
The Magic Triangle in Oral Potentially Malignant Disorders: Vitamin D, Vitamin D Receptor, and Malignancy



Abstract
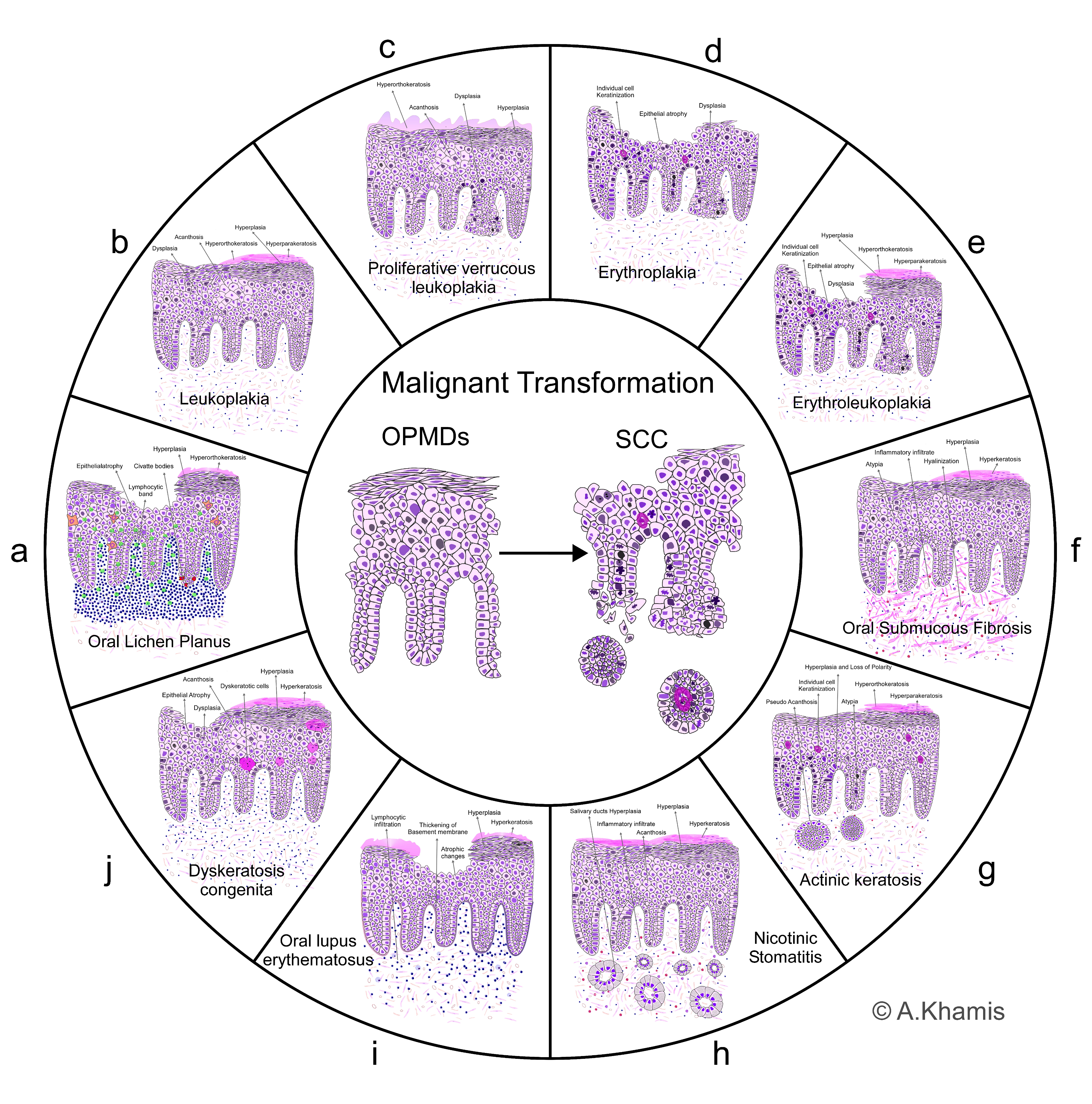
:1. Oral Potentially Malignant Disorders
1.1. Oral Lichen Planus (OLP)
1.2. Leukoplakia
1.3. Proliferative Verrucous Leukoplakia
1.4. Erythroplakia
1.5. Erythroleukoplakia
1.6. Oral Submucous Fibrosis (OSF)
1.7. Actinic Keratosis (AK)
1.8. Nicotinic Stomatitis (Palatal Lesion in Reverse Smokers)
1.9. Oral Lupus Erythematosus (OLE)
1.10. Dyskeratosis Congenita (DKC)
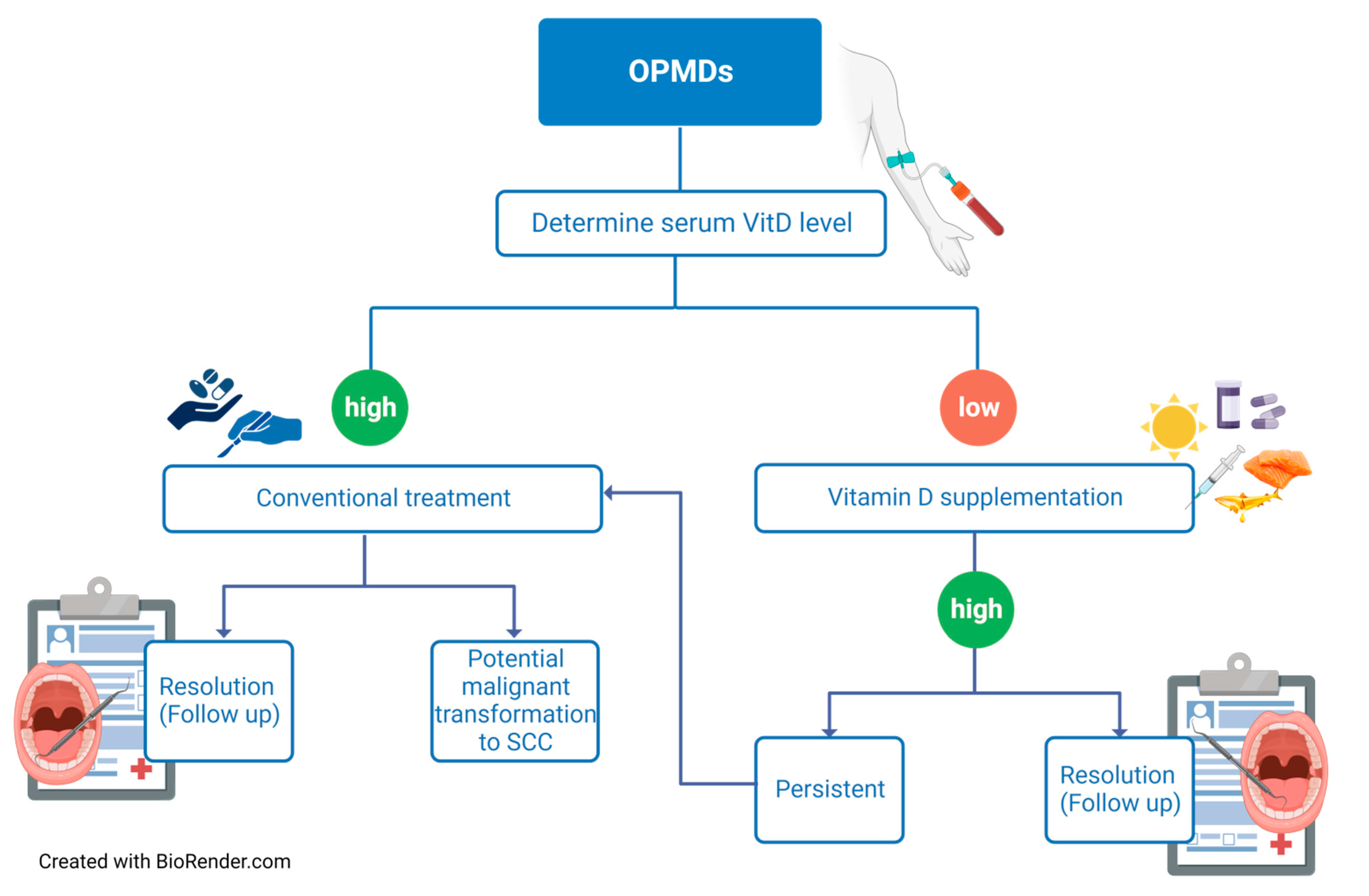
2. Preventive Measures and Treatment Options for OPMDs
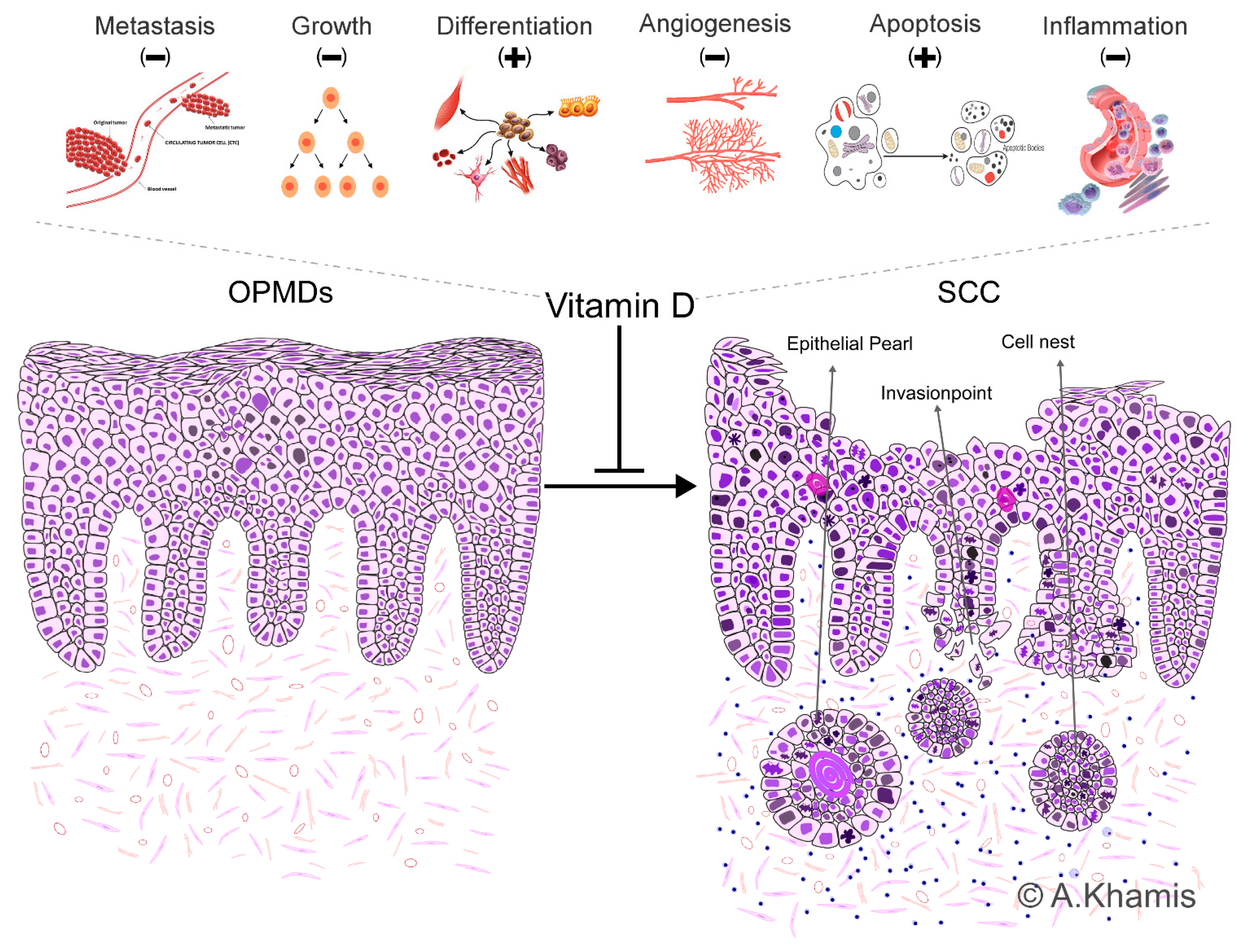
3. Physiological Roles of Vitamin D and Vitamin D Receptor
4. Vitamin D and Head and Neck Cancer
5. Vitamin D and OPMDs
6. Discussion and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lorini, L.; Bescós Atín, C.; Thavaraj, S.; Müller-Richter, U.; Alberola Ferranti, M.; Pamias Romero, J.; Sáez Barba, M.; de Pablo García-Cuenca, A.; Braña García, I.; Bossi, P.; et al. Overview of oral potentially malignant disorders: From risk factors to specific therapies. Cancers 2021, 13, 3696. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2021, 27, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Tilakaratne, W.; Jayasinghe, R.D. Oral Potentially Malignant Disorders (OPMDs). In Atlas of Dermatoses in Pigmented Skin; Springer: Singapore, 2021; pp. 879–902. [Google Scholar]
- Rad, M.; Hashemipoor, M.A.; Mojtahedi, A.; Zarei, M.R.; Chamani, G.; Kakoei, S.; Izadi, N. Correlation between clinical and histopathologic diagnoses of oral lichen planus based on modified WHO diagnostic criteria. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2009, 107, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Alaraik, A.F.; Sollecito, T.P.; Stoopler, E.T.; Akintoye, S.O.; Bindakhil, M.A. A Retrospective Pilot Study of the Clinical and Histopathological Features of Oral Lichen Planus: Comparison of the Diagnostic Criteria. Master’s Thesis, University of Pennsylvania, Philadelphia, PA, USA, 2022. [Google Scholar]
- Khamis, A.K.; Aboushelib, M.N.; Helal, M.H. Clinical Management Protocol for Dental Implants Inserted in Patients with Active Lichen Planus. Part II 4-Year Follow-Up. J. Prosthodont. 2019, 28, 519–525. [Google Scholar] [CrossRef]
- Tovaru, S.; Costache, M.; Perlea, P.; Caramida, M.; Totan, C.; Warnakulasuriya, S.; Parlatescu, I. Oral leukoplakia: A clinicopathological study and malignant transformation. Oral Dis. 2023, 29, 1454–1463. [Google Scholar] [CrossRef]
- Evren, I.; Brouns, E.R.; Poell, J.B.; Wils, L.J.; Brakenhoff, R.H.; Bloemena, E.; de Visscher, J.G. Associations between clinical and histopathological characteristics in oral leukoplakia. Oral Dis. 2023, 29, 696–706. [Google Scholar] [CrossRef]
- Farah, C.S. Molecular, genomic and mutational landscape of oral leukoplakia. Oral Dis. 2021, 27, 803–812. [Google Scholar] [CrossRef]
- Thompson, L.D.; Fitzpatrick, S.G.; Müller, S.; Eisenberg, E.; Upadhyaya, J.D.; Lingen, M.W.; Vigneswaran, N.; Woo, S.-B.; Bhattacharyya, I.; Bilodeau, E.A.; et al. Proliferative verrucous leukoplakia: An expert consensus guideline for standardized assessment and reporting. Head Neck Pathol. 2021, 15, 572–587. [Google Scholar] [CrossRef]
- Upadhyaya, J.D.; Fitzpatrick, S.G.; Cohen, D.M.; Bilodeau, E.A.; Bhattacharyya, I.; Lewis, J.S.; Lai, J.; Wright, J.M.; Bishop, J.A.; Leon, M.E. Inter-observer variability in the diagnosis of proliferative verrucous leukoplakia: Clinical implications for oral and maxillofacial surgeon understanding: A collaborative pilot study. Head Neck Pathol. 2020, 14, 156–165. [Google Scholar] [CrossRef]
- Parasuraman, L.; Bal, M.; Pai, P.S. Erythroplakia and erythroleucoplakia. In Premalignant Conditions of the Oral Cavity; Springer: Singapore, 2019; pp. 87–95. [Google Scholar]
