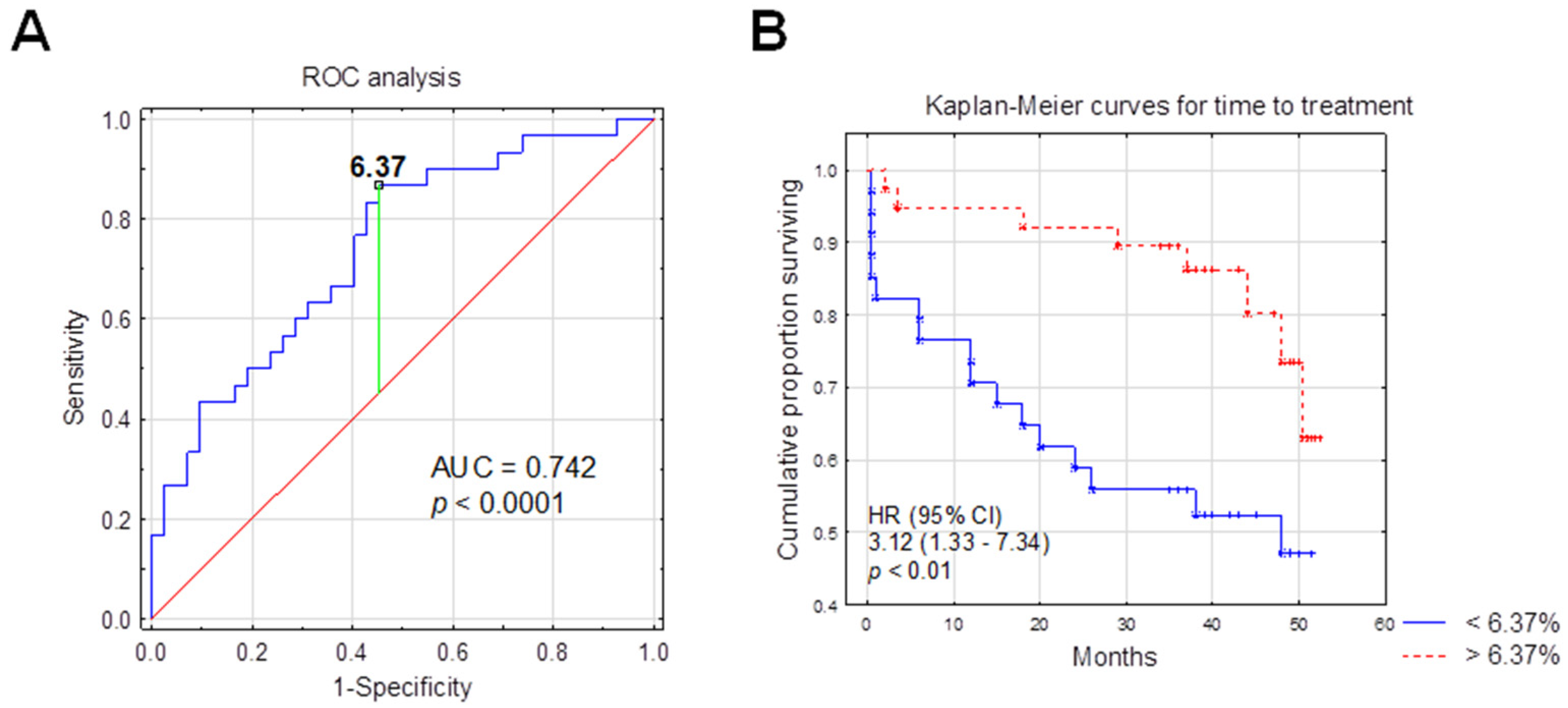
2.4. SLAN-Positive Monocyte Subpopulation Was Decreased in CLL Patients Who Require Therapy
2.5. The Percentage of SLAN-Positive Monocyte Subpopulations and the Time-to-Treatment
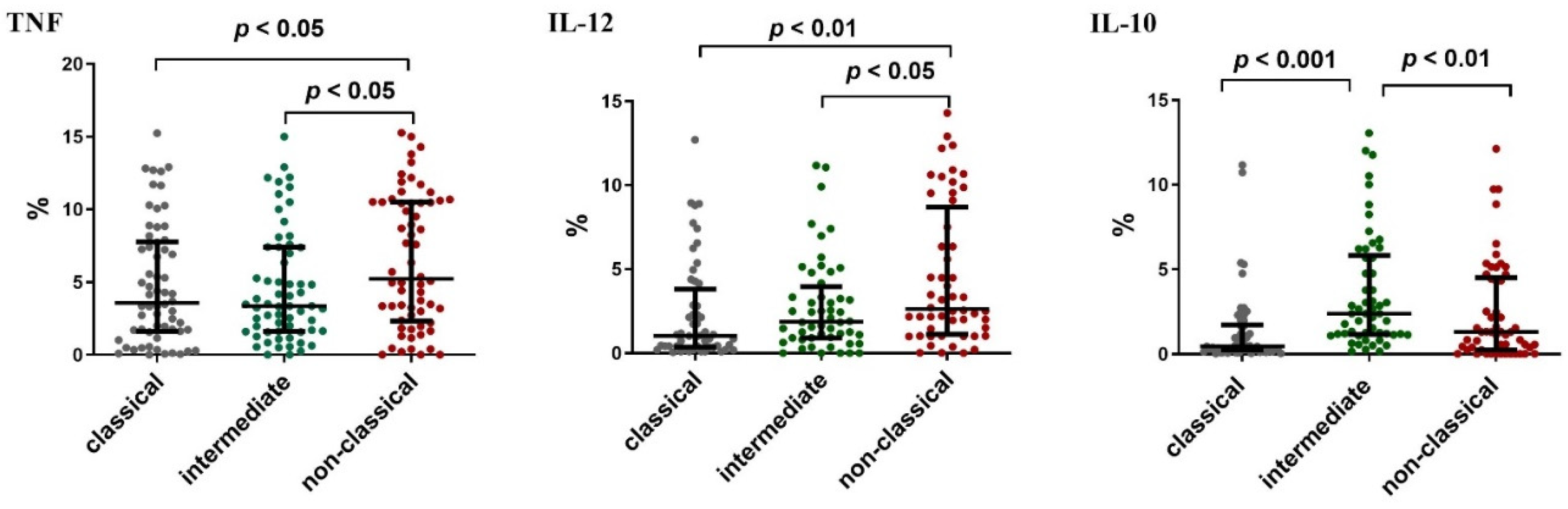
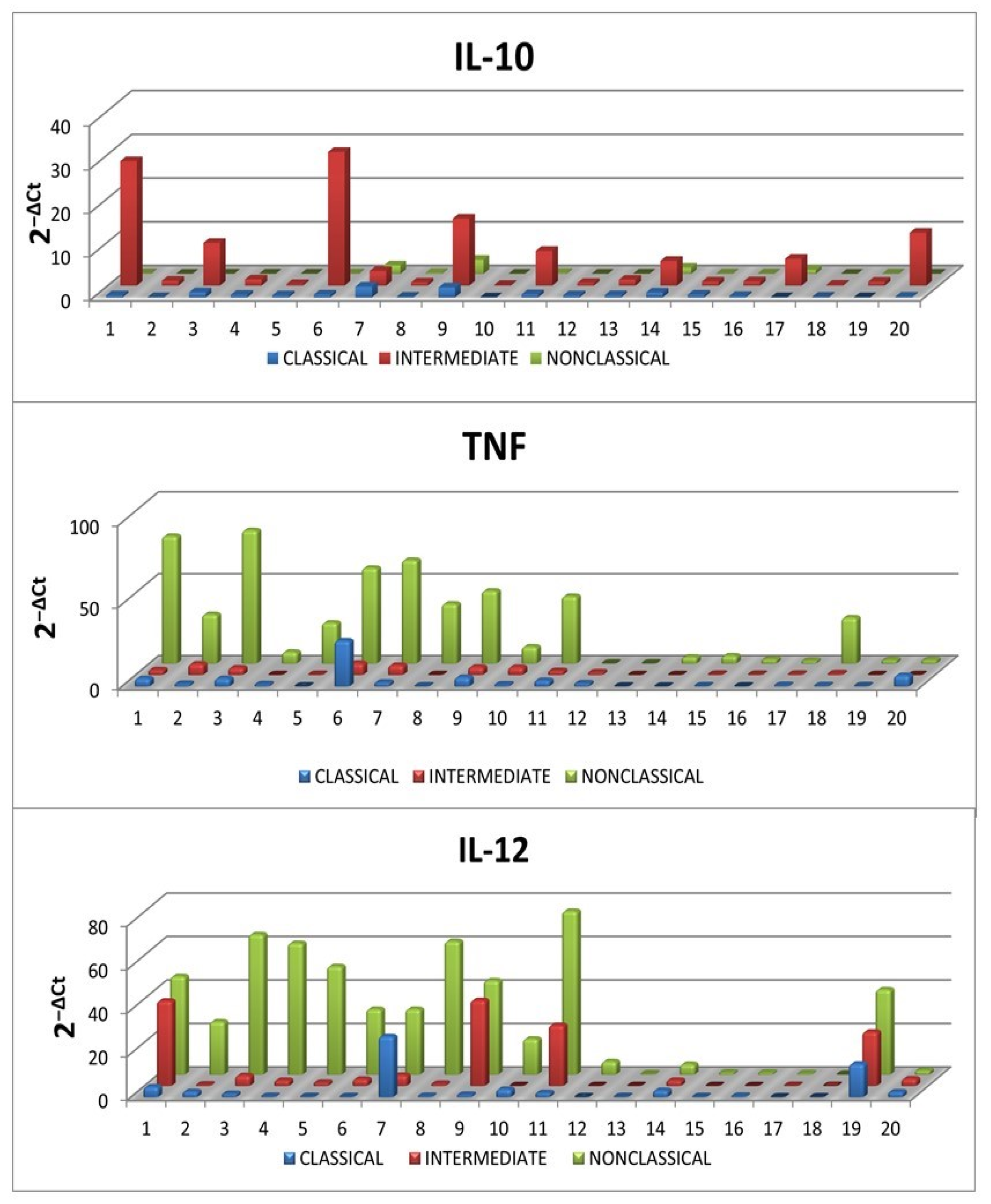
2.6. Intracellular Expression of Cytokines in SLAN-Positive and SLAN-Negative Monocytes
3. Discussion
4. Materials and Methods
4.1. Study and Control Groups
4.2. Ethical Approval
4.3. Isolation of Peripheral Blood Mononuclear Cells (PBMC)
4.4. Flow Cytometry Analysis of Cell Viability
4.5. Flow Cytometry Analysis of Subpopulations of Monocytes
4.6. Analysis of Intracellular Expression TNF, IL-12, IL-10 in SLAN-Positive and SLAN-Negative Monocytes
4.7. SLAN-Positive and SLAN-Negative Monocytes Sorting for RT-qPCR
4.8. RT-qPCR for TNF, IL-12 and IL-10
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mandl, M.; Schmitz, S.; Weber, C.; Hristov, M. Characterization of the CD14++CD16+ Monocyte Population in Human Bone Marrow. PLoS ONE 2014, 9, e112140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler-Heitbrock, L.; Ancuta, P.; Crowe, S.; Dalod, M.; Grau, V.; Hart, D.N.; Leenen, P.J.M.; Liu, Y.-J.; MacPherson, G.; Randolph, G.J.; et al. Nomenclature of Monocytes and Dendritic Cells in Blood. Blood 2010, 116, e74–e80. [Google Scholar] [CrossRef] [PubMed]
- Saha, P.; Geissmann, F. Toward a Functional Characterization of Blood Monocytes. Immunol. Cell Biol. 2011, 89, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Ziegler-Heitbrock, H.W.L.; Ulevitch, R.J. CD14: Cell Surface Receptor and Differentiation Marker. Immunol. Today 1993, 14, 121–125. [Google Scholar] [CrossRef]
- Nimmerjahn, F.; Ravetch, J.V. Fcγ Receptors: Old Friends and New Family Members. Immunity 2006, 24, 19–28. [Google Scholar] [CrossRef] [Green Version]
