
Ganglionated Plexus Ablation Procedures to Treat Vasovagal Syncope


Heart and Vascular Institute, United Health Services, Johnson City, NY 13790, USA
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2023, 24(17), 13264; https://doi.org/10.3390/ijms241713264
Submission received: 7 August 2023
/
Revised: 21 August 2023
/
Accepted: 23 August 2023
/
Published: 26 August 2023
(This article belongs to the Special Issue Recent Advances in Hypertension and Cardiovascular Disease)
Abstract
:Vasovagal syncope (VVS) refers to a heterogeneous group of conditions whereby the cardiovascular reflexes normally controlling the circulation are interrupted irregularly in response to a trigger, resulting in vasodilation, bradycardia, or both. VVS affects one-third of the population at least once in their lifetime or by the age of 60, reduces the quality of life, and may cause disability affecting certain routines. It poses a considerable economic burden on society, and, despite its prevalence, there is currently no proven pharmacological treatment for preventing VVS. The novel procedure of ganglionated plexus (GP) ablation has emerged rapidly in the past two decades, and has been proven successful in treating syncope. Several parameters influence the success rate of GP ablation, including specific ablation sites, localization and surgical techniques, method of access, and the integration of other interventions. This review aims to provide an overview of the existing literature on the physiological aspects and clinical effectiveness of GP ablation in the treatment of VVS. Specifically, we explore the association between GPs and VVS and examine the impact of GP ablation procedures as reported in human clinical trials. Our objective is to shed light on the therapeutic significance of GP ablation in eliminating VVS and restoring normal sinus rhythm, particularly among young adults affected by this condition.
1. Introduction
Vasovagal syncope (VVS) is the most common form of neurally mediated reflex syncope (NMS), and usually refers to a heterogeneous group of conditions whereby the cardiovascular reflexes normally controlling the circulation are interrupted irregularly in response to a trigger. This results in vasodilation, bradycardia, or both, thereby promoting syncope [1]. Also known as reflex neurocardiogenic syncope, VVS is the most frequent cause of a temporary loss of consciousness, especially in young adults without a substantial heart disease [2]. VVS is a frequent clinical problem affecting one-third of the population at least once in their lifetime [3], or by the age of 60 [4,5]; it reduces the quality of life, and may cause disability affecting certain routines. It poses a considerable economic burden on society [6], and, despite its prevalence, there is currently no proven pharmacological treatment to prevent VVS [7]. The placement of dual-chamber pacing is effective in only a subgroup of VVS patients with significant asystolic NMS [8]. The novel procedure of ganglionated plexus (GP) ablation has developed rapidly in the past two decades, and has been proven successful in treating syncope. Several parameters influence the success rate of GP ablation, including specific ablation sites, localization and surgical techniques, method of access, and integration with other interventions. This review aims to provide an overview of the existing literature on the physiological aspects and clinical effectiveness of GP ablation in the treatment of VVS. Specifically, we explore the association between GPs and VVS and examine the impact of GP ablation procedures as reported in human clinical trials. Our objective is to shed light on the therapeutic significance of GP ablation in eliminating VVS and restoring normal sinus rhythm, particularly among young adults affected by this condition.
2. Cardiac Innervation
The heart is innervated by nerves from the brain and spinal cord, which either stimulate or inhibit physiological cardiac functions such as heart rate and contraction force. These nerves make up the cardiac autonomic nervous system (CANS) and include sympathetic and parasympathetic avenues. Under pathological conditions, the density of these nerve fibers in the heart may be altered, leading to either too much activation (hyper-innervation) or too little (hypo-innervation). This difference in innervation may cause a spatial imbalance in the activation of the heart, leading to cardiac autonomic dysfunction [9] related to the development and progression of cardiovascular diseases such as myocardial infarction (MI), arrhythmias, hypertension, heart failure [10,11,12,13], and several types of syncope [1,3].
Cardiac contraction and heart rate are achieved by the innervation of heart tissue via CANS. All neuronal elements, including cell bodies, axons, and dendrites, are arranged and bundled to form nerves; the sympathetic and parasympathetic nerves that comprise CANS originate in the central nervous system (CNS) as preganglionic nerves, while sensory afferent nerves originate in the heart tissue and blood vessels and project into the CNS. The difference between the sensory and autonomic nervous systems is the location of their ganglia, where synapses of the postganglionic neurons derive. Innervation of the heart is established via postganglionic synapses, where acetylcholine neurotransmitters bind to postsynaptic receptors located on the postganglionic neuron inside the heart.
Sensory nerves have a different anatomy and function than the sympathetic and parasympathetic nerves. Their main cardiac function is to provide feedback from baroreceptors on the aortic arch to the brain to maintain homeostasis. Sensory nerves provide information to the CNS and convey information on blood pressure, oxygen, carbon dioxide, and sugar levels in the blood. The sensory cell body gives rise to axons which sprout to both the heart and brain. The signal starts in the heart and is directed towards the brain via the neuronal cell body, whereas in sympathetic and parasympathetic nerves, the cell body also indicates the starting site of the signal. The sensory cell body lies within the dorsal root ganglia in the peripheral nervous system (PNS). Sensory nerves lay in close proximity to the autonomic nerves, and while responding to the cardiac stimulus, they relay back to the brain. Subsequently, the brain modulates output towards the heart, which is regulated by the parasympathetic and sympathetic nerves.
The cardiac autonomic nervous system can be simply divided into extrinsic and intrinsic elements according to the alignment and localization of nerve fibers, their cell bodies, and joint ganglia. The extrinsic, or central, CANS comprises central nerves originating in the brain and the spinal cord and forming the external ganglia, which then synapse with secondary neurons en route to the heart. The intrinsic CANS is confined within the heart and specifies small parasympathetic neurons that synapse with vagal sprouting nerves to activate their responses within the heart. The intrinsic system designates an extensive epicardial neural network comprising clustered nerve fibers of all types and parasympathetic cell bodies, which together constitute the GP, on both the atria and ventricles, as well as around pulmonary veins and great vessels [14]. These GPs, usually embedded within epicardial fat pads, vary in size from very few neurons to containing over 400 neurons [15,16]. Notably, the most dense autonomic innervation is localized at the posterior wall of the left atrium, predominantly at the pulmonary vein–atrial junction [16].
3. GP Anatomy and Physiology
The GPs are composed of a heterogeneous population of neurons, including efferent (into the heart), afferent (away from the heart), and many small interconnecting neurons comprising the bulk of the GP [17]. Additionally, GPs encompass both sympathetic and parasympathetic neural elements, and function as communication centers between the intrinsic and the extrinsic CANS, managing and controlling the electrophysiological, vascular, and contractile functions [18].
3.1. Anatomic Location of GPs
Anatomically, the four major atrial GPs are located in close proximity to the pulmonary veins (PVs), and each innervates one of the four PVs, as well as the surrounding atrial myocardium [15,16] (Figure 1). In addition, the fifth left lateral GP (LLGP) is located around the ligament of Marshall. These GPs can be identified during electrophysiological studies by applying high-frequency stimulation (HFS) (20 Hz) at the respective anatomical locations [19,20,21,22,23,24]. A positive response is defined as an increase in the R–R interval by >50% during atrial fibrillation (AF) [19]. The GPs were thus named based on their anatomical locations [19]. The complex anatomical layout and physiological interconnectivity of these GP sites is important to understanding the pathophysiology of VVS. Knowledge of GPs’ locations and their axonal projection pathways is important when considering targeted therapeutic interventions.
3.2. Physiology of GPs
As previously described, the CANS consists of parasympathetic, sympathetic, and sensory neural elements residing in different anatomical sites of the heart. It is recognized that parasympathetic and sympathetic systems reach their target organs via pre- and postganglionic nerve fibers. The cell bodies of postganglionic sympathetic and sensory neurons lie in the CNS and away from the heart, whereas cell bodies of postsynaptic parasympathetic neurons are very close to or within the heart (Figure 2). This distinct neuroanatomy facilitates selective vagal denervation, because only local postganglionic neuronal cell bodies are abolished by endocardial radiofrequency energy [25,26]. This is termed cardiac ablation, causing irreversible damage to vagal efferents, while postganglionic nerve fibers of sympathetic and sensory neurons are preserved, as they may be repaired by axonal regeneration [27,28] (Figure 2).
3.3. The Vagal Nerve
Under normal physiological conditions, the involuntary function of the heart is maintained by the balance of inhibitory (parasympathetic, vagal nerve) and excitatory (sympathetic) tones. This balance is facilitated by the brainstem and regulates the instantaneous heart rate. In certain instances, this balance is impaired due to an over-stimulated vagal response triggered by the vagal reflex. Physiologically, the vagal reflex, which can activate through multiple triggers, produces (1) severe cardioinhibition (causing asystole, serious bradycardia, and/or temporary complete AV block) and/or (2) vasodilation (the vasodepressor form, leading to critical and transient hypotension). In the case of cardioinhibition, which instigates prolonged asystole, the patient typically recovers spontaneously within minutes.
4. Neurophysiology of Ablation Targets
The mechanism of vagal stimulation is initiated by the local release of acetylcholine. There is an influx of acetylcholine stimulating the PV ganglia, inducing PV firing and reducing the action potential duration in the atrial myocytes in the PV sleeves, causing them to fire until suppressed [29], and thus maintaining AF. Studies have suggested that the serotonin signaling pathway is also over-regulated in VVS [30].
Several animal studies have shown that vagal efferent postganglionic neurons innervating the heart are primarily located in discrete epicardial ganglionic structures known as fat pads [31,32,33]. Subsequently, at these sites, emerging human studies have aimed to permanently denervate the vagal response by means of radiofrequency catheter ablation. The first studies were related to vagal-induced AF [34,35]. To define the exact localization of these fat pads, two different approaches were used: HFS-induced vagal reflex followed by atrial cardiac ablation to prevent AF [34] and fast Fourier transform (FFT) analysis to define GPs [35]. Good GP ablation resulted from a canine model of AF [36], promoting practitioners to target GP with ablation in patients.