- Lorenzo-Pouso, A.I.; Lafuente-Ibáñez de Mendoza, I.; Pérez-Sayáns, M.; Pérez-Jardón, A.; Chamorro-Petronacci, C.M.; Blanco-Carrión, A.; Aguirre-Urízar, J.M. Critical update, systematic review, and meta-analysis of oral erythroplakia as an oral potentially malignant disorder. J. Oral Pathol. Med. 2022, 51, 585–593. [Google Scholar] [CrossRef]
- Yuwanati, M.; Ramadoss, R.; Kudo, Y.; Ramani, P.; Senthil Murugan, M. Prevalence of oral submucous fibrosis among areca nut chewers: A systematic review and meta-analysis. Oral Dis. 2022, 29, 1920–1926. [Google Scholar] [CrossRef] [PubMed]
- Sarode, S.C.; Gondivkar, S.; Gadbail, A.; Sarode, G.S.; Yuwanati, M. Oral submucous fibrosis and heterogeneity in outcome measures: A critical viewpoint. Future Oncol. 2021, 17, 2123–2126. [Google Scholar] [CrossRef] [PubMed]
- Motgi, A.A.; Shete, M.V.; Chavan, M.S.; Diwaan, N.N.; Sapkal, R.; Channe, P. Assessment of correlation between clinical staging, functional staging, and histopathological grading of oral submucous fibrosis. J. Carcinog. 2021, 20, 16. [Google Scholar] [CrossRef] [PubMed]
- Reinehr, C.P.H.; Bakos, R.M. Actinic keratoses: Review of clinical, dermoscopic, and therapeutic aspects. An. Bras. Dermatol. 2020, 94, 637–657. [Google Scholar] [CrossRef] [PubMed]
- Balcere, A.; Konrāde-Jilmaza, L.; Pauliņa, L.A.; Čēma, I.; Krūmiņa, A. Clinical characteristics of actinic keratosis associated with the risk of progression to invasive squamous cell carcinoma: A systematic review. J. Clin. Med. 2022, 11, 5899. [Google Scholar] [CrossRef] [PubMed]
- Heerfordt, I.M.; Poulsen, T.; Wulf, H.C. Actinic keratoses contiguous with squamous cell carcinomas are mostly non-hyperkeratotic and with severe dysplasia. J. Clin. Pathol. 2022, 75, 560–563. [Google Scholar] [CrossRef]
- Won, J.; Clark, H. Palatal keratosis associated with reverse (or “backwards”) smoking (PKARS). N. Z. Med. J. (Online) 2022, 135, 104–107. [Google Scholar]
- Slootweg, P.J.; Merkx, T.A. Premalignant lesions of the oral cavity. In Surgical Pathology of the Head and Neck; CRC Press: Boca Raton, FL, USA, 2019; pp. 277–294. [Google Scholar]
- García-Ríos, P.; Pecci-Lloret, M.P.; Oñate-Sánchez, R.E. Oral Manifestations of Systemic Lupus Erythematosus: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11910. [Google Scholar] [CrossRef]
- Cardoso, I.L.; Leal, F.; Regis, R.C. Systemic lupus erythematosus and implications for the oral cavity. J. Med. Care Res. Rev. 2020, 3, 444–453. [Google Scholar] [CrossRef]
- Noto, Z.; Tomihara, K.; Furukawa, K.; Noguchi, M. Dyskeratosis congenita associated with leukoplakia of the tongue. Int. J. Oral Maxillofac. Surg. 2016, 45, 760–763. [Google Scholar] [CrossRef]
- Sinha, S.; Trivedi, V.; Krishna, A.; Rao, N. Dyskeratosis congenita-management and review of complications: A case report. Oman Med. J. 2013, 28, 281. [Google Scholar] [CrossRef] [PubMed]
- Moretti, S.; Spallanzani, A.; Chiarugi, A.; Muscarella, G.; Battini, M. Oral carcinoma in a young man: A case of dyskeratosis congenita. J. Eur. Acad. Dermatol. Venereol. 2000, 14, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Mohan, P. Assessment of the Feasibility of Opportunistic Screening for Oral Potentially Malignant Disorders and Oral Cancer at Dental Colleges in India: A Public Health Initiative from Bengaluru. 2022. Available online: https://core.ac.uk/display/544313902?source=2 (accessed on 27 September 2023).
- Kumari, P.; Debta, P.; Dixit, A. Oral potentially malignant disorders: Etiology, pathogenesis, and transformation into oral cancer. Front. Pharmacol. 2022, 13, 825266. [Google Scholar] [CrossRef] [PubMed]
- Iocca, O.; Sollecito, T.P.; Alawi, F.; Weinstein, G.S.; Newman, J.G.; De Virgilio, A.; Di Maio, P.; Spriano, G.; Pardiñas López, S.; Shanti, R.M. Potentially malignant disorders of the oral cavity and oral dysplasia: A systematic review and meta-analysis of malignant transformation rate by subtype. Head Neck 2020, 42, 539–555. [Google Scholar] [CrossRef]