- Wacleche, V.; Tremblay, C.; Routy, J.-P.; Ancuta, P. The Biology of Monocytes and Dendritic Cells: Contribution to HIV Pathogenesis. Viruses 2018, 10, 65. [Google Scholar] [CrossRef] [Green Version]
- Yeap, W.H.; Wong, K.L.; Shimasaki, N.; Teo, E.C.Y.; Quek, J.K.S.; Yong, H.X.; Diong, C.P.; Bertoletti, A.; Linn, Y.C.; Wong, S.C. CD16 Is Indispensable for Antibody-Dependent Cellular Cytotoxicity by Human Monocytes. Sci. Rep. 2016, 6, 34310. [Google Scholar] [CrossRef]
- Futosi, K.; Fodor, S.; Mócsai, A. Reprint of Neutrophil Cell Surface Receptors and Their Intracellular Signal Transduction Pathways. Int. Immunopharmacol. 2013, 17, 1185–1197. [Google Scholar] [CrossRef]
- Parihar, A.; Eubank, T.D.; Doseff, A.I. Monocytes and Macrophages Regulate Immunity through Dynamic Networks of Survival and Cell Death. J. Innate Immun. 2010, 2, 204–215. [Google Scholar] [CrossRef] [Green Version]
- Ziegler-Heitbrock, L. Blood Monocytes and Their Subsets: Established Features and Open Questions. Front. Immunol. 2015, 6. [Google Scholar] [CrossRef]
- Doseff, A.; Parihar, A. Monocyte Subsets and Their Role in Tumor Progression. In Tumor Microenvironment and Myelomonocytic Cells; Biswas, S., Ed.; InTech: London, UK, 2012; ISBN 978-953-51-0439-1. [Google Scholar]
- Ancuta, P. A Slan-Based Nomenclature for Monocytes? Blood 2015, 126, 2536–2538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofer, T.P.; Zawada, A.M.; Frankenberger, M.; Skokann, K.; Satzl, A.A.; Gesierich, W.; Schuberth, M.; Levin, J.; Danek, A.; Rotter, B.; et al. Slan-Defined Subsets of CD16-Positive Monocytes: Impact of Granulomatous Inflammation and M-CSF Receptor Mutation. Blood 2015, 126, 