
Signet-Ring Cell Squamous Cell Carcinoma: A Biphenotypic Neoplasm of the Gastro-Esophageal Junction with Uncertain Biological Potential: Case Report and Literature Review

 ,
, 
Abstract
:1. Introduction
2. Case Presentation
2.1. Personal History
2.2. Laboratory Examinations
2.3. Imaging and Endoscopic Examinations
2.4. Surgery
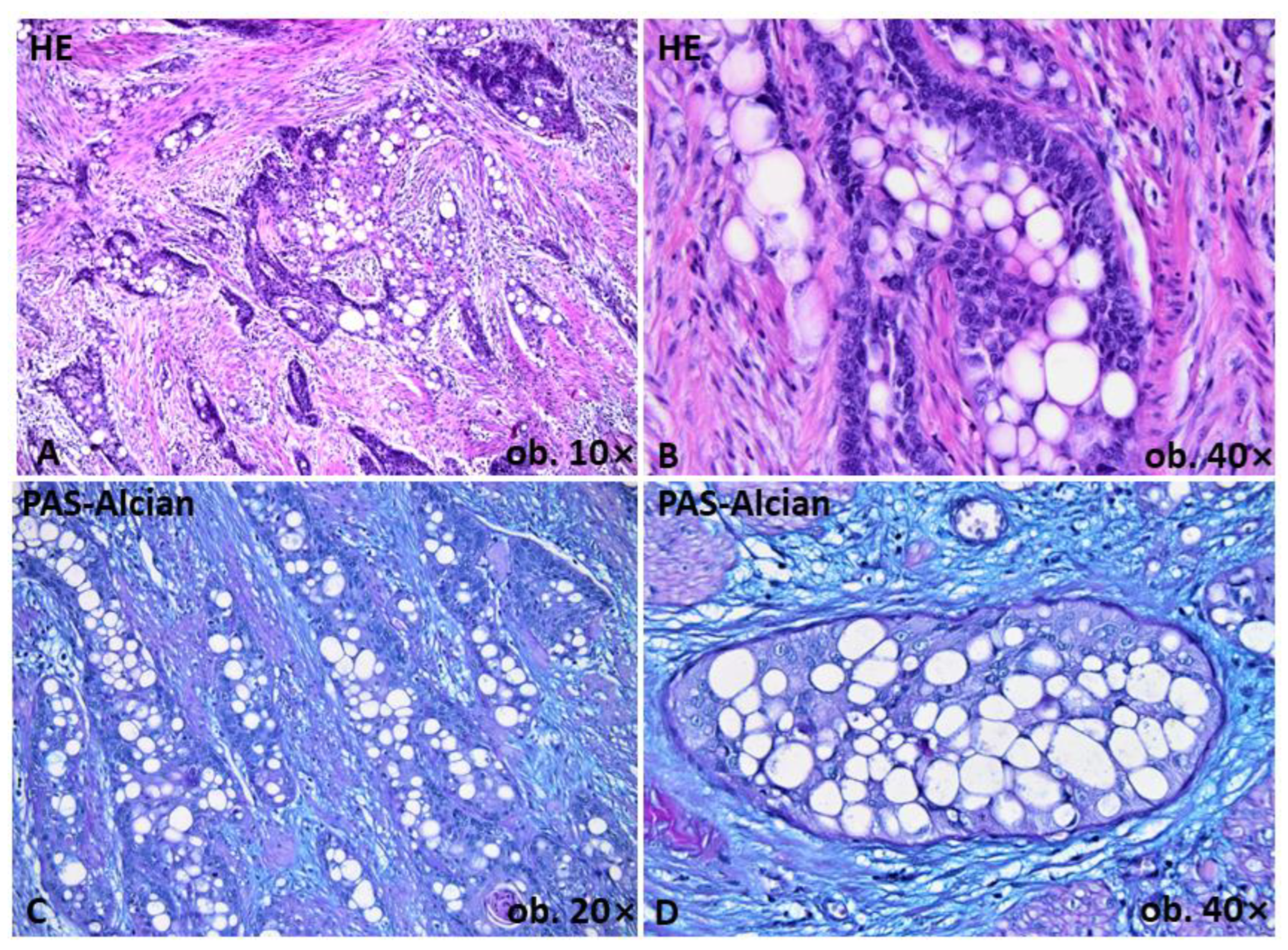
2.5. Gross and Histopathological Assessment of Surgical Specimens
2.6. Immunohistochemical and Molecular Profile of Tumor Cells
2.7. Outcome and Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Pineros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: International Agency for Reasearch on Cancer. Available online: https://gco.iarc.fr/ (accessed on 25 July 2020).
