
Comparative Efficacy and Safety of P2Y12 Inhibitor Monotherapy and Dual Antiplatelet Therapy in Patients with and without Diabetes Mellitus Undergoing Percutaneous Coronary Intervention

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Study Selection
2.2. Data Extraction and Main Outcomes
2.3. Statistical Analysis
3. Results
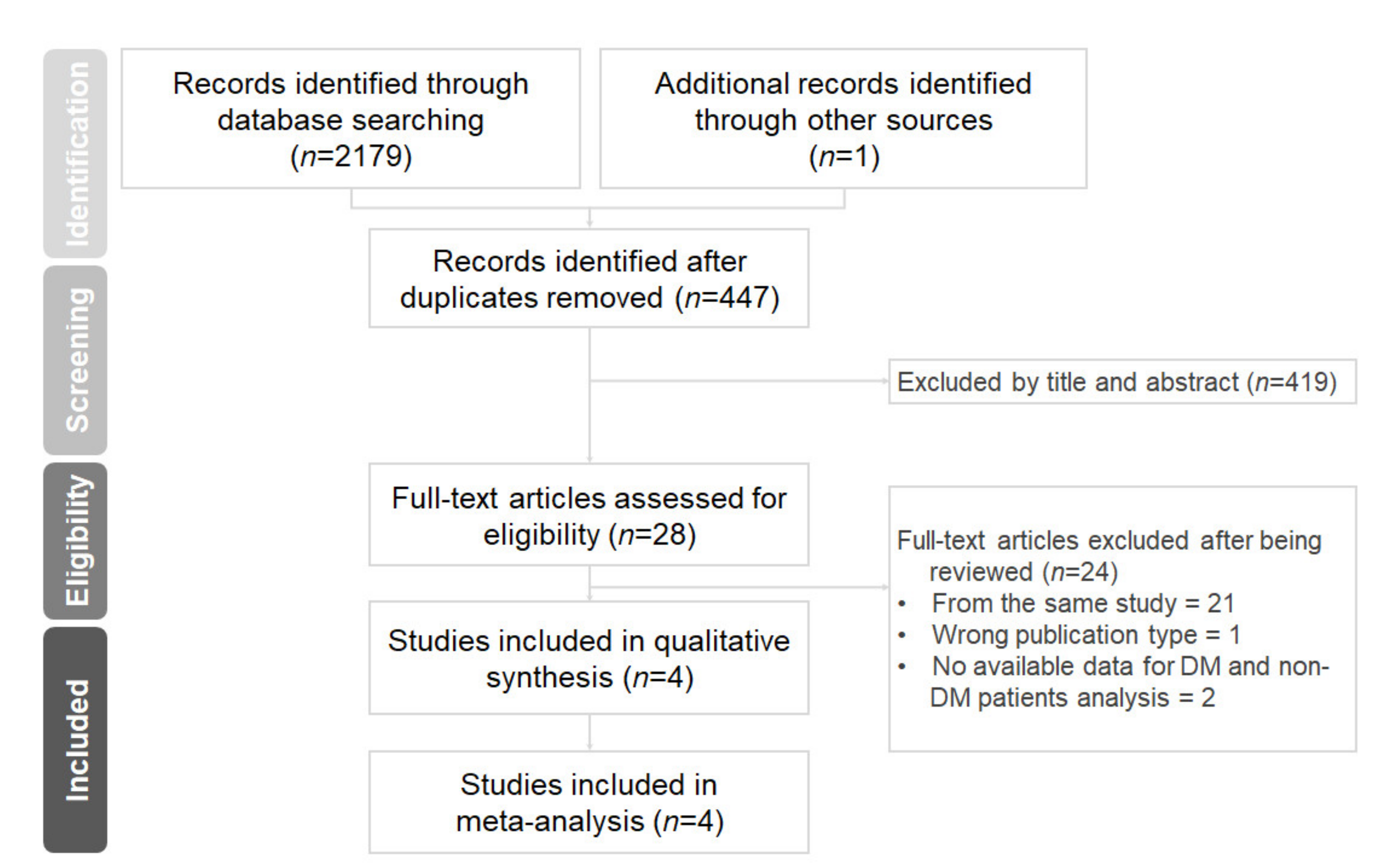
3.1. Search Results and Study Characteristics
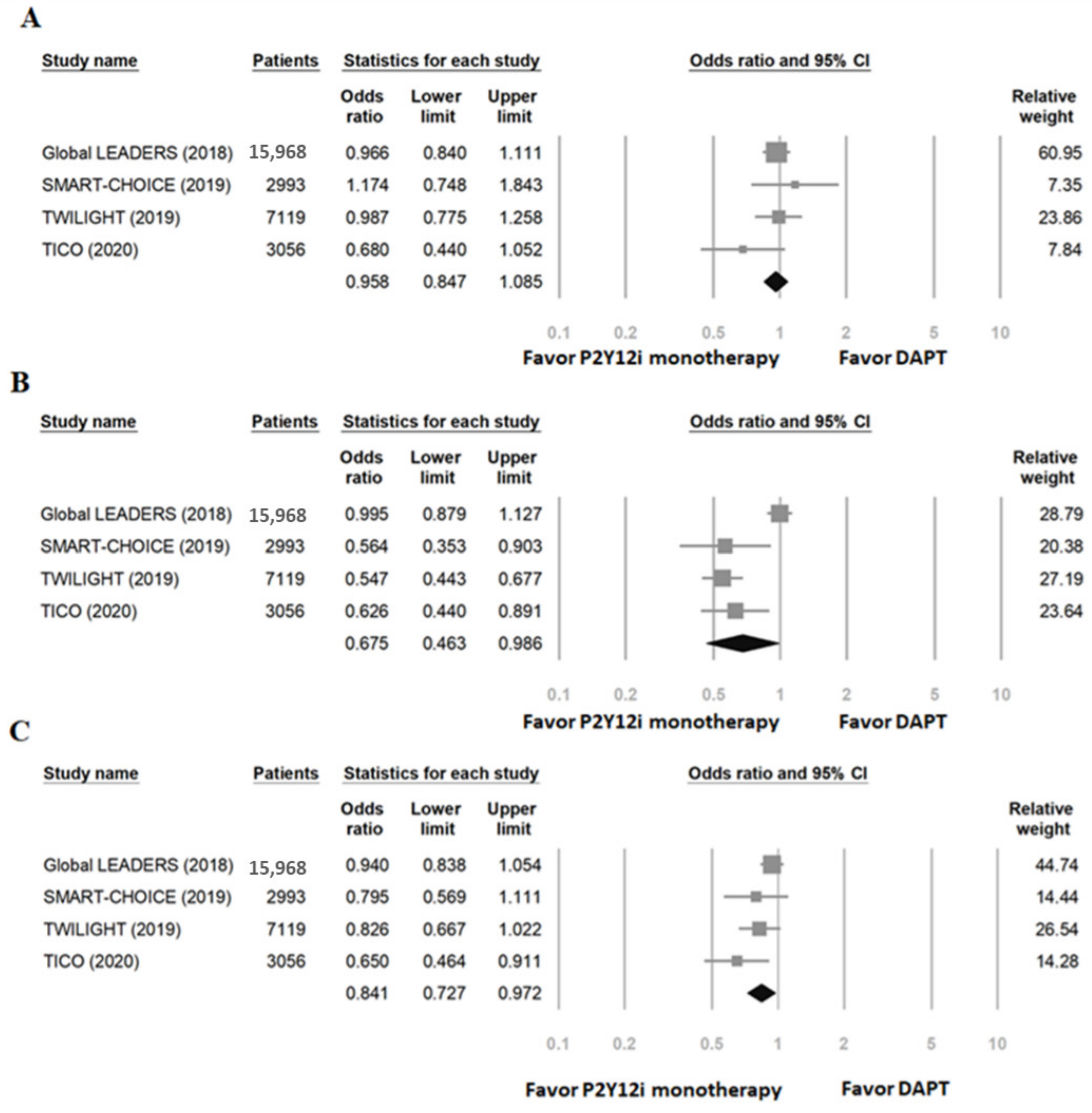
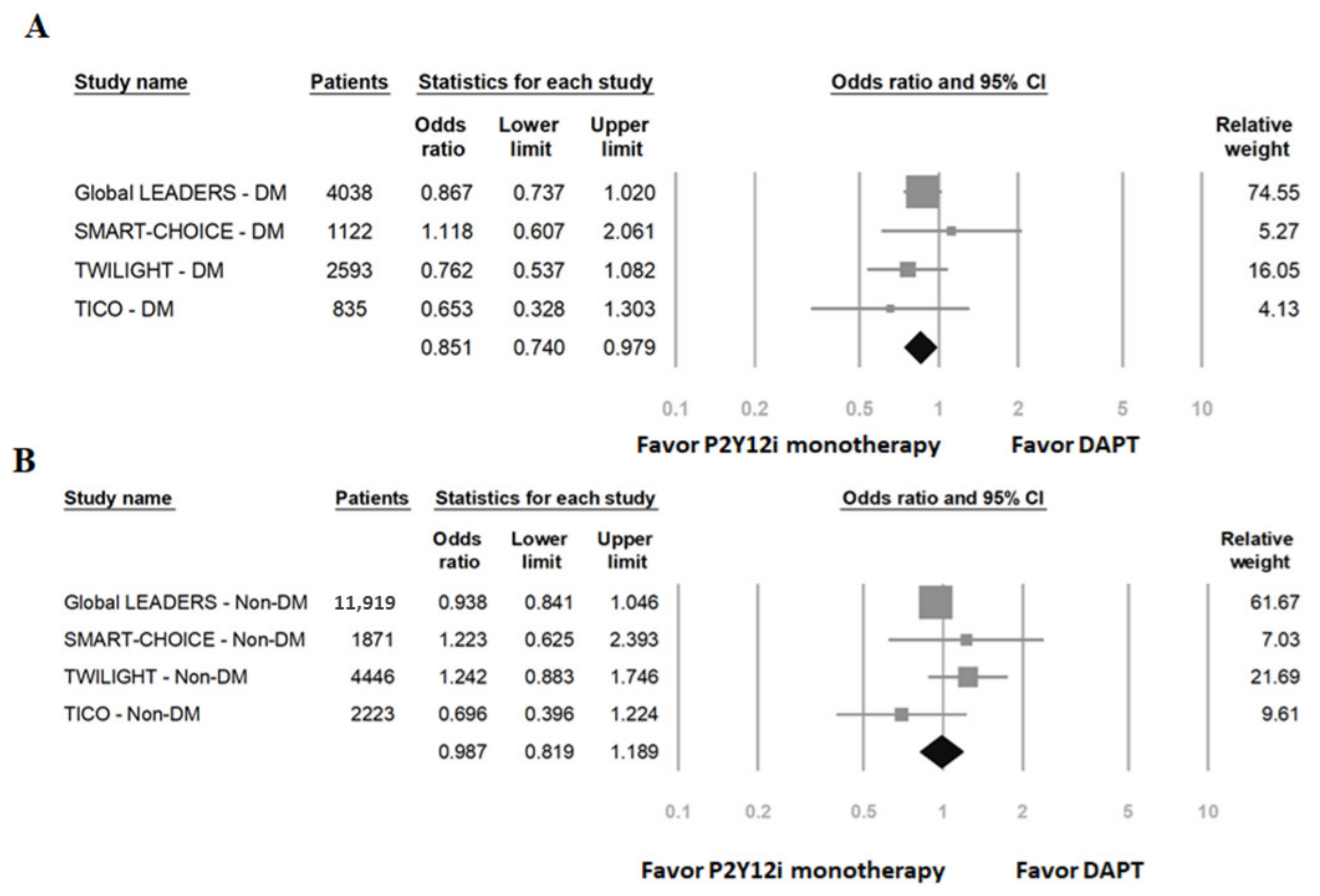
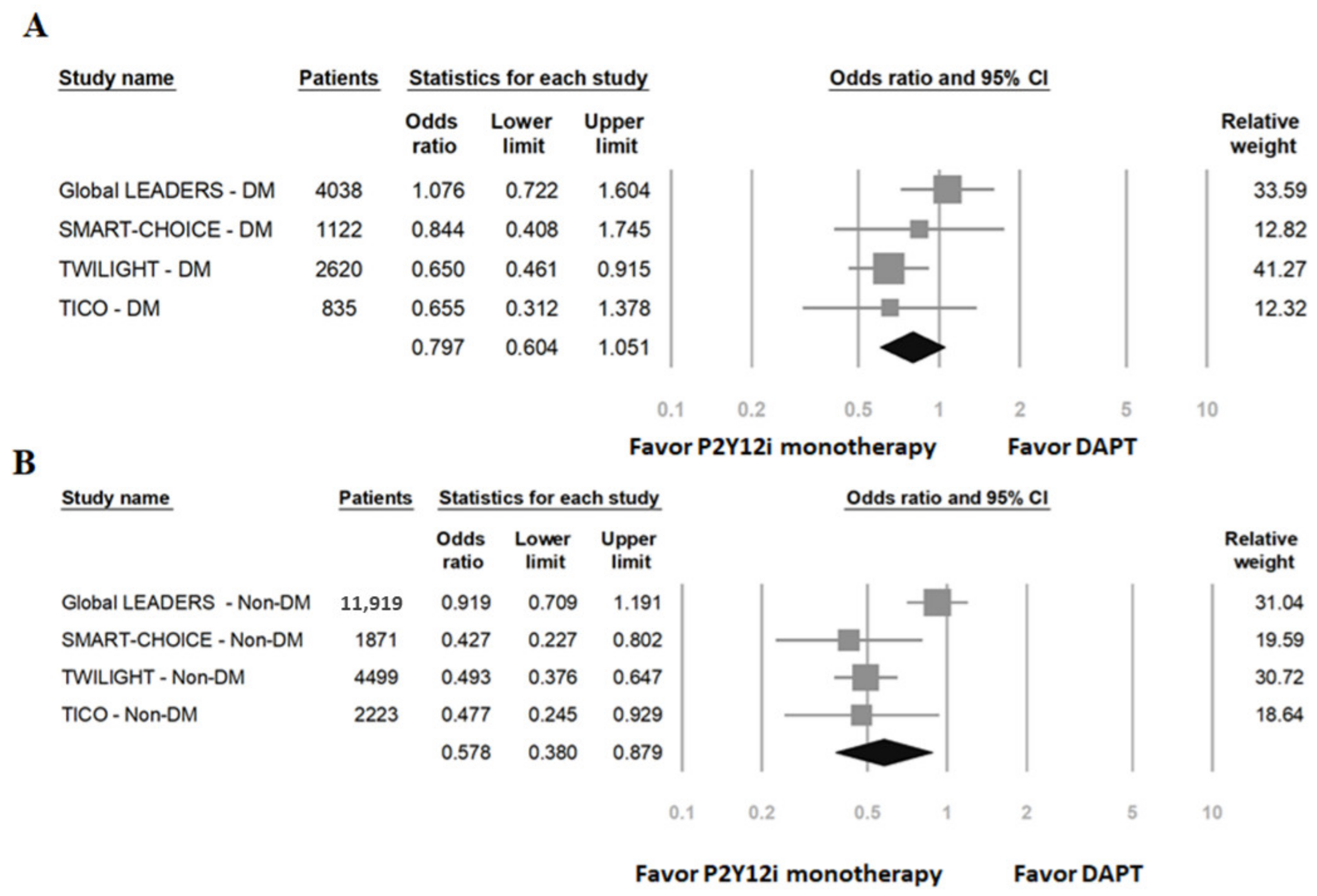
3.2. The Primary Efficacy and Safety Outcomes
3.3. Quality Assessment and Publication Bias
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levine, G.N.; Bates, E.R.; Bittl, J.A.; Brindis, R.G.; Fihn, S.D.; Fleisher, L.A.; Granger, C.B.; Lange, R.A.; Mack, M.J.; Mauri, L.; et al. 2016 acc/aha guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2016, 68, 1082–1115. [Google Scholar] [CrossRef] [PubMed]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: A multicentre, open-label, randomised superiority trial. Lancet (Lond. Engl.) 2018, 392, 940–949. [Google Scholar] [PubMed]
- Hahn, J.Y.; Song, Y.B.; Oh, J.H.; Chun, W.J.; Park, Y.H.; Jang, W.J.; Im, E.S.; Jeong, J.O.; Cho, B.R.; Oh, S.K.; et al. Effect of p2y12 inhibitor monotherapy vs dual antiplatelet therapy on cardiovascular events in patients undergoing percutaneous coronary intervention: The smart-choice randomized clinical trial. JAMA 2019, 321, 2428–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehran, R.; Baber, U.; Sharma, S.K.; Cohen, D.J.; Angiolillo, D.J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dangas, G.; Dudek, D.; et al. Ticagrelor with or without aspirin in high-risk patients after pci. N. Engl. J. Med. 2019, 381, 2032–2042. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Hong, S.J.; Cho, Y.H.; Yun, K.H.; Kim, Y.H.; Suh, Y.; Cho, J.Y.; Her, A.Y.; Cho, S.; Jeon, D.W.; et al. Effect of ticagrelor monotherapy vs ticagrelor with aspirin on major bleeding and cardiovascular events in patients with acute coronary syndrome: The tico randomized clinical trial. JAMA 2020, 323, 2407–2416. [Google Scholar] [CrossRef]
