
Utility of High-Sensitivity Modified Glasgow Prognostic Score in Cancer Prognosis: A Systemic Review and Meta-Analysis
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Database Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
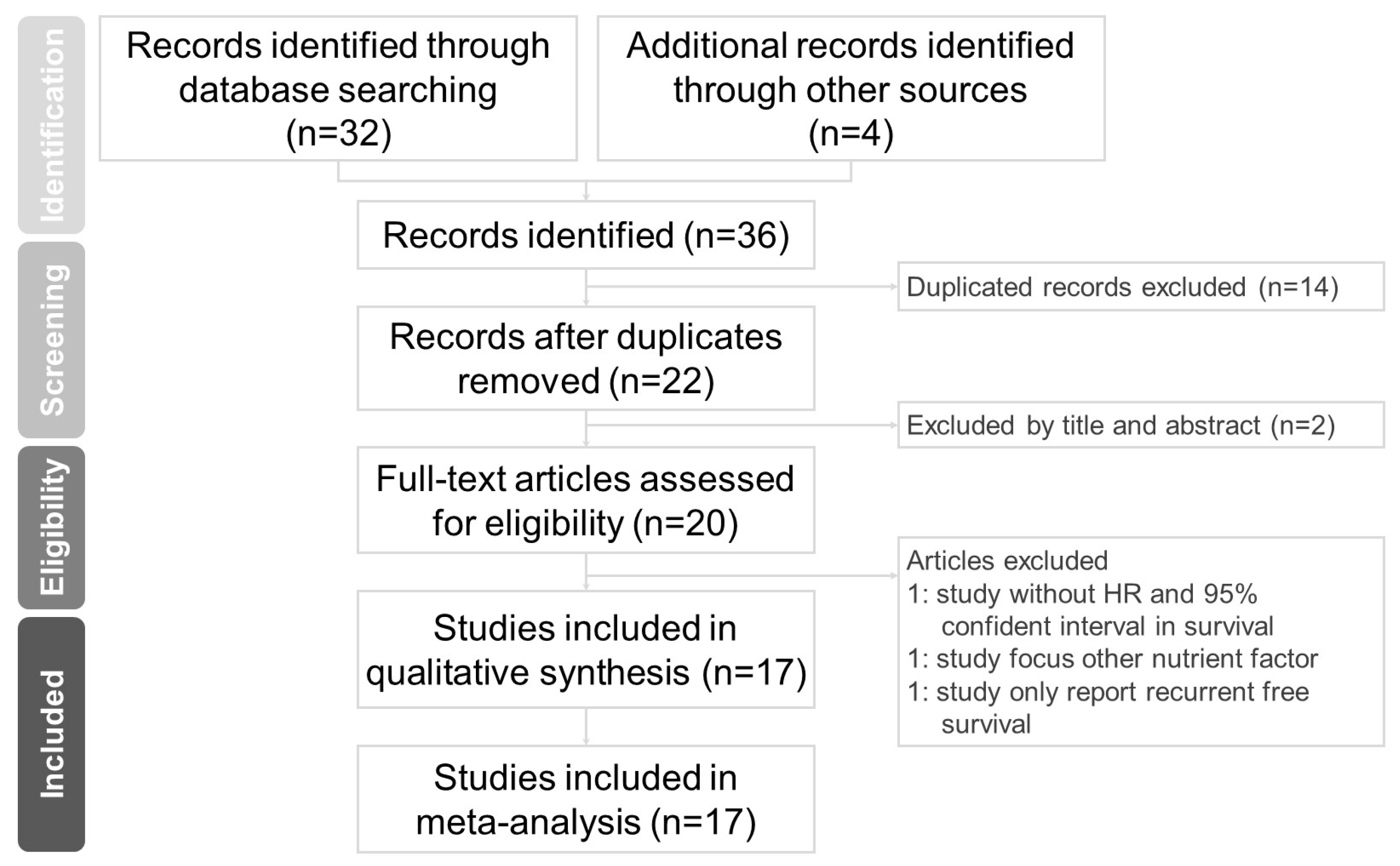
3.1. Literature Search
3.2. Study Characteristics
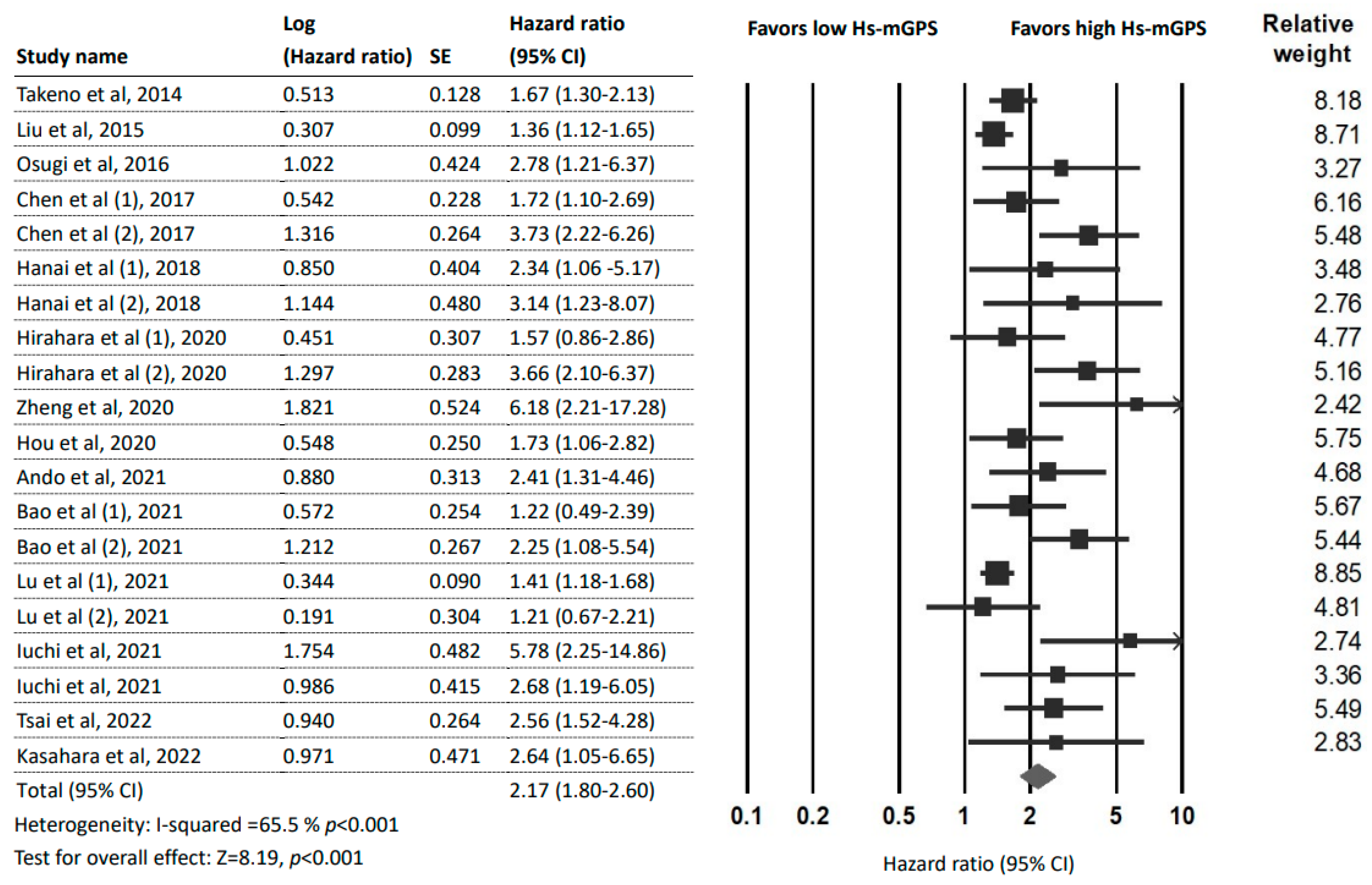
3.3. Prognostic Effect of the HS-mGPS for OS
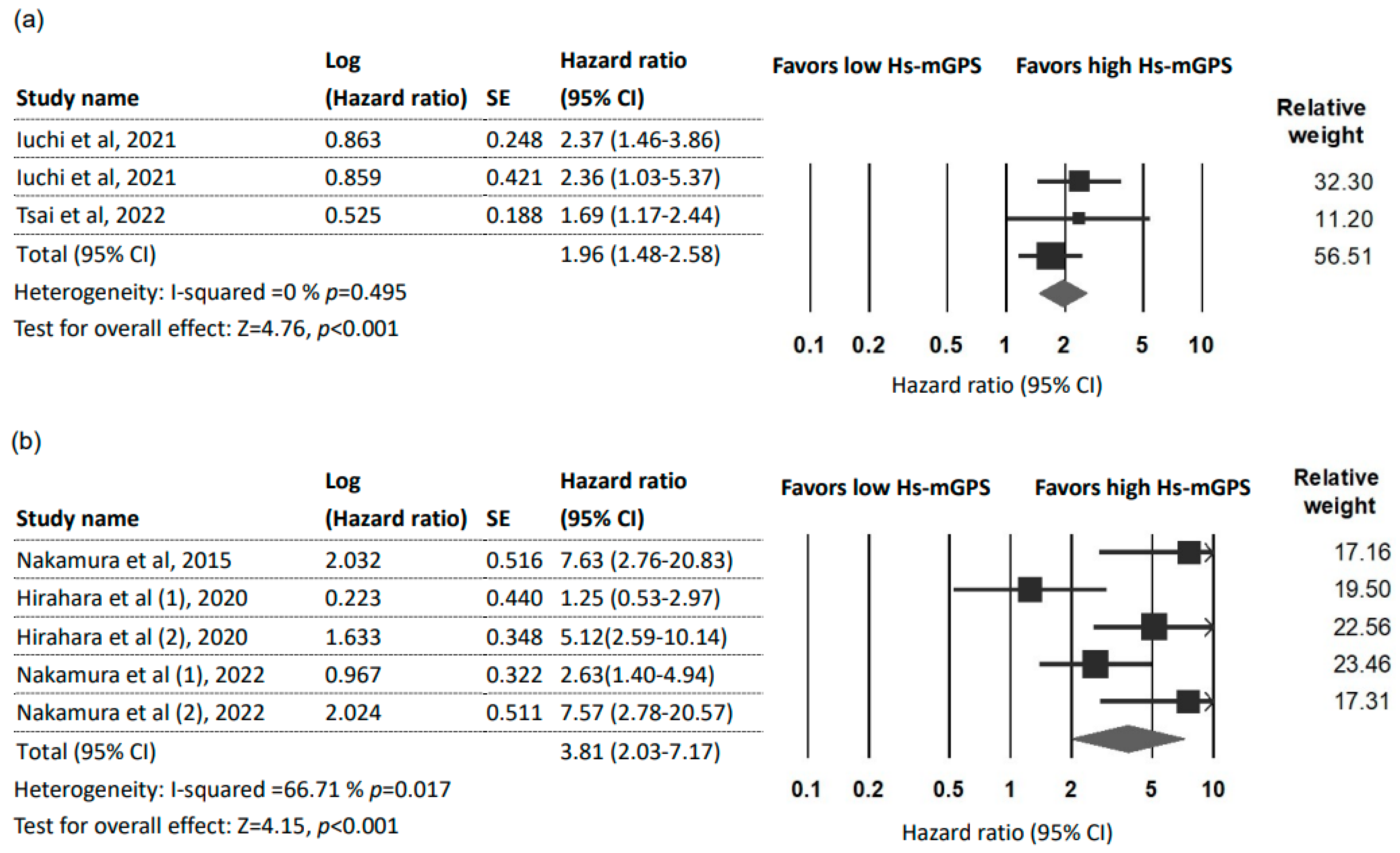
3.4. Prognostic Effect of the HS-mGPS on DFS
3.5. Prognostic Effect of the HS-mGPS on DSS
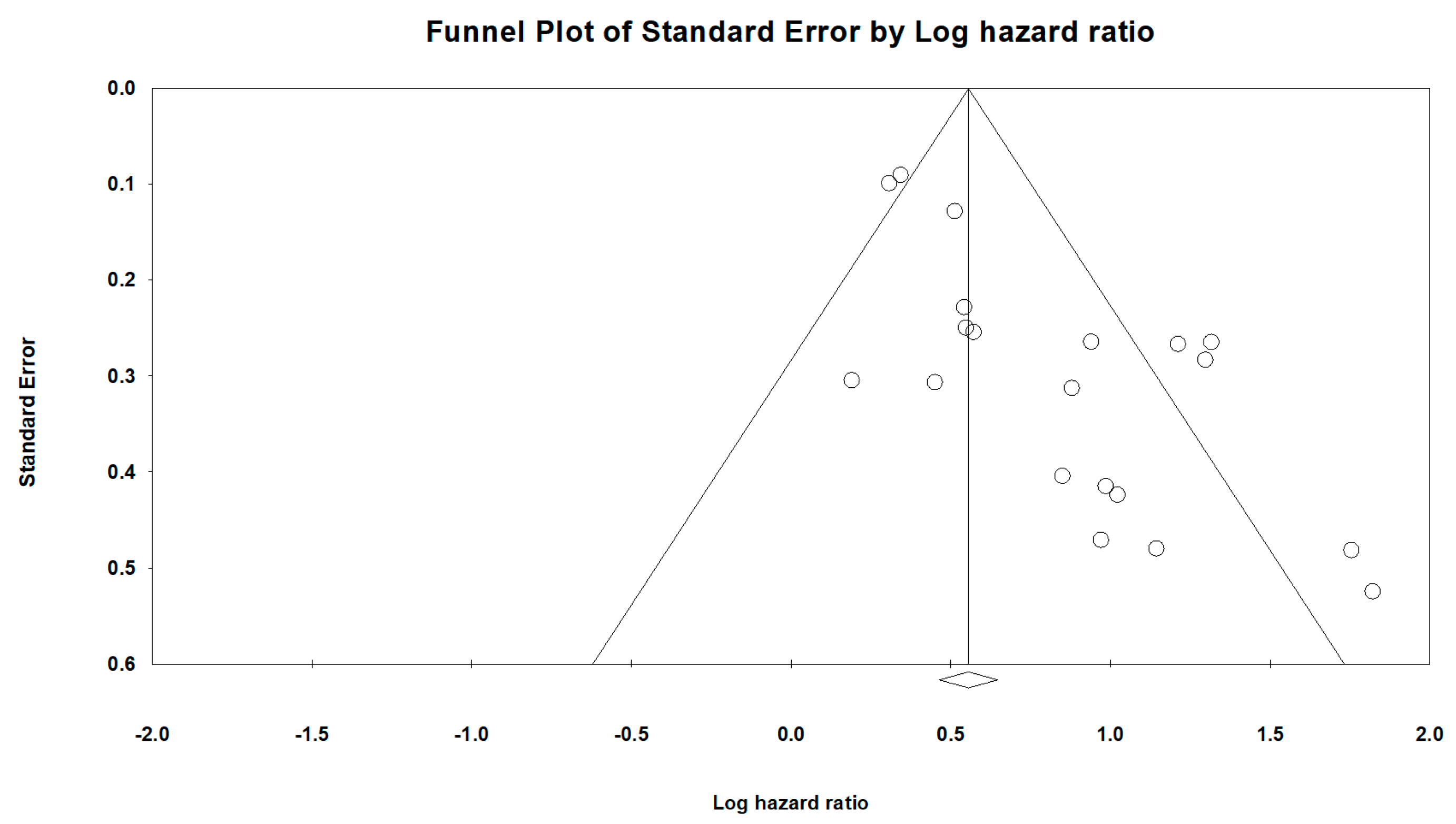
3.6. Publication Bias and Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef]
- Erdmann, F.; Frederiksen, L.E.; Bonaventure, A.; Mader, L.; Hasle, H.; Robison, L.L.; Winther, J.F. Childhood cancer: Survival, treatment modalities, late effects and improvements over time. Cancer Epidemiol. 2021, 71 Pt B, 101733. [Google Scholar] [CrossRef]
- Mody, M.D.; Rocco, J.W.; Yom, S.S.; Haddad, R.I.; Saba, N.F. Head and neck cancer. Lancet 2021, 398, 2289–2299. [Google Scholar] [CrossRef]
- Schiller, J.T.; Lowy, D.R. An Introduction to Virus Infections and Human Cancer. Recent Results Cancer Res. 2021, 217, 1–11. [Google Scholar]
- Luan, C.W.; Yang, H.Y.; Tsai, Y.T.; Hsieh, M.C.; Chou, H.H.; Chen, K.S. Prognostic Value of C-Reactive Protein-to-Albumin Ratio in Head and Neck Cancer: A Meta-Analysis. Diagnostics 2021, 11, 403. [Google Scholar] [CrossRef]
- Luan, C.W.; Tsai, Y.T.; Yang, H.Y.; Chen, K.Y.; Chen, P.H.; Chou, H.H. Pretreatment prognostic nutritional index as a prognostic marker in head and neck cancer: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 17117. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.T.; Fang, K.H.; Hsu, C.M.; Lai, C.-H.; Chang, S.-W.; Huang, E.I.; Tsai, M.-S.; Chang, G.-H.; Luan, C.-W. Prognostic Role of High-Sensitivity Modified Glasgow Prognostic Score for Patients With Operated Oral Cavity Cancer: A Retrospective Study. Front. Oncol. 2022, 12, 825967. [Google Scholar] [CrossRef]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.Y.; Xie, H.L.; Ruan, G.T.; Zhang, Q.; Ge, Y.-Z.; Liu, X.-Y.; Tang, M.; Song, M.-M.; Lin, S.-Q.; Yang, M.; et al. Lymphocyte to C-reactive protein ratio could better predict the prognosis of patients with stage IV cancer. BMC Cancer 2022, 22, 1080. [Google Scholar] [CrossRef] [PubMed]