- Sanchez-Danes, A.; Blanpain, C. Deciphering the cells of origin of squamous cell carcinomas. Nat. Rev. Cancer 2018, 18, 549–561. [Google Scholar] [CrossRef]
- Elder, D.E.; Massi, D.; Scolyer, R.A.; Willemze, R. WHO Classification of Skin Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2018; Volume 4, pp. 35–44. [Google Scholar]
- Rinker, M.H.; Fenske, N.A.; Scalf, L.A.; Glass, L.F. Histologic variants of squamous cell carcinoma of the skin. Cancer Control 2001, 8, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Gurzu, S.; Sugimura, H.; Szederjesi, J.; Szodorai, R.; Braicu, C.; Kobori, L.; Fodor, D.; Jung, I. Interaction between cadherins, vimentin, and V-set and immunoglobulin domain containing 1 in gastric-type hepatocellular carcinoma. Histochem. Cell Biol. 2021, 156, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Cramer, S.F.; Heggeness, L.M. Signet-ring squamous cell carcinoma. Am. J. Clin. Pathol. 1989, 91, 488–491. [Google Scholar] [CrossRef] [PubMed]
- McKinley, E.; Valles, R.; Bang, R.; Bocklage, T. Signet-ring squamous cell carcinoma: A case report. J. Cutan. Pathol. 1998, 25, 176–181. [Google Scholar] [CrossRef]
- Yigit, N.; Celik, E.; Yavan, I. Prominent signet ring cell morphology in a pulmonary squamous cell carcinoma. Turk. Patol. Derg. 2018, 34, 194–197. [Google Scholar] [CrossRef]
- Kupryjanczyk, J.; Kujcwa, M. Signet-ring cells in squamous cell carcinoma of the cervix and in non-neoplastic ectocervical epithelium. Int. J. Gynecol. Cancer 1992, 2, 152–156. [Google Scholar] [CrossRef]
- Lee, D. Acantholytic squamous cell carcinoma of the esophagus with prevalent single isolated tumor cells including signet ring cells and many osteoclast-like giant cells. Pathology 2016, 48, 281–283. [Google Scholar] [CrossRef]
- Nakajima, K.; Keneko, T.; Aizu, T.; Nakano, H.; Matsuzaki, Y.; Sawamura, D. Signet-ring cutaneous squamous cell carcinoma arising on the back of the finger. Case Rep. Dermatol. 2013, 10, 215–218. [Google Scholar] [CrossRef]
- El Demelawy, D.; Onuman, K.; Alowamy, S. Signet ring squamous cell carcinoma-the forgotten variant: Case report and review of the literature. J. Cutan. Pathol. 2011, 38, 306–308. [Google Scholar] [CrossRef]
- Park, H.S.; Lee, S. Acantholytic squamous cell carcinoma of the lung showing significant signet ring cell component. Histopathology 2016, 68, 463–465. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.R.; Wang, N.M.; Zhou, L.; Liu, Z.L.; Chen, N.P.; Hu, Y.P.; Deng, Y.J.; Qi, X.Q.; Huang, X.F.; Su, Y.; et al. Cutaneous clear cell/signet-ring cell squamous cell carcinoma arising in the right thigh of a patient with type 2 diabetes: Combined morphologic, immunohistochemical and etiologic analysis. Diagn. Pathol. 2016, 11, 36. [Google Scholar] [CrossRef] [PubMed]
- Bastian, B.C.; Kutzner, H.; Yen, T.S.B.; LeBoit, P.E. Signet-ring cell formation in cutaneous neoplasms. J. Am. Acad. Dermatol. 1999, 41, 606–613. [Google Scholar]
- Proia, A.D.; Selim, M.A.; Reutter, J.C.; Michon, J.J. Basal cell-signet-ring squamous cell carcinoma of the eyelid. Arch. Pathol. Lab. Med. 2006, 130, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Lortscher, D.N.; Satter, E.K.; Romero, L.S. Signet ring-like cells: No longer a “signature” of glandular differentiation. Dermatol. Online J. 2012, 18, 3. [Google Scholar] [CrossRef]
- Handra-Luca, A. Signet-ring cell morphotype in lung carcinoma. Turk. Patol. Derg. 2020, 36, 275–276. [Google Scholar] [CrossRef]