Pachon et al. [37] were the first to propose specific vagal denervation by catheter ablation and spectral mapping for different arrhythmias and severe cases of cardioinhibitory syncope, giving rise to cardio-neuroablation (CNA). Since then, practitioners have used CNA to completely abolish or significantly reduce the vagal response, eradicating symptoms in >75% of patients, with limited complications for 14 years. As a result, CNA became an effective substitute to treat syncope syndromes in young patients without requiring a pacemaker implantation. The first patient was ablated in 2002 via CNA of the vagal nerve as the ultimate remedy for severe VVS [2]. Since then, significant improvements followed, and many remarkable authors have been able to reproduce the results [19,38,39,40,41,42,43]. Accordingly, in the last 20 years, catheter cardiac ablation has become a recognized, essential treatment strategy for VVS.
5. GP Ablation as the Fundamental Treatment for VVS
Several strategies have emerged to treat VVS by CNA and are currently used to target GP inputs within the heart. This evolving comprehensive approach includes anatomic and electrocardiographic mapping techniques, as well as physiologic and pharmacologic methods. The physiologically-guided approaches incorporate spectral mapping or HFS, whereas anatomically-guided methodologies purely target the GPs by location. Currently, there is no consensus on the best tactic for identifying atrial GP sites for CNA. Several additional parameters have not yet been confirmed; these include (1) the extent to which GP ablation is necessary to attenuate the vagal activity in patients, and (2) corroboration of the vagal denervation endpoints [44].
Three subtypes of VVS can be divided into the following broad categories: (1) pure cardioinhibition (with or without asystole); (2) pure vasodepression, in which hypotension occurs without a significant decrease in heart rate; and (3) a mixed type of cardioinhibition and vasodepression. Cardioinhibition is caused by abrupt and intense vagal reflex with or without defined triggers. Despite pharmacological and pacemaker implantation efforts, the latter are highly rejected by young patients. The Second Vasovagal Pacemaker Study confirmed the weak evidence of the efficacy of pacemaker therapy [45].
6. Ganglia Detection Methods
Several different approaches have been used for identification of parasympathetic autonomic ganglia in atria, including HFS, spectral analysis (SA), and an anatomical approach (AA). We comprehensively examine them herein and discuss the pros and cons of each. Prior to the use of ablation as the principal method to denervate the CANS, the achievement of pulmonary vein isolation (PVI) served as a suitable procedure. PVI is associated with denervation of the CANS and a significant reduction in AF recurrence [46]. Endocardial and epicardial access during PVI procedures has been associated with unintentional damage and incidental ablation at GP sites [47]. PVI, via thermal epicardial approaches, can result in the overlap of ablation lesions with numerous GP sites, while endocardial thermal approaches may induce collateral damage by conductive heating. One downfall to this technique is that conventional PV antrum isolation often unknowingly involves ablation of autonomic nerves positioned at the right anterior GP (RAGP), left superior GP (LSGP), and ligament of Marshall; however, the left inferior GP (LIGP) and right inferior GP (RIGP) remain largely intact [19]. Thus, Katritis et al. showed that >50% of their paroximal AF patients had recurrent syncope after 12 months of follow-up [48].
As opposed to the PVI technique [48,49], GP ablation can be performed either empirically, at their presumed anatomical locations [21,50,51], or the GP can be identified by applying HFS, as described by the Oklahoma group [19] and others [19,20,21,22,23,24] (Table 1 and Table 2). The Oklahoma group suggested that the GPs function as “integration centers” between extrinsic and intrinsic cardiac CANS [19].
6.1. Spectral Mapping Analysis (SA)
In 2004, Pachon et al. [35] used the SA of the atrial potentials, by which this group of researchers recorded and studied the whole frequency spectrum of the endocardial potentials by the FFT. Using this methodology, they found two kinds of atrial myocardium, the compact and the fibrillar [35,37]. The compact myocardium displayed a homogeneous spectrum with one main frequency around 40 Hz and uniform conduction which resulted from a mass of very well-connected cells [35,76,77]. The fibrillary myocardium appeared as a heterogeneous, rough, and fractioned spectrum with frequencies higher than 100 Hz, shifting its FFT to the right [35,76,77]. This conformation of cell bundles working in grouped filaments, as nerve fibers interweave with myocardial cells, alters myocardial conduction from compact to the fibrillary pattern [35,76,77]. The concurrent mixture of cells changes some electrical properties of the atrial wall and can easily be detected by deviations in the spectrum as “AF Nests” [40,41,42,43]. Thus, the distinguished endocardial fibrillary pattern was used as a marker of the neuro-myocardial interface. The fibrillary myocardium predominantly encompasses the anatomical regions of the cardiac GP [35,77,78], and, therefore, characterizes these sites as AF nests.
By applying online, real-time spectral mapping, it is possible to reveal the fibrillary myocardium (AF nests) to lead the ablation of the first neuron [79]. Using this method, nearly all postganglionic parasympathetic neurons may be eliminated and may not recover, whereas the sympathetic and sensory terminal fibers usually recuperate within weeks to months [79].
In 2011, Pachon et al. performed extensive right and left atrial ablation to treat patients with VVS, guided by spectral analysis for “AF nests” to complete vagal denervation. In their study, 40 of 43 patients remained free of syncope after a mean follow-up of 45 months [52]. Although never used as a stand-alone strategy to guide ablation, this technique has been attempted in combination with empirical anatomic ablation, HFS, or both by distinct research groups [37,38,39,52,55,70,71].
6.2. Anatomically-Guided Approach (AA) [21]
As a stand-alone tactic, the AA was initially performed in two VVS cases by Rebecchi et al. [69]. In this study, the authors achieved practical ablation through the right atria and around three major ganglia up until all atrial electrical activity was fully exterminated. A similar approach was used by Debruyne et al. [72] in a 16-year old female suffering from VVS. In their work, only the superior right atrial ganglion was targeted and ablated using a multi-electrode irrigated ablation catheter. A computed tomographic scan characterizing the cardio-neuromodulation (CardNM) methodology (discussed below) was also used in this study.
In the same year, Sun et al. [21] compared 10 individuals who underwent HFS-guided ablations (see below) vs. 47 individuals undergoing AA ablations, all of whom had VVS (Table 1). In the HFS-guided group, ablation was performed by selective vagal denervation, as previously described in Yao’s study [23] (see below). In the AA group, the four previously defined parasympathetic autonomic ganglia (PAG) were targeted, and the radiofrequency energy was initially delivered to induce a vagal response (VR) within 10 s; further energy was delivered for at least 30 s until complete inhibition of VR was achieved. Further ablation performances adjacent to the initial lesion were implemented to produce a cloudlike lesion pattern until five repeated ablation efforts failed to induce additional VR.
In the following year, in 2017, AA was used by Rivarola et al. [50] in a heterogeneous group of patients suffering from VVS, advanced AVB, or sinus arrest. They targeted six experimentally defined sites based on the combination of ganglion localization methods used in Yao’s (HFS) and Rebecchi’s (AA) studies [23,69]. In that year, Qin et al. prospectively studied AA ablations in 62 patients < 50 years old with symptomatic sinus bradycardia (SB). They were able to show that all patients presented with significantly improved symptom outcomes one year after ablation. Very recently, in 2021, two studies were conducted on VVS patients using the AA methodology [51,60].
6.3. High Frequency Stimulation (HFS) Approach
Po et al. developed a technique to localize and ablate the GP, which serves as the “integration centers” of the intrinsic cardiac autonomic nervous system (ICANS) [19]. Applying HFS to the atria causes two modes of response: (1) VR, defined as a major prolongation of the P-R or R-R intervals; or (2) a normal response, characterized by no or insignificant fluctuations on the PR or RR intervals. These two reactions reveal vagal innervation sites and normal atrial myocardium, respectively. This group of researchers identified the four major atrial GP sites by delivering HFS (20 Hz, 10–150 V, 1–10 ms pulse width) to atrial tissue where GPs were postulated to be localized. Locations displaying a parasympathetic response, which they randomly classified as a ≥50% increase in the mean RR interval during AF, was allocated as a GP site. A subsequent radiofrequency current was applied at that site to abolish the parasympathetic response [19].
The first group to practice selective HFS-guided GP ablation for the treatment of VVS was introduced by Yao et al., who reported successful outcomes in 10 patients with highly symptomatic VVS [23]. Selective HFS-guided GP ablation resulted in an impressive amelioration of their prodromal symptoms and no recurrence of syncope over a 30-month follow-up period [23]. The same group recently reported their long-term results of GP ablation in a larger cohort of patients with VVS [21], as 57 consecutive patients with highly symptomatic VVS received either anatomical sequential ablation of all four major atrial GPs in their recognized anatomical locations or HFS-guided GP ablation. During a mean 36-month follow-up, 91% of patients remained syncope-free, and prodromes were significantly reduced [21]. There were no differences between anatomical and HFS-guided GP ablation in terms of syncope or prodromes [21]. The HFS technique to guide ablation of the PAG for VVS showed benefits in three cohort studies [21,23,53] and four case reports [20,40,41,66].
6.4. Cardio-Neuromodulation (CardNM) Approach
CardNM is a novel approach which was instigated in recent years by Debruyne et al. [72] in order to achieve a faster procedure, minimizing procedural risks in patients compared to the conventional ablation strategies of left-sided or bi-atrial multiple sites [65]. The group demonstrated that it is possible to treat NMS, functional sinus bradycardia, and vagal-mediated AVB by performing CardNM [64,65,72,80], but not functional AVB [65]. The principal strategy of this technique is to approach the left endocardium by targeting the ARGP. To avoid exposing patients to additional unnecessary risks, the investigators believed that CardNM via the right-sided approach should be the first step for all NMS patients referred for ablation, and that targeting the IRGP methodologically should not be performed [81]. To avoid entering the left atrium, the authors used computed tomography and fusion imaging to restrict the procedure to the right heart cavities [80]. Indeed, the mean ablation time for these procedures is significantly shorter than most other CNA performances [64]. The long-term clinical results of CardNM are good, with persisting adequate partial sinus node vagolysis [65].