- Douglas, E.; McMillan, D.C. Towards a simple objective framework for the investigation and treatment of cancer cachexia: The Glasgow Prognostic Score. Cancer Treat. Rev. 2014, 40, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Comparison of an inflammation-based prognostic score (GPS) with performance status (ECOG) in patients receiving platinum-based chemotherapy for inoperable non-small-cell lung cancer. Br. J. Cancer 2004, 90, 1704–1706. [Google Scholar] [CrossRef]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef]
- Chen, P.; Fang, M.; Wan, Q.; Zhang, X.; Song, T.; Wu, S. High-sensitivity modified Glasgow prognostic score (HS-mGPS) Is superior to the mGPS in esophageal cancer patients treated with chemoradiotherapy. Oncotarget 2017, 8, 99861–99870. [Google Scholar] [CrossRef] [PubMed]
- Osugi, J.; Muto, S.; Matsumura, Y.; Higuchi, M.; Suzuki, H.; Gotoh, M. Prognostic impact of the high-sensitivity modified Glasgow prognostic score in patients with resectable non-small cell lung cancer. J. Cancer Res. Ther. 2016, 12, 945–951. [Google Scholar] [PubMed]
- Takeno, S.; Hashimoto, T.; Shibata, R.; Maki, K.; Shiwaku, H.; Yamana, I.; Yamashita, R.; Yamashita, Y. The high-sensitivity modified Glasgow prognostic score is superior to the modified Glasgow prognostic score as a prognostic predictor in patients with resectable gastric cancer. Oncology 2014, 87, 205–214. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Nakamura, T.; Matsumine, A.; Asanuma, K.; Matsubara, T.; Sudo, A. The value of the high-sensitivity modified Glasgow prognostic score in predicting the survival of patients with a soft-tissue sarcoma. Bone Jt. J. 2015, 97-B, 847–852. [Google Scholar] [CrossRef]