- Feng, W.H.; Hsieh, I.C.; Li, Y.H. P2y12 inhibitor monotherapy after percutaneous coronary intervention: Is it safe to abandon aspirin? Acta Cardiol. Sin. 2021, 37, 1–8. [Google Scholar]
- Yang, Y.; Park, G.M.; Han, S.; Kim, Y.G.; Suh, J.; Park, H.W.; Won, K.B.; Ann, S.H.; Kim, S.J.; Kim, D.W.; et al. Impact of diabetes mellitus in patients undergoing contemporary percutaneous coronary intervention: Results from a korean nationwide study. PLoS ONE 2018, 13, e0208746. [Google Scholar] [CrossRef]
- Kedhi, E.; Généreux, P.; Palmerini, T.; McAndrew, T.C.; Parise, H.; Mehran, R.; Dangas, G.D.; Stone, G.W. Impact of coronary lesion complexity on drug-eluting stent outcomes in patients with and without diabetes mellitus: Analysis from 18 pooled randomized trials. J. Am. Coll. Cardiol. 2014, 63, 2111–2118. [Google Scholar] [CrossRef] [Green Version]
- Lovic, D.; Piperidou, A.; Zografou, I.; Grassos, H.; Pittaras, A.; Manolis, A. The growing epidemic of diabetes mellitus. Curr. Vasc. Pharmacol. 2020, 18, 104–109. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Baber, U.; Sartori, S.; Briguori, C.; Dangas, G.; Cohen, D.J.; Mehta, S.R.; Gibson, C.M.; Chandiramani, R.; Huber, K.; et al. Ticagrelor with or without aspirin in high-risk patients with diabetes mellitus undergoing percutaneous coronary intervention. J. Am. Coll. Cardiol. 2020, 75, 2403–2413. [Google Scholar] [CrossRef]
- Chichareon, P.; Modolo, R.; Kogame, N.; Takahashi, K.; Chang, C.C.; Tomaniak, M.; Botelho, R.; Eeckhout, E.; Hofma, S.; Trendafilova-Lazarova, D.; et al. Association of diabetes with outcomes in patients undergoing contemporary percutaneous coronary intervention: Pre-specified subgroup analysis from the randomized global leaders study. Atherosclerosis 2020, 295, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 esc focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with eacts. