
Extracellular Vesicles in Liver Transplantation: Current Evidence and Future Challenges
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. EVs as Diagnostics Tools
2.1.1. Liver Cirrhosis
2.1.2. Acute Liver Failure
2.1.3. Alcoholic Hepatitis
2.1.4. Liver Cancer
2.2. EVs and Rejection
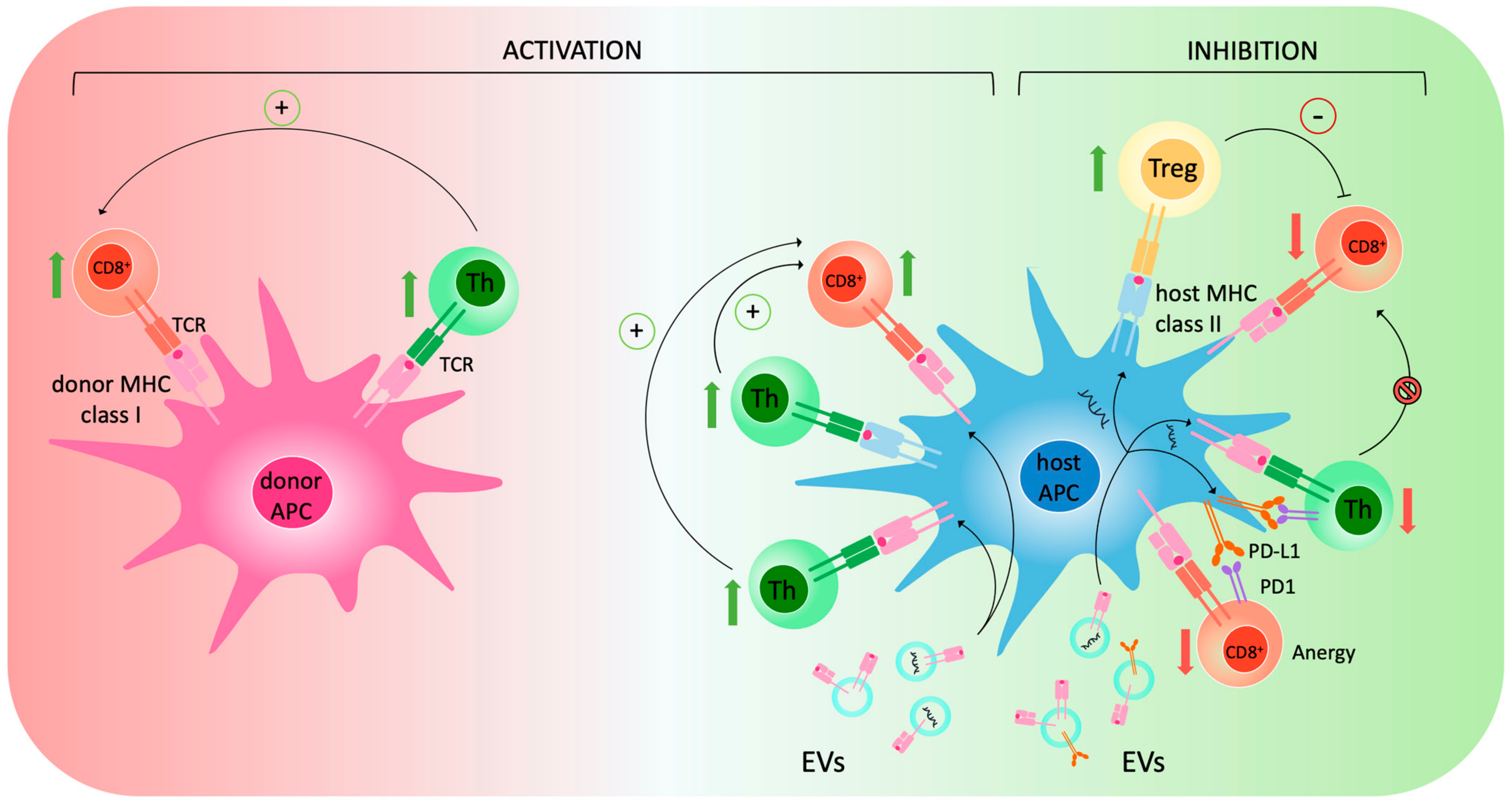
2.2.1. EVs and the Immune System
2.2.2. Applications of EVs in Rejection
2.3. Therapeutic Applications of EVs
2.3.1. Mechanisms of Protection against Liver IRI
2.3.2. EV-Based Therapies during MP
3. Discussion
Challenges to Clinical Translation
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jadlowiec, C.C.; Taner, T. Liver Transplantation: Current Status and Challenges. World J. Gastroenterol. 2016, 22, 4438–4445. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.X.S.; Weber, A.; Dutkowski, P.; Clavien, P. Machine Perfusion in Liver Transplantation. Hepatology 2022, 76, 1531–1549. [Google Scholar] [CrossRef] [PubMed]
- Ghinolfi, D.; Lai, Q.; Dondossola, D.; De Carlis, R.; Zanierato, M.; Patrono, D.; Baroni, S.; Bassi, D.; Ferla, F.; Lauterio, A.; et al. Machine Perfusions in Liver Transplantation: The Evidence-Based Position Paper of the Italian Society of Organ and Tissue Transplantation. Liver Transplant. 2020, 26, 1298–1315. [Google Scholar] [CrossRef] [PubMed]
- Patrono, D.; De Stefano, N.; Rigo, F.; Cussa, D.; Romagnoli, R. Some like it hot. Utility and mechanisms of ex-situ normothermic machine perfusion of the liver. Eur. J. Transplant. 2023, 1, 92–112. [Google Scholar] [CrossRef]
- Patrono, D.; Cussa, D.; Rigo, F.; Romagnoli, R. Liver Machine Perfusion Survey Group Heterogeneous Indications and the Need for Viability Assessment: An International Survey on the Use of Machine Perfusion in Liver Transplantation. Artif. Organs 2022, 46, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Nikokiraki, C.; Psaraki, A.; Roubelakis, M.G. The Potential Clinical Use of Stem/Progenitor Cells and Organoids in Liver Diseases. Cells 2022, 11, 1410. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Mergental, H.; Fondevila, C.; Porte, R.J.; Friend, P.J.; Dutkowski, P. Machine Perfusion of the Liver and Bioengineering. J. Hepatol. 2023, 78, 1181–1198. [Google Scholar] [CrossRef] [PubMed]
- De Stefano, N.; Calleri, A.; Navarro-Tableros, V.; Rigo, F.; Patrono, D.; Romagnoli, R. State-of-the-Art and Future Directions in Organ Regeneration with Mesenchymal Stem Cells and Derived Products during Dynamic Liver Preservation. Med. Kaunas Lith. 2022, 58, 1826. [Google Scholar] [CrossRef]
- Barile, L.; Vassalli, G. Exosomes: Therapy Delivery Tools and Biomarkers of Diseases. Pharmacol. Ther. 2017, 174, 63–78. [Google Scholar] [CrossRef]
- Malhi, H. Emerging Role of Extracellular Vesicles in Liver Diseases. Am. J. Physiol. Gastrointest. Liver Physiol. 2019, 317, G739–G749. [Google Scholar] [CrossRef]
- Ding, Y.; Luo, Q.; Que, H.; Wang, N.; Gong, P.; Gu, J. Mesenchymal Stem Cell-Derived Exosomes: A Promising Therapeutic Agent for the Treatment of Liver Diseases. Int. J. Mol. Sci. 2022, 23, 10972. [Google Scholar] [CrossRef] [PubMed]
- Kostallari, E.; Valainathan, S.; Biquard, L.; Shah, V.H.; Rautou, P.-E. Role of Extracellular Vesicles in Liver Diseases and Their Therapeutic Potential. Adv. Drug Deliv. Rev. 2021, 175, 113816. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Patel, T.; Freedman, J.E. Circulating Extracellular Vesicles in Human Disease. N. Engl. J. Med. 2018, 379, 958–966. [Google Scholar] [CrossRef] [PubMed]
- Benichou, G.; Wang, M.; Ahrens, K.; Madsen, J.C. Extracellular Vesicles in Allograft Rejection and Tolerance. Cell. Immunol. 2020, 349, 104063. [Google Scholar] [CrossRef] [PubMed]
- Mastoridis, S.; Martinez-Llordella, M.; Sanchez-Fueyo, A. Extracellular Vesicles as Mediators of Alloimmunity and Their Therapeutic Potential in Liver Transplantation. World J. Transplant. 2020, 10, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, J.; Wehrkamp, C.; Ota, Y.; Thomas, J.N.; Yan, I.K.; Patel, T. Biological Nanotherapeutics for Liver Disease. Hepatology 2021, 74, 2863–2875. [Google Scholar] [CrossRef] [PubMed]
- Psaraki, A.; Ntari, L.; Karakostas, C.; Korrou-Karava, D.; Roubelakis, M.G. Extracellular Vesicles Derived from Mesenchymal Stem/Stromal Cells: The Regenerative Impact in Liver Diseases. Hepatology 2022, 75, 1590–1603. [Google Scholar] [CrossRef]
- Grange, C.; Bellucci, L.; Bussolati, B.; Ranghino, A. Potential Applications of Extracellular Vesicles in Solid Organ Transplantation. Cells 2020, 9, 369. [Google Scholar] [CrossRef]
- Huang, D.Q.; Terrault, N.A.; Tacke, F.; Gluud, L.L.; Arrese, M.; Bugianesi, E.; Loomba, R. Global Epidemiology of Cirrhosis—Aetiology, Trends and Predictions. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 388–398. [Google Scholar] [CrossRef]
- Payancé, A.; Silva-Junior, G.; Bissonnette, J.; Tanguy, M.; Pasquet, B.; Levi, C.; Roux, O.; Nekachtali, O.; Baiges, A.; Hernández-Gea, V.; et al. Hepatocyte Microvesicle Levels Improve Prediction of Mortality in Patients with Cirrhosis. Hepatology 2018, 68, 1508–1518. [Google Scholar] [CrossRef]