2601–2610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffei, R.; Bulgarelli, J.; Fiorcari, S.; Bertoncelli, L.; Martinelli, S.; Guarnotta, C.; Castelli, I.; Deaglio, S.; Debbia, G.; De Biasi, S.; et al. The Monocytic Population in Chronic Lymphocytic Leukemia Shows Altered Composition and Deregulation of Genes Involved in Phagocytosis and Inflammation. Haematologica 2013, 98, 1115–1123. [Google Scholar] [CrossRef]
- Damasceno, D.; Andrés, M.P.; van den Bossche, W.B.; Flores-Montero, J.; de Bruin, S.; Teodosio, C.; van Dongen, J.J.; Orfao, A.; Almeida, J. Expression Profile of Novel Cell Surface Molecules on Different Subsets of Human Peripheral Blood Antigen-Presenting Cells. Clin. Transl. Immunol. 2016, 5, e100. [Google Scholar] [CrossRef] [PubMed]
- Cros, J.; Cagnard, N.; Woollard, K.; Patey, N.; Zhang, S.-Y.; Senechal, B.; Puel, A.; Biswas, S.K.; Moshous, D.; Picard, C.; et al. Human CD14dim Monocytes Patrol and Sense Nucleic Acids and Viruses via TLR7 and TLR8 Receptors. Immunity 2010, 33, 375–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherjee, R.; Kanti Barman, P.; Kumar Thatoi, P.; Tripathy, R.; Kumar Das, B.; Ravindran, B. Non-Classical Monocytes Display Inflammatory Features: Validation in Sepsis and Systemic Lupus Erythematous. Sci. Rep. 2015, 5, 13886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, K.L.; Tai, J.J.-Y.; Wong, W.-C.; Han, H.; Sem, X.; Yeap, W.-H.; Kourilsky, P.; Wong, S.-C. Gene Expression Profiling Reveals the Defining Features of the Classical, Intermediate, and Nonclassical Human Monocyte Subsets. Blood 2011, 118, e16–e31. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, F.; Döbel, T.; Schmitz, M.; Schäkel, K. Current Concepts on 6-Sulfo LacNAc Expressing Monocytes (SlanMo). Front. Immunol. 2019, 10, 948. [Google Scholar] [CrossRef]