Qin et al. further confirmed that targeting the ARGP and the aorta-superior vena cava (Ao-SVC) fat pad (using the AA approach) is sufficient to terminate the vasovagal response, as the sinus rate (SR) increased considerably at these particular sites promptly post-ablation [61]. However, ablation to other areas, namely, SLPG, ILGP, and IRGP, did not substantially increase the mean SR in young patients (<50 years old) suffering from symptomatic SB [61]. This fact alone can potentially decrease the ablation time drastically, and should also minimize cardiac bruising.
6.5. Fractionation High-Density Mapping
The new methodology of high-density mapping in combination with an auto-algorithm fraction mapping system, developed by Aksu et al. to treat AF and VVS [54], may allow for better and faster localization of GPs during ablation, as a complement to anatomically-guided approaches. Recent studies investigating the treatment of VVS using this method [73,74] have shown improved results in these patients [54] compared to combined spectral analysis with HFS-mapping approaches (Table 1 and Table 2). Additional studies using this mapping strategy, in addition to longer follow-ups for possible VVS recurrence, are still lacking.
7. Routes to Access Ablation
As mentioned above, there are several anatomical sites at which to approach the ablation, but the main ones are through the left or right atrium, or both, and sometimes also through the superior vena cava (SVC). Very seldom, other tactics are used. Authors have discussed the pros and cons to each approachable anatomical site, and we summarize their justifications here.
The right atrium GP controls the function of the SA node; electrical stimulation of the RAGP reduces the SR [82]. The SLGP of the left vagosympathetic trunk traverses with the RAGP before proceeding to the SA node; however, Qin et al. showed that RAGP may serve as a “gateway” through which the cardiac autonomic nervous system can modulate the sinus node [61]. Furthermore, the authors showed that ablation of the Ao-SVC GP, which integrates most of the efferent vagal fibers to the atria and then projects onto the RAGP and RIGP [33], suppresses the effects of vagal stimulation on SR slowing [60] and increases the SR [24,61]. Thus, the authors suggest that there is a RAGP-independent and a RAGP-dependent pathway [61].
8. Post-Ablation Validations
Several useful methods have been applied in order to evaluate the completion and success of the ablation. Extracardiac vagal stimulation remains the best tool with which to identify and achieve the procedural endpoint [83], and may more accurately distinguish patients who are truly vagally suppressed following CNA [66]. The atrophine test immediately following the ablation, as well as the tilt-test in the chronic phase post-neuroablation, are used to assess the amount of reinnervation and the reappearance of the VR [52]. Heart rate variability (HRV) is another measure used long-term through the 24 h Holter recording. HRV is affected by age, sex, physical fitness, clinical conditions, rest alertness, sleep, and medication [84,85,86], which are all stable parameters during the 24 h testing period.
As the gold standard, the 24 h SDNN (standard deviation of all normal R-R intervals) predicts morbidity and mortality in high-risk and comorbid patients, where SDNN values < 50 ms are classified as at risk, 50–100 ms as compromised health, and >100 ms as healthy [87]. For CNA procedure success, practitioners use the 24 h Holter for SDNN detection, which markedly decreases due to reduced vagal response after the ablation. This apparent reduction, triggered by denervation of the parasympathetic tone, should be distinguished from the declining SDNN values that predict cardiac risk [87]. Herein, we indicate the success of each reported ablation by HRV p-values pre- and post-ablation (Table 1 and Table 2) during the period of follow-up.
9. Discussion
GP ablation appears to be an efficacious technique for improving outcomes, primarily in patients with neurocardiogenic syncopes. Nonetheless, some very important questions remain unanswered. The long-term outcomes of GP ablation, the precise location and depth of GPs, and the ultimate mechanism of GP ablation to improve VVS are still not fully understood. A recent study by Xu et al. validated that HFS and AA are both efficient and safe approaches to successful VVS relief [57].
Collateral damage is a major disadvantage of current thermal ablation techniques, and introduces a risk of damaging the myocardium and the surrounding tissue. Alternative, less damaging methods are currently available to treat paroxysmal and persistent AF, but do not fix the physiological effects produced by GPs during VVS. The pulsed-field ablation technique is tissue-selective, only damaging myocardial cells [88] and leaving vagal nerves intact and activated. This technique uses non-thermal high-voltage energy to kill cardiomyocytes [89], but not the parasympathetic and sympathetic nerves.
Another problem is the difficulty of delivering precise, appropriate energy to GPs. While GPs, in association with PVs, are accessed with relative ease, others are found in concealed locations. Overall, there is significant complexity involved in catheter positioning both within the pericardial space and the heart itself. A more efficient and effective visualization of GPs using imaging techniques may provide useful information for improved localization. These advances have significantly propelled research over the last decade. While the understanding of GP locations is sometimes obscure, this may be due to the degree of anatomical variability between individuals [47].
However, the specifics in terms of report accuracy of the GPs that have been targeted in some research papers remain ambiguous, with some studies not including nor clearly describing which GPs were targeted or where they were ablated [19,51,62,63]. This causes difficulty when comparing results from different studies targeting specific GPs associated with the maintenance of neural pathways and their subsequent effects on the SA and AV nodes [22,90]. Due to the different techniques and study designs in the literature, it is difficult to assess and make a true comparison regarding success. A recent study confirmed that the order of the targeted GPs affected the occurrence rate of VR and BP reduction during cardio-neuroablation [58]. The RAGP was a critical target for increasing HR and inhibiting VR during the procedure; thus, it may be an integration center in the regulation of other GPs of the LA [58,59].
HRV has been found to be a predictor of ablation success, and is a useful, non-invasive tool for investigating cardiac autonomic tone [91,92]; it measures the fluctuations of time intervals between consecutive heartbeats [85]. It is evident that sufficient disruption of VR results in increased HR and AF relief. It is still possible that post-procedural efficacy may be short-term, due to incomplete ablation of the GPs and the regeneration and formation of new re-entrant pathways in the proximity of the GP.
Recurrent syncope episodes post-CNA are not well described in the literature. Long-term follow-up studies are needed to determine whether nerve regeneration leads to the recurrence of syncope symptoms. A recent report suggested that reinnervation of GPs, in some cases, may be the cause of recurrent syncopes 7 months post-ablation [66]; further indications are warranted. Needless to say, the quality of life post-ablation in patients with previous VVS was improved significantly after a 1-year follow up [93].
Currently, sample size is a major limitation in many studies, with numbers ranging from individual case studies to research including up to 123 patients [63]. Evidently, variation in patient population significantly influence percent outcomes, making it difficult to draw accurate comparisons. From the expansive research and meta-analyses performed to study GP ablation, most results show relief from VVS, both initially and in the long term [21,50,51,55,60,62,63]. While much work is still needed in order to achieve consistency between experiments, it is evident that the potential exists for significant advances in the treatment of VVS through targeted ablation of GP sites.
The use of GP ablation as an adjunctive technique to enhance the outcomes of PVI isolation in patients with paroxysmal AF appears to be both safe and effective. Potential complications associated with GP ablation may rarely occur, especially after LA procedures, such as cardiac perforation, sinus node dysfunction, AV block, phrenic nerve paralysis, and stroke. Two patients (out of sixty-six) developed postoperative bradycardia following HFS-directed CAN, but quickly recovered with drug treatment [57]. In another case of AF, where the AA-CAN was approached from the RA, symptomatic inappropriate sinus tachycardia had occurred in the patient, but completely resolved after 1 month of therapy with a low dose of β-blockers [94]. Finally, two patients experienced sinus node artery occlusion after RA followed by LA-CAN [95].
Encouraging results have been observed regarding GP ablation in patients with VVS. However, several important questions remain unanswered. Firstly, the long-term outcomes of GP ablation, particularly over a period of 5 years, have not been thoroughly studied. Secondly, the precise mechanism through which GP ablation leads to improved outcomes is not fully understood. To address these uncertainties, it is recommended that a randomized, preferably blinded, placebo-controlled trial be conducted to elucidate the true role of GP ablation in VVS patients. Furthermore, the correlation between the clinical outcomes and the extent or technique of ablation remains unknown. Lastly, CNA is an innovative and promising therapeutic option for certain patients with VVS. Existing observational evidence highlights significant success in eliminating syncope in this population, and the occurrence of recurrent syncope following CNA has not been extensively described.