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2018, 53, 34–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahaffey, K.W.; Wojdyla, D.M.; Carroll, K.; Becker, R.C.; Storey, R.F.; Angiolillo, D.J.; Held, C.; Cannon, C.P.; James, S.; Pieper, K.S.; et al. Ticagrelor compared with clopidogrel by geographic region in the platelet inhibition and patient outcomes (plato) trial. Circulation 2011, 124, 544–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FitzGerald, G.A.; Oates, J.A.; Hawiger, J.; Maas, R.L.; Roberts, L.J., 2nd; Lawson, J.A.; Brash, A.R. Endogenous biosynthesis of prostacyclin and thromboxane and platelet function during chronic administration of aspirin in man. J. Clin. Investig. 1983, 71, 676–688. [Google Scholar] [CrossRef]
- Cattaneo, M.; Lecchi, A. Inhibition of the platelet p2y12 receptor for adenosine diphosphate potentiates the antiplatelet effect of prostacyclin. J. Thromb. Haemost. JTH 2007, 5, 577–582. [Google Scholar] [CrossRef]
- Warner, T.D.; Nylander, S.; Whatling, C. Anti-platelet therapy: Cyclo-oxygenase inhibition and the use of aspirin with particular regard to dual anti-platelet therapy. Br. J. Clin. Pharmacol. 2011, 72, 619–633. [Google Scholar] [CrossRef] [Green Version]
- Ho, A.C.; Egolum, U.; Parker, S.; Dimmel, J.; Hawkins, A.; Ling, H. P2y12 inhibitor monotherapy after a short dual antiplatelet therapy versus standard-term dual antiplatelet therapy in patients undergoing percutaneous coronary intervention: A contemporary meta-analysis. Clin. Drug Investig. 2020, 40, 799–808. [Google Scholar] [CrossRef]
- Valgimigli, M.; Gragnano, F.; Branca, M.; Franzone, A.; Baber, U.; Jang, Y.; Kimura, T.; Hahn, J.Y.; Zhao, Q.; Windecker, S.; et al. P2y12 inhibitor monotherapy or dual antiplatelet therapy after coronary revascularisation: Individual patient level meta-analysis of randomised controlled trials. BMJ (Clin. Res. Ed.) 2021, 373, n1332. [Google Scholar] [CrossRef]
