
Adipokines and Inflammatory Markers in Acute Myocardial Infarction Patients with and without Obstructive Sleep Apnea: A Comparative Analysis
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Clinical Features
2.2. Sleep Quality
2.3. Home Respiratory Polygraphy
2.4. Serum Levels of Inflammatory Mediators
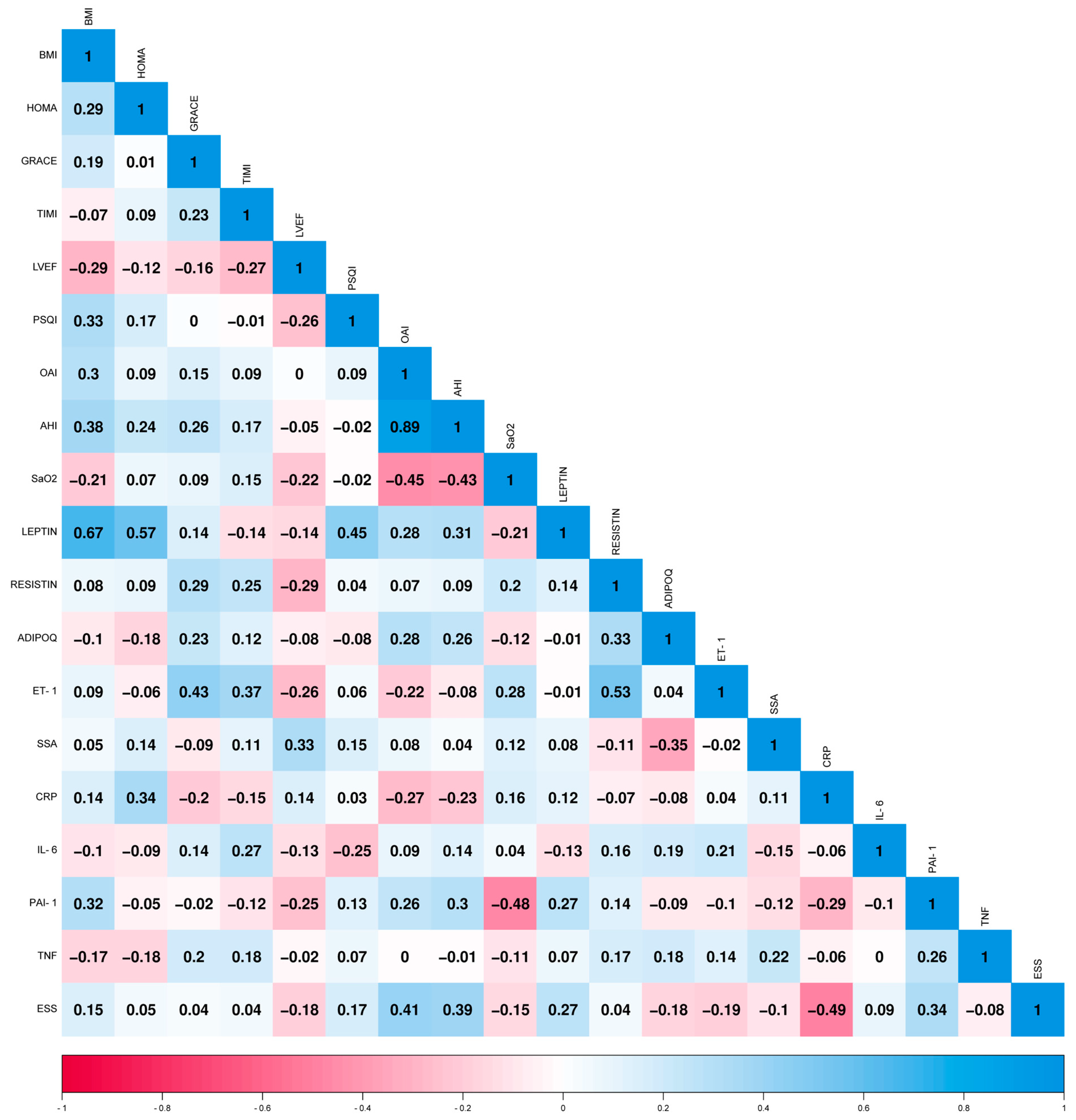
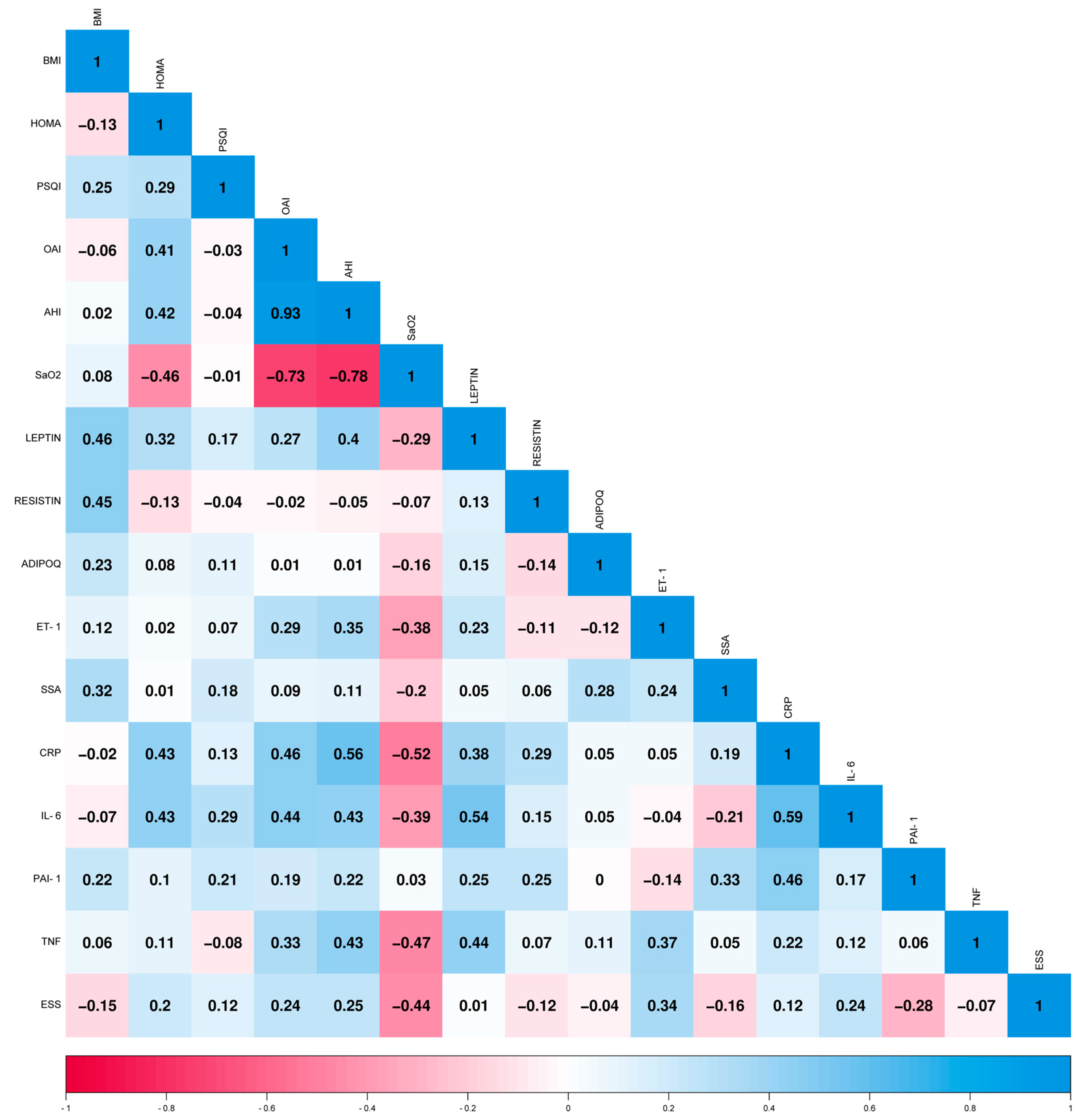
2.5. Correlation of Adipokine Levels with Biomarkers for Clinical Use and Risk Scales
2.5.1. AMI Patients
2.5.2. Control Subjects
3. Discussion
4. Material and Methods
4.1. Study Participants
Ethical Approval
4.2. AMI Diagnosis
4.2.1. Clinical Classification of AMI
4.2.2. Risk Scale for AMI
4.3. Laboratory Procedures
4.4. Sleep Quality Assessment
4.5. Home Respiratory Polygraphy
4.6. Diagnosis of Obstructive Sleep Apnea
4.7. Body Composition Analysis
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mitsis, A.; Gragnano, F. Myocardial Infarction with and without ST-segment Elevation: A Contemporary Reappraisal of Similarities and Differences. Curr. Cardiol. Rev. 2021, 17, e230421189013. [Google Scholar] [CrossRef]
- Stătescu, C.; Anghel, L.; Tudurachi, B.-S.; Leonte, A.; Benchea, L.-C.; Sascău, R.-A. From Classic to Modern Prognostic Biomarkers in Patients with Acute Myocardial Infarction. Int. J. Mol. Sci. 2022, 23, 9168. [Google Scholar] [CrossRef]
- Buchner, S.; Wester, M.; Hobelsberger, S.; Fisser, C.; Debl, K.; Hetzenecker, A.; Hamer, O.-W.; Zeman, F.; Maier, L.-S.; Arzt, M. Obstructive sleep apnoea is associated with the development of diastolic dysfunction after myocardial infarction with preserved ejection fraction. Sleep Med. 2022, 94, 63–69. [Google Scholar] [CrossRef]
- Garcia-Rio, F.; Alonso-Fernández, A.; Armada, E.; Mediano, O.; Lores, V.; Rojo, B.; Fernández-Lahera, J.; Fernández-Navarro, I.; Carpio, C.; Ramírez, T. CPAP effect on recurrent episodes in patients with sleep apnea and myocardial infarction. Int. J. Cardiol. 2013, 168, 1328–1335. [Google Scholar] [CrossRef]
- Khokhrina, A.; Andreeva, E.; Degryse, J.-M. A systematic review on the association of sleep-disordered breathing with cardiovascular pathology in adults. NPJ Prim. Care Respir. Med. 2022, 32, 41. [Google Scholar] [CrossRef]
- Lévy, P.; Pépin, J.-L.; Arnaud, C.; Tamisier, R.; Borel, J.-C.; Dematteis, M.; Godin-Ribuot, D.; Ribuot, C. Intermittent hypoxia and sleep-disordered breathing: Current concepts and perspectives. Eur. Respir. J. 2008, 32, 1082–1095. [Google Scholar] [CrossRef]