- Chen, J.; Tang, Z.; Slominski, A.T.; Li, W.; Żmijewski, M.A.; Liu, Y.; Chen, J. Vitamin D and its analogs as anticancer and anti-inflammatory agents. Eur. J. Med. Chem. 2020, 207, 112738. [Google Scholar] [CrossRef]
- Janoušek, J.; Pilařová, V.; Macáková, K.; Nomura, A.; Veiga-Matos, J.; da Silva, D.D.; Remião, F.; Saso, L.; Malá-Ládová, K.; Malý, J.; et al. Vitamin D: Sources, physiological role, biokinetics, deficiency, therapeutic use, toxicity, and overview of analytical methods for detection of vitamin D and its metabolites. Crit. Rev. Clin. Lab. Sci. 2022, 59, 517–554. [Google Scholar] [CrossRef]
- Starczak, Y.; Reinke, D.C.; Barratt, K.R.; Ryan, J.W.; Russell, P.K.; Clarke, M.V.; St-Arnaud, R.; Morris, H.A.; Davey, R.A.; Atkins, G.J.; et al. Absence of vitamin D receptor in mature osteoclasts results in altered osteoclastic activity and bone loss. J. Steroid Biochem. Mol. Biol. 2018, 177, 77–82. [Google Scholar] [CrossRef]
- Vincent-Chong, V.K.; DeJong, H.; Attwood, K.; Hershberger, P.A.; Seshadri, M. Preclinical Prevention Trial of Calcitriol: Impact of Stage of Intervention and Duration of Treatment on Oral Carcinogenesis. Neoplasia 2019, 21, 376–388. [Google Scholar] [CrossRef]
- Schweitzer, A.; Knauer, S.K.; Stauber, R.H. Nuclear receptors in head and neck cancer: Current knowledge and perspectives. Int. J. Cancer 2010, 126, 801–809. [Google Scholar] [CrossRef]
- Warwick, T.; Schulz, M.H.; Gilsbach, R.; Brandes, R.P.; Seuter, S. Nuclear receptor activation shapes spatial genome organization essential for gene expression control: Lessons learned from the vitamin D receptor. Nucleic Acids Res. 2022, 50, 3745–3763. [Google Scholar] [CrossRef]
- Haussler, M.R.; Jurutka, P.W.; Mizwicki, M.; Norman, A.W. Vitamin D receptor (VDR)-mediated actions of 1α, 25 (OH) 2vitamin D3: Genomic and non-genomic mechanisms. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 543–559. [Google Scholar] [CrossRef] [PubMed]
- Carlberg, C.; Muñoz, A. An update on vitamin D signaling and cancer. Semin. Cancer Biol. 2020, 79, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Bakke, D.; Sun, J. Ancient nuclear receptor VDR with new functions: Microbiome and inflammation. Inflamm. Bowel Dis. 2018, 24, 1149–1154. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Khamis, A.; Gül, D.; Wandrey, M.; Lu, Q.; Knauer, S.K.; Reinhardt, C.; Strieth, S.; Hagemann, J.; Stauber, R.H. The Vitamin D Receptor–BIM Axis Overcomes Cisplatin Resistance in Head and Neck Cancer. Cancers 2022, 14, 5131. [Google Scholar] [CrossRef]
- Bikle, D.; Christakos, S. New aspects of vitamin D metabolism and action—Addressing the skin as source and target. Nat. Rev. Endocrinol. 2020, 16, 234–252. [Google Scholar] [CrossRef]
- Saponaro, F.; Saba, A.; Zucchi, R. An update on vitamin D metabolism. Int. J. Mol. Sci. 2020, 21, 6573. [Google Scholar] [CrossRef] [PubMed]
- Minisola, S.; Ferrone, F.; Danese, V.; Cecchetti, V.; Pepe, J.; Cipriani, C.; Colangelo, L. Controversies Surrounding Vitamin D: Focus on Supplementation and Cancer. Int. J. Environ. Res. Public Health 2019, 16, 189. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.; Querings, K.; Reichrath, J. Vitamin D and skin: New aspects for dermatology. Exp. Dermatol. 2004, 13, 11–15. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D; Humana Press: Totowa, NJ, USA, 2010. [Google Scholar] [CrossRef]
- Carlberg, C. Nutrigenomics of Vitamin D. Nutrients 2019, 11, 676. [Google Scholar] [CrossRef]
- Deb, S.; Reeves, A.A.; Lafortune, S. Simulation of Physicochemical and Pharmacokinetic Properties of Vitamin D3 and Its Natural Derivatives. Pharmaceuticals 2020, 13, 160. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, B.; Meurer, M. Vitamin D metabolism. Dermatol. Ther. 2010, 23, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D: Production, metabolism and mechanisms of action. In Endotext [Internet]; MDText.com, Inc.: South Dartmouth, MA, USA, 2021. [Google Scholar]