- Giacoppo, D.; Matsuda, Y.; Fovino, L.N.; D’Amico, G.; Gargiulo, G.; Byrne, R.A.; Capodanno, D.; Valgimigli, M.; Mehran, R.; Tarantini, G. Short dual antiplatelet therapy followed by p2y12 inhibitor monotherapy vs. Prolonged dual antiplatelet therapy after percutaneous coronary intervention with second-generation drug-eluting stents: A systematic review and meta-analysis of randomized clinical trials. Eur. Heart J. 2021, 42, 308–319. [Google Scholar]
- Ferreiro, J.L.; Angiolillo, D.J. Diabetes and antiplatelet therapy in acute coronary syndrome. Circulation 2011, 123, 798–813. [Google Scholar] [CrossRef]
- Ferroni, P.; Basili, S.; Falco, A.; Davì, G. Platelet activation in type 2 diabetes mellitus. J. Thromb. Haemost. JTH 2004, 2, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Bernardo, E.; Sabaté, M.; Jimenez-Quevedo, P.; Costa, M.A.; Palazuelos, J.; Hernández-Antolin, R.; Moreno, R.; Escaned, J.; Alfonso, F.; et al. Impact of platelet reactivity on cardiovascular outcomes in patients with type 2 diabetes mellitus and coronary artery disease. J. Am. Coll. Cardiol. 2007, 50, 1541–1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivas Rios, J.R.; Franchi, F.; Rollini, F.; Angiolillo, D.J. Diabetes and antiplatelet therapy: From bench to bedside. Cardiovasc. Diagn. Ther. 2018, 8, 594–609. [Google Scholar] [CrossRef] [PubMed]
- Severino, P.; D’Amato, A.; Prosperi, S.; Magnocavallo, M.; Mariani, M.V.; Netti, L.; Birtolo, L.I.; De Orchi, P.; Chimenti, C.; Maestrini, V.; et al. Potential role of enos genetic variants in ischemic heart disease susceptibility and clinical presentation. J. Cardiovasc. Dev. Dis. 2021, 8, 116. [Google Scholar] [CrossRef] [PubMed]
- Theofilis, P.; Sagris, M.; Oikonomou, E.; Antonopoulos, A.S.; Tsioufis, K.; Tousoulis, D. Factors associated with platelet activation-recent pharmaceutical approaches. Int. J. Mol. Sci. 2022, 23, 3301. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, S.S.; Vanhoutte, P.M.; Leung, S.W.; Yusof, M.I.; Sulaiman, W.A.W.; Saad, A.Z.M.; Suppian, R.; Rasool, A.H.G. Reduced expression of prostacyclin synthase and nitric oxide synthase in subcutaneous arteries of type 2 diabetic patients. Tohoku J. Exp. Med. 2013, 231, 217–222. [Google Scholar] [CrossRef] [Green Version]