- Mitra, A.-K.; Bhuiyan, A.-R.; Jones, E.-A. Association and Risk Factors for Obstructive Sleep Apnea and Cardiovascular Diseases: A Systematic Review. Diseases 2021, 2, 88. [Google Scholar] [CrossRef]
- Nicolini, A.; Piroddi, I.-M.-G.; Barbagelata, E.; Barlascini, C. Obesity and Breathing Related Sleep Disorders. In Obesity; Ahmad, S., Imam, S., Eds.; Springer: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- Kirichenko, T.-V.; Markina, Y.-V.; Bogatyreva, A.-I.; Tolstik, T.-V.; Varaeva, Y.-R.; Starodubova, A.-V. The Role of Adipokines in Inflammatory Mechanisms of Obesity. Int. J. Mol. Sci. 2022, 23, 14982. [Google Scholar] [CrossRef]
- Xu, X.; Xu, J. Effects of different obesity-related adipokines on the occurrence of obstructive sleep apnea. Endocr. J. 2020, 67, 485–500. [Google Scholar] [CrossRef]
- Singh, M.; Benencia, F. Inflammatory processes in obesity: Focus on endothelial dysfunction and the role of adipokines as inflammatory mediators. Int. Rev. Immunol. 2019, 38, 157–171. [Google Scholar] [CrossRef]
- Janmohammadi, P.; Raeisi, T.; Zarei, M.; Nejad, M.-M.; Karimi, R.; Mirali, Z.; Zafary, R.; Alizadeh, S. Adipocytokines in obstructive sleep apnea: A systematic review and meta-analysis. Respir. Med. 2023, 208, 107122. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Chen, Y.; Upender, R.-P. Adipokines in Sleep Disturbance and Metabolic Dysfunction: Insights from Network Analysis. Clocks Sleep 2022, 4, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.; Arnaud, C.; Fitzpatrick, S.-F.; Gaucher, J.; Tamisier, R.; Pépin, J.-L. Adipose tissue as a key player in obstructive sleep apnoea. Eur. Respir. Rev. 2019, 26, 190006. [Google Scholar] [CrossRef] [PubMed]
- Redline, S.; Azarbarzin, A.; Peker, Y. Obstructive sleep apnoea heterogeneity and cardiovascular disease. Nat. Rev. Cardiol. 2023, 20, 560–573. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P.; McHill, A.-W.; Cox, R.-C.; Broussard, J.-L.; Dutil, C.; da Costa, B.-G.-G.; Sampasa-Kanyinga, H.; Wright, K.-P., Jr. The role of insufficient sleep and circadian misalignment in obesity. Nat. Rev. Endocrinol. 2023, 2, 82–97. [Google Scholar] [CrossRef]