- Engelmann, C.; Splith, K.; Krohn, S.; Herber, A.; Boehlig, A.; Boehm, S.; Pratschke, J.; Berg, T.; Schmelzle, M. Absolute Quantification of Microparticles by Flow Cytometry in Ascites of Patients with Decompensated Cirrhosis: A Cohort Study. J. Transl. Med. 2017, 15, 188. [Google Scholar] [CrossRef] [PubMed]
- Stravitz, R.T.; Lee, W.M. Acute Liver Failure. Lancet 2019, 394, 869–881. [Google Scholar] [CrossRef] [PubMed]
- O’Grady, J.G.; Alexander, G.J.M.; Hayllar, K.M.; Williams, R. Early Indicators of Prognosis in Fulminant Hepatic Failure. Gastroenterology 1989, 97, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Bismuth, H.; Samuel, D.; Castaing, D.; Adam, R.; Saliba, F.; Johann, M.; Azoulay, D.; Ducot, B.; Chiche, L. Orthotopic Liver Transplantation in Fulminant and Subfulminant Hepatitis The Paul Brousse Experience. Ann. Surg. 1995, 222, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Stravitz, R.T.; Bowling, R.; Bradford, R.L.; Key, N.S.; Glover, S.; Thacker, L.R.; Gabriel, D.A. Role of Procoagulant Microparticles in Mediating Complications and Outcome of Acute Liver Injury/Acute Liver Failure. Hepatology 2013, 58, 304–313. [Google Scholar] [CrossRef]
- Germani, G.; Mathurin, P.; Lucey, M.R.; Trotter, J. Early Liver Transplantation for Severe Acute Alcohol-Related Hepatitis after More than a Decade of Experience. J. Hepatol. 2023, 78, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Sukriti, S.; Maras, J.S.; Bihari, C.; Das, S.; Vyas, A.K.; Sharma, S.; Hussain, S.; Shasthry, S.; Choudhary, A.; Premkumar, M.; et al. Microvesicles in Hepatic and Peripheral Vein Can Predict Nonresponse to Corticosteroid Therapy in Severe Alcoholic Hepatitis. Aliment. Pharmacol. Ther. 2018, 47, 1151–1161. [Google Scholar] [CrossRef]
- Vogel, A.; Meyer, T.; Sapisochin, G.; Salem, R.; Saborowski, A. Hepatocellular Carcinoma. Lancet 2022, 400, 1345–1362. [Google Scholar] [CrossRef]
- De’Angelis, N. Managements of Recurrent Hepatocellular Carcinoma after Liver Transplantation: A Systematic Review. World J. Gastroenterol. 2015, 21, 11185. [Google Scholar] [CrossRef]
- Chaiteerakij, R.; Zhang, X.; Addissie, B.D.; Mohamed, E.A.; Harmsen, W.S.; Theobald, P.J.; Peters, B.E.; Balsanek, J.G.; Ward, M.M.; Giama, N.H.; et al. Combinations of Biomarkers and Milan Criteria for Predicting Hepatocellular Carcinoma Recurrence after Liver Transplantation. Liver Transplant. 2015, 21, 599–606. [Google Scholar] [CrossRef]
- Malik, J.; Klammer, M.; Rolny, V.; Chan, H.L.-Y.; Piratvisuth, T.; Tanwandee, T.; Thongsawat, S.; Sukeepaisarnjaroen, W.; Esteban, J.I.; Bes, M.; et al. Comprehensive Evaluation of MicroRNA as a Biomarker for the Diagnosis of Hepatocellular Carcinoma. World J. Gastroenterol. 2022, 28, 3917–3933. [Google Scholar] [CrossRef] [PubMed]
- Sohn, W.; Kim, J.; Kang, S.H.; Yang, S.R.; Cho, J.-Y.; Cho, H.C.; Shim, S.G.; Paik, Y.-H. Serum Exosomal MicroRNAs as Novel Biomarkers for Hepatocellular Carcinoma. Exp. Mol. Med. 2015, 47, e184. [Google Scholar] [CrossRef]
- Cho, H.; Eun, J.; Baek, G.; Seo, C.; Ahn, H.; Kim, S.; Cho, S.; Cheong, J. Serum Exosomal MicroRNA, MiR-10b-5p, as a Potential Diagnostic Biomarker for Early-Stage Hepatocellular Carcinoma. J. Clin. Med. 2020, 9, 281. [Google Scholar] [CrossRef]
- Wang, S.; Yang, Y.; Sun, L.; Qiao, G.; Song, Y.; Liu, B. Exosomal MicroRNAs as Liquid Biopsy Biomarkers in Hepatocellular Carcinoma. OncoTargets Ther. 2020, 13, 2021–2030. [Google Scholar] [CrossRef]
- Sorop, A.; Iacob, R.; Iacob, S.; Constantinescu, D.; Chitoiu, L.; Fertig, T.E.; Dinischiotu, A.; Chivu-Economescu, M.; Bacalbasa, N.; Savu, L.; et al. Plasma Small Extracellular Vesicles Derived MiR-21-5p and MiR-92a-3p as Potential Biomarkers for Hepatocellular Carcinoma Screening. Front. Genet. 2020, 11, 712. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Lee, Y.-T.; Zhang, R.Y.; Kao, R.; Teng, P.-C.; Yang, Y.; Yang, P.; Wang, J.J.; Smalley, M.; Chen, P.-J.; et al. Purification of HCC-Specific Extracellular Vesicles on Nanosubstrates for Early HCC Detection by Digital Scoring. Nat. Commun. 2020, 11, 4489. [Google Scholar] [CrossRef] [PubMed]
- Gondaliya, P.; Sayyed, A.A.; Driscoll, J.; Patel, K.; Patel, T. Extracellular Vesicle RNA Signaling in the Liver Tumor Microenvironment. Cancer Lett. 2023, 558, 216089. [Google Scholar] [CrossRef]
- Wang, W.; Li, H.; Zhou, Y.; Jie, S. Peripheral Blood Microvesicles Are Potential Biomarkers for Hepatocellular Carcinoma. Cancer Biomark. 2013, 13, 351–357. [Google Scholar] [CrossRef]
- Xue, X.; Zhao, Y.; Wang, X.; Qin, L.; Hu, R. Development and Validation of Serum Exosomal MicroRNAs as Diagnostic and Prognostic Biomarkers for Hepatocellular Carcinoma. J. Cell. Biochem. 2019, 120, 135–142. [Google Scholar] [CrossRef]
- Fang, T.; Lv, H.; Lv, G.; Li, T.; Wang, C.; Han, Q.; Yu, L.; Su, B.; Guo, L.; Huang, S.; et al. Tumor-Derived Exosomal MiR-1247-3p Induces Cancer-Associated Fibroblast Activation to Foster Lung Metastasis of Liver Cancer. Nat. Commun. 2018, 9, 191. [Google Scholar] [CrossRef]