10. Conclusions
Several strategies for atrial autonomic denervation have been reported. However, the optimal technique for identifying atrial GP sites, either physiologically guided (SA, HFS) or anatomically guided, has not been established yet [23,37,41,50,52,82]. Further, there is no consensus on the extension of GP ablation for attenuating vagal activity for the treatment of functional bradycardias and VVS, whether ablating all atrial GPs, selectively ablating GPs on both sides of the inter-atrial septum, or exclusively targeting specific areas of the RA or LA GP [21,23,37,39,41,42,50,52,71]. In contrast to pharmacological therapy and pacemaker implantation, GP ablation is designed to target the fundamental problems, which are disturbances in the ICANS. Although the details of CNA required to treat VVS remain to be determined, the results presented in this review indicate, collectively, that GP ablation is an effective and safe treatment option for patients with refractory VVS. This novel technique should be evaluated in large-scale, randomized, controlled trials to demonstrate the efficiency, reliability, and appropriate patient selection criteria.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AA | Anatomical approach |
| ARGP | Anterior right ganglionated plexus |
| Ao-SVC | Aorta-superior vena cava |
| AF | Atrial fibrillation |
| AVB | Atrioventricular block |
| CANS | Cardiac autonomic nervous system |
| CNA | Cardio-neuroablation |
| CardNM | Cardio-neuromodulation |
| CNS | Central nervous system |
| FFT | Fourier transform |
| GP | Ganglionated plexus |
| HRV | Heart rate variability |
| HFS | High-frequency stimulation |
| ILGP | Inferior left ganglionated plexus |
| IRGP | Inferior right ganglionated plexus |
| ICANS | Intrinsic cardiac autonomic nervous system |
| LA | Left atrium |
| NMS | Neurally mediated syncope |
| PAG | Parasympathetic autonomic ganglia |
| PNS | Peripheral nervous system |
| PV | Pulmonary vein |
| PVI | pulmonary vein isolation |
| RA | Right atrium |
| SB | Sinus bradycardia |
| SR | Sinus rate |
| SA | Spectral mapping analysis |
| SDNN | Standard deviation of all normal R-R intervals |
| SLPG | Superior left ganglionated plexus |
| SVC | Superior vena cava |
| VR | Vagal response |
| VVS | Vasovagal syncope |
References
- Task Force for the Diagnosis and Management of Syncope; European Society of Cardiology (ESC); European Heart Rhythm Association (EHRA); Heart Failure Association (HFA); Heart Rhythm Society (HRS); Moya, A.; Sutton, R.; Ammirati, F.; Blanc, J.-J.; Brignole, M.; et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur. Heart J. 2009, 30, 2631–2671. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, R.S.; Grubb, B.P., 2nd; Olshansky, B.; Shen, W.-K.; Calkins, H.; Brignole, M.; Raj, S.R.; Krahn, A.D.; Morillo, C.A.; Stewart, J.M.; et al. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm 2015, 12, e41–e63. [Google Scholar] [CrossRef]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.-C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martín, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Ganzeboom, K.S.; Mairuhu, G.; Reitsma, J.B.; Linzer, M.; Wieling, W.; VAN Dijk, N. Lifetime Cumulative Incidence of Syncope in the General Population: A Study of 549 Dutch Subjects Aged 35–60 Years. J. Cardiovasc. Electrophysiol. 2006, 17, 1172–1176. [Google Scholar] [CrossRef]
- Serletis, A.; Rose, S.; Sheldon, A.G.; Sheldon, R.S. Vasovagal syncope in medical students and their first-degree relatives. Eur. Heart J. 2006, 27, 1965–1970. [Google Scholar] [CrossRef]
- Sutton, R.; Benditt, D.G. Epidemiology and economic impact of cardiac syncope in western countries. Future Cardiol. 2012, 8, 467–472. [Google Scholar] [CrossRef]
- Romme, J.J.; Reitsma, J.B.; Black, C.N.; Colman, N.; Scholten, R.J.; Wieling, W.; Van Dijk, N. Drugs and pacemakers for vasovagal, carotid sinus and situational syncope. Cochrane Database Syst. Rev. 2011, 5, CD004194. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Menozzi, C.; Moya, A.; Andresen, D.; Blanc, J.J.; Krahn, A.D.; Wieling, W.; Beiras, X.; Deharo, J.C.; Russo, V.; et al. Pacemaker therapy in patients with neurally mediated syncope and documented asystole: Third International Study on Syncope of Uncertain Etiology (ISSUE-3): A randomized trial. Circulation 2012, 125, 2566–2571. [Google Scholar] [CrossRef]
- Kimura, K.; Ieda, M.; Kanazawa, H.; Yagi, T.; Tsunoda, M.; Ninomiya, S.-I.; Kurosawa, H.; Yoshimi, K.; Mochizuki, H.; Yamazaki, K.; et al. Cardiac sympathetic rejuvenation: A link between nerve function and cardiac hypertrophy. Circ. Res. 2007, 100, 1755–1764. [Google Scholar] [CrossRef]
- Mj, S.; Dp, Z. Role of the autonomic nervous system in modulating cardiac arrhythmias. Circ. Res. 2014, 114, 1004–1021. [Google Scholar]
- Mancia, G.; Grassi, G. The autonomic nervous system and hypertension. Circ. Res. 2014, 114, 1804–1814. [Google Scholar] [CrossRef]
- Florea, V.G.; Cohn, J.N. The Autonomic Nervous System and Heart Failure. Circ. Res. 2014, 114, 1815–1826. [Google Scholar] [CrossRef] [PubMed]
- Diller, G.-P.; Dimopoulos, K.; Okonko, D.; Uebing, A.; Broberg, C.S.; Babu-Narayan, S.; Bayne, S.; Poole-Wilson, P.A.; Sutton, R.; Francis, D.P.; et al. Heart Rate Response during Exercise Predicts Survival in Adults with Congenital Heart Disease. J. Am. Coll. Cardiol. 2006, 48, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Hasan, W. Autonomic cardiac innervation: Development and adult plasticity. Organogenesis 2013, 9, 176–193. [Google Scholar] [CrossRef]
- Armour, J.A.; Murphy, D.A.; Yuan, B.-X.; MacDonald, S.; Hopkins, D.A. Gross and microscopic anatomy of the human intrinsic cardiac nervous system. Anat. Rec. 1997, 247, 289–298. [Google Scholar] [CrossRef]
- Pauza, D.H.; Skripka, V.; Pauziene, N.; Stropus, R. Morphology, distribution, and variability of the epicardiac neural ganglionated subplexuses in the human heart. Anat. Rec. 2000, 259, 353–382. [Google Scholar] [CrossRef]
- Shivkumar, K.; Ajijola, O.A.; Anand, I.; Armour, J.A.; Chen, P.-S.; Esler, M.; De Ferrari, G.M.; Fishbein, M.C.; Goldberger, J.J.; Harper, R.M.; et al. Clinical neurocardiology defining the value of neuroscience-based cardiovascular therapeutics. J. Physiol. 2016, 594, 3911–3954. [Google Scholar] [CrossRef] [PubMed]
- Armour, J.A.; Ardell, J.L.; Rajendran, P.S.; Nier, H.A.; KenKnight, B.H.; Hardwick, J.C.; Ryan, S.E.; Powers, E.N.; Southerland, E.M.; Gourine, A.; et al. Cardiac neuronal hierarchy in health and disease. Am. J. Physiol. Integr. Comp. Physiol. 2004, 287, R262–R271. [Google Scholar] [CrossRef] [PubMed]
- Po, S.S.; Nakagawa, H.; Jackman, W.M. Localization of Left Atrial Ganglionated Plexi in Patients with Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2009, 20, 1186–1189. [Google Scholar] [CrossRef]
- Lu, Y.; Wei, W.; Upadhyay, G.A.; Tung, R. Catheter-Based Cardio-Neural Ablation for Refractory Vasovagal Syncope: First U.S. Report. JACC Case Rep. 2020, 2, 1161–1165. [Google Scholar] [CrossRef]
- Sun, W.; Zheng, L.; Qiao, Y.; Shi, R.; Hou, B.; Wu, L.; Guo, J.; Zhang, S.; Yao, Y. Catheter Ablation as a Treatment for Vasovagal Syncope: Long-Term Outcome of Endocardial Autonomic Modification of the Left Atrium. J. Am. Heart Assoc. 2016, 5, e003471. [Google Scholar] [CrossRef] [PubMed]
- Malcolme-Lawes, L.C.; Lim, P.B.; Wright, I.; Kojodjojo, P.; Koa-Wing, M.; Jamil-Copley, S.; Dehbi, H.-M.; Francis, D.P.; Davies, D.W.; Peters, N.S.; et al. Characterization of the Left Atrial Neural Network and its Impact on Autonomic Modification Procedures. Circ. Arrhythmia Electrophysiol. 2013, 6, 632–640. [Google Scholar] [CrossRef]
- Yao, Y.; Shi, R.; Wong, T.; Zheng, L.; Chen, W.; Yang, L.; Huang, W.; Bao, J.; Zhang, S. Endocardial autonomic denervation of the left atrium to treat vasovagal syncope: An early experience in humans. Circ. Arrhythm Electrophysiol. 2012, 5, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Jiang, W.; Zhou, L.; Wang, Y.; Zhang, X.; Wu, S.; Xu, K.; Liu, X. Atrial autonomic denervation for the treatment of long-standing symptomatic sinus bradycardia in non-elderly patients. J. Interv. Card. Electrophysiol. 2015, 43, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Morillo, C.A.; Eckberg, D.L.; Ellenbogen, K.A.; Beightol, L.A.; Hoag, J.B.; Tahvanainen, K.U.; Kuusela, T.A.; Diedrich, A.M. Vagal and Sympathetic Mechanisms in Patients with Orthostatic Vasovagal Syncope. Circulation 1997, 96, 2509–2513. [Google Scholar] [CrossRef]
- Armour, J.A. Potential clinical relevance of the ‘little brain’ on the mammalian heart. Exp. Physiol. 2008, 93, 165–176. [Google Scholar] [CrossRef]
- Wilson, R.F.; Laxson, D.D.; Christensen, B.V.; McGinn, A.L.; Kubo, S.H. Regional differences in sympathetic reinnervation after human orthotopic cardiac transplantation. Circulation 1993, 88, 165–171. [Google Scholar] [CrossRef]
- Bernardi, L.; Valenti, C.; Wdowczyck-Szulc, J.; Frey, A.W.; Rinaldi, M.; Spadacini, G.; Passino, C.; Martinelli, L.; Viganò, M.; Finardi, G. Influence of Type of Surgery on the Occurrence of Parasympathetic Reinnervation after Cardiac Transplantation. Circulation 1998, 97, 1368–1374. [Google Scholar] [CrossRef]