- Kaur, R.; Kaur, M.; Singh, J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: Molecular insights and therapeutic strategies. Cardiovasc. Diabetol. 2018, 17, 121. [Google Scholar] [CrossRef]
- Armstrong, P.C.; Leadbeater, P.D.; Chan, M.V.; Kirkby, N.S.; Jakubowski, J.A.; Mitchell, J.A.; Warner, T.D. In the presence of strong p2y12 receptor blockade, aspirin provides little additional inhibition of platelet aggregation. J. Thromb. Haemost. JTH 2011, 9, 552–561. [Google Scholar] [CrossRef] [Green Version]
- Baber, U.; Zafar, M.U.; Dangas, G.; Escolar, G.; Angiolillo, D.J.; Sharma, S.K.; Kini, A.S.; Sartori, S.; Joyce, L.; Vogel, B.; et al. Ticagrelor with or without aspirin after pci: The twilight platelet substudy. J. Am. Coll. Cardiol. 2020, 75, 578–586. [Google Scholar] [CrossRef]
- Johnson, T.W.; Baos, S.; Collett, L.; Hutchinson, J.L.; Nkau, M.; Molina, M.; Aungraheeta, R.; Reilly-Stitt, C.; Bowles, R.; Reeves, B.C.; et al. Pharmacodynamic comparison of ticagrelor monotherapy versus ticagrelor and aspirin in patients after percutaneous coronary intervention: The template (ticagrelor monotherapy and platelet reactivity) randomized controlled trial. J. Am. Heart Assoc. 2020, 9, e016495. [Google Scholar] [CrossRef]
- Moulias, A.; Xanthopoulou, I.; Alexopoulos, D. Does ticagrelor improve endothelial function? J. Cardiovasc. Pharmacol. Ther. 2019, 24, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Rosenson, R.S.; Chen, Q.; Najera, S.D.; Krishnan, P.; Lee, M.L.; Cho, D.J. Ticagrelor improves blood viscosity-dependent microcirculatory flow in patients with lower extremity arterial disease: The hema-kinesis clinical trial. Cardiovasc. Diabetol. 2019, 18, 77. [Google Scholar] [CrossRef] [Green Version]