- Findeis, S.K.; Readinger, A.; Mitchell, J.; Agarwal, A. Cutaneous signet-ring cell squamous cell carcinoma. Bayl. Univ. Med. Cent. Proc. 2020, 33, 424–426. [Google Scholar] [CrossRef]
- Haghayeghi, K.; Telang, G.; Robinson-Bostom, L. Signet-ring squamous cell carcinoma: A report of a rare variant and review of the literature. Dermatol. Online J. 2020, 26, 6. [Google Scholar] [CrossRef]
- Islam, F.; Gopalan, V.; Wahab, R.; Smith, R.A.; Lam, A.K.-Y. Cancer stem cells in esophageal squamous cell carcinoma: Identification, prognostic, and treatment perspectives. Crit. Rev. Oncol. Hematol. 2015, 96, 9–19. [Google Scholar] [CrossRef]
- Liu, K.; Lin, B.; Zhao, M.; Yang, X.; Chen, M.; Gao, A.; Liu, F.; Que, J.; Lan, X. The multiple roles for Sox2 in stem cell maintenance and tumorigenesis. Cell. Signal. 2013, 25, 1264–1271. [Google Scholar] [CrossRef]
- Liu, X.; Qiao, B.; Zhao, T.; Hu, F.; Lam, A.K.-Y.; Tao, Q. Sox2 promotes tumor aggressiveness and epithelial-mesenchymal transition in tongue squamous cell carcinoma. Int. J. Mol. Med. 2018, 42, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Mahamad Apandi, N.I.; Ramanathan, A.; Ismail, S.M.; Ranganathan, K. Do Clear Cell Changes in Oral Squamous Cell Carcinoma Warrant It Being Recognised as a Variant? Cureus 2022, 14, e25057. [Google Scholar] [CrossRef] [PubMed]
- Bayo, P.; Jou, A.; Stenzinger, A.; Shao, C.; Gross, M.; Jensen, A.; Grabe, N.; Mende, C.H.; Rados, P.V.; Debus, J.; et al. Loss of SOX2 expression induces cell motility via vimentin up-regulation and is an unfavourable risk factor for survival of head and neck squamous cell carcinoma. Mol. Oncol. 2015, 9, 1704–1719. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Antibody | Clone | Manufacturer/ Country | Retrieval | Dilution | Classic SCC Component | Signet-Ring Cells |
|---|---|---|---|---|---|---|
| Cytokeratin | AE1/AE3 | ImmunoLogic/ Netherland | High pH | RTU | Positive | Positive |
| Keratin 5/6 | D5/16B4 | Dako/Denmark | High pH | RTU | Positive | Positive |
| p63 | 4A4 | ImmunoLogic | High pH | 1:100 | Positive | Positive |
| p40 | ZR8 | BioSB/USA | High pH | 1:50 | Positive | Positive |
| MLH1 | ES05 | Dako | High pH | RTU | Positive | Positive |
| MSH2 | FE11 | Dako | High pH | RTU | Positive | Positive |
| MSH6 | EP49 | Dako | High pH | RTU | Positive | Positive |
| PMS2 | EP51 | Dako | High pH | RTU | Positive | Positive |
| β-catenin | β-catenin1 | Dako | High pH | RTU | Membrane positivity | Nuclear positivity |
| E-cadherin | NCH-38 | Dako | High pH | RTU | Positive | Focally loss |
| N-cadherin | 6G11 | Dako | Citrate | 1:100 | Negative | Negative |
| Vimentin | V9 | Dako | High pH | 1:800 | Negative | Positive |
| Slug | H-140 | Santa Cruz/USA | High pH | 1:100 | Negative | Positive |
| HER2 | Polyclonal | Dako | High pH | 1:800 | Negative | Negative |
| PD-1 | NAT105 | A.Menarini/Italy | High pH | 1:50 | Negative | Negative |
| PD-L1 | 22C3 | Dako | Citrate | 1:50 | Negative | Negative |
| VEGF | VG-1 | Abcam/UK | High pH | 1:50 | Negative | Negative |
| EGFR/HER1 | H11 | Dako | High pH | 1:100 | Positive | Positive |
| Sox2 | Polyclonal | EMD Millipore/USA | Citrate | 1:6000 | Negative | Positive |
| Oct3/4 | N1NK | Dako | High pH | 1:50 | Negative | Negative |
| CD44 | DF1485 | Dako | Citrate | 1:50 | Positive | Positive |
| CEA | II-7 | Dako | High pH | 1:50 | Negative | Negative |
| CA125 | M11 | Dako | Citrate | 1:20 | Negative | Negative |
