
Immunohistochemical Expression of Glutathione Peroxidase-2 (Gpx-2) and Its Clinical Relevance in Colon Adenocarcinoma Patients
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
2.2. Correlations between Gpx-2 Immunohistochemical Expression and Clinicopathological Parameters (as Independent Variables)
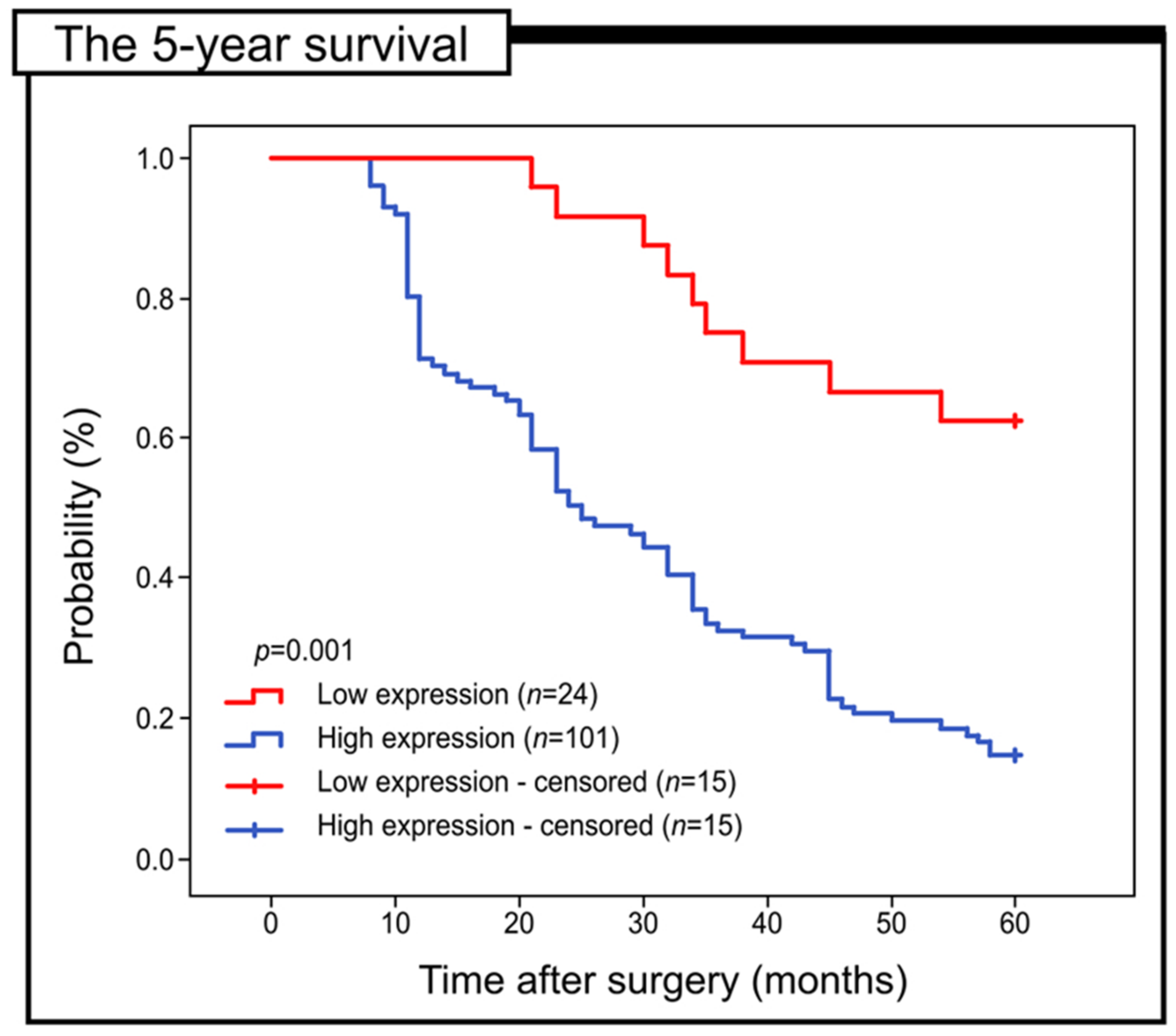
2.3. Prognostic Role of Gpx-2 Expression in Colon Adenocarcinoma
2.4. Immunofluorescence Staining
2.5. Intracellular Localization of Gpx-2 using the Method of Immunogold Labelling with the Use of Transmission Electron Microscopy (TEM)
3. Discussion
4. Materials and Methods
4.1. Patients and Tumour Samples
4.2. Immunohistochemical and Immunofluorescence Staining
4.3. Immunogold Electron Microscopy
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Gpx-2 | glutathione peroxidase 2 |
| COAD | colon adenocarcinoma |
| CRC | colorectal cancer |
| ROS | reactive oxygen species |
| H2O2 | hydrogen peroxide |
| PCNA | proliferating cell nuclear antigen |
| NSCLC | non-small cell lung cancer cells |
| HCC | hepatocellular carcinoma |
| PC | pancreatic cancer |
| EMT | epithelial to mesenchymal transition |
| LPR | Dako Liquid Permanent Red chromogen |
| BSA | bovine serum albumin |
References
- Li, X.; Yu, W.; Liang, C.; Xu, Y.; Zhang, M.; Ding, X.; Cai, X. INHBA is a prognostic predictor for patients with colon adenocarcinoma. BMC Cancer 2020, 20, 305. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Huang, J.; Lok, V.; Wang, J.; Fung, F.; Ding, H.; Zheng, Z.J. Differences in Incidence and Mortality Trends of Colorectal Cancer Worldwide Based on Sex, Age, and Anatomic Location. Clin. Gastroenterol. Hepatol. 2021, 19, 955–966.e61. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Paschke, S.; Jafarov, S.; Staib, L.; Kreuser, E.D.; Maulbecker-Armstrong, C.; Roitman, M.; Holm, T.; Harris, C.C.; Link, K.H.; Kornmann, M. Are Colon and Rectal Cancer Two Different Tumor Entities? A Proposal to Abandon the Term Colorectal Cancer. Int. J. Mol. Sci. 2018, 19, 2577. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Jin, Y.; Chen, Y.; Jiang, Z.; Liu, Z.; Zhao, Z.; Yan, P.; Wang, G.; Wang, X. The Incidence Characteristics of Second Primary Malignancy after Diagnosis of Primary Colon and Rectal Cancer: A Population Based Study. PLoS ONE 2015, 10, e0143067. [Google Scholar] [CrossRef]
- Margis, R.; Dunand, C.; Teixeira, F.K.; Margis-Pinheiro, M. Glutathione peroxidase family—An evolutionary overview. FEBS J. 2008, 275, 3959–3970. [Google Scholar] [CrossRef]