- Niedermaier, T.; Gredner, T.; Kuznia, S.; Schöttker, B.; Mons, U.; Lakerveld, J.; Ahrens, W.; Brenner, H.; PEN-Consortium. Vitamin D food fortification in European countries: The underused potential to prevent cancer deaths. Eur. J. Epidemiol. 2022, 37, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, E.; Kiely, M.; James, A.P.; Singh, T.; Black, L.J. The efficacy of vitamin D food fortification and biofortification in children and adults: A systematic review protocol. JBI Evid. Synth. 2020, 18, 2694–2703. [Google Scholar] [CrossRef]
- Moslemi, E.; Musazadeh, V.; Kavyani, Z.; Naghsh, N.; Shoura, S.M.S.; Dehghan, P. Efficacy of vitamin D supplementation as an adjunct therapy for improving inflammatory and oxidative stress biomarkers: An umbrella meta-analysis. Pharmacol. Res. 2022, 186, 106484. [Google Scholar] [CrossRef]
- Bouillon, R.; Gomez, J.M.Q. Comparison of calcifediol with vitamin D for prevention or cure of vitamin D deficiency. J. Steroid Biochem. Mol. Biol. 2023, 228, 106248. [Google Scholar] [CrossRef]
- Giustina, A.; Bouillon, R.; Dawson-Hughes, B.; Ebeling, P.R.; Lazaretti-Castro, M.; Lips, P.; Marcocci, C.; Bilezikian, J.P. Vitamin D in the older population: A consensus statement. Endocrine 2023, 79, 31–44. [Google Scholar] [CrossRef]
- Gandini, S.; Boniol, M.; Haukka, J.; Byrnes, G.; Cox, B.; Sneyd, M.J.; Mullie, P.; Autier, P. Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. Int. J. Cancer 2011, 128, 1414–1424. [Google Scholar] [CrossRef]
- Billington, E.O.; Burt, L.A.; Rose, M.S.; Davison, E.M.; Gaudet, S.; Kan, M.; Boyd, S.K.; Hanley, D.A. Safety of high-dose vitamin D supplementation: Secondary analysis of a randomized controlled trial. J. Clin. Endocrinol. Metab. 2020, 105, 1261–1273. [Google Scholar] [CrossRef]
- Farrell, C.-J.; Herrmann, M. Determination of vitamin D and its metabolites. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 675–688. [Google Scholar] [CrossRef]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A. Skeletal and extraskeletal actions of vitamin D: Current evidence and outstanding questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [PubMed]
- Heath, A.K.; Kim, I.Y.; Hodge, A.M.; English, D.R.; Muller, D.C. Vitamin D Status and Mortality: A Systematic Review of Observational Studies. Int. J. Environ. Res. Public Health 2019, 16, 383. [Google Scholar] [CrossRef] [PubMed]
- Migliaccio, S.; Di Nisio, A.; Magno, S.; Romano, F.; Barrea, L.; Colao, A.M.; Muscogiuri, G.; Savastano, S. Vitamin D deficiency: A potential risk factor for cancer in obesity? Int. J. Obes. 2022, 46, 707–717. [Google Scholar] [CrossRef]
- Sîrbe, C.; Rednic, S.; Grama, A.; Pop, T.L. An Update on the Effects of Vitamin D on the Immune System and Autoimmune Diseases. Int. J. Mol. Sci. 2022, 23, 9784. [Google Scholar]
- Filipe Rosa, L.; Petersen, P.P.; Görtz, L.F.; Stolzer, I.; Kaden-Volynets, V.; Günther, C.; Bischoff, S.C. Vitamin A-and D-Deficient Diets Disrupt Intestinal Antimicrobial Peptide Defense Involving Wnt and STAT5 Signaling Pathways in Mice. Nutrients 2023, 15, 376. [Google Scholar]
- Shahrajabian, M.H.; Cheng, Q.; Sun, W. Vitamin C and D Supplements to Prevent the Risk of COVID-19. Nat. Prod. J. 2023, 13, 47–59. [Google Scholar]
- Koll, L.; Gül, D.; Elnouaem, M.I.; Raslan, H.; Ramadan, O.R.; Knauer, S.K.; Strieth, S.; Hagemann, J.; Stauber, R.H.; Khamis, A. Exploiting Vitamin D Receptor and Its Ligands to Target Squamous Cell Carcinomas of the Head and Neck. Int. J. Mol. Sci. 2023, 24, 4675. [Google Scholar] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef]