- Lee, Y.R.; Kim, G.; Tak, W.Y.; Jang, S.Y.; Kweon, Y.O.; Park, J.G.; Lee, H.W.; Han, Y.S.; Chun, J.M.; Park, S.Y.; et al. Circulating Exosomal Noncoding RNAs as Prognostic Biomarkers in Human Hepatocellular Carcinoma: Circulating Exosomal Noncoding RNAs in HCC. Int. J. Cancer 2019, 144, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Parikh, N.D.; Tayob, N.; Singal, A.G. Blood-Based Biomarkers for Hepatocellular Carcinoma Screening: Approaching the End of the Ultrasound Era? J. Hepatol. 2023, 78, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Sugimachi, K.; Matsumura, T.; Hirata, H.; Uchi, R.; Ueda, M.; Ueo, H.; Shinden, Y.; Iguchi, T.; Eguchi, H.; Shirabe, K.; et al. Identification of a Bona Fide MicroRNA Biomarker in Serum Exosomes That Predicts Hepatocellular Carcinoma Recurrence after Liver Transplantation. Br. J. Cancer 2015, 112, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Chen, I.-H.; Wang, C.-C.; Chen, P.-J.; Tseng, H.-P.; Huang, K.-T.; Hu, T.-H.; Li, L.-C.; Goto, S.; Cheng, Y.-F.; et al. Circulating Exosomal MiR-92b: Its Role for Cancer Immunoediting and Clinical Value for Prediction of Posttransplant Hepatocellular Carcinoma Recurrence. Am. J. Transplant. 2019, 19, 3250–3262. [Google Scholar] [CrossRef]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next Horizon in Mechanisms and Management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- McMillan, R.R.; Saharia, A.; Abdelrahim, M.; Ghobrial, R.M. New Breakthroughs for Liver Transplantation of Cholangiocarcinoma. Curr. Transplant. Rep. 2021, 8, 21–27. [Google Scholar] [CrossRef]
- Alvaro, D.; Gores, G.J.; Walicki, J.; Hassan, C.; Sapisochin, G.; Komuta, M.; Forner, A.; Valle, J.W.; Laghi, A.; Ilyas, S.I.; et al. EASL-ILCA Clinical Practice Guidelines on the Management of Intrahepatic Cholangiocarcinoma. J. Hepatol. 2023, 79, 181–208. [Google Scholar] [CrossRef]
- Lapitz, A.; Azkargorta, M.; Milkiewicz, P.; Olaizola, P.; Zhuravleva, E.; Grimsrud, M.M.; Schramm, C.; Arbelaiz, A.; O’Rourke, C.J.; La Casta, A.; et al. Liquid Biopsy-Based Protein Biomarkers for Risk Prediction, Early Diagnosis, and Prognostication of Cholangiocarcinoma. J. Hepatol. 2023, 79, 93–108. [Google Scholar] [CrossRef]
- Li, L.; Masica, D.; Ishida, M.; Tomuleasa, C.; Umegaki, S.; Kalloo, A.N.; Georgiades, C.; Singh, V.K.; Khashab, M.; Amateau, S.; et al. Human Bile Contains MicroRNA-Laden Extracellular Vesicles That Can Be Used for Cholangiocarcinoma Diagnosis. Hepatology 2014, 60, 896–907. [Google Scholar] [CrossRef]
- Julich-Haertel, H.; Urban, S.K.; Krawczyk, M.; Willms, A.; Jankowski, K.; Patkowski, W.; Kruk, B.; Krasnodębski, M.; Ligocka, J.; Schwab, R.; et al. Cancer-Associated Circulating Large Extracellular Vesicles in Cholangiocarcinoma and Hepatocellular Carcinoma. J. Hepatol. 2017, 67, 282–292. [Google Scholar] [CrossRef]
- Maspero, M.; Sposito, C.; Virdis, M.; Citterio, D.; Pietrantonio, F.; Bhoori, S.; Belli, F.; Mazzaferro, V. Liver Transplantation for Hepatic Metastases from Colorectal Cancer: Current Knowledge and Open Issues. Cancers 2023, 15, 345. [Google Scholar] [CrossRef]
- Osumi, H.; Shinozaki, E.; Yamaguchi, K.; Zembutsu, H. Early Change in Circulating Tumor DNA as a Potential Predictor of Response to Chemotherapy in Patients with Metastatic Colorectal Cancer. Sci. Rep. 2019, 9, 17358. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J.; Rodríguez-Perálvarez, M.L.; Pageaux, G.-P.; Sanchez-Fueyo, A.; Feng, S. Liver Transplantation Immunology: Immunosuppression, Rejection, and Immunomodulation. J. Hepatol. 2023, 78, 1199–1215. [Google Scholar] [CrossRef] [PubMed]
- Benichou, G.; Valujskikh, A.; Heeger, P.S. Contributions of Direct and Indirect T Cell Alloreactivity during Allograft Rejection in Mice. J. Immunol. 1999, 162, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Marino, J.; Paster, J.; Benichou, G. Allorecognition by T Lymphocytes and Allograft Rejection. Front. Immunol. 2016, 7, 582. [Google Scholar] [CrossRef] [PubMed]
- Marino, J.; Babiker-Mohamed, M.H.; Crosby-Bertorini, P.; Paster, J.T.; LeGuern, C.; Germana, S.; Abdi, R.; Uehara, M.; Kim, J.I.; Markmann, J.F.; et al. Donor Exosomes Rather than Passenger Leukocytes Initiate Alloreactive T Cell Responses after Transplantation. Sci. Immunol. 2016, 1, aaf8759. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Rojas-Canales, D.M.; Divito, S.J.; Shufesky, W.J.; Stolz, D.B.; Erdos, G.; Sullivan, M.L.G.; Gibson, G.A.; Watkins, S.C.; Larregina, A.T.; et al. Donor Dendritic Cell-Derived Exosomes Promote Allograft-Targeting Immune Response. J. Clin. Investig. 2016, 126, 2805–2820. [Google Scholar] [CrossRef]
- Frelinger, J.A.; Neiderhuber, J.E.; David, C.S.; Shreffler, D.C. Evidence for the Expression of Ia (H-2-Associated) Antigens on Thymus-Derived Lymphocytes. J. Exp. Med. 1974, 140, 1273–1284. [Google Scholar] [CrossRef]