| CA19-9 | CA19-9 | Leica/UK | Citrate | 1:200 | Negative | Negative |
| CA72-4 | B72.3 | ThermoScientific/ UK | High pH | 1:200 | Negative | Negative |
| EBV | CS.1-4 | Dako | Citrate | 1:100 | Negative | Negative |
| p16 | Anti-p16 | Biotech/USA | High pH | 1:100 | Negative | Negative |
| Case No. | Authors, Year of Publication | Patient’s Gender | Patient’s Age (Years) | Localization | Diameter (mm) |
|---|---|---|---|---|---|
| 1. | Cramer and Heggeness (1988) [6] | Male | 69 | Skin (forehead) | NA |
| 2. | Kupryjanczyk et al. (1992) [9] | Female | 74 | Uterine cervix | NA |
| 3. | Female | 84 | Uterine cervix | NA | |
| 4. | McKinley et al. (1998) [7] | Male | 50 | Skin (neck) | 6 mm |
| 5. | Bastian et al. (1999) [15] | Female | 79 | Skin (right cheek) | NA |
| 6. | Bastian et al. (1999) [15] | Male | 82 | Skin (temple) | NA |
| 7. | Bastian et al. (1999) [15] | Male | 83 | Skin (ear) | NA |
| 8. | Bastian et al. (1999) [15] | Male | 80 | Skin (forehead) | NA |
| 9. | Bastian et al. (1999) [15] | Male | 87 | Skin (scalp) | NA |
| 10. | Bastian et al. (1999) [15] | - | - | - | - |
| 11. | Bastian et al. (1999) [15] | Male | 76 | Skin (forehead) | NA |
| 12. | Proia et al. (2006) [16] | Female | 93 | Skin (eyelid) | 17 mm |
| 13. | El Demellawy et al. (2011) [12] | Female | 84 | Upper Lip | 11 mm |
| 14. | Lortscher et al. (2012) [17] | Male | 67 | Skin (canthus/palpebral commissure) | 15 mm |
| 15. | Nakajima et al. (2013) [11] | Male | 83 | Skin (finger) | 31 mm |
| 16. | Park (2015) [13] | Male | 64 | Lung | 29 mm |
| 17. | Wang et al. (2016) [14] | Female | 78 | Skin (thigh) | 50 mm |
| 18. | Lee (2016) [10] | Female | 82 | Esophagus | 55 mm |
| 19. | Yigit et al. (2018) [8] | Male | 85 | Lung | 42 mm |
| 20. | Handra-Luca (2019) [18] | - | - | Lung | - |
| 21. | Findeis et al. (2020) [19] | Female Transgender | 66 | Skin (parotid region) | 56 mm |
| 22. | Haghayeghi et al. (2020) [20] | Male | 71 | Skin (ear) | 15 mm |
| 23. | Apandi et al. (2022) [24] | Male | 65 | Oral cavity (gingiva) | 10 mm |
| 24. | Present case | Male | 59 | Esophagus | 33 mm |
| Signet-Ring SCC | Clear Cell SCC | Acantholytic/Adenoid/ Pseudo-Glandular SCC | |
|---|---|---|---|
| Histology |
|
|
|
| Special stains |
|
|
|
| IHC |
|
|
|
| Clinical behavior | High aggressivity | Moderate/high aggressivity | Moderate aggressivity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satala, C.B.; Kovacs, Z.; Bara, T., Jr.; Jung, I.; Gurzu, S. Signet-Ring Cell Squamous Cell Carcinoma: A Biphenotypic Neoplasm of the Gastro-Esophageal Junction with Uncertain Biological Potential: Case Report and Literature Review. Int. J. Mol. Sci. 2023, 24, 9535. https://doi.org/10.3390/ijms24119535
Satala CB, Kovacs Z, Bara T Jr., Jung I, Gurzu S. Signet-Ring Cell Squamous Cell Carcinoma: A Biphenotypic Neoplasm of the Gastro-Esophageal Junction with Uncertain Biological Potential: Case Report and Literature Review. International Journal of Molecular Sciences. 2023; 24(11):9535. https://doi.org/10.3390/ijms24119535
Chicago/Turabian StyleSatala, Catalin Bogdan, Zsolt Kovacs, Tivadar Bara, Jr., Ioan Jung, and Simona Gurzu. 2023. "Signet-Ring Cell Squamous Cell Carcinoma: A Biphenotypic Neoplasm of the Gastro-Esophageal Junction with Uncertain Biological Potential: Case Report and Literature Review" International Journal of Molecular Sciences 24, no. 11: 9535. https://doi.org/10.3390/ijms24119535