- Tuna, S.; Aydin, M.A.; Aydin, M.F. The Four Horsemen of the Apocalypse: Cancer, Depression, Vitamin D Deficiency, and Obesity: An Observational Study. Dis. Markers 2023, 2023, 9652491. [Google Scholar] [CrossRef]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A. Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef]
- Looker, A.C.; Johnson, C.L.; Lacher, D.A.; Pfeiffer, C.M.; Schleicher, R.L.; Sempos, C.T. Vitamin D status: United states, 2001–2006. NCHS Data Brief 2011, 59, 1–8. [Google Scholar]
- Hagenau, T.; Vest, R.; Gissel, T.; Poulsen, C.; Erlandsen, M.; Mosekilde, L.; Vestergaard, P. Global vitamin D levels in relation to age, gender, skin pigmentation and latitude: An ecologic meta-regression analysis. Osteoporos. Int. 2009, 20, 133–140. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Conzelmann, M.; Stähelin, H.; Dick, W.; Carpenter, M.; Adkin, A.L.; Theiler, R.; Pfeifer, M.; Allum, J.H. Is fall prevention by vitamin D mediated by a change in postural or dynamic balance? Osteoporos. Int. 2006, 17, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [PubMed]
- Wietrzyk, J.; Milczarek, M.; Kutner, A. The effect of combined treatment on head and neck human cancer cell lines with novel analogs of calcitriol and cytostatics. Oncol. Res. 2007, 16, 517–525. [Google Scholar] [CrossRef]
- Martinez-Reza, I.; Diaz, L.; Barrera, D.; Segovia-Mendoza, M.; Pedraza-Sanchez, S.; Soca-Chafre, G.; Larrea, F.; Garcia-Becerra, R. Calcitriol Inhibits the Proliferation of Triple-Negative Breast Cancer Cells through a Mechanism Involving the Proinflammatory Cytokines IL-1beta and TNF-alpha. J. Immunol. Res. 2019, 2019, 6384278. [Google Scholar] [CrossRef]
- Garland, C.F.; Gorham, E.D.; Mohr, S.B.; Garland, F.C. Vitamin D for cancer prevention: Global perspective. Ann. Epidemiol. 2009, 19, 468–483. [Google Scholar] [CrossRef]
- Muñoz, A.; Grant, W.B. Vitamin D and cancer: An historical overview of the epidemiology and mechanisms. Nutrients 2022, 14, 1448. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Alonso, P.; Boughanem, H.; Canudas, S.; Becerra-Tomás, N.; Fernández de la Puente, M.; Babio, N.; Macias-Gonzalez, M.; Salas-Salvadó, J. Circulating vitamin D levels and colorectal cancer risk: A meta-analysis and systematic review of case-control and prospective cohort studies. Crit. Rev. Food Sci. Nutr. 2023, 63, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Brozyna, A.A.; Hoffman, R.M.; Slominski, A.T. Relevance of Vitamin D in Melanoma Development, Progression and Therapy. Anticancer Res. 2020, 40, 473–489. [Google Scholar] [CrossRef] [PubMed]
- Carlberg, C.; Velleuer, E. Vitamin D and the risk for cancer: A molecular analysis. Biochem. Pharmacol. 2022, 196, 114735. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.S.-C.; Kiang, K.M.-Y.; Leung, G.K.-K. Anti-tumor effects of vitamin D in glioblastoma: Mechanism and therapeutic implications. Lab. Investig. 2022, 102, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, J.K.; Nurmi, T.; Aro, A.; Bertone-Johnson, E.R.; Hyppönen, E.; Kröger, H.; Lamberg-Allardt, C.; Manson, J.E.; Mursu, J.; Mäntyselkä, P.; et al. Vitamin D supplementation and prevention of cardiovascular disease and cancer in the Finnish Vitamin D Trial: A randomized controlled trial. Am. J. Clin. Nutr. 2022, 115, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Zanello, L.P.; Norman, A. 1alpha,25(OH)2 vitamin D3 actions on ion channels in osteoblasts. Steroids 2006, 71, 291–297. [Google Scholar] [CrossRef]
- Negri, M.; Gentile, A.; de Angelis, C.; Montò, T.; Patalano, R.; Colao, A.; Pivonello, R.; Pivonello, C. Vitamin D-Induced Molecular Mechanisms to Potentiate Cancer Therapy and to Reverse Drug-Resistance in Cancer Cells. Nutrients 2020, 12, 1798. [Google Scholar] [CrossRef]