- Smyth, L.A.; Herrera, O.B.; Golshayan, D.; Lombardi, G.; Lechler, R.I. A Novel Pathway of Antigen Presentation by Dendritic and Endothelial Cells: Implications for Allorecognition and Infectious Diseases. Transplantation 2006, 82, S15–S18. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kelesidis, T.; Yang, O.O. Detection of Donor-Derived Microparticles in the Peripheral Blood of a Hand Transplant Recipient During Rejection. Transplant. Direct 2017, 3, e131. [Google Scholar] [CrossRef]
- Vallabhajosyula, P.; Korutla, L.; Habertheuer, A.; Yu, M.; Rostami, S.; Yuan, C.-X.; Reddy, S.; Liu, C.; Korutla, V.; Koeberlein, B.; et al. Tissue-Specific Exosome Biomarkers for Noninvasively Monitoring Immunologic Rejection of Transplanted Tissue. J. Clin. Investig. 2017, 127, 1375–1391. [Google Scholar] [CrossRef] [PubMed]
- Mastoridis, S.; Londoño, M.-C.; Kurt, A.; Kodela, E.; Crespo, E.; Mason, J.; Bestard, O.; Martínez-Llordella, M.; Sánchez-Fueyo, A. Impact of Donor Extracellular Vesicle Release on Recipient Cell “Cross-Dressing” Following Clinical Liver and Kidney Transplantation. Am. J. Transplant. 2021, 21, 2387–2398. [Google Scholar] [CrossRef] [PubMed]
- LeMaoult, J.; Caumartin, J.; Daouya, M.; Favier, B.; Le Rond, S.; Gonzalez, A.; Carosella, E.D. Immune Regulation by Pretenders: Cell-to-Cell Transfers of HLA-G Make Effector T Cells Act as Regulatory Cells. Blood 2007, 109, 2040–2048. [Google Scholar] [CrossRef] [PubMed]
- Tilburgs, T.; Evans, J.H.; Crespo, Â.C.; Strominger, J.L. The HLA-G Cycle Provides for Both NK Tolerance and Immunity at the Maternal-Fetal Interface. Proc. Natl. Acad. Sci. USA 2015, 112, 13312–13317. [Google Scholar] [CrossRef] [PubMed]
- Bracamonte-Baran, W.; Florentin, J.; Zhou, Y.; Jankowska-Gan, E.; Haynes, W.J.; Zhong, W.; Brennan, T.V.; Dutta, P.; Claas, F.H.J.; van Rood, J.J.; et al. Modification of Host Dendritic Cells by Microchimerism-Derived Extracellular Vesicles Generates Split Tolerance. Proc. Natl. Acad. Sci. USA 2017, 114, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.; Lundin, S.; Dahlgren, U.; Kahu, H.; Pettersson, I.; Telemo, E. “Tolerosomes” Are Produced by Intestinal Epithelial Cells. Eur. J. Immunol. 2001, 31, 2892–2900. [Google Scholar] [CrossRef] [PubMed]
- Ono, Y.; Perez-Gutierrez, A.; Nakao, T.; Dai, H.; Camirand, G.; Yoshida, O.; Yokota, S.; Stolz, D.B.; Ross, M.A.; Morelli, A.E.; et al. Graft-Infiltrating PD-L1hi Cross-Dressed Dendritic Cells Regulate Antidonor T Cell Responses in Mouse Liver Transplant Tolerance. Hepatology 2018, 67, 1499–1515. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.-L.; Mancham, S.; Hansen, B.E.; de Knegt, R.J.; de Jonge, J.; van der Laan, L.J.W.; Rivadeneira, F.; Metselaar, H.J.; Kwekkeboom, J. Counter-Regulation of Rejection Activity against Human Liver Grafts by Donor PD-L1 and Recipient PD-1 Interaction. J. Hepatol. 2016, 64, 1274–1282. [Google Scholar] [CrossRef]
- Li, Y.; Wu, Y.; Federzoni, E.A.; Wang, X.; Dharmawan, A.; Hu, X.; Wang, H.; Hawley, R.J.; Stevens, S.; Sykes, M.; et al. CD47 Cross-Dressing by Extracellular Vesicles Expressing CD47 Inhibits Phagocytosis without Transmitting Cell Death Signals. eLife 2022, 11, e73677. [Google Scholar] [CrossRef]
- Zhang, A.; Peng, Y.; Jia, J.; Nie, Y.; Zhang, S.; Xie, H.; Zhou, L.; Zheng, S. Exosome-Derived Galectin-9 May Be a Novel Predictor of Rejection and Prognosis after Liver Transplantation. J. Zhejiang Univ. Sci. B 2019, 20, 605–612. [Google Scholar] [CrossRef]
- Wang, W.; Li, W.; Cao, L.; Wang, B.; Liu, C.; Qin, Y.; Guo, B.; Huang, C. Serum Extracellular Vesicle MicroRNAs as Candidate Biomarkers for Acute Rejection in Patients Subjected to Liver Transplant. Front. Genet. 2022, 13, 1015049. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Hui, J.; Gao, L.; Liang, J.; Wang, C.; Xu, J. Extracellular Vesicles from Bone Marrow Mesenchymal Stem Cells Alleviate Acute Rejection Injury after Liver Transplantation by Carrying MiR-22-3p and Inducing M2 Polarization of Kupffer Cells. J. Gene Med. 2023, 25, e3497. [Google Scholar] [CrossRef] [PubMed]
- Cui, B.; Sun, J.; Li, S.-P.; Zhou, G.-P.; Chen, X.-J.; Sun, L.-Y.; Wei, L.; Zhu, Z.-J. CD80+ Dendritic Cell Derived Exosomes Inhibit CD8+ T Cells through Down-Regulating NLRP3 Expression after Liver Transplantation. Int. Immunopharmacol. 2022, 109, 108787. [Google Scholar] [CrossRef] [PubMed]
- Carlson, K.; Kink, J.; Hematti, P.; Al-Adra, D.P. Extracellular Vesicles as a Novel Therapeutic Option in Liver Transplantation. Liver Transpl. 2020, 26, 1522–1531. [Google Scholar] [CrossRef] [PubMed]
- Nong, K.; Wang, W.; Niu, X.; Hu, B.; Ma, C.; Bai, Y.; Wu, B.; Wang, Y.; Ai, K. Hepatoprotective Effect of Exosomes from Human-Induced Pluripotent Stem Cell–Derived Mesenchymal Stromal Cells against Hepatic Ischemia-Reperfusion Injury in Rats. Cytotherapy 2016, 18, 1548–1559. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zheng, J.; Cai, J.; Zeng, K.; Zhou, C.; Zhang, J.; Li, S.; Li, H.; Chen, L.; He, L.; et al. Extracellular Vesicles Derived from Human Umbilical Cord Mesenchymal Stem Cells Alleviate Rat Hepatic Ischemia-reperfusion Injury by Suppressing Oxidative Stress and Neutrophil Inflammatory Response. FASEB J. 2019, 33, 1695–1710. [Google Scholar] [CrossRef] [PubMed]