- Angiolillo, D.J.; Fernandez-Ortiz, A.; Bernardo, E.; Ramírez, C.; Sabaté, M.; Jimenez-Quevedo, P.; Hernández, R.; Moreno, R.; Escaned, J.; Alfonso, F.; et al. Platelet function profiles in patients with type 2 diabetes and coronary artery disease on combined aspirin and clopidogrel treatment. Diabetes 2005, 54, 2430–2435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angiolillo, D.J.; Jakubowski, J.A.; Ferreiro, J.L.; Tello-Montoliu, A.; Rollini, F.; Franchi, F.; Ueno, M.; Darlington, A.; Desai, B.; Moser, B.A.; et al. Impaired responsiveness to the platelet p2y12 receptor antagonist clopidogrel in patients with type 2 diabetes and coronary artery disease. J. Am. Coll. Cardiol. 2014, 64, 1005–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, E.R.; Lau, W.C.; Angiolillo, D.J. Clopidogrel-drug interactions. J. Am. Coll. Cardiol. 2011, 57, 1251–1263. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.W.; Feng, W.H.; Ho, M.Y.; Su, C.H.; Huang, S.W.; Cheng, C.W.; Yeh, H.I.; Chen, C.P.; Huang, W.C.; Fang, C.C.; et al. P2y12 inhibitor monotherapy with clopidogrel versus ticagrelor in patients with acute coronary syndrome undergoing percutaneous coronary intervention. J. Clin. Med. 2020, 9, 1657. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Trials | Global Leaders [2] | Global Leaders [2] | Smart-Choice [3] | Smart- Choice [3] | Twilight [4] | Twilight [4] | Tico [5] | Tico [5] |
|---|---|---|---|---|---|---|---|---|
| Year | 2018 | 2018 | 2019 | 2019 | 2019 | 2019 | 2020 | 2020 |
| Study population | PCI | PCI | PCI | PCI | High-risk, PCI | High-risk, PCI | ACS, PCI | ACS, PCI |
| Arm | DAPT 1 m, then mono | DAPT | DAPT 3 m, then mono | DAPT | DAPT 3 m, then mono | DAPT | DAPT 3 m, then mono | DAPT |
| P2Y12 inhibitor | Ticagrelor | Ticagrelor or clopidogrel | Clopidogrel (77%) | Clopidogrel (77%) | Ticagrelor | Ticagrelor | Ticagrelor | Ticagrelor |
| Patients number | 7980 | 7988 | 1495 | 1498 | 3555 | 3564 | 1527 | 1529 |
| Age (mean) | 64.5 | 64.6 | 64.6 | 64.4 | 65.2 | 65.1 | 61 | 61 |
| ACS (%) | 3750 (47.0) | 3737 (46.8) | 870 (58.2) | 873 (58.2) | 2273 (63.9) | 2341 (65.7) | 1527 (100) | 1529 (100) |
| STEMI (%) | 1062 (13.3) | 1030 (12.9) | 164 (11.0) | 150 (10.0) | Excluded | Excluded | 546 (35.7) | 557 (36.4) |
| NSTEMI (%) | 1684 (21.1) | 1689 (21.1) | 239 (16.0) | 230 (15.4) | 1024 (28.8) | 1096 (30.8) | 539 (35.3) | 488 (31.9) |