- Lemola, K.; Chartier, D.; Yeh, Y.-H.; Dubuc, M.; Cartier, R.; Armour, A.; Ting, M.; Sakabe, M.; Shiroshita-Takeshita, A.; Comtois, P.; et al. Pulmonary vein region ablation in experimental vagal atrial fibrillation: Role of pulmonary veins versus autonomic ganglia. Circulation 2008, 117, 470–477. [Google Scholar] [CrossRef]
- Sheldon, R.S.; Sandhu, R.K. The Search for the Genes of Vasovagal Syncope. Front. Cardiovasc. Med. 2019, 6, 175. [Google Scholar] [CrossRef]
- Randall, W.C.; Milosavljevic, M.; Wurster, R.D.; Geis, G.S.; Ardell, J.L. Selective vagal innervation of the heart. Ann. Clin. Lab. Sci. 1986, 16, 198–208. [Google Scholar] [PubMed]
- Randall, W.C.; Ardell, J.L.; O’Toole, M.F.; Wurster, R.D. Differential autonomic control of SAN and AVN regions of the canine heart: Structure and function. Prog. Clin. Biol. Res. 1988, 275, 15–31. [Google Scholar] [PubMed]
- Chiou, C.-W.; Eble, J.N.; Zipes, D.P. Efferent Vagal Innervation of the Canine Atria and Sinus and Atrioventricular Nodes. The third fat pad. Circulation 1997, 95, 2573–2584. [Google Scholar] [CrossRef] [PubMed]
- Scanavacca, M.I.; Pisani, C.F.; Hachul, D.; Trombetta, I.C.; Lara, S.; Hardy, C.; Grupi, C.; Darrieux, F.; Negrão, C.E.; Sosa, E.A. P5-70: Selective atrial vagal denervation guided by evoked vagal reflex to treat patients with paroxysmal atrial fibrillation. Heart Rhythm 2006, 3, S283. [Google Scholar] [CrossRef]
- Jose, C.P.M.; Enrique, I.P.M.; Juan, C.P.M.; Lobo, T.J.; Pachon, M.Z.; Vargas, R.N.A.; Pachon, D.Q.V.; Lopez M, F.J.; Jatene, A.D. A new treatment for atrial fibrillation based on spectral analysis to guide the catheter RF-ablation. Europace 2004, 6, 590–601. [Google Scholar]
- Lu, Z.; Scherlag, B.J.; Lin, J.; Niu, G.; Fung, K.-M.; Zhao, L.; Ghias, M.; Jackman, W.M.; Lazzara, R.; Jiang, H.; et al. Atrial fibrillation begets atrial fibrillation: Autonomic mechanism for atrial electrical remodeling induced by short-term rapid atrial pacing. Circ. Arrhythm Electrophysiol. 2008, 1, 184–192. [Google Scholar] [CrossRef]
- Pachon, J.C.; Pachon, E.I.; Pachon, J.C.; Lobo, T.J.; Pachon, M.Z.; Vargas, R.N.A.; Jatene, A.D. ‘Cardioneuroablation’—New treatment for neurocardiogenic syncope, functional AV block and sinus dysfunction using catheter RF-ablation. Europace 2005, 7, 1–13. [Google Scholar] [CrossRef]
- Aksu, T.; Golcuk, E.; Yalin, K.; Guler, T.E.; Erden, I. Simplified Cardioneuroablation in the Treatment of Reflex Syncope, Functional AV Block, and Sinus Node Dysfunction. Pacing Clin. Electrophysiol. 2015, 39, 42–53. [Google Scholar] [CrossRef]
- Rivarola, E.; Hardy, C.; Sosa, E.; Hachul, D.; Furlan, V.; Raimundi, F.; Scanavacca, M. Selective atrial vagal denervation guided by spectral mapping to treat advanced atrioventricular block. Europace 2015, 18, 445–449. [Google Scholar] [CrossRef]
- Liang, Z.; Jiayou, Z.; Zonggui, W.; Dening, L. Selective Atrial Vagal Denervation Guided by Evoked Vagal Reflex to Treat Refractory Vasovagal Syncope. Pacing Clin. Electrophysiol. 2012, 35, e214–e218. [Google Scholar] [CrossRef]
- Scanavacca, M.; Hachul, D.; Pisani, C.; Sosa, E. Selective Vagal Denervation of the Sinus and Atrioventricular Nodes, Guided by Vagal Reflexes Induced by High Frequency Stimulation, to Treat Refractory Neurally Mediated Syncope. J. Cardiovasc. Electrophysiol. 2009, 20, 558–563. [Google Scholar] [CrossRef]
- Fukunaga, M.; Wichterle, D.; Peichl, P.; Aldhoon, B.; Čihák, R.; Kautzner, J. Differential effect of ganglionic plexi ablation in a patient with neurally mediated syncope and intermittent atrioventricular block. Europace 2016, 19, 119–126. [Google Scholar] [CrossRef]
- Stavrakis, S.; Scherlag, B.J.; Po, S.S. Autonomic modulation: An emerging paradigm for the treatment of cardiovascular diseases. Circ. Arrhythm Electrophysiol. 2012, 5, 247–248. [Google Scholar] [CrossRef]
- Pachon M, J.C.; Pachon M, E.I.; Santillana P, T.G.; Lobo, T.J.; Pachon, C.T.C.; Pachon M, J.C.; Albornoz V, R.N.; Zerpa A, J.C. Simplified Method for Vagal Effect Evaluation in Cardiac Ablation and Electrophysiological Procedures. JACC Clin. Electrophysiol. 2015, 1, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Sheldon, R.; Thorpe, K.E.; Roberts, R.S.; Ellenbogen, K.A.; Wilkoff, B.L.; Morillo, C.; Gent, M.; VPS II Investigators. Pacemaker therapy for prevention of syncope in patients with recurrent severe vasovagal syncope: Second Vasovagal Pacemaker Study (VPS II): A randomized trial. JAMA 2003, 289, 2224–2229. [Google Scholar] [CrossRef] [PubMed]
- Pappone, C.; Santinelli, V.; Manguso, F.; Vicedomini, G.; Gugliotta, F.; Augello, G.; Mazzone, P.; Tortoriello, V.; Landoni, G.; Zangrillo, A.; et al. Pulmonary Vein Denervation Enhances Long-Term Benefit after Circumferential Ablation for Paroxysmal Atrial Fibrillation. Circulation 2004, 109, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Zdarska, J.; Osmancik, P.; Budera, P.; Herman, D.; Prochazkova, R.; Talavera, D.; Straka, Z. The absence of effect of ganglionated plexi ablation on heart rate variability parameters in patients after thoracoscopic ablation for atrial fibrillation. J. Thorac. Dis. 2017, 9, 4997–5007. [Google Scholar] [CrossRef] [PubMed]
- Katritsis, D.G.; Giazitzoglou, E.; Zografos, T.; Pokushalov, E.; Po, S.S.; Camm, A.J. Rapid pulmonary vein isolation combined with autonomic ganglia modification: A randomized study. Heart Rhythm 2011, 8, 672–678. [Google Scholar] [CrossRef]
- Katritsis, D.G.; Pokushalov, E.; Romanov, A.; Giazitzoglou, E.; Siontis, G.C.M.; Po, S.S.; Camm, A.J.; Ioannidis, J.P.A. Autonomic denervation added to pulmonary vein isolation for paroxysmal atrial fibrillation: A randomized clinical trial. J. Am. Coll. Cardiol. 2013, 62, 2318–2325. [Google Scholar] [CrossRef]
- Rivarola, E.W.; Hachul, D.; Wu, T.; Pisani, C.; Hardy, C.; Raimundi, F.; Melo, S.; Darrieux, F.; Scanavacca, M. Targets and End Points in Cardiac Autonomic Denervation Procedures. Circ. Arrhythm Electrophysiol. 2017, 10, e004638. [Google Scholar] [CrossRef]
- Zheng, L.; Sun, W.; Qiao, Y.; Hou, B.; Guo, J.; Killu, A.; Yao, Y. Symptomatic Premature Ventricular Contractions in Vasovagal Syncope Patients: Autonomic Modulation and Catheter Ablation. Front. Physiol. 2021, 12, 653225. [Google Scholar] [CrossRef]
- Pachon, J.C.M.; Pachon, E.I.M.; Pachon, M.Z.C.; Lobo, T.J.; Pachon, J.C.M.; Santillana, T.G.P. Catheter ablation of severe neurally meditated reflex (neurocardiogenic or vasovagal) syncope: Cardioneuroablation long-term results. Europace 2011, 13, 1231–1242. [Google Scholar] [CrossRef] [PubMed]
- Aksu, T.; Guler, T.E.; Bozyel, S.; Ozcan, K.S.; Yalin, K.; Mutluer, F.O. Cardioneuroablation in the treatment of neurally mediated reflex syncope: A review of the current literature. Turk Kardiyol. Dern. Ars. 2016, 45, 4–41. [Google Scholar] [CrossRef] [PubMed]
- Aksu, T.; Guler, T.E.; Mutluer, F.O.; Bozyel, S.; Golcuk, S.E.; Yalin, K. Electroanatomic-mapping-guided cardioneuroablation versus combined approach for vasovagal syncope: A cross-sectional observational study. J. Interv. Card. Electrophysiol. 2019, 54, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Pachon-M, J.C.; Pachon-M, E.I.; Pachon, C.T.C.; Santillana-P, T.G.; Lobo, T.J.; Pachon-M, J.C.; Zerpa-A, J.C.; Cunha-P, M.Z.; Higuti, C.; Ortencio, F.A.; et al. Long-Term Evaluation of the Vagal Denervation by Cardioneuroablation Using Holter and Heart Rate Variability. Circ. Arrhythmia Electrophysiol. 2020, 13, e008703. [Google Scholar] [CrossRef]
- Aksu, T.; Yalin, K.; Mutluer, F.O.; Farhat, K.; Tanboga, H.I.; Po, S.S.; Stavrakis, S. The impact of the clinical diagnosis on the vagal response and heart rate after ganglionated plexus ablation. J. Interv. Card. Electrophysiol. 2022, 1–8. [Google Scholar] [CrossRef]
- Xu, L.; Zhao, Y.; Duan, Y.; Wang, R.; Hou, J.; Wang, J.; Chen, B.; Yang, Y.; Xue, X.; Zhao, Y.; et al. Clinical Efficacy of Catheter Ablation in the Treatment of Vasovagal Syncope. J. Clin. Med. 2022, 11, 5371. [Google Scholar] [CrossRef]
- Hu, F.; Zheng, L.; Liu, S.; Shen, L.; Liang, E.; Liu, L.; Wu, L.; Ding, L.; Yao, Y. The impacts of the ganglionated plexus ablation sequence on the vagal response, heart rate, and blood pressure during cardioneuroablation. Auton. Neurosci. 2021, 233, 102812. [Google Scholar] [CrossRef]
- Hu, F.; Zheng, L.; Liang, E.; Ding, L.; Wu, L.; Chen, G.; Fan, X.; Yao, Y. Right anterior ganglionated plexus: The primary target of cardioneuroablation? Heart Rhythm 2019, 16, 1545–1551. [Google Scholar] [CrossRef]
- Calo, L.; Rebecchi, M.; Sette, A.; Sciarra, L.; Borrelli, A.; Scara, A.; Grieco, D.; Politano, A.; Sgueglia, M.; De Luca, L.; et al. Catheter ablation of right atrial ganglionated plexi to treat cardioinhibitory neurocardiogenic syncope: A long-term follow-up prospective study. J. Interv. Card. Electrophysiol. 2021, 61, 499–510. [Google Scholar] [CrossRef]