- Haga, H.; Yan, I.K.; Borrelli, D.A.; Matsuda, A.; Parasramka, M.; Shukla, N.; Lee, D.D.; Patel, T. Extracellular Vesicles from Bone Marrow–Derived Mesenchymal Stem Cells Protect against Murine Hepatic Ischemia/Reperfusion Injury. Liver Transpl. 2017, 23, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.-K.; Chen, C.-H.; Chang, C.-L.; Chiang, H.-J.; Sung, P.-H.; Chen, K.-H.; Chen, Y.-L.; Chen, S.-Y.; Kao, G.-S.; Chang, H.-W.; et al. Melatonin Treatment Enhances Therapeutic Effects of Exosomes against Acute Liver Ischemia-Reperfusion Injury. Am. J. Transl. Res. 2017, 9, 1543–1560. [Google Scholar]
- Zhang, Y.; Li, Y.; Wang, Q.; Zheng, D.; Feng, X.; Zhao, W.; Cai, L.; Zhang, Q.; Xu, H.; Fu, H. Attenuation of Hepatic Ischemia-reperfusion Injury by Adipose Stem Cell-derived Exosome Treatment via ERK1/2 and GSK-3β Signaling Pathways. Int. J. Mol. Med. 2021, 49, 13. [Google Scholar] [CrossRef]
- Gong, Y.; Dai, H.; Liu, W.; Liao, R.; Chen, H.; Zhang, L.; Wang, X.; Chen, Z. Exosomes Derived from Human Adipose-derived Stem Cells Alleviate Hepatic Ischemia–Reperfusion (I/R) Injury through the MiR-183/ALOX5 Axis. FASEB J. 2023, 37, e22782. [Google Scholar] [CrossRef]
- Yang, B.; Duan, W.; Wei, L.; Zhao, Y.; Han, Z.; Wang, J.; Wang, M.; Dai, C.; Zhang, B.; Chen, D.; et al. Bone Marrow Mesenchymal Stem Cell-Derived Hepatocyte-Like Cell Exosomes Reduce Hepatic Ischemia/Reperfusion Injury by Enhancing Autophagy. Stem Cells Dev. 2020, 29, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Song, Y.; Chen, L.; Li, D.; Feng, H.; Lu, Z.; Fan, T.; Chen, Z.; Livingston, M.J.; Geng, Q. MiR-20a-containing Exosomes from Umbilical Cord Mesenchymal Stem Cells Alleviates Liver Ischemia/Reperfusion Injury. J. Cell. Physiol. 2020, 235, 3698–3710. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Li, D.; Han, C.; Wu, H.; Xu, L.; Zhang, M.; Zhang, J.; Chen, X. Exosomes from Human-Induced Pluripotent Stem Cell–Derived Mesenchymal Stromal Cells (HiPSC-MSCs) Protect Liver against Hepatic Ischemia/Reperfusion Injury via Activating Sphingosine Kinase and Sphingosine-1-Phosphate Signaling Pathway. Cell. Physiol. Biochem. 2017, 43, 611–625. [Google Scholar] [CrossRef] [PubMed]
- Anger, F.; Camara, M.; Ellinger, E.; Germer, C.-T.; Schlegel, N.; Otto, C.; Klein, I. Human Mesenchymal Stromal Cell-Derived Extracellular Vesicles Improve Liver Regeneration After Ischemia Reperfusion Injury in Mice. Stem Cells Dev. 2019, 28, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Ichinohe, N.; Ishii, M.; Tanimizu, N.; Mizuguchi, T.; Yoshioka, Y.; Ochiya, T.; Suzuki, H.; Mitaka, T. Extracellular Vesicles Containing MiR-146a-5p Secreted by Bone Marrow Mesenchymal Cells Activate Hepatocytic Progenitors in Regenerating Rat Livers. Stem Cell Res. Ther. 2021, 12, 312. [Google Scholar] [CrossRef] [PubMed]
- Herrera, M.B.; Bruno, S.; Buttiglieri, S.; Tetta, C.; Gatti, S.; Deregibus, M.C.; Bussolati, B.; Camussi, G. Isolation and Characterization of a Stem Cell Population from Adult Human Liver. Stem Cells 2006, 24, 2840–2850. [Google Scholar] [CrossRef] [PubMed]
- Herrera, M.B.; Fonsato, V.; Bruno, S.; Grange, C.; Gilbo, N.; Romagnoli, R.; Tetta, C.; Camussi, G. Human Liver Stem Cells Improve Liver Injury in a Model of Fulminant Liver Failure. Hepatology 2013, 57, 311–319. [Google Scholar] [CrossRef]
- Navarro-Tableros, V.; Herrera Sanchez, M.B.; Figliolini, F.; Romagnoli, R.; Tetta, C.; Camussi, G. Recellularization of Rat Liver Scaffolds by Human Liver Stem Cells. Tissue Eng. Part A 2015, 21, 1929–1939. [Google Scholar] [CrossRef]
- Spada, M.; Porta, F.; Righi, D.; Gazzera, C.; Tandoi, F.; Ferrero, I.; Fagioli, F.; Sanchez, M.B.H.; Calvo, P.L.; Biamino, E.; et al. Intrahepatic Administration of Human Liver Stem Cells in Infants with Inherited Neonatal-Onset Hyperammonemia: A Phase I Study. Stem Cell Rev. Rep. 2020, 16, 186–197. [Google Scholar] [CrossRef]
- Calleri, A.; Roggio, D.; Navarro-Tableros, V.; De Stefano, N.; Pasquino, C.; David, E.; Frigatti, G.; Rigo, F.; Antico, F.; Caropreso, P.; et al. Protective Effects of Human Liver Stem Cell-Derived Extracellular Vesicles in a Mouse Model of Hepatic Ischemia-Reperfusion Injury. Stem Cell Rev. Rep. 2021, 17, 459–470. [Google Scholar] [CrossRef]
- Van Rijn, R.; Schurink, I.J.; de Vries, Y.; van den Berg, A.P.; Cortes Cerisuelo, M.; Darwish Murad, S.; Erdmann, J.I.; Gilbo, N.; de Haas, R.J.; Heaton, N.; et al. Hypothermic Machine Perfusion in Liver Transplantation—A Randomized Trial. N. Engl. J. Med. 2021, 384, 1391–1401. [Google Scholar] [CrossRef] [PubMed]
- Czigany, Z.; Pratschke, J.; Froněk, J.; Guba, M.; Schöning, W.; Raptis, D.A.; Andrassy, J.; Kramer, M.; Strnad, P.; Tolba, R.H.; et al. Hypothermic Oxygenated Machine Perfusion Reduces Early Allograft Injury and Improves Post-Transplant Outcomes in Extended Criteria Donation Liver Transplantation From Donation After Brain Death: Results From a Multicenter Randomized Controlled Trial (HOPE ECD-DBD). Ann. Surg. 2021, 274, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Ravaioli, M.; Germinario, G.; Dajti, G.; Sessa, M.; Vasuri, F.; Siniscalchi, A.; Morelli, M.C.; Serenari, M.; Del Gaudio, M.; Zanfi, C.; et al. Hypothermic Oxygenated Perfusion in Extended Criteria Donor Liver Transplantation—A Randomized Clinical Trial. Am. J. Transplant. 2022, 22, 2401–2408. [Google Scholar] [CrossRef]