- Vermi, W.; Micheletti, A.; Finotti, G.; Tecchio, C.; Calzetti, F.; Costa, S.; Bugatti, M.; Calza, S.; Agostinelli, C.; Pileri, S.; et al. Slan+ Monocytes and Macrophages Mediate CD20-Dependent B Cell Lymphoma Elimination via ADCC and ADCP. Cancer Res. 2018, 78, 3544–3559. [Google Scholar] [CrossRef] [Green Version]
- Ożańska, A.; Szymczak, D.; Rybka, J. Pattern of Human Monocyte Subpopulations in Health and Disease. Scand. J. Immunol. 2020, 92, e12883. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, Inflammation, and Cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landskron, G.; De la Fuente, M.; Thuwajit, P.; Thuwajit, C.; Hermoso, M.A. Chronic Inflammation and Cytokines in the Tumor Microenvironment. J. Immunol. Res. 2014, 2014, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallek, M.; Cheson, B.D.; Catovsky, D.; Caligaris-Cappio, F.; Dighiero, G.; Döhner, H.; Hillmen, P.; Keating, M.J.; Montserrat, E.; Rai, K.R.; et al. Guidelines for the Diagnosis and Treatment of Chronic Lymphocytic Leukemia: A Report from the International Workshop on Chronic Lymphocytic Leukemia Updating the National Cancer Institute–Working Group 1996 Guidelines. Blood 2008, 111, 5446–5456. [Google Scholar] [CrossRef] [Green Version]
- Rai, K.R.; Sawitsky, A.; Cronkite, E.; Chanana, A.; Levy, R.; Pasternack, B. Clinical Staging of Chronic Lymphocytic Leukemia. Blood 1975, 46, 219–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rai, K.R. A critical analysis of staging in CLL. In Chronic Lymphocytic Leukemia. Recent Progress and Future Direction; Alan R Liss: New York, NY, USA, 1987; pp. 253–264. [Google Scholar]
- Zarobkiewicz, M.; Kowalska, W.; Chocholska, S.; Tomczak, W.; Szymańska, A.; Morawska, I.; Wojciechowska, A.; Bojarska-Junak, A. High M-MDSC Percentage as a Negative Prognostic Factor in Chronic Lymphocytic Leukaemia. Cancers 2020, 12, 2614. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients | nMohigh (>6.37%) | nMolow (<6.37%) | |