- Wu, X.; Hu, W.; Lu, L.; Zhao, Y.; Zhou, Y.; Xiao, Z.; Zhang, L.; Zhang, H.; Li, X.; Li, W.; et al. Repurposing vitamin D for treatment of human malignancies via targeting tumor microenvironment. Acta Pharm. Sin. B 2019, 9, 203–219. [Google Scholar] [CrossRef]
- Valdés-López, J.F.; Velilla, P.; Urcuqui-Inchima, S. Vitamin D modulates the expression of Toll-like receptors and pro-inflammatory cytokines without affecting Chikungunya virus replication, in monocytes and macrophages. Acta Trop. 2022, 232, 106497. [Google Scholar] [CrossRef]
- Ali, A.J.M.; Hamoud, M.J.M. Estimation the Relationship Between Vitamin D and Some Immune Parameters Among Patients with Graves’ Disease. Pak. J. Med. Health Sci. 2022, 16, 854. [Google Scholar]
- Henn, M.; Martin-Gorgojo, V.; Martin-Moreno, J.M. Vitamin D in Cancer Prevention: Gaps in Current Knowledge and Room for Hope. Nutrients 2022, 14, 4512. [Google Scholar] [CrossRef] [PubMed]
- Gugatschka, M.; Kiesler, K.; Obermayer-Pietsch, B.; Groselj-Strele, A.; Griesbacher, A.; Friedrich, G. Vitamin D status is associated with disease-free survival and overall survival time in patients with squamous cell carcinoma of the upper aerodigestive tract. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Orell–Kotikangas, H.; Schwab, U.; Österlund, P.; Saarilahti, K.; Mäkitie, O.; Mäkitie, A.A. High prevalence of vitamin D insufficiency in patients with head and neck cancer at diagnosis. Head Neck 2012, 34, 1450–1455. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Bojesen, S.E.; Nordestgaard, B.G. Low plasma 25-hydroxyvitamin D and risk of tobacco-related cancer. Clin. Chem. 2013, 59, 771–780. [Google Scholar] [CrossRef]
- Fanidi, A.; Muller, D.C.; Midttun, Ø.; Ueland, P.M.; Vollset, S.E.; Relton, C.; Vineis, P.; Weiderpass, E.; Skeie, G.; Brustad, M.; et al. Circulating vitamin D in relation to cancer incidence and survival of the head and neck and oesophagus in the EPIC cohort. Sci. Rep. 2016, 6, 36017. [Google Scholar] [CrossRef]
- Mostafa, B.E.-D.; Abdelmageed, H.M.; El-Begermy, M.M.; Taha, M.S.; Hamdy, T.A.-E.; Omran, A.; Lotfy, N. Value of vitamin D assessment in patients with head and neck squamous cell cancer before treatment. Egypt. J. Otolaryngol. 2016, 32, 279–286. [Google Scholar] [CrossRef]
- Bochen, F.; Balensiefer, B.; Körner, S.; Bittenbring, J.T.; Neumann, F.; Koch, A.; Bumm, K.; Marx, A.; Wemmert, S.; Papaspyrou, G. Vitamin D deficiency in head and neck cancer patients–prevalence, prognostic value and impact on immune function. Oncoimmunology 2018, 7, e1476817. [Google Scholar] [CrossRef]
- Nejatinamini, S.; Debenham, B.J.; Clugston, R.D.; Mawani, A.; Parliament, M.; Wismer, W.V.; Mazurak, V.C. Poor Vitamin Status is Associated with Skeletal Muscle Loss and Mucositis in Head and Neck Cancer Patients. Nutrients 2018, 10, 1236. [Google Scholar] [CrossRef]
- Arem, H.; Weinstein, S.J.; Horst, R.L.; Virtamo, J.; Yu, K.; Albanes, D.; Abnet, C.C. Serum 25-Hydroxyvitamin D and Risk of Oropharynx and Larynx Cancers in Finnish MenVitamin D and Head and Neck Cancers. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1178–1184. [Google Scholar] [CrossRef]
- Skaaby, T.; Husemoen, L.L.N.; Thuesen, B.H.; Pisinger, C.; Jørgensen, T.; Roswall, N.; Larsen, S.C.; Linneberg, A. Prospective Population-Based Study of the Association between Serum 25-Hydroxyvitamin-D Levels and the Incidence of Specific Types of CancerVitamin D and Cancer Incidence. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1220–1229. [Google Scholar] [CrossRef] [PubMed]
- Akutsu, T.; Kitamura, H.; Himeiwa, S.; Kitada, S.; Akasu, T.; Urashima, M. Vitamin D and Cancer Survival: Does Vitamin D Supplementation Improve the Survival of Patients with Cancer? Curr. Oncol. Rep. 2020, 22, 62. [Google Scholar] [CrossRef] [PubMed]
- Lathers, D.M.; Clark, J.I.; Achille, N.J.; Young, M.R.I. Phase IB study of 25-hydroxyvitamin D3 treatment to diminish suppressor cells in head and neck cancer patients. Hum. Immunol. 2001, 62, 1282–1293. [Google Scholar] [CrossRef] [PubMed]