- Schlegel, A.; Mueller, M.; Muller, X.; Eden, J.; Panconesi, R.; Von Felten, S.; Steigmiller, K.; Sousa Da Silva, R.X.; De Rougemont, O.; Mabrut, J.-Y.; et al. A Multicenter Randomized-Controlled Trial of Hypothermic Oxygenated Perfusion (HOPE) for Human Liver Grafts before Transplantation. J. Hepatol. 2023, 78, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Ghinolfi, D.; Rreka, E.; De Tata, V.; Franzini, M.; Pezzati, D.; Fierabracci, V.; Masini, M.; Cacciatoinsilla, A.; Bindi, M.L.; Marselli, L.; et al. Pilot, Open, Randomized, Prospective Trial for Normothermic Machine Perfusion Evaluation in Liver Transplantation From Older Donors. Liver Transpl. 2019, 25, 436–449. [Google Scholar] [CrossRef] [PubMed]
- Nasralla, D.; Coussios, C.C.; Mergental, H.; Akhtar, M.Z.; Butler, A.J.; Ceresa, C.D.L.; Chiocchia, V.; Dutton, S.J.; García-Valdecasas, J.C.; Heaton, N.; et al. A Randomized Trial of Normothermic Preservation in Liver Transplantation. Nature 2018, 557, 50–56. [Google Scholar] [CrossRef]
- Markmann, J.F.; Abouljoud, M.S.; Ghobrial, R.M.; Bhati, C.S.; Pelletier, S.J.; Lu, A.D.; Ottmann, S.; Klair, T.; Eymard, C.; Roll, G.R.; et al. Impact of Portable Normothermic Blood-Based Machine Perfusion on Outcomes of Liver Transplant: The OCS Liver PROTECT Randomized Clinical Trial. JAMA Surg. 2022, 157, 189. [Google Scholar] [CrossRef]
- Patrono, D.; Surra, A.; Catalano, G.; Rizza, G.; Berchialla, P.; Martini, S.; Tandoi, F.; Lupo, F.; Mirabella, S.; Stratta, C.; et al. Hypothermic Oxygenated Machine Perfusion of Liver Grafts from Brain-Dead Donors. Sci. Rep. 2019, 9, 9337. [Google Scholar] [CrossRef]
- Patrono, D.; Cussa, D.; Sciannameo, V.; Montanari, E.; Panconesi, R.; Berchialla, P.; Lepore, M.; Gambella, A.; Rizza, G.; Catalano, G.; et al. Outcome of Liver Transplantation with Grafts from Brain-Dead Donors Treated with Dual Hypothermic Oxygenated Machine Perfusion, with Particular Reference to Elderly Donors. Am. J. Transplant. 2022, 22, 1382–1395. [Google Scholar] [CrossRef]
- Brüggenwirth, I.M.A.; Mueller, M.; Lantinga, V.A.; Camagni, S.; De Carlis, R.; De Carlis, L.; Colledan, M.; Dondossola, D.; Drefs, M.; Eden, J.; et al. Prolonged Preservation by Hypothermic Machine Perfusion Facilitates Logistics in Liver Transplantation: A European Observational Cohort Study. Am. J. Transplant. 2022, 22, 1842–1851. [Google Scholar] [CrossRef]
- Ravikumar, R.; Jassem, W.; Mergental, H.; Heaton, N.; Mirza, D.; Perera, M.T.P.R.; Quaglia, A.; Holroyd, D.; Vogel, T.; Coussios, C.C.; et al. Liver Transplantation After Ex Vivo Normothermic Machine Preservation: A Phase 1 (First-in-Man) Clinical Trial. Am. J. Transplant. 2016, 16, 1779–1787. [Google Scholar] [CrossRef]
- Muller, X.; Schlegel, A.; Kron, P.; Eshmuminov, D.; Würdinger, M.; Meierhofer, D.; Clavien, P.-A.; Dutkowski, P. Novel Real-Time Prediction of Liver Graft Function During Hypothermic Oxygenated Machine Perfusion Before Liver Transplantation. Ann. Surg. 2019, 270, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Schlegel, A.; Muller, X.; Mueller, M.; Stepanova, A.; Kron, P.; De Rougemont, O.; Muiesan, P.; Clavien, P.-A.; Galkin, A.; Meierhofer, D.; et al. Hypothermic Oxygenated Perfusion Protects from Mitochondrial Injury before Liver Transplantation. EBioMedicine 2020, 60, 103014. [Google Scholar] [CrossRef]
- Mergental, H.; Laing, R.W.; Kirkham, A.J.; Perera, M.T.P.R.; Boteon, Y.L.; Attard, J.; Barton, D.; Curbishley, S.; Wilkhu, M.; Neil, D.A.H.; et al. Transplantation of Discarded Livers Following Viability Testing with Normothermic Machine Perfusion. Nat. Commun. 2020, 11, 2939. [Google Scholar] [CrossRef]
- Patrono, D.; Lonati, C.; Romagnoli, R. Viability Testing during Liver Preservation. Curr. Opin. Organ Transplant. 2022, 27, 454–465. [Google Scholar] [CrossRef] [PubMed]
- Patrono, D.; Roggio, D.; Mazzeo, A.T.; Catalano, G.; Mazza, E.; Rizza, G.; Gambella, A.; Rigo, F.; Leone, N.; Elia, V.; et al. Clinical Assessment of Liver Metabolism during Hypothermic Oxygenated Machine Perfusion Using Microdialysis. Artif. Organs 2022, 46, 281–295. [Google Scholar] [CrossRef]
- Patrono, D.; Catalano, G.; Rizza, G.; Lavorato, N.; Berchialla, P.; Gambella, A.; Caropreso, P.; Mengozzi, G.; Romagnoli, R. Perfusate Analysis During Dual Hypothermic Oxygenated Machine Perfusion of Liver Grafts: Correlations With Donor Factors and Early Outcomes. Transplantation 2020, 104, 1929–1942. [Google Scholar] [CrossRef] [PubMed]
- Patrono, D.; De Carlis, R.; Gambella, A.; Farnesi, F.; Podestà, A.; Lauterio, A.; Tandoi, F.; De Carlis, L.; Romagnoli, R. Viability Assessment and Transplantation of Fatty Liver Grafts Using End-ischemic Normothermic Machine Perfusion. Liver Transpl. 2023, 29, 508–520. [Google Scholar] [CrossRef]
