

The Clinical and Molecular Profile of Lung Cancer Patients Harboring the TP53 R337H Germline Variant in a Brazilian Cancer Center: The Possible Mechanism of Carcinogenesis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Demographic, Clinical Features, and Molecular Profile
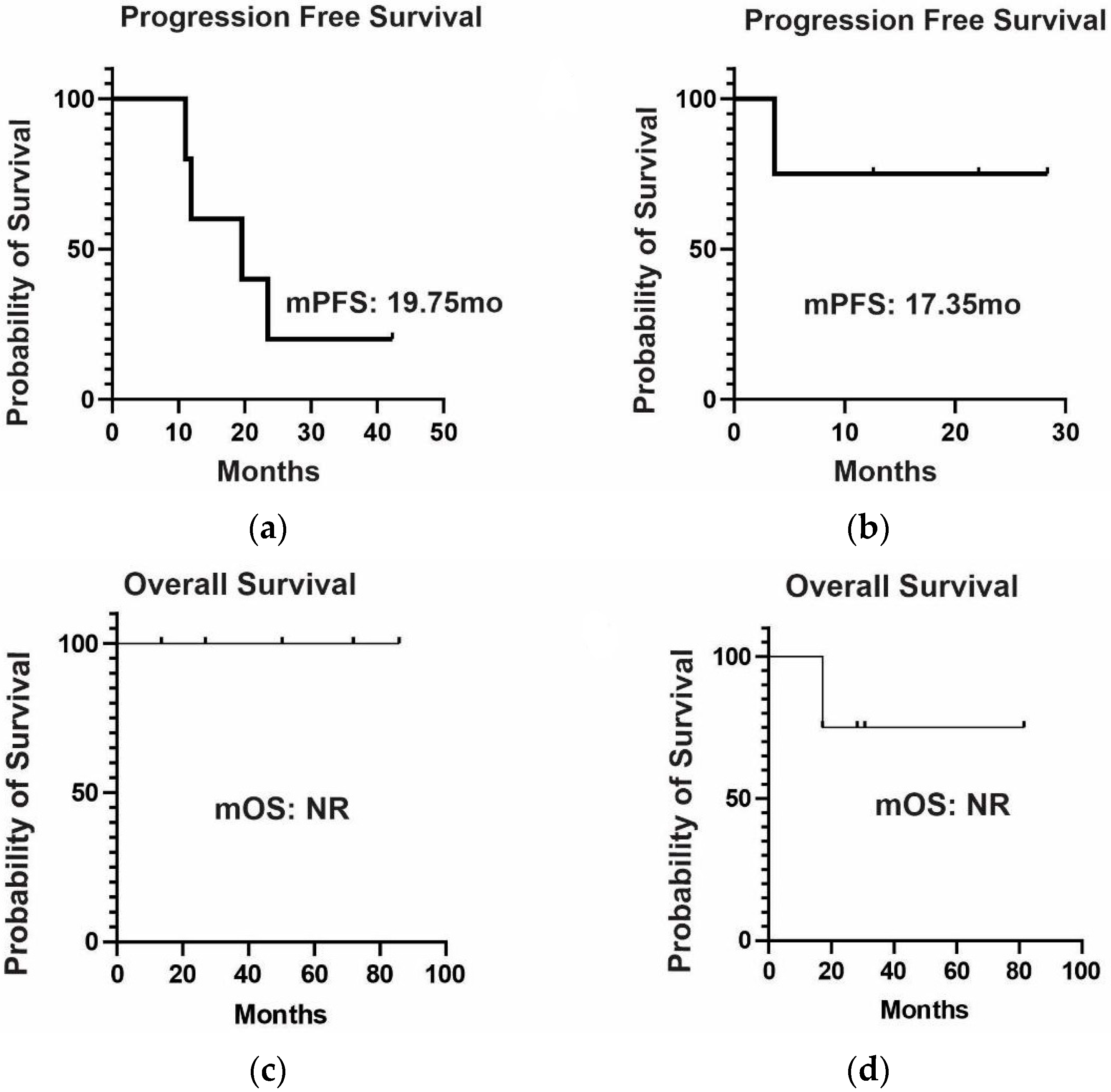
2.2. Clinical Outcomes
2.3. PM2.5 Measurements
3. Discussion
4. Materials and Methods
4.1. Demographic, Clinical, and Genomic Information
4.2. Clinical Outcomes
4.3. Measurement of Pollution Level
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- American Cancer Society. Lung Cancer. 2022. Available online: https://www.cancer.org/cancer/lung-cancer/about/keystatistics.html (accessed on 16 January 2023).