|---|---|---|---|---|
| No. of patients | 70 | 37 | 33 | |
| Sex | Female * | 26 (37.14) | 9 (24.32) | 17 (51.52) |
| Male * | 44 (62.86) | 28 (75.68) | 16 (48.48) | |
| Risk groups | Low-risk (Stage 0) * | 28 (40.00) | 17 (45.95) | 11 (33.33) |
| Intermediate-risk (Stage I–II) * | 34 (48.57) | 15 (40.54) | 19 (57.58) | |
| High-risk (Stages III–IV) * | 8 (11.43) | 5 (13.51) | 3 (9.09) | |
| ZAP-70 (cut off 20%) a | ZAP-70-positive * | 27 (38.57) | 12 (32.43) | 15 (45.45) |
| ZAP-70-negative * | 43 (61.43) | 25 (67.57) | 18 (54.55) | |
| CD38 (cut off 30%) b | CD38-positive * | 25 (35.71) | 13 (35.14) | 12 (36.36) |
| CD38-negative * | 45 (64.29) | 24 (64.86) | 21 (63.64) | |
| Cytogenetic aberrations | del(11q22.3) or/and del(17p13.1) * | 14 (20.59) | 8 (21.62) | 6 (18.18) |
| Without del(11q22.3) or/and del(17p13.1) * | 56 (79.41) | 29 (78.38) | 27 (81.82) | |
| Patients requiring treatment * | 24 (34.29) | 8 (21.62) | 16 (44.48) | |
| Untreated patients * | 46 (65.71) | 29 (78.38) | 17 (51.52) | |
| WBC count (G/L) # | 26.03 (10.11–194.54) | 24.39 (10.11–114.84) $ | 35.18 (13.39–194.54) $ | |
| LYMPH (G/1) # | 19.38 (5.51–181.09) | 18.60 (5.51–109.55) $ | 30.87 (9.57–181.09) $ | |
| LDH (IU/L) # | 373 (231–618) | 356 (266–533) | 383 (231–68) | |
| Hemoglobin (g/dL) # | 13.95 (8.00–17.20) | 14.30 (11.30–16.10) | 13.70 (8.10–17.20) | |
| PLT (G/L) # | 189.00 (49.00–525.00) | 189 (49–525) | 180 (90–399) | |
| β2M (mg/dl) # | 2.35 (1.36–12.37) | 2.29 (1.45–6.04) | 2.54 (1.36–12.37) | |
| % cells CD19+/CD5+/ZAP-70+ a # | 15.84 (0.21–59.05) | 12.20 (1.58–59.05) $ | 17.15 (0.21–56.21) $ | |