- Zitser, J.; Allen, I.-E.; Falgàs, N.; Le, M.-M.; Neylan, T.-C.; Kramer, J.-H.; Walsh, C.-M. Pittsburgh Sleep Quality Index (PSQI) responses are modulated by total sleep time and wake after sleep onset in healthy older adults. PLoS ONE 2022, 6, e0270095. [Google Scholar] [CrossRef]
- Sejbuk, M.; Mirończuk-Chodakowska, I.; Witkowska, A.M. Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients 2022, 14, 1912. [Google Scholar] [CrossRef]
- Javaheri, S.; Barbe, F.; Campos-Rodriguez, F.; Dempsey, J.-A.; Khayat, R.; Javaheri, S.; Malhotra, A.; Martinez-Garcia, M.-A.; Mehra, R.; Pack, A.-I.; et al. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequences. J. Am. Coll. Cardiol. 2017, 69, 841–858. [Google Scholar] [CrossRef]
- Lévy, P.; Kohler, M.; McNicholas, W.-T.; Barbé, F.; McEvoy, R.-D.; Somers, V.-K.; Lavie, L.; Pépin, J.-L. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Primers 2015, 25, 15015. [Google Scholar] [CrossRef]
- Oikonomou, E.-K.; Antoniades, C. The role of adipose tissue in cardiovascular health and disease. Nat. Rev. Cardiol. 2019, 16, 83–99. [Google Scholar] [CrossRef]
- Lam, D.-C.; Lam, K.-S.; Ip, M.-S. Obstructive sleep apnoea, insulin resistance and adipocytokines. Clin. Endocrinol. 2015, 82, 165–177. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.-L.; Lugus, J.-J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Broch, K.; Anstensrud, A.-K.; Woxholt, S.; Sharma, K.; Tøllefsen, I.-M.; Bendz, B.; Aakhus, S.; Ueland, T.; Amundsen, B.-H.; Damås, J.-K.; et al. Randomized Trial of Interleukin-6 Receptor Inhibition in Patients with Acute ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2021, 77, 1845–1855. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, K.; Devarajan, N.; Ganesan, M.; Ragunathan, M. Obesity, Inflammation and Acute Myocardial Infarction—Expression of leptin, IL-6 and high sensitivity-CRP in Chennai based population. Thromb. J. 2012, 10, 13. [Google Scholar] [CrossRef]
- Scărlătescu, A.-I.; Micheu, M.-M.; Popa-Fotea, N.; Pascal, A.-M.; Mihail, A.-M.; Petre, I.; Deaconu, S.; Vîjîiac, A.; Dorobanțu, M. IL-6, IL-1RA and Resistin as Predictors of Left Ventricular Remodeling and Major Adverse Cardiac Events in Patients with Acute ST Elevation Myocardial Infarction. Diagnostics 2022, 12, 266. [Google Scholar] [CrossRef]