- Hanai, N.; Sawabe, M.; Kimura, T.; Suzuki, H.; Ozawa, T.; Hirakawa, H.; Fukuda, Y.; Hasegawa, Y. The high-sensitivity modified Glasgow prognostic score is superior to the modified Glasgow prognostic score as a prognostic predictor for head and neck cancer. Oncotarget 2018, 9, 37008–37016. [Google Scholar] [CrossRef]
- Hou, T.; Guo, T.; Nie, R.; Hong, D.; Zhou, Z.; Zhang, X.; Liang, Y. The prognostic role of the preoperative systemic immune-inflammation index and high-sensitivity modified Glasgow prognostic score in patients after radical operation for soft tissue sarcoma. Eur. J. Surg. Oncol. 2020, 46, 1496–1502. [Google Scholar] [CrossRef]
- Zheng, C.; Liu, S.; Feng, J.; Zhao, X. Prognostic Value of Inflammation Biomarkers for Survival of Patients with Neuroblastoma. Cancer Manag. Res. 2020, 12, 2415–2425. [Google Scholar] [CrossRef]
- Ando, K.; Sakamoto, S.; Saito, S.; Maimaiti, M.; Imamura, Y.; Sazuka, T.; Sato, N.; Komiya, A.; Anzai, N.; Ichikawa, T. Prognostic Value of High-Sensitivity Modified Glasgow Prognostic Score in Castration-Resistant Prostate Cancer Patients Who Received Docetaxel. Cancers 2021, 13, 773. [Google Scholar] [CrossRef]
- Iuchi, H.; Ohori, J.; Ando, Y.; Tokushige, T.; Haraguchi, M.; Yamashita, M. Utility of the High-Sensitivity Modified Glasgow Prognostic Scores for Oropharyngeal Carcinoma. OTO Open 2021, 5, 2473974X211042302. [Google Scholar] [CrossRef]
- Iuchi, H.; Ohori, J.; Matsuzaki, H.; Kiyama, S.; Yamashita, M. Utility of the Modified and High-Sensitivity Modified Glasgow Prognostic Scores for Hypopharyngeal Squamous Cell Carcinoma. OTO Open 2021, 5, 2473974X211067423. [Google Scholar] [CrossRef]
- Lu, L.H.; Wei, W.; Li, S.H.; Zhang, Y.F.; Guo, R.P. The lymphocyte-C-reactive protein ratio as the optimal inflammation-based score in patients with hepatocellular carcinoma underwent TACE. Aging 2021, 13, 5358–5368. [Google Scholar] [CrossRef]
- Kasahara, K.; Enomoto, M.; Udo, R.; Tago, T.; Mazaki, J.; Ishizaki, T.; Yamada, T.; Nagakawa, Y.; Katsumata, K.; Tsuchida, A. Prognostic value of preoperative high-sensitivity modified Glasgow prognostic score in advanced colon cancer: A retrospective observational study. BMC Cancer 2022, 22, 20. [Google Scholar] [CrossRef]