- Cancer INd. Estatísticas de Câncer: INCA. 2022. Available online: https://www.gov.br/inca/pt-br/assuntos/cancer/numeros (accessed on 16 January 2023).
- Cancer Facts & Figures. 2020. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2020.html. (accessed on 16 January 2023).
- Loomis, D.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Baan, R.; Mattock, H.; Straif, K. The carcinogenicity of outdoor air pollution. Lancet Oncol. 2013, 14, 1262–1263. [Google Scholar] [CrossRef]
- Yang, L.; Li, C.; Tang, X. The Impact of PM2.5 on the Host Defense of Respiratory System. Front. Cell Dev. Biol. 2020, 8, 91. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Pan, B.; Wu, J.; Chen, E.; Chen, L. Relationship between exposure to PM2.5 and lung cancer incidence and mortality: A meta-analysis. Oncotarget 2017, 8, 43322–43331. [Google Scholar] [CrossRef] [PubMed]
- Spitz, M.R.; Wei, Q.; Dong, Q.; Amos, I.C.; Wu, X. Genetic susceptibility to lung cancer: The role of DNA damage and repair. Cancer Epidemiol. Biomark. Prev. 2003, 12, 689–698. [Google Scholar]
- Zhou, W.; Liu, G.; Thurston, S.W.; Xu, L.L.; Miller, D.P.; Wain, J.C.; Lynch, T.J.; Christiani, D.C. Genetic polymorphisms in N-acetyltransferase-2 and microsomal epoxide hydrolase, cumulative cigarette smoking, and lung cancer. Cancer Epidemiol. Biomark. Prev. 2002, 11, 15–219. [Google Scholar]
- Robson, M.E.; Bradbury, A.R.; Arun, B.; Domchek, S.M.; Ford, J.M.; Hampel, H.L.; Lipkin, S.M.; Syngal, S.; Wollins, D.S.; Lindor, N.M. American society of clinical oncology policy statement update: Genetic and genomic testing for cancer susceptibility. J. Clin. Oncol. 2015, 33, 3660–3667. [Google Scholar] [CrossRef] [PubMed]
- Sorscher, S.; LoPiccolo, J.; Chen, E.; Heald, B.; Michalski, S.T.; Nielsen, S.M.; Nussbaum, R.L.; Martins, R.G.; Esplin, E.D. Landscape of pathogenic germline variants in patients with lung cancer. J. Clin. Oncol. 2022, 40, 388570. [Google Scholar] [CrossRef]
- National Cancer Institute. The TP53 Database: NCI. 2022. Available online: https://tp53.isb-cgc.org/ (accessed on 16 January 2023).