- McGaffin, K.R.; Witham, W.G.; Yester, K.A.; Romano, L.C.; O’Doherty, R.M.; McTiernan, C.F.; O’Donnell, C.P. Cardiac-specific leptin receptor deletion exacerbates ischemic heart failure in mice. Cardiovasc. Res. 2011, 89, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Grzywocz, P.; Mizia-Stec, K.; Wybraniec, M.; Chudek, J. Adipokines and endothelial dysfunction in acute myocardial infarction and the risk of recurrent cardiovascular events. J. Cardiovasc. Med. 2015, 16, 37–44. [Google Scholar] [CrossRef]
- Fei, Q.; Tan, Y.; Yi, M.; Zhao, W.; Zhang, Y. Associations between cardiometabolic phenotypes and levels of TNF-α, CRP, and interleukins in obstructive sleep apnea. Sleep Breath. 2022, 19, 1033–1042. [Google Scholar] [CrossRef]
- Motamedi, V.; Kanefsky, R.; Matsangas, P.; Mithani, S.; Jeromin, A.; Brock, M.-S.; Mysliwiec, V.; Gill, J. Elevated tau and interleukin-6 concentrations in adults with obstructive sleep apnea. Sleep Med. 2018, 43, 71–76. [Google Scholar] [CrossRef]
- Calcaianu, G.; Bresson, D.; Calcaianu, M.; Morisset, B.; El-Nazer, T.; Deodati, C.; Virot, E.; Holtea, D.; Iamandi, C.; Debieuvre, D. The Importance of Apneic Events in Obstructive Sleep Apnea Associated with Acute Coronary Syndrome. Sleep Disord. 2019, 21, 6039147. [Google Scholar] [CrossRef]
- Xie, L.; Zhen, P.; Yu, F.; Yu, X.; Qian, H.; Yang, F.; Tong, J. Effects of sleep apnea hypopnea syndromes on cardiovascular events: A systematic review and meta-analysis. Sleep Breath. 2022, 26, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Besedovsky, L.; Lange, T.; Haack, M. The Sleep-Immune Crosstalk in Health and Disease. Physiol. Rev. 2019, 99, 1325–1380. [Google Scholar] [CrossRef] [PubMed]
- Arias-Mendoza, A.; González-Pacheco, H.; Álvarez-Sangabriel, A.; Gopar-Nieto, R.; Rodríguez-Chávez, L.L.; Araiza-Garaygordobil, D.; Ramírez-Rangel, P.; Martínez, D.S.; Del Carmen Lacy-Niebla, M.; Briseño-De la Cruz, J.L.; et al. Women with Acute Myocardial Infarction: Clinical Characteristics, Treatment, and In-Hospital Outcomes from a Latin American Country. Glob. Heart 2023, 18, 19. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC); American College of Cardiology (ACC); American Heart Association (AHA); et al. Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Kosaraju, A.; Goyal, A.; Grigorova, Y.; Makaryus, A.N. Left Ventricular Ejection Fraction; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Cruz-Aragón, G.; Márquez, M.F.; Cueva-Parra, A.D.; González-Pacheco, H.; Iturralde, P.; Nava, S. Relación del intervalo QT corregido con la escala GRACE en pacientes con infarto de miocardio sin elevación del segmento ST. Arch. Peru. Cardiol. Y Cirugía Cardiovasc. 2022, 3, 132–138. [Google Scholar] [CrossRef]