- Qin, M.; Zhang, Y.; Liu, X.; Jiang, W.-F.; Wu, S.-H.; Po, S. Atrial Ganglionated Plexus Modification: A Novel Approach to Treat Symptomatic Sinus Bradycardia. JACC Clin. Electrophysiol. 2017, 3, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Aksu, T.; Padmanabhan, D.; Shenthar, J.; Yalin, K.; Gautam, S.; Valappil, S.P.; Banavalikar, B.; Guler, T.E.; Bozyel, S.; Tanboga, I.H.; et al. The benefit of cardioneuroablation to reduce syncope recurrence in vasovagal syncope patients: A case-control study. J. Interv. Card. Electrophysiol. 2021, 63, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Tu, B.; Wu, L.; Hu, F.; Fan, S.; Liu, S.; Liu, L.; Ding, L.; Zheng, L.; Yao, Y. Cardiac deceleration capacity as an indicator for cardioneuroablation in patients with refractory vasovagal syncope. Heart Rhythm 2022, 19, 562–569. [Google Scholar] [CrossRef]
- Debruyne, P.; Rossenbacker, T.; Collienne, C.; Roosen, J.; Ector, B.; Janssens, L.; Charlier, F.; Vankelecom, B.; Dewilde, W.; Wijns, W. Unifocal Right-Sided Ablation Treatment for Neurally Mediated Syncope and Functional Sinus Node Dysfunction under Computed Tomographic Guidance. Circ. Arrhythmia Electrophysiol. 2018, 11, e006604. [Google Scholar] [CrossRef] [PubMed]
- Debruyne, P.; Rossenbacker, T.; Janssens, L.; Collienne, C.; Ector, J.; Haemers, P.; Waroux, J.-B.l.P.d.; Bazelmans, C.; Boussy, T.; Wijns, W. Durable Physiological Changes and Decreased Syncope Burden 12 Months after Unifocal Right-Sided Ablation Under Computed Tomographic Guidance in Patients with Neurally Mediated Syncope or Functional Sinus Node Dysfunction. Circ. Arrhythmia Electrophysiol. 2021, 14, e009747. [Google Scholar] [CrossRef]
- Thurber, C.J.; Sneider, D.R.; Sauer, W.H.; Kapur, S. Recurrent vasovagal syncope following successful cardioneuroablation. Heart Rhythm Case Rep. 2022, 8, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Sarabanda, A.V.; Melo, S.L.; Rivarola, E.; Hachul, D.; Scanavacca, M. Anatomically guided atrial ganglionated plexus ablation evaluated by extracardiac vagal stimulation for vagally mediated atrioventricular block. Heart Rhythm Case Rep. 2021, 7, 301–305. [Google Scholar] [CrossRef]
- Suenaga, H.; Murakami, M.; Tani, T.; Saito, S. Frequent neurally mediated reflex syncope in a young patient with dextrocardia: Efficacy of catheter ablation of the superior vena cava-aorta ganglionated plexus. J. Arrhythmia 2014, 31, 172–176. [Google Scholar] [CrossRef]
- Rebecchi, M.; de Ruvo, E.; Strano, S.; Sciarra, L.; Golia, P.; Martino, A.; Calò, L. Ganglionated plexi ablation in right atrium to treat cardioinhibitory neurocardiogenic syncope. J. Interv. Card. Electrophysiol. 2012, 34, 231–235. [Google Scholar] [CrossRef]
- Pachon M, J.C.; Pachon M, E.I.; Lobo, T.J.; Pachon, M.J.C.; Pachon, M.Z.C.; Vargas, R.N.A.; Manrique, R.M.; Jatene, A.D. Syncopal High-Degree AV Block Treated with Catheter RF Ablation without Pacemaker Implantation. Pacing Clin. Electrophysiol. 2006, 29, 318–322. [Google Scholar] [CrossRef]
- Aksu, T.; Golcuk, S.E.; Guler, T.E.; Yalin, K.; Erden, I. Functional permanent 2:1 atrioventricular block treated with cardioneuroablation: Case report. Heart Rhythm Case Rep. 2015, 1, 58–61. [Google Scholar] [CrossRef]
- Debruyne, P. “Cardio-Neuromodulation” with a Multi-Electrode Irrigated Catheter A Potential New Approach for Patients with Cardio-Inhibitory Syncope. J. Cardiovasc. Electrophysiol. 2016, 27, 1110–1113. [Google Scholar] [CrossRef]
- Osorio, J.; Doud, D.M.; Aksu, T. Fractionation Mapping by Using a High-density Catheter to Map Ganglionated Plexus Sites during Sinus Rhythm. J. Innov. Card. Rhythm Manag. 2021, 12, 7–8. [Google Scholar] [CrossRef]
- John, L.; Mullis, A.; Payne, J.; Tung, R.; Aksu, T.; Winterfield, J. Fractionation Mapping of the Ganglionated Plexi for Cardioneuroablation. J. Innov. Card. Rhythm Manag. 2021, 12, 4473–4476. [Google Scholar] [CrossRef] [PubMed]
- Aksu, T.; Guler, T.E.; Bozyel, S.; Yalin, K. Selective vagal innervation principles of ganglionated plexi: Step-by-step cardioneuroablation in a patient with vasovagal syncope. J. Interv. Card. Electrophysiol. 2021, 60, 453–458. [Google Scholar] [CrossRef]
- Singhal, R.; Lo, L.-W.; Lin, Y.-J.L.; Chang, S.-L.; Hu, Y.-F.; Chao, T.-F.; Chung, F.-P.; Chiou, C.-W.; Tsao, H.-M.; Chen, S.-A. Intrinsic Cardiac Autonomic Ganglionated Plexi within Epicardial Fats Modulate the Atrial Substrate Remodeling: Experiences with Atrial Fibrillation Patients Receiving Catheter Ablation. Acta Cardiol. Sin. 2016, 32, 174–184. [Google Scholar] [CrossRef]
- Mateos, J.C.P.; Mateos, E.I.P.; Lobo, T.J.; Pachón, M.Z.C.; Mateos, J.C.P.; Pachón, D.Q.V.; Vargas, R.N.A.; Piegas, L.S.; Jatene, A.D. Radiofrequency catheter ablation of atrial fibrillation guided by spectral mapping of atrial fibrillation nests in sinus rhythm. Arq. Bras. Cardiol. 2007, 89, 140–150. [Google Scholar]
- Chang, H.-Y.; Lo, L.-W.; Lin, Y.-J.; Lee, S.-H.; Chiou, C.-W.; Chen, S.-A. Relationship Between Intrinsic Cardiac Autonomic Ganglionated Plexi and the Atrial Fibrillation Nest. Circ. J. 2014, 78, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Mateos, J.C.P.; Mateos, E.I.P.; Higuti, C.; Peña, T.G.S.; Lobo, T.J.; Pachón, C.T.C.; Mateos, J.C.P.; Acosta, J.C.Z.; Ortencio, F.; Amarante, R. Cardioneuroablation: Catheter Vagal Denervation as a New Therapy for Cardioinhibitory Syncope. J. Card. Arrhythm. 2020, 32, 182–196. [Google Scholar] [CrossRef]
- Debruyne, P.; Wijns, W. Cardio-Neuromodulation: The Right-Sided Approach. JACC Clin. Electrophysiol. 2017, 3, 1056–1057. [Google Scholar] [CrossRef]
- Debruyne, P. Letter by Debruyne regarding article “Selective ablation of atrial ganglionated plexus attenuates vasovagal reflex in a canine model”. Pacing Clin. Electrophysiol. 2019, 42, 390. [Google Scholar] [CrossRef]
- Hou, Y.; Scherlag, B.J.; Lin, J.; Zhou, J.; Song, J.; Zhang, Y.; Patterson, E.; Lazzara, R.; Jackman, W.M.; Po, S.S. Interactive atrial neural network: Determining the connections between ganglionated plexi. Heart Rhythm 2007, 4, 56–63. [Google Scholar] [CrossRef]
- Li, L.; Po, S.; Yao, Y. Cardioneuroablation for Treating Vasovagal Syncope: Current Status and Future Directions. Arrhythmia Electrophysiol. Rev. 2023, 12, e18. [Google Scholar] [CrossRef]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T., Jr.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.Y.; Neuzil, P.; Koruth, J.S.; Petru, J.; Funosako, M.; Cochet, H.; Sediva, L.; Chovanec, M.; Dukkipati, S.R.; Jais, P. Pulsed Field Ablation for Pulmonary Vein Isolation in Atrial Fibrillation. J. Am. Coll. Cardiol. 2019, 74, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Di Monaco, A.; Vitulano, N.; Troisi, F.; Quadrini, F.; Romanazzi, I.; Calvi, V.; Grimaldi, M. Pulsed Field Ablation to Treat Atrial Fibrillation: A Review of the Literature. J. Cardiovasc. Dev. Dis. 2022, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Ueda, M.; Watanabe, M.; Ishimura, M.; Kajiyama, T.; Hashiguchi, N.; Kanaeda, T.; Nakano, M.; Hiranuma, Y.; Ishizaka, T.; et al. Identification of Left Atrial Ganglionated Plexi by Dense Epicardial Mapping as Ablation Targets for the Treatment of Concomitant Atrial Fibrillation. Pacing Clin. Electrophysiol. 2013, 36, 1336–1341. [Google Scholar] [CrossRef]
- Goff, Z.D.; Laczay, B.; Yenokyan, G.; Sivasambu, B.; Sinha, S.K.; Marine, J.E.; Ashikaga, H.; Berger, R.D.; Akhtar, T.; Spragg, D.D.; et al. Heart rate increase after pulmonary vein isolation predicts freedom from atrial fibrillation at 1 year. J. Cardiovasc. Electrophysiol. 2019, 30, 2818–2822. [Google Scholar] [CrossRef] [PubMed]
- Vesela, J.; Osmancik, P.; Herman, D.; Prochazkova, R. Changes in heart rate variability in patients with atrial fibrillation after pulmonary vein isolation and ganglionated plexus ablation. Physiol. Res. 2019, 68, 49–57. [Google Scholar] [CrossRef]
- Baysal, E.; Mutluer, F.O.; Dagsali, A.E.; Kumrulu, U.C.; Huang, H.D.; Aksu, T. Improved health-related quality of life after cardioneuroablation in patients with vasovagal syncope. J. Interv. Card. Electrophysiol. 2022, 1–8. [Google Scholar] [CrossRef]
- Calò, L.; Rebecchi, M.; Sciarra, L.; De Luca, L.; Fagagnini, A.; Zuccaro, L.M.; Pitrone, P.; Dottori, S.; Porfirio, M.; de Ruvo, E.; et al. Catheter Ablation of Right Atrial Ganglionated Plexi in Patients with Vagal Paroxysmal Atrial Fibrillation. Circ. Arrhythmia Electrophysiol. 2012, 5, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Scanavacca, M.; Rivarola, E.W.; Torres, R.V.A.; Hardy, C.; Wu, T.C.; Darrieux, F.; Pisani, C.; Hachul, D. Sinus Node Artery Occlusion during Cardiac Denervation Procedures. JACC Case Rep. 2022, 4, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A 3-dimentional representation of the four anatomical GP locations. White (anterior) and grey (posterior) circles indicate GP areas within the heart. (1) The right anterior GP (RAGP) is located on the posterior superior surface of the RA, adjacent to the junction of the superior vena cava (SVC) and RA, close to the right superior pulmonary vein (RSPV). (2) The left superior GP (LSGP) is found on the posterior surface of the LA between the left pulmonary veins (PVs). (3) The right inferior GP (RIGP) is situated on the posterior surface of the RA, adjacent to the interatrial groove. (4) The left inferior GP (LIGP) is located on the posterior medial surface of the LA, close to the left inferior pulmonary vein (LIPV). The left lateral GP (LLGP, not shown) is situated in the area around the ligament of Marshall and can be viewed with a left lateral view.