- Grimm, M.; Cetindis, M.; Biegner, T.; Lehman, M.; Munz, A.; Teriete, P.; Reinert, S. Serum vitamin D levels of patients with oral squamous cell carcinoma (OSCC) and expression of vitamin D receptor in oral precancerous lesions and OSCC. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e188–e195. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Holt, H.; Greenig, M.; Talaei, M.; Perdek, N.; Pfeffer, P.; Vivaldi, G.; Maltby, S.; Symons, J.; Barlow, N.L.; et al. Effect of a test-and-treat approach to vitamin D supplementation on risk of all cause acute respiratory tract infection and covid-19: Phase 3 randomised controlled trial (CORONAVIT). BMJ 2022, 378, e071230. [Google Scholar] [CrossRef]
- Maturana-Ramírez, A.; Aitken-Saavedra, J.; Guevara-Benítez, A.L.; Espinoza-Santander, I. Hypovitaminosis D, oral potentially malignant disorders, and oral squamous cell carcinoma: A systematic review. Med. Oral Patol. Oral Cirugía Bucal 2022, 27, e135–e141. [Google Scholar] [CrossRef]
- Palma, V.d.M.; Koerich Laureano, N.; Frank, L.A.; Rados, P.V.; Visioli, F. Chemoprevention in oral leukoplakia: Challenges and current landscape. Front. Oral Health 2023, 4, 1191347. [Google Scholar] [CrossRef]
- Hung, M.; Almpani, K.; Thao, B.; Sudweeks, K.; Lipsky, M.S. Vitamin D in the Prevention and Treatment of Oral Cancer: A Scoping Review. Nutrients 2023, 15, 2346. [Google Scholar] [CrossRef]
- Shukla, A.; Mehrotra, D. Oral Potentially Malignant Disorders. In Fundamentals of Oral and Maxillofacial Surgery-E-Book; Elsevier: Chennai, India, 2020; Volume 313. [Google Scholar]
- Gupta, J.; Aggarwal, A.; Asadullah, M.; Khan, M.H.; Agrawal, N.; Khwaja, K.J. Vitamin D in the treatment of oral lichen planus: A pilot clinical study. J. Indian Acad. Oral Med. Radiol. 2019, 31, 222–227. [Google Scholar]
- McMahon, L.; Schwartz, K.; Yilmaz, O.; Brown, E.; Ryan, L.K.; Diamond, G. Vitamin D-mediated induction of innate immunity in gingival epithelial cells. Infect. Immun. 2011, 79, 2250–2256. [Google Scholar] [CrossRef]
- Walsh, J.E.; Clark, A.-M.; Day, T.A.; Gillespie, M.B.; Young, M.R.I. Use of α, 25-dihydroxyvitamin D3 treatment to stimulate immune infiltration into head and neck squamous cell carcinoma. Hum. Immunol. 2010, 71, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Sakyi, S.A.; Owusu-Yeboah, M.; Obirikorang, C.; Dadzie Ephraim, R.K.; Kwarteng, A.; Opoku, S.; Afranie, B.O.; Senu, E.; Boateng, A.O.; Boakye, D.K.; et al. Profiling vitamin D, its mediators and proinflammatory cytokines in rheumatoid arthritis: A case–control study. Immun. Inflamm. Dis. 2022, 10, e676. [Google Scholar] [CrossRef] [PubMed]
- Halim, C.; Mirza, A.F.; Sari, M.I. The Association between TNF-α, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, N.; Turan, H.; Bayraktar, M.; Ozturk, A.; Erdoğdu, H. Analysis of serum cytokine and protective vitamin D levels in severe cases of COVID-19. J. Med. Virol. 2022, 94, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Giulietti, A.; van Etten, E.; Overbergh, L.; Stoffels, K.; Bouillon, R.; Mathieu, C. Monocytes from type 2 diabetic patients have a pro-inflammatory profile: 1, 25-Dihydroxyvitamin D3 works as anti-inflammatory. Diabetes Res. Clin. Pract. 2007, 77, 47–57. [Google Scholar] [CrossRef]
- Gwenzi, T.; Zhu, A.; Schrotz-King, P.; Schöttker, B.; Hoffmeister, M.; Brenner, H. Effects of vitamin D supplementation on inflammatory response in patients with cancer and precancerous lesions: Systematic review and meta-analysis of randomized trials. Clin. Nutr. 2023, 42, 1142–1150. [Google Scholar] [CrossRef]
- McLachlan, C.S. The angiotensin-converting enzyme 2 (ACE2) receptor in the prevention and treatment of COVID-19 are distinctly different paradigms. Clin. Hypertens. 2020, 26, 14. [Google Scholar] [CrossRef]