- Lee, J.W.; Fang, X.; Gupta, N.; Serikov, V.; Matthay, M.A. Allogeneic Human Mesenchymal Stem Cells for Treatment of E. Coli Endotoxin-Induced Acute Lung Injury in the Ex Vivo Perfused Human Lung. Proc. Natl. Acad. Sci. USA 2009, 106, 16357–16362. [Google Scholar] [CrossRef]
- Laing, R.W.; Stubblefield, S.; Wallace, L.; Roobrouck, V.D.; Bhogal, R.H.; Schlegel, A.; Boteon, Y.L.; Reynolds, G.M.; Ting, A.E.; Mirza, D.F.; et al. The Delivery of Multipotent Adult Progenitor Cells to Extended Criteria Human Donor Livers Using Normothermic Machine Perfusion. Front. Immunol. 2020, 11, 1226. [Google Scholar] [CrossRef]
- Thompson, E.R.; Bates, L.; Ibrahim, I.K.; Sewpaul, A.; Stenberg, B.; McNeill, A.; Figueiredo, R.; Girdlestone, T.; Wilkins, G.C.; Wang, L.; et al. Novel Delivery of Cellular Therapy to Reduce Ischemia Reperfusion Injury in Kidney Transplantation. Am. J. Transplant. 2021, 21, 1402–1414. [Google Scholar] [CrossRef] [PubMed]
- Gennai, S.; Monsel, A.; Hao, Q.; Park, J.; Matthay, M.A.; Lee, J.W. Microvesicles Derived From Human Mesenchymal Stem Cells Restore Alveolar Fluid Clearance in Human Lungs Rejected for Transplantation. Am. J. Transplant. 2015, 15, 2404–2412. [Google Scholar] [CrossRef]
- Stone, M.L.; Zhao, Y.; Robert Smith, J.; Weiss, M.L.; Kron, I.L.; Laubach, V.E.; Sharma, A.K. Mesenchymal Stromal Cell-Derived Extracellular Vesicles Attenuate Lung Ischemia-Reperfusion Injury and Enhance Reconditioning of Donor Lungs after Circulatory Death. Respir. Res. 2017, 18, 212. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, S.; Lim, H.; Liu, A.; Hu, S.; Lee, J.; Zhuo, H.; Hao, Q.; Matthay, M.A.; Lee, J.-W. Therapeutic Effects of Human Mesenchymal Stem Cell Microvesicles in an Ex Vivo Perfused Human Lung Injured with Severe E. Coli Pneumonia. Thorax 2019, 74, 43–50. [Google Scholar] [CrossRef]
- Lonati, C.; Bassani, G.A.; Brambilla, D.; Leonardi, P.; Carlin, A.; Maggioni, M.; Zanella, A.; Dondossola, D.; Fonsato, V.; Grange, C.; et al. Mesenchymal Stem Cell–Derived Extracellular Vesicles Improve the Molecular Phenotype of Isolated Rat Lungs during Ischemia/Reperfusion Injury. J. Heart Lung Transplant. 2019, 38, 1306–1316. [Google Scholar] [CrossRef] [PubMed]
- Gregorini, M.; Corradetti, V.; Pattonieri, E.F.; Rocca, C.; Milanesi, S.; Peloso, A.; Canevari, S.; De Cecco, L.; Dugo, M.; Avanzini, M.A.; et al. Perfusion of Isolated Rat Kidney with Mesenchymal Stromal Cells/Extracellular Vesicles Prevents Ischaemic Injury. J. Cell. Mol. Med. 2017, 21, 3381–3393. [Google Scholar] [CrossRef]
- Rigo, F.; De Stefano, N.; Navarro-Tableros, V.; David, E.; Rizza, G.; Catalano, G.; Gilbo, N.; Maione, F.; Gonella, F.; Roggio, D.; et al. Extracellular Vesicles from Human Liver Stem Cells Reduce Injury in an Ex Vivo Normothermic Hypoxic Rat Liver Perfusion Model. Transplantation 2018, 102, e205–e210. [Google Scholar] [CrossRef]
- De Stefano, N.; Navarro-Tableros, V.; Roggio, D.; Calleri, A.; Rigo, F.; David, E.; Gambella, A.; Bassino, D.; Amoroso, A.; Patrono, D.; et al. Human Liver Stem Cell-derived Extracellular Vesicles Reduce Injury in a Model of Normothermic Machine Perfusion of Rat Livers Previously Exposed to a Prolonged Warm Ischemia. Transpl. Int. 2021, 34, 1607–1617. [Google Scholar] [CrossRef]
- Rampino, T.; Gregorini, M.; Germinario, G.; Pattonieri, E.F.; Erasmi, F.; Grignano, M.A.; Bruno, S.; Alomari, E.; Bettati, S.; Asti, A.; et al. Extracellular Vesicles Derived from Mesenchymal Stromal Cells Delivered during Hypothermic Oxygenated Machine Perfusion Repair Ischemic/Reperfusion Damage of Kidneys from Extended Criteria Donors. Biology 2022, 11, 350. [Google Scholar] [CrossRef]
- Grignano, M.A.; Bruno, S.; Viglio, S.; Avanzini, M.A.; Tapparo, M.; Ramus, M.; Croce, S.; Valsecchi, C.; Pattonieri, E.F.; Ceccarelli, G.; et al. CD73-Adenosinergic Axis Mediates the Protective Effect of Extracellular Vesicles Derived from Mesenchymal Stromal Cells on Ischemic Renal Damage in a Rat Model of Donation after Circulatory Death. Int. J. Mol. Sci. 2022, 23, 10681. [Google Scholar] [CrossRef]
- Du, S.; Guan, Y.; Xie, A.; Yan, Z.; Gao, S.; Li, W.; Rao, L.; Chen, X.; Chen, T. Extracellular Vesicles: A Rising Star for Therapeutics and Drug Delivery. J. Nanobiotechnol. 2023, 21, 231. [Google Scholar] [CrossRef] [PubMed]
- Kou, M.; Huang, L.; Yang, J.; Chiang, Z.; Chen, S.; Liu, J.; Guo, L.; Zhang, X.; Zhou, X.; Xu, X.; et al. Mesenchymal Stem Cell-Derived Extracellular Vesicles for Immunomodulation and Regeneration: A next Generation Therapeutic Tool? Cell Death Dis. 2022, 13, 580. [Google Scholar] [CrossRef] [PubMed]
- Pirisinu, M.; Pham, T.C.; Zhang, D.X.; Hong, T.N.; Nguyen, L.T.; Le, M.T. Extracellular Vesicles as Natural Therapeutic Agents and Innate Drug Delivery Systems for Cancer Treatment: Recent Advances, Current Obstacles, and Challenges for Clinical Translation. Semin. Cancer Biol. 2022, 80, 340–355. [Google Scholar] [CrossRef]
- Blondeel, J.; Gilbo, N.; De Bondt, S.; Monbaliu, D. Stem Cell Derived Extracellular Vesicles to Alleviate Ischemia-Reperfusion Injury of Transplantable Organs. A Systematic Review. Stem Cell Rev. Rep. 2023. ahead of print. [Google Scholar] [CrossRef]