- Achatz, M.I.W.; Olivier, M.; Le Calvez, F.; Martel-Planche, G.; Lopes, A.; Rossi, B.M.; Ashton-Prolla, P.; Giugliani, R.; Palmero, E.I.; Vargas, F.R.; et al. The TP53 mutation, R337H, is associated with Li-Fraumeni and Li-Fraumeni-like syndromes in Brazilian families. Cancer Lett. 2007, 245, 96–102. [Google Scholar] [CrossRef]
- Couto, P.P.; Bastos-Rodrigues, L.; Schayek, H.; Melo, F.M.; Lisboa, R.G.C.; Miranda, D.M.; Vilhena, A.; Bale, E.A.; Friedman, E.; De Marco, L. Spectrum of germline mutations in smokers and non-smokers in Brazilian non-small-cell lung cancer (NSCLC) patients. Carcinogenesis 2017, 38, 1112–1118. [Google Scholar] [CrossRef]
- Barbosa, M.V.R.; de Lima, V.C.C.; Formiga, M.N.; de Paula, C.A.A.; Torrezan, G.T.; Carraro, D.M. High prevalence of EGFR mutations in lung adenocarcinomas from brazilian patients harboring the TP53 p.R337H variant. Clin. Lung Cancer 2020, 21, e37–e44. [Google Scholar] [CrossRef]
- Mascarenhas, E.; Gelatti, A.C.; Araújo, L.H.; Baldotto, C.; Mathias, C.; Zukin, M.; Werutsky, G.; Pacheco, P.; Gomes, R.; de Castro, G., Jr.; et al. Comprehensive genomic profiling of Brazilian non-small cell lung cancer patients (GBOT 0118/LACOG0418). Thorac. Cancer 2021, 12, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, R.L.; Polidorio, N.; Leite, A.C.R.; Cartaxo, M.; Pisani, J.P.; Quirino, C.V.; Cezana, L.; Pereira, N.G.; Pereira, A.A.L.; Rossi, B.M.; et al. Breast cancer phenotype associated with li-fraumeni syndrome: A brazilian cohort enriched by TP53 p.R337H carriers. Front. Oncol. 2022, 12, 836937. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Air Quality. 2022. Available online: https://environment.ec.europa.eu/topics/air/air-quality_en (accessed on 16 January 2023).
- Achatz, M.I.W.; Hainaut, P.; Ashton-Prolla, P. Highly prevalent TP53 mutation predisposing to many cancers in the Brazilian population: A case for newborn screening? Lancet Oncol. 2009, 10, 920–925. [Google Scholar] [CrossRef]
- Achatz, M.I.; Zambetti, G.P. The Inherited p53 mutation in the brazilian population. Cold Spring Harb. Perspect. Med. 2016, 6, a026195. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, R.L.; Masotti, C.; de Macedo, M.P.; Ribeiro, M.F.S.A.; Leite, A.C.R.; Meireles, S.I.; Bovolin, R.M.; Santini, F.C.; Munhoz, R.R.; Jardim, D.L.F.; et al. Identification of the TP53 p.R337H Variant in Tumor Genomic Profiling Should Prompt Consideration of Germline Testing for Li-Fraumeni Syndrome. JCO Glob. Oncol. 2021, 7, 1141–1150. [Google Scholar] [CrossRef]
- Zehir, A.; Benayed, R.; Shah, R.H.; Syed, A.; Middha, S.; Kim, H.R.; Srinivasan, P.; Gao, J.; Chakravarty, D.; Devlin, S.M.; et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat. Med. 2017, 23, 703–713. [Google Scholar] [CrossRef]
- Mermejo, L.M.; Leal, L.F.; Colli, L.M.; Fragoso, M.C.; Latronico, A.C.; Tone, L.G.; Scrideli, C.A.; Tucci, S.; Martinelli, C.E.; Yunes, J.A.; et al. Altered expression of noncanonical Wnt pathway genes in paediatric and adult adrenocortical tumours. Clin. Endocrinol. 2014, 81, 503–510. [Google Scholar] [CrossRef]