- Zhang, L.; Wu, M.; Yu, D.; Teng, Y.; Wei, T.; Chen, C.; Song, W. Identification of Glutathione Peroxidase (GPX) Gene Family in Rhodiola crenulata and Gene Expression Analysis under Stress Conditions. Int. J. Mol. Sci. 2018, 19, 3329. [Google Scholar] [CrossRef]
- Emmink, B.L.; Laoukili, J.; Kipp, A.P.; Koster, J.; Govaert, K.M.; Fatrai, S.; Verheem, A.; Steller, E.J.; Brigelius-Flohé, R.; Jimenez, C.R.; et al. GPx2 suppression of H2O2 stress links the formation of differentiated tumor mass to metastatic capacity in colorectal cancer. Cancer Res. 2014, 74, 6717–6730. [Google Scholar] [CrossRef]
- Naiki, T.; Naiki-Ito, A.; Iida, K.; Etani, T.; Kato, H.; Suzuki, S.; Yamashita, Y.; Kawai, N.; Yasui, T.; Takahashi, S. GPX2 promotes development of bladder cancer with squamous cell differentiation through the control of apoptosis. Oncotarget 2018, 9, 15847–15859. [Google Scholar] [CrossRef]
- Liu, T.; Kan, X.F.; Ma, C.; Chen, L.L.; Cheng, T.T.; Zou, Z.W.; Li, Y.; Cao, F.J.; Zhang, W.J.; Yao, J.; et al. GPX2 overexpression indicates poor prognosis in patients with hepatocellular carcinoma. Tumor Biol. 2017, 39, 1010428317700410. [Google Scholar] [CrossRef] [PubMed]
- Lei, C.; Chen, W.; Wang, Y.; Zhao, B.; Liu, P.; Kong, Z.; Liu, D.; Dai, C.; Wang, Y.; Wang, Y.; et al. Prognostic Prediction Model for Glioblastoma: A Metabolic Gene Signature and Independent External Validation. J. Cancer 2021, 12, 3796–3808. [Google Scholar] [CrossRef] [PubMed]
- Brigelius-Flohé, R.; Maiorino, M. Glutathione peroxidases. Biochim. Biophys. Acta 2013, 1830, 3289–3303. [Google Scholar] [CrossRef] [PubMed]
- Chu, F.F.; Doroshow, J.H.; Esworthy, R.S. Expression, characterization, and tissue distribution of a new cellular selenium-dependent glutathione peroxidase, GSHPx-GI. J. Biol. Chem. 1993, 268, 2571–2576. [Google Scholar] [CrossRef]
- Florian, S.; Wingler, K.; Schmehl, K.; Jacobasch, G.; Kreuzer, O.J.; Meyerhof, W.; Brigelius-Flohé, R. Cellular and subcellular localization of gastrointestinal glutathione peroxidase in normal and malignant human intestinal tissue. Free Radic. Res. 2001, 35, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Murawaki, Y.; Tsuchiya, H.; Kanbe, T.; Harada, K.; Yashima, K.; Nozaka, K.; Tanida, O.; Kohno, M.; Mukoyama, T.; Nis-Himuki, E.; et al. Aberrant expression of selenoproteins in the progression of colorectal cancer. Cancer Lett. 2008, 259, 218–230. [Google Scholar] [CrossRef]