- Yoo, M.H.; Lee, A.-R.; Moon, K.-S. Characteristics of Extracellular Vesicles and Preclinical Testing Considerations Prior to Clinical Applications. Biomedicines 2022, 10, 869. [Google Scholar] [CrossRef] [PubMed]
- Théry, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal Information for Studies of Extracellular Vesicles 2018 (MISEV2018): A Position Statement of the International Society for Extracellular Vesicles and Update of the MISEV2014 Guidelines. J. Extracell. Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Author | Disease | Population | EVs Subtype | Outcomes |
|---|---|---|---|---|
| Stravitz et al., 2013 [25] | ALF |
50 ALI (39 ALF): 27 spontaneous survivors, 23 LT or death |
|
|
| Wang et al., 2013 [38] | HCC |
55 HCC 40 LC | NA |
|
| Sugimachi et al., 2015 [43] | HCC | 65 LDLT for HCC | TSG101+ | Exosomal miR-718 was downregulated in patients who presented HCC recurrence |
| Engelmann et al., 2017 [21] | aCLD | 163 LC |
|
|
| Julich-Haertel et al., 2017 [50] | HCC/CCA |
22 HCC 26 CCA | AnnexinV + EpCAM + tumor-associated EVs |
|
| Payancè et al., 2018 [49] | aCLD | 242 LC | Hepatocyte-derived EV (CK-18+) |
|
| Sukriti et al., 2018 [27] | AH | 101 AH (71 responders, 30 non-responders to steroid therapy) |
| Baseline serum EV levels predicted steroid non-response in 94% of cases |
| Xue et al., 2019 [39] | AH |
80 HCC 30 healthy controls |
| Exosomal miR-106a was a prognostic factor for HCC, predicting 2- and 10-year survival |
| Fang et al., 2018 [40] | HCC |
90 HCC without lung metastasis 20 HCC with lung metastasis | HCC-derived EVs |
|
| Lee et al., 2019 [41] | HCC | 79 HCC |
|
|
| Nakano et al., 2019 [44] | HCC | 93 HCC pts who underwent LDLT | NA | Increase in exosomal miR-92b before LDLT reflects a risk for posttransplant early HCC recurrence |
| Sorop et al., 2020 [35] | HCC |
48 HCC 38 LC |
| Exosomal miR-21-5p was upregulated, and miR-92a-3p was downregulated in HCC patients |
| Lapitz et al., 2023 [48] | CCA | 45 PSC 69 PSC-CCA 56 CA 34 HCC |
|
|
| Author | Organ | Injury | Perfusion | Timing | Treatment | Dose | Outcomes |
|---|---|---|---|---|---|---|---|
| Gennai et al., 2015 [112] | Human lungs | Grafts rejected for transplant | Normothermic | 8 h | BM-MSC-EVs | 100 or 200 μL of supernatant (10 μL isolated from 1 × 106 cells) | ↑ Alveolar fluid clearance, ↑ Pulmonary compliance ↓ PAP and PVR |
| Stone et al., 2017 [113] | Mouse lungs |
Warm ischemia (60 min) | Normothermic | 1 h | Umbilical cord derived-MSC-EVs | 1 × 106 EVs prior to ischemia and 3 × 106 EVs during perfusion | ↑ Pulmonary compliance ↓ PAP ↓ Edema and neutrophil infiltration |
| Gregorini et al., 2017 [116] | Rat kidney |
Warm ischemia (20 min) | Hypothermic | 4 h | BM-MSC-EVs | EVs isolated from 3 × 106 cells | ↓ Tissue injury ↓ Lactate, LDH, MDA |
| Rigo et al., 2018 [117] | Rat liver | Hypoxic injury | Normothermic | 4 h | HLSC-EVs | 5 × 108 EVs/g liver | ↓ AST, LDH ↓ tissue injury, apoptotic cells ↓ HIF-1α, TGF-β1 |
| Park et al., 2019 [114] | Human lungs | Grafts rejected for transplant with E. coli pneumonia | Normothermic | 6 h | BM-MSC-EVs | 200 or 400 μL of supernatant (10 μL × 1 × 106 cells) | ↑ Alveolar fluid clearance |
| Lonati et al., 2019 [115] | Rat lungs | - | Normothermic | 3 h | MSC-EVs | 24.56 ± 5.53 × 1010 EVs | ↓ PVR ↑ NO metabolites and ATP |
| De Stefano et al., 2021 [118] | Rat liver |
Warm ischemia (60 min) | Normothermic | 6 h | HLSC-EVs | 5 × 108 EVs/g liver 25 × 108 EVs/g liver | ↓ AST, ALT, phosphates, ↓ Total HCO3− need ↑ Bile production (High dose only) ↓ Necrosis ↑ proliferation (High dose only) ↓ Vascular resistance (High dose only) |
| Rampino et al., 2022 [119] | Human kidney | Grafts rejected for transplant | Hypothermic | 4 h | BM-MSC-EVs | 28.5 × 109 EVs | ↓ Tissue injury ↓ caspase-3 ↑ COX IV-1, HGF and VEGF |
| Grignano et al., 2022 [120] | Rat kidney |
Warm ischemia (20 min) | Hypothermic | 4 h | BM-MSC-EVs or BM-MSC-EVs silenced for CD73 | EVs isolated from 3 × 106 cells | ↓ Tissue injury ↑ ATP and tubular proliferation Silencing CD73 abolished protection |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Stefano, N.; Calleri, A.; Faini, A.C.; Navarro-Tableros, V.; Martini, S.; Deaglio, S.; Patrono, D.; Romagnoli, R. Extracellular Vesicles in Liver Transplantation: Current Evidence and Future Challenges. Int. J. Mol. Sci. 2023, 24, 13547. https://doi.org/10.3390/ijms241713547
De Stefano N, Calleri A, Faini AC, Navarro-Tableros V, Martini S, Deaglio S, Patrono D, Romagnoli R. Extracellular Vesicles in Liver Transplantation: Current Evidence and Future Challenges. International Journal of Molecular Sciences. 2023; 24(17):13547. https://doi.org/10.3390/ijms241713547
Chicago/Turabian StyleDe Stefano, Nicola, Alberto Calleri, Angelo Corso Faini, Victor Navarro-Tableros, Silvia Martini, Silvia Deaglio, Damiano Patrono, and Renato Romagnoli. 2023. "Extracellular Vesicles in Liver Transplantation: Current Evidence and Future Challenges" International Journal of Molecular Sciences 24, no. 17: 13547. https://doi.org/10.3390/ijms241713547