Figure 1.
A 3-dimentional representation of the four anatomical GP locations. White (anterior) and grey (posterior) circles indicate GP areas within the heart. (1) The right anterior GP (RAGP) is located on the posterior superior surface of the RA, adjacent to the junction of the superior vena cava (SVC) and RA, close to the right superior pulmonary vein (RSPV). (2) The left superior GP (LSGP) is found on the posterior surface of the LA between the left pulmonary veins (PVs). (3) The right inferior GP (RIGP) is situated on the posterior surface of the RA, adjacent to the interatrial groove. (4) The left inferior GP (LIGP) is located on the posterior medial surface of the LA, close to the left inferior pulmonary vein (LIPV). The left lateral GP (LLGP, not shown) is situated in the area around the ligament of Marshall and can be viewed with a left lateral view.
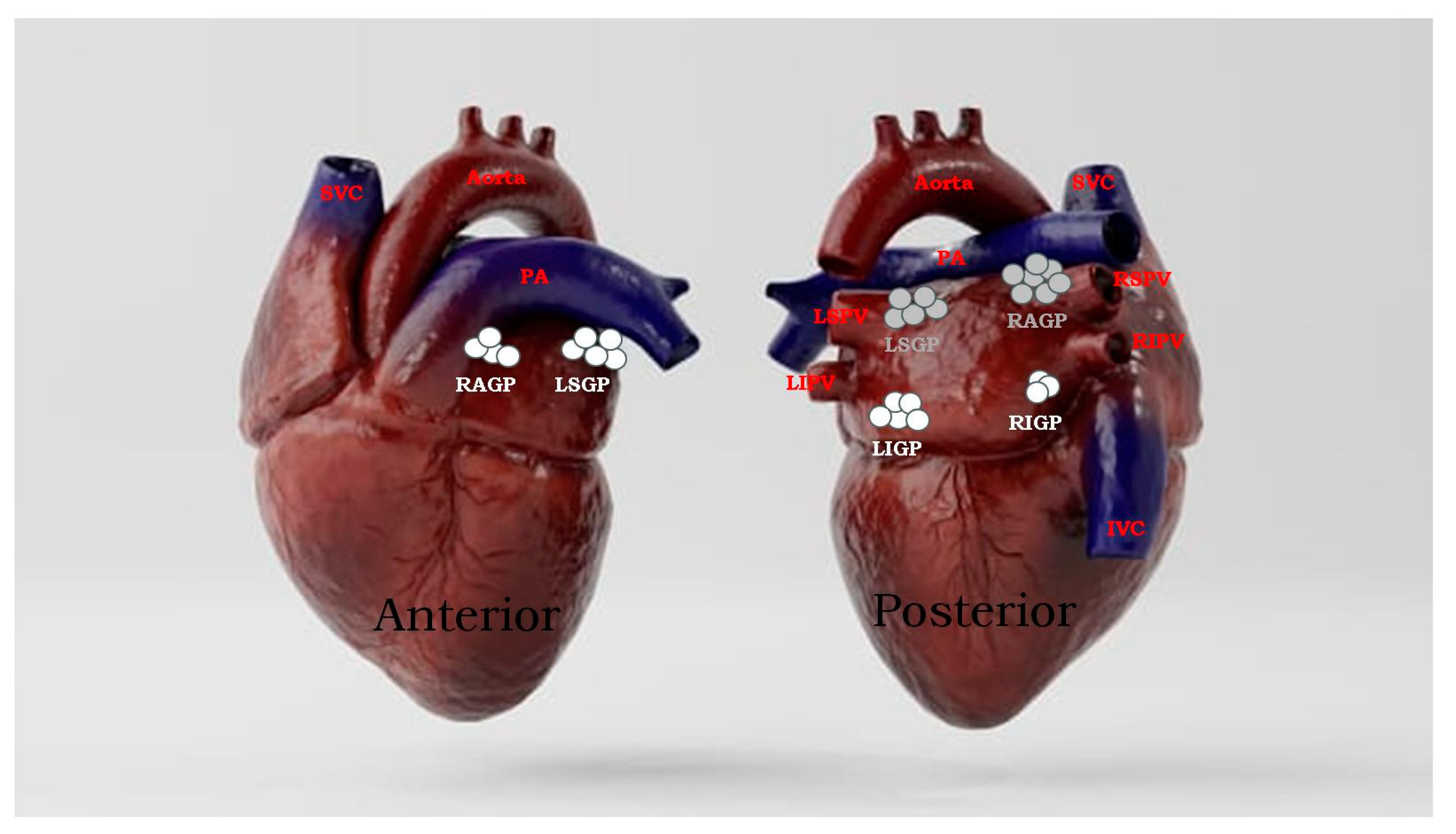
Figure 2.
Innervation of the heart includes the afferent (sensory) neurons (green), which transmit information from baroreceptors in the heart to the spinal cord and brain (CNS), and efferent (motor) neurons, which innervate the heart. These efferent motor neurons comprise the cardiac autonomic nervous system, and includes the sympathetic (purple) and parasympathetic (yellow) neurons. Depending on the location of neuronal cell bodies of each neuron type, cardiac innervation is divided into intrinsic and extrinsic elements. Intracardiac vagal innervation (pink) originates in the brain and relays information into the heart, whereas vagal neurons (yellow) synapse with secondary interneurons (pink) to activate the parasympathetic tone. The cell bodies of interconnecting neurons and neural elements of other cell types all cluster into what are known as the ganglionated plexi (small dark dots) in specific cardiac locations with diverse densities. Ao, aorta; IVC, inferior vena cava; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; SVC, superior vena cava.
Figure 2.
Innervation of the heart includes the afferent (sensory) neurons (green), which transmit information from baroreceptors in the heart to the spinal cord and brain (CNS), and efferent (motor) neurons, which innervate the heart. These efferent motor neurons comprise the cardiac autonomic nervous system, and includes the sympathetic (purple) and parasympathetic (yellow) neurons. Depending on the location of neuronal cell bodies of each neuron type, cardiac innervation is divided into intrinsic and extrinsic elements. Intracardiac vagal innervation (pink) originates in the brain and relays information into the heart, whereas vagal neurons (yellow) synapse with secondary interneurons (pink) to activate the parasympathetic tone. The cell bodies of interconnecting neurons and neural elements of other cell types all cluster into what are known as the ganglionated plexi (small dark dots) in specific cardiac locations with diverse densities. Ao, aorta; IVC, inferior vena cava; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; SVC, superior vena cava.


{kind=link}
{kind=link}
Table 1.