- Killip, T., 3rd; Kimball, J.T. Treatment of myocardial infarction in a coronary care unit. A two-year experience with 250 patients. Am. J. Cardiol. 1967, 4, 457–464. [Google Scholar] [CrossRef]
- Fernandez-Mendoza, J.; Rodriguez-Muñoz, A.; Vela-Bueno, A.; Olavarrieta-Bernardino, S.; Calhoun, S.-L.; Bixler, E.-O.; Vgontzas, A.-N. The Spanish version of the Insomnia Severity Index: A confirmatory factor analysis. Sleep Med. 2012, 13, 207–210. [Google Scholar] [CrossRef]
- Carpenter, J.S.; Andrykowski, M.A. Psychometric evaluation of the Pittsburgh Sleep Quality Index. J. Psychosom. Res. 1998, 45, 5–13. [Google Scholar] [CrossRef]
- Guerrero-Zúñiga, S.; Gaona-Pineda, E.-B.; Cuevas-Nasu, L.; Torre-Bouscoulet, L.; Reyes-Zúñiga, M.; Shamah-Levy, T.; Perez-Padilla, R. Prevalencia de síntomas de sueño y riesgo de apnea obstructiva del sueño en México [Prevalence of sleep symptoms and risk of obstructive sleep apnea in Mexico]. Salud Publica Mex. 2018, 60, 347–355. [Google Scholar] [CrossRef]
- Duan, X.; Zheng, M.; Zhao, W.; Huang, J.; Lao, L.; Li, H.; Lu, J.; Chen, W.; Liu, X.; Deng, H. Associations of Depression, Anxiety, and Life Events with the Risk of Obstructive Sleep Apnea Evaluated by Berlin Questionnaire. Front. Med. 2022, 9, 799792. [Google Scholar] [CrossRef]
- Sandoval-Rincón, M.; Alcalá-Lozano, R.; Herrera-Jiménez, I.; Jiménez-Genchi, A. Validación de la escala de somnolencia de Epworth en población mexicana [Validation of the Epworth sleepiness scale in Mexican population]. Gac. Médica México 2013, 149, 409–416. [Google Scholar]
- Lok, R.; Zeitzer, J.M. Physiological correlates of the Epworth Sleepiness Scale reveal different dimensions of daytime sleepiness. Sleep Adv. 2021, 2, zpab008. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.-L.; Goldberg, A.-N.; Alt, J.-A.; Mohammed, A.; Ashbrook, L.; Auckley, D.; Ayappa, I.; Bakhtiar, H.; Barrera, J.-E.; Bartley, B.-L.; et al. International Consensus Statement on Obstructive Sleep Apnea. Int. Forum Allergy Rhinol. 2022, 6, 1061–1482. [Google Scholar] [CrossRef] [PubMed]