- Pellavio, G.; Martinotti, S.; Patrone, M.; Ranzato, E.; Laforenza, U. Aquaporin-6 May Increase the Resistance to Oxidative Stress of Malignant Pleural Mesothelioma Cells. Cells 2022, 11, 1892. [Google Scholar] [CrossRef]
- Zaric, B.L.; Macvanin, M.T.; Isenovic, E.R. Free radicals: Relationship to Human Diseases and Potential Therapeutic applications. Int. J. Biochem. Cell Biol. 2023, 154, 106346. [Google Scholar] [CrossRef]
- Halliwell, B. Reactive oxygen species (ROS), oxygen radicals and antioxidants: Where are we now, where is the field going and where should we go? Biochem. Biophys. Res. Commun. 2022, 633, 17–19. [Google Scholar] [CrossRef]
- Zinellu, A.; Mangoni, A.A. A Systematic Review and Meta-Analysis of the Effect of Statins on Glutathione Peroxidase, Superoxide Dismutase, and Catalase. Antioxidants 2021, 10, 1841. [Google Scholar] [CrossRef]
- Brigelius-Flohé, R.; Kipp, A. Glutathione peroxidases in different stages of carcinogenesis. Biochim. Biophys. Acta 2009, 1790, 1555–1568. [Google Scholar] [CrossRef] [PubMed]
- Kelman, Z. PCNA: Structure, functions and interactions. Oncogene 1997, 14, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Sun, L.; Tong, J.; Chen, X.; Li, H.; Zhang, Q. Prognostic significance of glutathione peroxidase 2 in gastric carcinoma. Tumor Biol. 2017, 39, 1010428317701443. [Google Scholar] [CrossRef] [PubMed]
- Lei, Z.; Tian, D.; Zhang, C.; Zhao, S.; Su, M. Clinicopathological and prognostic significance of GPX2 protein expression in esophageal squamous cell carcinoma. BMC Cancer 2016, 16, 410. [Google Scholar] [CrossRef]
- Suzuki, S.; Pitchakarn, P.; Ogawa, K.; Naiki-Ito, A.; Chewonarin, T.; Punfa, W.; Asamoto, M.; Shirai, T.; Takahashi, S. Expression of glutathione peroxidase 2 is associated with not only early hepatocarcinogenesis but also late stage metastasis. Toxicology 2013, 311, 115–123. [Google Scholar] [CrossRef]
- Naiki-Ito, A.; Asamoto, M.; Hokaiwado, N.; Takahashi, S.; Yamashita, H.; Tsuda, H.; Ogawa, K.; Shirai, T. Gpx2 is an overexpressed gene in rat breast cancers induced by three different chemical carcinogens. Cancer Res. 2007, 67, 11353–11358. [Google Scholar] [CrossRef]
- Naiki, T.; Naiki-Ito, A.; Asamoto, M.; Kawai, N.; Tozawa, K.; Etani, T.; Sato, S.; Suzuki, S.; Shirai, T.; Kohri, K.; et al. GPX2 overexpression is involved in cell proliferation and prognosis of castration-resistant prostate cancer. Carcinogenesis 2014, 35, 1962–1967. [Google Scholar] [CrossRef]
- Croute, F.; Beau, B.; Murat, J.C.; Vincent, C.; Komatsu, H.; Obata, F.; Soleilhavoup, J.P. Expression of stress-related genes in a cadmium-resistant A549 human cell line. J. Toxicol. Environ. Health Part A 2005, 68, 703–718. [Google Scholar] [CrossRef]