- Liu, X.; Sun, X.; Liu, J.; Kong, P.; Chen, S.; Zhan, Y.; Xu, D. Preoperative C-Reactive Protein/Albumin Ratio Predicts Prognosis of Patients after Curative Resection for Gastric Cancer. Transl. Oncol. 2015, 8, 339–345. [Google Scholar] [CrossRef]
- Hirahara, N.; Matsubara, T.; Kaji, S.; Kawabata, Y.; Hyakudomi, R.; Yamamoto, T.; Uchida, Y.; Ishitobi, K.; Takai, K.; Tajima, Y. Glasgow prognostic score is a better predictor of the long-term survival in patients with gastric cancer, compared to the modified Glasgow prognostic score or high-sensitivity modified Glasgow prognostic score. Oncotarget 2020, 11, 4169–4177. [Google Scholar] [CrossRef]
- Bao, Y.; Yang, J.; Duan, Y.; Chen, Y.; Chen, W.; Sun, D. The C-reactive protein to albumin ratio is an excellent prognostic predictor for gallbladder cancer. Biosci. Trends 2021, 14, 428–435. [Google Scholar] [CrossRef]
- Nakamura, T.; Asanuma, K.; Hagi, T.; Sudo, A. Modified Glasgow Prognostic Score is Better for Predicting Oncological Outcome in Patients with Soft Tissue Sarcoma, Compared to High-Sensitivity Modified Glasgow Prognostic Score. J. Inflamm. Res. 2022, 15, 3891–3899. [Google Scholar] [CrossRef]
- Dolan, R.D.; Lim, J.; McSorley, S.T.; Horgan, P.G.; McMillan, D.C. The role of the systemic inflammatory response in predicting outcomes in patients with operable cancer: Systematic review and meta-analysis. Sci. Rep. 2017, 7, 16717. [Google Scholar] [CrossRef]
- Li, C.; Tian, W.; Zhao, F.; Li, M.; Ye, Q.; Wei, Y.; Li, T.; Xie, K. Systemic immune-inflammation index, SII, for prognosis of elderly patients with newly diagnosed tumors. Oncotarget 2018, 9, 35293–35299. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, F.; Wang, Y. Evidence of the Prognostic Value of Pretreatment Systemic Inflammation Response Index in Cancer Patients: A Pooled Analysis of 19 Cohort Studies. Dis. Markers 2020, 2020, 8854267. [Google Scholar] [CrossRef]