- Mediano, O.; González Mangado, N.; Montserrat, J.-M.; Alonso-Álvarez, M.-L.; Almendros, I.; Alonso-Fernández, A.; Barbé, F.; Borsini, E.; Caballero-Eraso, C.; Cano-Pumarega, I.; et al. International Consensus Document on Obstructive Sleep Apnea. Arch. Bronconeumol. 2022, 58, 52–68. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Features | |||
|---|---|---|---|
| AMI n = 30 | Control n = 25 | p | |
| Men, n (%) | 25 (83) | 21 (84) | >0.999 |
| Age, years Median (IQR) | 56 (30–61) | 51 (45–57) | 0.069 |
| Diabetes, n (%) | 11 (36.7) | 4 (16) | 0.129 |
| Hypertension, n (%) | 13 (43.3) | 7 (28) | 0.273 |
| Dyslipidemia, n (%) | 6 (20) | 0 (0) | 0.026 |
| Smoking, n (%) | 18 (60) | 1 (4) | <0.001 |
| Overweight, n (%) | 8 (26.7) | 19 (76) | <0.001 |
| Obese, n (%) | 13 (43.3) | 6 (24) | 0.163 |
| WHR Median (IQR) | 0.97 (0.9–1.0) | 1.01 (0.9–1.0) | 0.170 |
| Glucose (mmol/L) Median (IQR) | 6.41 (5.8–8.3) | 5.55 (5.0–6.0) | <0.001 |
| HOMA index Median (IQR) | 4.1 (2.9–10) | 3.7 (2.4–11) | 0.096 |
| Triglycerides (mg/dL) Median (IQR) | 177 (120.8–215.5) | 165 (130–293) | 0.824 |
| Total cholesterol (mg/dL) Median (IQR) | 138 (124.5–175) | 194 (157.5–216.5) | <0.001 |
| HDL (mg/dL) Median (IQR) | 32.95 (28.4–38) | 41.3 (37.2–48.9) | <0.001 |
| LDL (mg/dL) Median (IQR) | 86.8 (68.8–106.5) | 118 (95.2–136.5) | 0.006 |
| Sleep Quality | |||
| Sleep quantity, (hours) Median (IQR) | 6 (4.7–7) | 5 (4.7–8) | 0.241 |
| Global PSQI score Median (IQR) | 10 (5.7–13) | 10 (6–11.5) | 0.707 |
| ESS Median (IQR) | 9 (5.7–14.2) | 10 (6–11.5) | 0.683 |
| Berlin Questionnaire, n (%) | 15 (50) | 7 (28) | 0.016 |
| AHI Median (IQR) | 13.5 (6.7–21) | 17.3 (6.7–28.8) | 0.635 |
| Clinical Features | |||
|---|---|---|---|
| AMI w OSA n = 15 | AMI w/o OSA n = 15 | p | |
| Sex, men (%) | 13 (86.7) | 12 (80) | >0.999 |
| Age (years) Median (IQR) | 56 (53–62) | 54 (45 -58) | 0.183 |
| Diabetes, n (%) | 8 (61.5) | 3 (20) | 0.051 |
| Hypertension, n (%) | 8 (53.3) | 5 (33.3) | 0.462 |
| Dyslipidemia, n (%) | 3 (20) | 3 (20) | >0.999 |
| Smoking, n (%) | 8 (53.3) | 10 (66.7) | 0.710 |
| Overweight, n (%) | 3 (20) | 5 (33.3) | 0.682 |
| Obese, n (%) | 8 (53.3) | 5 (33.3) | 0.462 |
| WHR Median (IQR) | 0.98 (0.96–1.0) | 0.96 (0.93–0.99) | 0.227 |
| Glucose (mmol/L) Median (IQR) | 7.4 (5.9–8.5) | 6.2 (5.9–7.0) | 0.361 |
| HOMA index Median (IQR) | 8.8 (3–11) | 4 (2.8–7) | 0.244 |
| Triglycerides (mg/dL) Median (IQR) | 179 (114–215) | 176 (122–217) | 0.713 |
| Total cholesterol (mg/dL) Median (IQR) | 134 (123–176) | 150 (125–179) | 0.418 |