- Ren, Z.; Liang, H.; Galbo, P.M., Jr.; Dharmaratne, M.; Kulkarni, A.S.; Fard, A.T.; Aoun, M.L.; Martinez-Lopez, N.; Suyama, K.; Benard, O.; et al. Redox signaling by glutathione peroxidase 2 links vascular modulation to metabolic plasticity of breast cancer. Proc. Natl. Acad. Sci. USA 2022, 119, e2107266119. [Google Scholar] [CrossRef]
- Chang, I.W.; Lin, V.C.; Hung, C.H.; Wang, H.P.; Lin, Y.Y.; Wu, W.J.; Huang, C.N.; Li, C.C.; Li, W.M.; Wu, J.Y.; et al. GPX2 underexpression indicates poor prognosis in patients with urothelial carcinomas of the upper urinary tract and urinary bladder. World J. Urol. 2015, 33, 1777–1789. [Google Scholar] [CrossRef]
- Peng, F.; Xu, Q.; Jing, X.; Chi, X.; Zhang, Z.; Meng, X.; Liu, X.; Yan, J.; Liu, X.; Shao, S. GPX2 promotes EMT and metastasis in non-small cell lung cancer by activating PI3K/AKT/mTOR/Snail signaling axis. FASEB BioAdvances 2023, 5, 233–250. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.; Zhang, K.; Chen, X.; Yang, L.; Zhu, S.; Wei, Y.; Xie, Z.; Chen, Y.; Shang, C. GPX2 is a potential therapeutic target to induce cell apoptosis in lenvatinib against hepatocellular carcinoma. J. Adv. Res. 2023, 44, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Dai, L.; Niu, J. GPX2 silencing relieves epithelial-mesenchymal transition, invasion, and metastasis in pancreatic cancer by downregulating Wnt pathway. J. Cell. Physiol. 2020, 235, 7780–7790. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.; Tuli, H.S.; Varol, A.; Thakral, F.; Yerer, M.B.; Sak, K.; Varol, M.; Jain, A.; Khan, M.A.; Sethi, G. Role of Reactive Oxygen Species in Cancer Progression: Molecular Mechanisms and Recent Advancements. Biomolecules 2019, 9, 735. [Google Scholar] [CrossRef] [PubMed]
- Esworthy, R.S.; Doroshow, J.H.; Chu, F.F. The beginning of GPX2 and 30 years later. Free Radic. Biol. Med. 2022, 188, 419–433. [Google Scholar] [CrossRef]
- Wang, M.; Chen, X.; Fu, G.; Ge, M. Glutathione peroxidase 2 overexpression promotes malignant progression and cisplatin resistance of KRAS-mutated lung cancer cells. Oncol. Rep. 2022, 48, 207. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Vorschlag zur einheitlichen Definition eines Immunreaktiven Score (IRS) für den im-mun-histochemischen Ostrogenrezeptor-Nachweis (ER-ICA) im Mammakarzinomgewebe [Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical oestrogen receptor detection (ER-ICA) in breast cancer tissue]. Der Pathologe 1987, 8, 138–140. [Google Scholar]