- Lorton, C.M.; Higgins, L.; O’Donoghue, N.; Donohoe, C.; O’Connell, J.; Mockler, D.; Reynolds, J.V.; Walsh, D.; Lysaght, J. C-Reactive Protein and C-Reactive Protein-Based Scores to Predict Survival in Esophageal and Junctional Adenocarcinoma: Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2022, 29, 1853–1865. [Google Scholar] [CrossRef]
- Proctor, M.J.; Horgan, P.G.; Talwar, D.; Fletcher, C.D.; Morrison, D.S.; McMillan, D.C. Optimization of the systemic inflammation-based Glasgow prognostic score: A Glasgow Inflammation Outcome Study. Cancer 2013, 119, 2325–2332. [Google Scholar] [CrossRef]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef]
- Slaats, J.; Ten Oever, J.; van de Veerdonk, F.L.; Netea, M.G. IL-1beta/IL-6/CRP and IL-18/ferritin: Distinct Inflammatory Programs in Infections. PLoS Pathog. 2016, 12, e1005973. [Google Scholar] [CrossRef]
- Whiteside, T.L. The tumor microenvironment and its role in promoting tumor growth. Oncogene 2008, 27, 5904–5912. [Google Scholar] [CrossRef]
- Nakamura, T.; Matsumine, A.; Matsubara, T.; Asanuma, K.; Uchida, A.; Sudo, A. Clinical significance of pretreatment serum C-reactive protein level in soft tissue sarcoma. Cancer 2012, 118, 1055–1061. [Google Scholar] [CrossRef]
- Gagnon, B.; Abrahamowicz, M.; Xiao, Y.; Beauchamp, M.-E.; Macdonald, N.; Kasymjanova, G.; Kreisman, H.; Small, D. Flexible modeling improves assessment of prognostic value of C-reactive protein in advanced non-small cell lung cancer. Br. J. Cancer 2010, 102, 1113–1122. [Google Scholar] [CrossRef]
- Tuomisto, K.; Jousilahti, P.; Sundvall, J.; Pajunen, P.; Salomaa, V. C-reactive protein, interleukin-6 and tumor necrosis factor alpha as predictors of incident coronary and cardiovascular events and total mortality. A population-based, prospective study. Thromb. Haemost. 2006, 95, 511–518. [Google Scholar] [CrossRef]
- Maxwell, M.B. Cancer, hypoalbuminemia, and nutrition. Cancer Nurs. 1981, 4, 451–458. [Google Scholar] [CrossRef]