| HDL (mg/dL) Median (IQR) | 33.4 (28.3–37.6) | 32 (28.4–39.1) | 0.829 |
| LDL (mg/dL) Median (IQR) | 86.6 (65.2–106) | 91.9 (76.3–123) | 0.486 |
| CK (U/L) Median (IQR) | 1430 (301–5432) | 377 (125–2194) | 0.036 |
| CK-MB (ng/mL) median (IQR) | 64.6 (15.1–300) | 9.7 (4.3–148) | 0.044 |
| Pro-BNP (pg/mL) Median (IQR) | 247 (115–854) | 351 (170–768) | 0.653 |
| cTnT (pg/mL) Median (IQR) | 2298 (382–17854) | 356 (142–1021) | 0.041 |
| Type of heart attack (STEMI), n (%) | 13 (86.7) | 9 (60) | 0.215 |
| GRACE Median (IQR) | 101 (95–115) | 95 (77–109) | 0.221 |
| % LVEF Median (IQR) | 54 (38–57) | 54 (45–56) | 0.628 |
| K-K [I], n (%) | 12 (80) | 13 (86.7) | >0.999 |
| Basic therapy | |||
| Lipid-lowering agents, n (%) | 2 (13.3) | 0 (0) | 0.483 |
| Insulin, n (%) | 1 (6.7) | 1 (6.7) | >0.999 |
| Metformin, n (%) | 4 (26.7) | 3 (20) | >0.999 |
| Antihypertensives, n (%) | 6 (40) | 3 (20) | 0.427 |
| ASA, n (%) | 0 (0) | 2 (13.3) | 0.483 |
| Emergency therapy | |||
| DAPT, n (%) | 9 (45) | 9 (45) | >0.999 |
| Beta-blockers, n (%) | 4 (26.7) | 3 (20) | >0.009 |
| ACEi/ARA II, n (%) | 5 (33.3) | 4 (26.7) | >0.999 |
| Anticoagulant, n (%) | 6 (40) | 5 (33.3) | >0.999 |
| Statin, n (%) | 11 (73.3) | 10 (66.7) | >0.999 |
| Sleep Quality | ||||||
|---|---|---|---|---|---|---|
| AMI w OSA n = 15 | Control w OSA n = 13 | p | AMI w/o OSA n = 15 | Control w/o OSA n = 12 | p | |
| Sleep quality Median (IQR) | 1 (1–2) | 1 (1–2) | 0.451 | 1 (1–2) | 1 (1–1.75) | 0.951 |
| Sleep latency Median (IQR) | 1 (0–2) | 1 (0–2.5) | 0.631 | 2 (0–3) | 1.5 (0.2–2) | 0.299 |
| Sleep duration Median (IQR) | 2 (0–2) | 2 (2–3) | 0.083 | 2 (1–3) | 2 (2–3) | 0.451 |
| Sleep efficiency Median (IQR) | 2 (0–3) | 1 (0–2) | 0.258 | 2 (0–3) | 1 (0–2) | 0.568 |
| Sleep disturbance Median (IQR) | 2 (1–2) | 2 (1–2) | 0.258 | 2 (1–2) | 1.5 (1–2) | 0.625 |
| Sleep medication Median (IQR) | 0 (0–0) | 0 (0–0) | 0.484 | 0 (0–0) | 0 (0–0) | 0.487 |
| Daily dysfunction Median (IQR) | 1 (0–2) | 2 (0–3) | 0.752 | 2 (0–3) | 1 (1–2.7) | 0.971 |
| Global PSQI score Median (IQR) | 10 (4–13) | 9 (6–12) | 0.936 | 10 (7–13) | 10 (2.2–10.5) | 0.602 |
| ESS Median (IQR) | 13 (6–17) | 12 (6.5–14) | 0.516 | 7 (4–11) | 9 (4–12.5) | 0.636 |
| Berlin Questionnaire, n (%) | 9 (64.3) | 4 (30.8) | 0.128 | 6 (40) | 4 (33.3) | >0.999 |