- Alnuaimi, A.R.; Bottner, J.; Nair, V.A.; Ali, N.; Alnakhli, R.; Dreyer, E.; Talaat, I.M.; Busch, H.; Perner, S.; Kirfel, J.; et al. Immunohistochemical Expression Analysis of Caldesmon Isoforms in Colorectal Carcinoma Reveals Interesting Correlations with Tumor Characteristics. Int. J. Mol. Sci. 2023, 24, 2275. [Google Scholar] [CrossRef]
- Brzozowa-Zasada, M.; Piecuch, A.; Michalski, M.; Matysiak, N.; Kucharzewski, M.; Łos, M.J. The Clinical Application of Immunohistochemical Expression of Notch4 Protein in Patients with Colon Adenocarcinoma. Int. J. Mol. Sci. 2023, 24, 7502. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (Number of Cases) | % | ||
|---|---|---|---|
| Gender | Females | 60 | 48.00 |
| Males | 65 | 52.00 | |
| Age (years) | ≤60 years | 43 | 34.40 |
| 61–75 years | 44 | 35.20 | |
| >75 years | 38 | 30.40 | |
| M ± SD | 65.54 ± 13.11 | ||
| Me (Q1–Q3) | 65 (56–77) | ||
| Min–Max | 33–89 | ||
| Grade of histological differentiation (G) | G1 | 22 | 17.60 |
| G2 | 64 | 51.20 | |
| G3 | 39 | 31.20 | |
| Depth of invasion (T) | T1 | 10 | 8.00 |
| T2 | 14 | 11.20 | |
| T3 | 78 | 62.40 | |
| T4 | 23 | 18.40 | |
| Regional lymph node involvement (N) | N0 | 45 | 36.00 |
| N1 | 45 | 36.00 | |
| N2 | 35 | 28.00 | |
| Location of tumour | Proximal | 63 | 50.40 |
| Distal | 62 | 49.60 | |
| Angioinvasion | No | 27 | 21.60 |
| Yes | 98 | 78.40 | |
| PCNA immunohistochemical expression | Low | 17 | 13.60 |
| High | 108 | 86.40 | |
| Staging | I | 14 | 11.20 |
| II | 31 | 24.80 | |
| III | 80 | 64.00 | |
| The Immunoexpression Level of Gpx-2 | p-Value | |||||
|---|---|---|---|---|---|---|
| Low | High | |||||
| PCNA expression | Low | 12 | (9.60%) | 5 | (4.00%) | p < 0.001 |
| High | 12 | (9.60%) | 96 | (76.80%) | p = 0.146 | |
| The Immunoexpression Level of Gpx-2 | ||||||
|---|---|---|---|---|---|---|
| Low | High | p-Value | ||||
| Age (years) | ≤60 years | 7 | (16.28%) | 36 | (83.72%) | p = 0.410 |
| 61–75 years | 7 | (15.91%) | 37 | (84.09%) | ||
| >75 years | 10 | (26.32%) | 28 | (73.68%) | ||
| Gender | Females | 13 | (21.67%) | 47 | (78.33%) | p = 0.501 |
| Males | 11 | (16.92%) | 54 | (83.08%) | ||
| Grade of histological differentiation (G) | G1 | 16 | (72.73%) | 6 | (27.27%) | p < 0.001 |
| G2 | 7 | (10.94%) | 57 | (89.06%) | ||
| G3 | 1 | (2.6%) | 38 | (97.44%) | ||
| Depth of invasion (T) | T1/T2 | 11 | (45.83%) | 13 | (54.17%) | p = 0.001 |
| T3/T4 | 13 | (12.87%) | 88 | (87.13%) | ||