Previous cohort studies of catheter ablation for neurally mediated syncope.
| Technique | N | Age (y) | Diagnosis | Approach | Procedure Time (min) | Follow-Up Duration (months) | Syncope Recurrence | Heart Rate Variability (p-Value) | Year, Reference |
|---|---|---|---|---|---|---|---|---|---|
| SA + AA * | 6 | 47.5 ± 16 | NMS | LA, RA, SVC | 38.9 ± 15.4 | 9.2 | 0 | 2005 [37] | |
| SA + AA * | 7 | 47.5 ± 16 | Functional high degree AVB | LA, RA, SVC | 38.9 ± 15.4 | 9.2 | 0 | 2005 [37] | |
| SA (FFT) + AA * | 13 | 47.5 ± 16 | Sinus node dysfunction | LA, RA, SVC | 38.9 ± 15.4 | 9.2 | 0 | 0.003 | 2005 [37] |
| SA + AA | 43 | 32.9 ± 15 | NMS | SVC, RA, inferior–posterior interatrial septum | NR | 21.7 ± 11 | 3 (6.9%) | 0.001 | 2011 [52] |
| SA (FFT) + HFS * | 7 | 42.7 ± 14.7 | AVB | RA in 6 patients, followed by LA in 1 patient | 121.2 ± 16.4 (for all patients in this study) | 6 | 1 (14.3%) | NR | 2016 [53] |
| SA (FFT) + HFS * | 8 | 42.7 ± 14.7 | NMS | LA then RA | 121.2 ± 16.4 (for all patients in this study) | 12.3 ± 3.4 | 0 | 0.001 (SDNN 6 months post procedure) | 2016 [53] |
| SA (FFT) + HFS * | 7 | 42.7 ± 14.7 | SND | LA then RA | 121.2 ± 16.4 (for all patients in this study) | 9.5 ± 3.1 | 0 | 0.001 (SDNN 6 months post procedure) | 2016 [53] |
| Fractionation * Mapping | 12 | NR | VVS | NR | NR | 12 | 0 | SD | 2019 [54] |
| SA + HFS * | 8 | NR | VVS | NR | NR | 12 | 2 | SD | 2019 [54] |
| SA + AA | 83 | 47.3 ± 17 | AF VVS | RA, LA | 237.2 ± 38 | 40 | 0 | 0.001 | 2020 [55] |
| PVI | 67 | 53.2 ± 11.3; 55.2 ± 11.6 | Paroximal AF | LA | 105.2 ± 22.3; 126.0 ± 26.7 | 12 | 18 (54.5%) | NR | 2011 [48] |
| HFS + PVI | 83 | NR | AF | NR | NR | 22 | NR | NR | 2009 [19] |
| HFS (selective vagal denervation) | 10 | 50.4 ± 6.4 | Recurrent NMS | LA | 50.2 ± 3.8 | 30 ± 16 | 0 | 0.002 | 2012 [23] |
| Synchronized HFS * | 20 | 50–69 | Paroximal AF, AVB | LA | NR | NR | NR | NR | 2013 [22] |
| Continuous HFS * | 10 | 54–68 | Persistent AF, AVB | LA | NR | NR | NR | NR | 2013 [22] |
| HFS | 11 | 45.9 ± 10.9 | Symptomatic SB | LA, RA, SVC | NR | 18 ± 6 | Significant symptom improvement | 0.001 | 2015 [24] |
| HFS * | 10 | 50.4 ± 6.4 | VVS | LA | 50.2 ± 3.8 | 36.4 ± 22.2 | 0 | 0.751 | 2016 [21] |
| AA * | 47 | 41.7 ± 14.1 | VVS | LA | 43.7 ± 6.1 | 36.4 ± 22.2 | 5 | 0.751 | 2016 [21] |
| HFS * | 43 | NR | VVS | NR | NR | NR | NR | SD | 2022 [56] |
| HFS * | 40 | NR | AF | NR | NR | NR | NR | SD | 2022 [56] |
| AA * | 42 | 51.2 ± 15.3 | VVS | LA | NR | 8 | 16% | SD | 2022 [57] |
| HFS * | 66 | 51.2 ± 15.3 | VVS | LA | NR | 8 | 16% | SD | 2022 [57] |
| HFS | 28 | NR | VVS | LA | NR | NR | NR | SD | 2021 [58] |
| HFS + AA | 115 | NR | VVS | LA | NR | 21.4 ± 13.1 | NR | SD | 2019 [59] |
| AA | 14 | 34.0 ± 13.8 | VVS, advanced AVB, sinus arrest | LA, RV, LA | 112 ± 15 | 22.5 ± 11.3 | 0 VVS; 0 sinus arrest; 4 AV block | 0.002 (SDNN 30) days post-procedure); 0.002 (pNN > 50, 30 days post-procedure) | 2017 [50] |
| AA | 18 | 36.9 ± 11.2 | VVS | RA | NR | 34.1 ± 6.1 | 3 (16.6%) | 0.001 | 2021 [60] |
| ‡ AA | 62 | 47.8 ± 12.6 | Symptomatic SB | LA, RA, SVC | NR | 12 | Significant symptom improvement in | SD | 2017 [61] |
| AA | 26 | 41.8 ± 15.4 | VVS + PVCs | LA | NR | 10.6 ± 6.8 | 1 (3.8%) | 2021 [51] | |
| † NR | 51 | NR | VVS | NR | NR | 22 | 2 (3.9%) | NR | 2022 [62] |
| NR | 123 | 42.2 ± 17.1 | VVS | LA | NR | 48 ± 13.2 | 33 (26.8%) | NR | 2022 [63] |
| ‡ CardNM (computed tomographic scan + electro-anatomical mapping) | 20 | 41.4 ± 18.8 | NMS | RA, SVC, coronary sinus | 7 ± 4 | 6 | 4 (20%) | 0.001 | 2018 [64] |
| ‡ CardNM (computed tomographic scan + electro-anatomical mapping) | 50 | 42.4 ± 17 | NMS | RA, SVC, coronary sinus | 8 ± 4 | 12 | 13 (26%) | 0.001 | 2021 [65] |
SA, spectral analysis; AA, anatomic approach; NMS, neurally mediated syncope; LA, left atrium’ RA, right atrium; SVC, superior vena cava; AVB atrioventricular block; FFT, fast Fourier transform analysis; NR, not reported; HFS, high-frequency stimulation; SDNN, standard deviation of all normal R-R intervals in the 24 h ECG recording; SND, sinus node dysfunction; pNN > 50, percentage of sinus cycles differing from the preceding cycle by >50 ms during the 24 h ECG recording; AF, atrial fibrillation; VVS, vasovagal syncope; PVI, pulmonary vein isolation; SB, sinus bradycardia; SD, significantly decreased; PVCs, premature ventricular contractions; CardNM, cardio-neuromodulation. * These data were taken from the same study. †: Case-control study; ‡: prospective study.
Table 2.
Previous case studies of catheter ablation for neurally mediated syncope.
| Technique | Age (y), (Sex) | Diagnosis | Approach | Procedure Time (min) | Follow-Up Duration (Months) | Syncope Recurrence | Heart Rate Variability (p-Value) | Year, Reference |
|---|---|---|---|---|---|---|---|---|
| HFS | 20 (F) | VVS | RA, LA | NR | 7 | 1 | SD | 2022 [66] |
| HFS | 52 (F) | VVS | RA, LA | 18.8 | 18 | 0 | NR | 2020 [20] |
| HFS (selective vagal denervation) | 57 (F) | VVS | RA, LA | NR | 12 | 0 | SD | 2012 [40] |
| HFS | 15 (F) | NMS | RA, RV, LA | NR | 13 | 3 | SD | 2009 [41] |
| Electro-anatomical mapping CARTO3 | 38 (M) | AVB | RA, LV, coronary sinus, His bundle, LA | NR | 11 | NR | NR | 2021 [67] |
| Electro-anatomical mapping CARTO3 | 35 (F) | NMS and AVB | SA and AV nodes (RA, SVC, R, L, interatrial septum, LA) | NR | 10 | 2 | NR | 2016 [42] |
| Electro-anatomical mapping CARTO3 + spectral mapping | 17 (M) | NMS | SVC | NR | 12 | 0 | NR | 2015 [68] |
| Electro-anatomical mapping CARTO3 * | 31 (F) | VVS | RA, SVC, IVC, sinus AV nodes | NR | 8 | 0 | NS | 2012 [69] |
| Electro-anatomical mapping CARTO3 * | 45 (F) | VVS | RA, SVC, IVC, sinus AV nodes | NR | 8 | 0 | NS | 2012 [69] |
| Spectral mapping (fibrillar myocardium) | 23 (F) | AVB | RA, His bundle region, AV and sinus nodes | NR | 21 | NR | SD | 2006 [70] |
| Spectral mapping + HFS | 55 (F) | AVB | RA, SVC | 75 | 12 | 0 | NR | 2015 [71] |
| Spectral mapping (fibrillar myocardium) | 38 (M) | Vagal mediated AVB | Sinus nodes, AV nodes (R, L inter-atrial septum innervation) | 87 | 15 | NA | SD | 2016 [39] |
| ‡ CardNM (computed tomographic scan + electro-anatomical mapping) | 16 (F) | VVS | LA | 3 | 22 | 0 | SD | 2016 [72] |
| Fractionation mapping software (Ensite Precision, Abbott https://www.cardiovascular.abbott/us/en/hcp/products/electrophysiology/mapping-systems/ensite.html, accessed on 6 August 2023) | 18 (M) | VVS | LA, RA | NR | NR | NR | NR | 2021 [73] |
| Fractionation mapping software (Ensite Precision, Abbott) | 20 (F) | VVS | RA | 11.4 | 1 | 0 | SD | 2021 [74] |
| Fractionation mapping software (Ensite Precision, Abbott) | 46 (F) | VVS | RA | NR | NR | NR | NR | 2021 [75] |
HFS, high-frequency stimulation; VVS, vasovagal syncope; RA, right atrium; NR, not reported; LA, left atrium; SD, significantly decreased; AVB atrioventricular block; LV, left ventricle; LA, left atrium; NMS, neurally mediated syncope; SA, sinoatrial; AV, atrioventricular; SVC, superior vena cava, IVC, inferior vena cava. * These data were taken from the same study. ‡: Prospective study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yarkoni, M.; Rehman, W.u.; Bajwa, A.; Yarkoni, A.; Rehman, A.u. Ganglionated Plexus Ablation Procedures to Treat Vasovagal Syncope. Int. J. Mol. Sci. 2023, 24, 13264. https://doi.org/10.3390/ijms241713264
AMA Style
Yarkoni M, Rehman Wu, Bajwa A, Yarkoni A, Rehman Au. Ganglionated Plexus Ablation Procedures to Treat Vasovagal Syncope. International Journal of Molecular Sciences. 2023; 24(17):13264. https://doi.org/10.3390/ijms241713264
Chicago/Turabian StyleYarkoni, Merav, Wajeeh ur Rehman, Ata Bajwa, Alon Yarkoni, and Afzal ur Rehman. 2023. "Ganglionated Plexus Ablation Procedures to Treat Vasovagal Syncope" International Journal of Molecular Sciences 24, no. 17: 13264. https://doi.org/10.3390/ijms241713264
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.