- Chang, K.-H.; Teng, C.-L.J.; Hsu, Y.-C.; Tsai, S.C.-S.; Lin, H.-J.; Hsieh, T.-L.; Muo, C.-H.; Hsu, C.Y.; Chou, R.-H. Long-Term Exposure to Air Pollution Associates the Risk of Benign Brain Tumor: A Nationwide, Population-Based, Cohort Study in Taiwan. Toxics 2022, 10, 176. [Google Scholar] [CrossRef]
- Guo, H.; Li, W.; Wu, J. Ambient PM2.5 and Annual Lung Cancer Incidence: A Nationwide Study in 295 Chinese Counties. Int. J. Environ. Res. Public Health 2020, 17, 1481. [Google Scholar] [CrossRef]
- Liu, J.; Chen, X.; Dou, M.; He, H.; Ju, M.; Ji, S.; Zhou, J.; Chen, C.; Zhang, D.; Miao, C.; et al. Particulate matter disrupts airway epithelial barrier via oxidative stress to promote Pseudomonas aeruginosa infection. J. Thorac. Dis. 2019, 11, 2617–2627. [Google Scholar] [CrossRef]
- Swanton, C.; Hill, W.; Lim, E.; Lee, C.; Weeden, C.; Augustine, M.; Chen, K.; Kuan, F.-C.; Marongiu, F.; Rodrigues, F.; et al. LBA1 Mechanism of action and an actionable inflammatory axis for air pollution induced non-small cell lung cancer: Towards molecular cancer prevention. Ann. Oncol. 2022, 33, S1413. [Google Scholar] [CrossRef]
- Spella, M.; Lilis, I.; Pepe, M.; Chen, Y.; Armaka, M.; Lamort, A.S.; Zazara, D.; Roumelioti, F.; Vreka, M.; Kanellakis, N.; et al. Club cells form lung adenocarcinomas and maintain the alveoli of adult mice. eLife 2019, 8, e45571. [Google Scholar] [CrossRef] [PubMed]
- Ubertini, V.; Norelli, G.; D’Arcangelo, D.; Gurtner, A.; Cesareo, E.; Baldari, S.; Gentileschi, M.P.; Piaggio, G.; Nisticò, P.; Soddu, S.; et al. Mutant p53 gains new function in promoting inflammatory signals by repression of the secreted interleukin-1 receptor antagonist. Oncogene 2015, 34, 2493–2504. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Variables | Overall Population n = 28 (%) |
|---|---|
| Mean age of diagnosis (range) | 54.6 (22–72) years |
| Gender: | |
| Female | 19 (68%) |
| Male | 9 (32%) |
| Adenocarcinoma | 28 (100%) |
| Smoking status: | |
| No | 22 (78.6%) |
| Yes | 5 (17.9%) |
| Unavailable | 1 (3.6%) |
| LC as first tumor | 22 (78.6%) |
| Secondary neoplasia: | |
| No | 15 (53.8%) |
| Yes | 12 (42.9%) |
| Unavailable | 1 (3.6%) |
| Stage at diagnosis (AJCC 8th ed.) 1: | |
| I–II | 12 (42.9%) |
| III (A/B) | 5 (17.9%) |
| IV (A/B) | 10 (35.7%) |
| Molecular assessment: | |
| No | 8 (28.6%) |
| Yes | 20 (71.4%) |
| Type of molecular assessment: | |
| NGS | 16 (57.1%) |
| RT-PCR for EGFR and ALK | 4 (14.3%) |
| ERBB Family Status | Population n = 20 (%) |
|---|---|
| Mutated/Wild-type | 14 (70%)/6 (30%) |
| EGFR exon 19 deletion | 3 (21.4%) |
| EGFR exon 18 mutation | 1 (7.1%) |
| EGFR exon 20 insertion | 2 (14.3%) |
| EGFR L858R | 7 (50%) |
| EGFR HER 2 insertion | 1 (7.1%) |
| City | Estate | Number of Cases | Ages of LC Diagnosis (Years) | Year of LC Diagnosis | Mean PM2.5 (µg/m3) | Method of Measurement | Period of Measurement |
|---|---|---|---|---|---|---|---|