| Regional lymph node involvement (N) | N0 | 10 | (22.22%) | 35 | (77.78%) | p = 0.661 |
| N1 | 9 | (20.00%) | 36 | (80.00%) | ||
| N2 | 5 | (14.29%) | 30 | (85.71%) | ||
| Location of tumour | Proximal | 8 | (12.70%) | 55 | (87.30%) | p = 0.063 |
| Distal | 16 | (25.81%) | 46 | (74.19%) | ||
| Angioinvasion | No | 15 | (55.56%) | 12 | (44.44%) | p < 0.001 |
| Yes | 9 | (9.18%) | 89 | (90.82%) | ||
| PCNA immunohistochemical expression | Low | 12 | (70.59%) | 5 | (29.41%) | p < 0.001 |
| High | 12 | (11.11%) | 96 | (88.89%) | ||
| Staging | I | 7 | (50.00%) | 7 | (50.00%) | p = 0.005 |
| II | 3 | (9.68%) | 28 | (90.32%) | ||
| III | 14 | (17.50%) | 66 | (82.50%) | ||
| Prognostic Parameter | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Gender | 0.898 | 0.600–1.343 | 0.600 | - | - | - |
| Age | 0.999 | 0.985–1.014 | 0.912 | - | - | - |
| Grade of histological differentiation (G) | 2.382 | 1.751–3.241 | <0.001 | 1.919 | 1.254–2.936 | 0.003 |
| Depth of invasion (T) | 1.664 | 1.265–2.188 | <0.001 | 1.045 | 0.739–1.478 | 0.803 |
| Regional LN involvement (N) | 1.136 | 0.885–1.458 | 0.318 | - | - | - |
| Location of tumour | 1.063 | 0.711–1.590 | 0.767 | - | - | - |
| Gpx-2 immunohistochemical expression | 4.046 | 2.028–8.072 | <0.001 | 2.286 | 1.069–4.890 | 0.033 |
| Angioinvasion | 2.745 | 1.522–4.950 | 0.001 | 0.948 | 0.434–2.070 | 0.893 |
| PCNA immunohistochemical expression | 4.133 | 1.800–9.486 | 0.001 | 1.242 | 0.387–3.987 | 0.715 |
| Staging | 1.287 | 0.956–1.731 | 0.096 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzozowa-Zasada, M.; Ianaro, A.; Piecuch, A.; Michalski, M.; Matysiak, N.; Stęplewska, K. Immunohistochemical Expression of Glutathione Peroxidase-2 (Gpx-2) and Its Clinical Relevance in Colon Adenocarcinoma Patients. Int. J. Mol. Sci. 2023, 24, 14650. https://doi.org/10.3390/ijms241914650
Brzozowa-Zasada M, Ianaro A, Piecuch A, Michalski M, Matysiak N, Stęplewska K. Immunohistochemical Expression of Glutathione Peroxidase-2 (Gpx-2) and Its Clinical Relevance in Colon Adenocarcinoma Patients. International Journal of Molecular Sciences. 2023; 24(19):14650. https://doi.org/10.3390/ijms241914650
Chicago/Turabian StyleBrzozowa-Zasada, Marlena, Angela Ianaro, Adam Piecuch, Marek Michalski, Natalia Matysiak, and Katarzyna Stęplewska. 2023. "Immunohistochemical Expression of Glutathione Peroxidase-2 (Gpx-2) and Its Clinical Relevance in Colon Adenocarcinoma Patients" International Journal of Molecular Sciences 24, no. 19: 14650. https://doi.org/10.3390/ijms241914650