| DM (%) | 2049 (25.7) | 1989 (24.9) | 570 (38.2) | 552 (36.8) | 1319 (37.1) | 1301 (36.5) | 418 (27.4) | 417 (27.2) |
| Follow-up time | 24 m | 24 m | 12 m | 12 m | 12 m | 12 m | 12 m | 12 m |
| Primary endpoint | Death, new Q-wave MI | Death, new Q-wave MI | death, MI, stroke | death, MI, stroke | Bleeding | Bleeding | NACE | NACE |
| MACCE (%) | 407 (5.10) | 421 (5.27) | 42 (2.9) | 36 (2.5) | 135 (3.9) | 137 (3.9) | 35 (2.3) | 51 (3.4) |
| All-cause death at 12 m (%) | 108 (1.35) | 131 (1.64) | 21 (1.4) | 18 (1.2) | 34 (1.0) | 45 (1.3) | 16 (1.1) | 23 (1.5) |
| CV death at 12 m (%) | N/A | N/A | 11 (0.8) | 13 (0.9) | 26 (0.8) | 37 (1.1) | 7 (0.5) | 12 (0.8) |
| MI at 12 m (%) | 179 (2.24) | 158 (1.98) | 11 (0.8) | 17 (1.2) | 95 (2.7) | 95 (2.7) | 6 (0.4) | 11 (0.7) |
| Stroke (%) | 52 (0.65) | 49 (0.61) | 11 (0.8) | 5 (0.3) | 16 (0.5) | 8 (0.2) | 8 (0.5) | 11 (0.7) |
| Stent thrombosis ‡ | 53 (0.66) | 41 (0.51) | 3 (0.2) | 2 (0.1) | 14 (0.4) | 19 (0.6) | 6 (0.4) | 4 (0.3) |
| Major or minor bleeding # | 529 (6.63) | 532 (6.66) | 28 (2.0) | 49 (3.4) | 141 (4.0) | 250 (7.1) | 53 (3.6) | 83 (5.5) |
| Major bleeding # | 117 (1.47) | 136 (1.70) | 12 (0.8) | 14 (1.0) | 34 (1.0) | 69 (2.0) | 25 (1.7) | 45 (3.0) |
| NACE | 616 (7.72) | 653 (8.17) | 65 (4.5) | 81 (5.6) | 163 (4.6) | 196 (5.5) | 59 (3.9) | 89 (5.9) |
| DM Patients | Non-DM Patients | |||||||
|---|---|---|---|---|---|---|---|---|
| P2Y12i Monotherapy | DAPT | Hazard Ratio (95% CI) | p-Value | P2Y12i Monotherapy | DAPT | Hazard Ratio (95% CI) | p-Value | |
| GLOBAL LEADERS | n = 4038 | n = 11,919 | ||||||
| MACE | 338 (16.7) | 369 (18.7) | 0.87 (0.74–1.02) | 0.09 | 711 (12.2) | 761 (12.8) | 0.94 (0.84–1.05) | 0.25 |
| Bleeding | 52 (2.6) | 47 (2.4) | 1.08 (0.72–1.60) | 0.72 | 111 (1.9) | 122 (2.1) | 0.92 (0.71–1.19) | 0.52 |
| SMART-CHOICE | n = 1122 | n = 1868 | ||||||
| MACE | 23 (4.1) | 20 (3.8) | 1.12 (0.61–2.06) | 0.72 | 19 (2.1) | 16 (1.7) | 1.22 (0.63–2.29) | 0.56 |
| Bleeding | 14 (2.6) | 16 (3.0) | 0.84 (0.41–1.75) | 0.65 | 14 (1.6) | 33 (3.6) | 0.43 (0.23–0.80) | 0.01 |