| Ribeirão Preto | SP | 2 | 57/22 | 2012/2003 | 51.7 | meter on land | 2018–2022 |
| São Paulo | SP | 8 | 53/72/40/47/58/55/49/70 | 2014/2019/2020/2013/2018/2015/2021 | 63.9 | meter on land | 2014–2022 |
| Santana do Parnaíba | SP | 1 | 72 | 2017 | 12.8 | - | - |
| São José do Rio Preto | SP | 1 | 52 | 2016 | 51.8 | meter on land | 2014–2022 |
| Jacarei | SP | 1 | 63 | 2020 | 42 | meter on land | 2018–2019 |
| Sertãozinho | SP | 1 | 57 | 2020 | 25.6 | - | - |
| Campinas | SP | 1 | 41 | 2022 | 56.9 | meter on land | 2015–2022 |
| Mogi das Cruzes | SP | 1 | 62 | 2021 | 19.5 | - | - |
| Uberlândia | MG | 1 | 59 | 2019 | 27.7 | - | - |
| Monte Sião | MG | 1 | 55 | 2021 | 26.9 | - | - |
| Goiânia | GO | 1 | 51 | 2015 | 33.8 | - | - |
| Brasília | DF | 1 | 33 | 2016 | 30.5 | meter on land | April–September/22 |
| Curitiba | PR | 3 | 59/62/44 | 2017/2009/2015 | 46.5 | meter on land | 2021–2022 |
| Belo Horizonte | MG | 1 | 49 | 2009 | 32.2 (0–193) | meter on land | February–September/22 |
| Ponta Grossa | PR | 3 | 67/35/60 | 2014/2017/2017 | 18.1 | - | - |
| Londrina | PR | 1 | 57 | 2016 | 32.9 | - | - |
| Blumenau | SC | 1 | 66 | 2012 | 12.2 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopes, C.D.H.; Antonacio, F.F.; Moraes, P.M.G.; Asprino, P.F.; Galante, P.A.F.; Jardim, D.L.; de Macedo, M.P.; Sandoval, R.L.; Katz, A.; de Castro, G., Jr.; et al. The Clinical and Molecular Profile of Lung Cancer Patients Harboring the TP53 R337H Germline Variant in a Brazilian Cancer Center: The Possible Mechanism of Carcinogenesis. Int. J. Mol. Sci. 2023, 24, 15035. https://doi.org/10.3390/ijms242015035
Lopes CDH, Antonacio FF, Moraes PMG, Asprino PF, Galante PAF, Jardim DL, de Macedo MP, Sandoval RL, Katz A, de Castro G Jr., et al. The Clinical and Molecular Profile of Lung Cancer Patients Harboring the TP53 R337H Germline Variant in a Brazilian Cancer Center: The Possible Mechanism of Carcinogenesis. International Journal of Molecular Sciences. 2023; 24(20):15035. https://doi.org/10.3390/ijms242015035
Chicago/Turabian StyleLopes, Carlos D. H., Fernanda F. Antonacio, Priscila M. G. Moraes, Paula F. Asprino, Pedro A. F. Galante, Denis L. Jardim, Mariana P. de Macedo, Renata L. Sandoval, Artur Katz, Gilberto de Castro, Jr., and et al. 2023. "The Clinical and Molecular Profile of Lung Cancer Patients Harboring the TP53 R337H Germline Variant in a Brazilian Cancer Center: The Possible Mechanism of Carcinogenesis" International Journal of Molecular Sciences 24, no. 20: 15035. https://doi.org/10.3390/ijms242015035
APA StyleLopes, C. D. H., Antonacio, F. F., Moraes, P. M. G., Asprino, P. F., Galante, P. A. F., Jardim, D. L., de Macedo, M. P., Sandoval, R. L., Katz, A., de Castro, G., Jr., & Achatz, M. I. (2023). The Clinical and Molecular Profile of Lung Cancer Patients Harboring the TP53 R337H Germline Variant in a Brazilian Cancer Center: The Possible Mechanism of Carcinogenesis. International Journal of Molecular Sciences, 24(20), 15035. https://doi.org/10.3390/ijms242015035