- Kose, E.; Wakabayashi, H.; Yasuno, N. Polypharmacy and Malnutrition Management of Elderly Perioperative Patients with Cancer: A Systematic Review. Nutrients 2021, 13, 1961. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Omitted Study | Year | Country | Study Period | Study Design | Survival Analysis | Sample Size | Cancer Type | Cancer Stage | Treatment | Outcome | Median Follow-Up (Months) | NOS Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Takeno et al. [16] | 2014 | Japan | 1995–2006 | retrospective | Multivariable | 494 | Gastric cancer | I–IV * (7th UICC) | OP ± adjuvant therapy | OS | NR | 8 |
| Nakamura et al. [21] | 2015 | Japan | 2001–2012 | retrospective | Multivariable | 139 | Soft tissue sarcoma | Grade 1–3 (FNCLCC) | OP/RT/CT | DSS | 60 | 8 |
| Liu et al. [30] | 2015 | China | 2005–2010 | retrospective | Univariable | 455 | Gastric cancer | I–III | D2 gastrectomy with R0 resection | OS | 25 | 7 |
| Osugi et al. [15] | 2016 | Japan | 2005–2009 | retrospective | Multivariable | 327 | Non-small cell lung cancer | I–III * (7th UICC) | OP | OS | 65 | 9 |
| Chen et al. [14] | 2017 | China | 2011–2014 | retrospective | Multivariable | 163 | Esophageal cancer | II–Iva (6th AJCC) | CCRT | OS | NR | 7 |
| Hanai et al. [22] | 2018 | Japan | 2012–2013 | retrospective | Multivariable | 129 | Head and neck cancer | I–IV (7th UICC) | OP/CCRT | OS | 43.6 | 8 |
| Hirahara et al. [31] | 2020 | Japan | 2010–2017 | retrospective | Univariable | 434 | Gastric cancer | I–IV * (4th JGCTG) | OP | OS/DSS | NR | 9 |
| Zheng et al. [24] | 2020 | China | 2008–2016 | retrospective | Multivariable | 70 | Neuroblastoma | 1–4 (INSS) | OP ± adjuvant therapy/CT | OS | 53.1 | 9 |
| Hou et al. [23] | 2020 | China | 2000–2016 | retrospective | Multivariable | 454 | Soft tissue sarcoma | I–III (AJCC), Grade 1–3 (FNCLCC) | OP/RT/CT | OS | 94.8 | 9 |
| Ando et al. [25] | 2021 | Japan | 2005–2019 | retrospective | Multivariable | 131 | Castration-resistant prostate cancer | IV | ADT plus docetaxel | OS/PFS | 21.1 | 8 |
| Bao et al. [32] | 2021 | China | 2010–2017 | retrospective | Multivariable | 144 | Gallbladder cancer | I–IV * (8th AJCC) | OP | OS | NR | 8 |