| TWILIGHT | n = 2620 | n = 4499 | ||||||
| MACE | 59 (4.6) | 75 (5.9) | 0.76 (0.54–1.08) | 0.13 | 76 (3.5) | 62 (2.8) | 1.24 (0.88–1.75) | 0.21 |
| Bleeding | 58 (4.5) | 86 (6.7) | 0.65 (0.46–0.91) | 0.01 | 83 (3.8) | 164 (7.3) | 0.50 (0.39–0.66) | <0.01 |
| TICO | n = 835 | n = 2221 | ||||||
| MACE | 14 (3.4) | 21 (5.1) | 0.65 (0.33–1.30) | 0.23 | 21 (1.9) | 30 (2.7) | 0.70 (0.40–1.22) | 0.21 |
| Bleeding | 12 (2.9) | 18 (4.5) | 0.66 (0.31–1.38) | 0.26 | 13 (1.2) | 27 (2.4) | 0.48 (0.24–0.93) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, W.-H.; Chang, Y.-C.; Lin, Y.-H.; Chen, H.-L.; Chang, H.-M.; Chu, C.-S. Comparative Efficacy and Safety of P2Y12 Inhibitor Monotherapy and Dual Antiplatelet Therapy in Patients with and without Diabetes Mellitus Undergoing Percutaneous Coronary Intervention. Int. J. Mol. Sci. 2022, 23, 4549. https://doi.org/10.3390/ijms23094549
Feng W-H, Chang Y-C, Lin Y-H, Chen H-L, Chang H-M, Chu C-S. Comparative Efficacy and Safety of P2Y12 Inhibitor Monotherapy and Dual Antiplatelet Therapy in Patients with and without Diabetes Mellitus Undergoing Percutaneous Coronary Intervention. International Journal of Molecular Sciences. 2022; 23(9):4549. https://doi.org/10.3390/ijms23094549
Chicago/Turabian StyleFeng, Wen-Han, Yong-Chieh Chang, Yi-Hsiung Lin, Hsiao-Ling Chen, Hsiu-Mei Chang, and Chih-Sheng Chu. 2022. "Comparative Efficacy and Safety of P2Y12 Inhibitor Monotherapy and Dual Antiplatelet Therapy in Patients with and without Diabetes Mellitus Undergoing Percutaneous Coronary Intervention" International Journal of Molecular Sciences 23, no. 9: 4549. https://doi.org/10.3390/ijms23094549
APA StyleFeng, W.-H., Chang, Y.-C., Lin, Y.-H., Chen, H.-L., Chang, H.-M., & Chu, C.-S. (2022). Comparative Efficacy and Safety of P2Y12 Inhibitor Monotherapy and Dual Antiplatelet Therapy in Patients with and without Diabetes Mellitus Undergoing Percutaneous Coronary Intervention. International Journal of Molecular Sciences, 23(9), 4549. https://doi.org/10.3390/ijms23094549