| % cells CD19+/CD5+/CD38+ b # | 10.18 (0.22–80.90) | 10.11 (0.66–80.90) | 9.92 (0.22–79.98) |
| Univariate | Multivariate | ||||
|---|---|---|---|---|---|
| Variable | Median TTT (Months) | HR (95% CI) | p | HR (95% CI) | p |
| ZAP-70 | |||||
| ≥20% | 37 | 2.89 (1.27–6.57) | <0.01 | 1.23 (0.35–4.52) | 0.79 |
| <20% | 30 | ||||
| CD38 | |||||
| ≥30% | 37 | 2.81 (1.26–6.22) | <0.01 | 1.88 (0.56–6,37) | 0.308 |
| <30% | 29 | ||||
| β2M | |||||
| ≥3.5 mg/dL | 39 | 4.94 (2.06–11.86) | <0.001 | 5.83 (2.13–15.926) | <0.001 |
| <3.5 mg/dL | 29 | ||||
| del(17p13.1) or del(11q22.3) | |||||
| Positive | 34 | 0,82 (0.18–3.56) | 0.392 | ||
| Negative | 47 | ||||
| nMolow | |||||
| ≥6.37% | 35 | 3.12 (1.33–7.34) | <0.01 | 2.26 (0.98–5.23) | 0.055 |
| >6.37% | 39 | ||||
| Age | |||||
| ≥65 years | 44 | 0.96 (0.43–2.16) | 0.360 | ||
| <65 years | 47 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalska, W.; Zarobkiewicz, M.; Tomczak, W.; Woś, J.; Morawska, I.; Bojarska-Junak, A. Reduced Percentage of CD14dimCD16+SLAN+ Monocytes Producing TNF and IL-12 as an Immunological Sign of CLL Progression. Int. J. Mol. Sci. 2022, 23, 3029. https://doi.org/10.3390/ijms23063029
Kowalska W, Zarobkiewicz M, Tomczak W, Woś J, Morawska I, Bojarska-Junak A. Reduced Percentage of CD14dimCD16+SLAN+ Monocytes Producing TNF and IL-12 as an Immunological Sign of CLL Progression. International Journal of Molecular Sciences. 2022; 23(6):3029. https://doi.org/10.3390/ijms23063029
Chicago/Turabian StyleKowalska, Wioleta, Michał Zarobkiewicz, Waldemar Tomczak, Justyna Woś, Izabela Morawska, and Agnieszka Bojarska-Junak. 2022. "Reduced Percentage of CD14dimCD16+SLAN+ Monocytes Producing TNF and IL-12 as an Immunological Sign of CLL Progression" International Journal of Molecular Sciences 23, no. 6: 3029. https://doi.org/10.3390/ijms23063029