| Lu et al. [28] | 2021 | China | 2006–2014 | retrospective | Multivariable | 1625 | Hepatocellular carcinoma | ABC (BCLC-C) | TACE | OS | NR | 7 |
| Iuchi et al. [26] | 2021 | Japan | 2009–2020 | retrospective | Multivariable | 106 | Oropharyngeal cancer | I–IV * (8th AJCC) | OP/CCRT | OS/DFS | 42 | 8 |
| Iuchi et al. [27] | 2021 | Japan | 2007–2019 | retrospective | Multivariable | 115 | Hypopharyngeal cancer | II–IV * (8th AJCC) | OP/CCRT | OS/DFS | 62 | 8 |
| Nakamura et al. [33] | 2022 | Japan | 2002–2018 | retrospective | Univariable | 144 | Soft tissue sarcoma | Grade 1–3 (FNCLCC) | OP | DSS | 76 | 9 |
| Tsai et al. [7] | 2022 | Taiwan | 2008–2017 | retrospective | Multivariable | 303 | Oral squamous cell carcinoma | I–IV * (8th AJCC) | OP ± adjuvant therapy | OS/DFS | 40.9 | 9 |
| Kasahara et al. [29] | 2022 | Japan | 2000–2015 | retrospective | Multivariable | 595 | Colorectal cancer | II–IV * | OP ± adjuvant therapy | OS | NR | 7 |
| Subgroup | No. of Datasets (Patients) | HR (95% CI) | p Value | Heterogeneity Test | |
|---|---|---|---|---|---|
| I2 % | p Value | ||||
| Total | 20 (5545) | 2.17 (1.80–2.60) | <0.001 | 65.5 | <0.01 |
| Tumor site | |||||
| Gastrointestinal cancer | 11 (4073) | 1.90 (1.53–2.35) | <0.001 | 70.14 | <0.01 |
| Gastric cancer | 4 (1383) | 1.79 (1.28–2.49) | =0.001 | 73.41 | 0.01 |
| Esophageal cancer | 2 (163) | 2.50 (1.17–5.34) | 0.018 | 79.64 | 0.03 |
| Hepatocellular carcinoma | 2 (1625) | 1.39 (1.18–1.65) | <0.001 | 0 | 0.63 |
| Gallbladder cancer | 2 (144) | 2.43 (1.30–4.55) | 0.006 | 66.86 | 0.08 |
| Colorectal cancer | 1 (595) | 2.64 (1.05–6.64) | 0.039 | ||
| Head and neck cancer | 5 (653) | 2.88 (2.07–4.01) | <0.001 | 0 | 0.62 |
| Oropharyngeal cancer | 1 (106) | 5.78 (2.25–14.85) | <0.001 | ||
| Hypopharyngeal cancer | 1 (115) | 2.68 (1.19–6.04) | 0.017 | ||
| Oral cancer | 1 (303) | 2.56 (1.53–4.30) | <0.001 | ||
| Mixed | 2 (129) | 2.64(1.44–4.85) | 0.002 | 0 | 0.64 |
| Soft tissue sarcoma | 2 (524) | 2.19 (1.41–3.40) | <0.001 | 79.19 | 0.03 |