| AMI w OSA n = 15 | Control w OSA n = 13 | p | AMI w/o OSA n = 15 | Control w/o OSA n = 12 | p | |
|---|---|---|---|---|---|---|
| AHI, events per h Median (IQR) | 20.9 (15.4–31) | 28.8 (19.2–47.9) | 0.115 | 6.9 (4.5–11.6) | 6.7 (4.3–8.0) | 0.493 |
| Total number of obstructive events Median (IQR) | 57 (30–90) | 90 (59–178) | 0.032 | 14 (5–31) | 5.5 (4–17.7) | 0.076 |
| Number of central apneas Median (IQR) | 1 (0–3) | 0 (0–0) | 0.016 | 0 (0–0) | 0 (0–0.7) | 0.932 |
| Number of hypopneas Median (IQR) | 74 (53–107) | 65 (54–103.5) | 0.973 | 33 (29–51) | 30.5 (14.7–42.2) | 0.304 |
| Total respiratory events Median (IQR) | 246 (118–188) | 185 (140–262) | 0.204 | 48 (37–89) | 39 (25–55) | 0.203 |
| OAI Median (IQR) | 8.6 (4.8–17.5) | 18.2 (8.8–30.5) | 0.047 | 1.9 (0.7–3.9) | 0.9 (0.5–2.8) | 0.231 |
| CAI Median (IQR) | 0.1 (0–0.4) | 0 (0–0) | 0.014 | 0 (0–0) | 0 (0–0.07) | 0.932 |
| Lowest SpO2 during sleep Median (IQR) | 73 (68–77) | 69 (65–74.5) | 0.221 | 80 (75–84) | 80 (76.8–81.7) | 0.691 |
| ODI > 4%, per h Median (IQR) | 45 (25.6–48.5) | 43.6 (28.2–58) | 0.488 | 18.1 (16.3–26.5) | 19.4 (11.8–26.9) | 0.782 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vega-Jasso, A.L.; Amezcua-Guerra, L.M.; González-Pacheco, H.; Sandoval-Zárate, J.; González-Díaz, C.A.; Escobar-Alvarado, J.; Manzano-Luna, J.D.; Brianza-Padilla, M. Adipokines and Inflammatory Markers in Acute Myocardial Infarction Patients with and without Obstructive Sleep Apnea: A Comparative Analysis. Int. J. Mol. Sci. 2023, 24, 14674. https://doi.org/10.3390/ijms241914674
Vega-Jasso AL, Amezcua-Guerra LM, González-Pacheco H, Sandoval-Zárate J, González-Díaz CA, Escobar-Alvarado J, Manzano-Luna JD, Brianza-Padilla M. Adipokines and Inflammatory Markers in Acute Myocardial Infarction Patients with and without Obstructive Sleep Apnea: A Comparative Analysis. International Journal of Molecular Sciences. 2023; 24(19):14674. https://doi.org/10.3390/ijms241914674
Chicago/Turabian StyleVega-Jasso, Ana L., Luis M. Amezcua-Guerra, Héctor González-Pacheco, Julio Sandoval-Zárate, César A. González-Díaz, Jennifer Escobar-Alvarado, Jennifer D. Manzano-Luna, and Malinalli Brianza-Padilla. 2023. "Adipokines and Inflammatory Markers in Acute Myocardial Infarction Patients with and without Obstructive Sleep Apnea: A Comparative Analysis" International Journal of Molecular Sciences 24, no. 19: 14674. https://doi.org/10.3390/ijms241914674