| Lung cancer | 1 (327) | 2.78 (1.21–6.38) | 0.016 | ||
| Prostate cancer | 1 (131) | 2.41 (1.31–4.45) | 0.005 | ||
| Region | |||||
| China | 9 (2911) | 1.92 (1.48–2.48) | <0.001 | 73.74 | <0.01 |
| Japan | 10 (2331) | 2.43 (1.88–3.15) | <0.001 | 37.21 | 0.11 |
| Taiwan | 1 (301) | 2.56 (1.53–4.30) | <0.001 | ||
| Sample size | |||||
| <165 | 10 (858) | 2.75 (2.12–3.56) | <0.001 | 36.15 | 0.12 |
| ≥165 | 10 (4687) | 1.74 (1.44–2.10) | <0.001 | 55.08 | 0.02 |
| Cutoff value of HS-mGPS | |||||
| 2 | 6 (2822) | 2.82 (1.95–4.07) | <0.001 | 50.77 | 0.07 |
| 1 | 5 (2495) | 1.51 (1.30–1.75) | <0.001 | 0 | 0.64 |
| ≥1 | 9 (2723) | 2.20 (1.66–2.92) | <0.001 | 65.76 | 0.01 |
| Analysis method | |||||
| Multivariable | 17 (4656) | 2.24 (1.83–2.75) | <0.001 | 60.83 | <0.01 |
| Univariable | 3 (889) | 1.92(1.06–3.50) | =0.032 | 81.67 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.-H.; Tsai, Y.-T.; Chen, K.-Y.; Yap, W.-K.; Luan, C.-W. Utility of High-Sensitivity Modified Glasgow Prognostic Score in Cancer Prognosis: A Systemic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 1318. https://doi.org/10.3390/ijms24021318
Wu T-H, Tsai Y-T, Chen K-Y, Yap W-K, Luan C-W. Utility of High-Sensitivity Modified Glasgow Prognostic Score in Cancer Prognosis: A Systemic Review and Meta-Analysis. International Journal of Molecular Sciences. 2023; 24(2):1318. https://doi.org/10.3390/ijms24021318
Chicago/Turabian StyleWu, Tsung-Hsien, Yao-Te Tsai, Kuan-Yin Chen, Wing-Keen Yap, and Chih-Wei Luan. 2023. "Utility of High-Sensitivity Modified Glasgow Prognostic Score in Cancer Prognosis: A Systemic Review and Meta-Analysis" International Journal of Molecular Sciences 24, no. 2: 1318. https://doi.org/10.3390/ijms24021318
APA StyleWu, T.-H., Tsai, Y.-T., Chen, K.-Y., Yap, W.-K., & Luan, C.-W. (2023). Utility of High-Sensitivity Modified Glasgow Prognostic Score in Cancer Prognosis: A Systemic Review and Meta-Analysis. International Journal of Molecular Sciences, 24(2), 1318. https://doi.org/10.3390/ijms24021318