- Zhang, Y.G.; Lu, R.; Xia, Y.; Zhou, D.; Petrof, E.; Claud, E.C.; Sun, J. Lack of Vitamin D Receptor Leads to Hyperfunction of Claudin-2 in Intestinal Inflammatory Responses. Inflamm. Bowel Dis. 2019, 25, 97–110. [Google Scholar] [CrossRef]
- Krishnan, A.V.; Feldman, D. Mechanisms of the anti-cancer and anti-inflammatory actions of vitamin D. Annu. Rev. Pharmacol. Toxicol. 2011, 51, 311–336. [Google Scholar] [CrossRef]
- Fernández-Barral, A.; Bustamante-Madrid, P.; Ferrer-Mayorga, G.; Barbáchano, A.; Larriba, M.J.; Muñoz, A. Vitamin D Effects on Cell Differentiation and Stemness in Cancer. Cancers 2020, 12, 2413. [Google Scholar] [CrossRef]
- Samuel, S.; Sitrin, M.D. Vitamin D’s role in cell proliferation and differentiation. Nutr. Rev. 2008, 66, S116–S124. [Google Scholar] [CrossRef] [PubMed]
- Hendi, N.N.; Nemer, G. Epigenetic regulation of vitamin D deficiency. Epigenomics 2023, 15, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Snegarova, V.; Naydenova, D. Vitamin D: A Review of its Effects on Epigenetics and Gene Regulation. Folia Medica 2020, 62, 662–667. [Google Scholar] [PubMed]
- Fetahu, I.S.; Höbaus, J.; Kállay, E. Vitamin D and the epigenome. Front. Physiol. 2014, 5, 164. [Google Scholar] [CrossRef]
- Skrajnowska, D.; Bobrowska-Korczak, B. Potential Molecular Mechanisms of the Anti-cancer Activity of Vitamin D. Anticancer Res. 2019, 39, 3353–3363. [Google Scholar] [CrossRef]
- Diaz, L.; Diaz-Munoz, M.; Garcia-Gaytan, A.C.; Mendez, I. Mechanistic Effects of Calcitriol in Cancer Biology. Nutrients 2015, 7, 5020–5050. [Google Scholar] [CrossRef]
- Vuolo, L.; Di Somma, C.; Faggiano, A.; Colao, A. Vitamin D and cancer. Front. Endocrinol. 2012, 3, 58. [Google Scholar] [CrossRef]
- Zhang, J.; Yang, S.; Xu, B.; Wang, T.; Zheng, Y.; Liu, F.; Ren, F.; Jiang, J.; Shi, H.; Zou, B.; et al. p62 functions as an oncogene in colorectal cancer through inhibiting apoptosis and promoting cell proliferation by interacting with the vitamin D receptor. Cell Prolif. 2019, 52, e12585. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Leukoplakia |
|---|---|
| Color | Primarily white |
| Appearance/shape | Homogenous: uniform, well-defined borders Non-homogenous: speckled, nodular with diffuse borders |
| Scrappability | Non-scrapable Remains after tissue retraction or stretching |
| Exclusion criteria | Presence of (chronic) traumatic irritation Signs or symptoms of other red/white lesions |
| Persistent | Persists after elimination of apparent traumatic causes |
| OPMDs | Site | Clinical Presentation | Key Histopathologic Features | Etiology | Demographics |
|---|---|---|---|---|---|
| Oral lichen planus | -Bilateral post buccal mucosa -Tongue -Lips and gingiva -Floor of the mouth | -Reticular -Plaque -Atrophic -Erosive -Bullous | -Hyperkeratosis, acanthosis, or atrophy -Saw-tooth rete-pegs -Atypia and dysplasia | Multi-factorial: -Immunological -Environmental -Drug reaction Stress | Sex: Female > Men Age: >40 |
| Leukoplakia | -Vermillion border -Buccal mucosa -Gingiva -Palate -Tongue -Floor of the mouth | -White patch or plaque -Cannot be scraped off | -Mild to severe dysplasia | -Smoking -Alcohol -Sunlight -Nutritional deficiency -Infectious | Sex: Female = Male Middle Age |
| Proliferative verrucous leukoplakia | Multifocal | -Early: Flat White lesion -Late: warty, papillary or verrucous | -Dysplasia -Invasion may also be seen | Unknown | Sex: Female > Male Age: >40 |
| Erythroplakia | Any | -Red Mucosal lesion -Cannot be scraped off -Sharply demarcated | -Mild to severe dysplasia -Carcinoma in situ -Invasion | Unknown | A common precursor of OSCC |
| Erythroleukoplakia | Any | Mixed mucosal lesion | Mild to severe dysplasia | Unknown | A common precursor of OSCC |
| Oral submucous fibrosis (OSF) | -Buccal mucosa -Retro molar area -Soft palate | -Marble-like pallor mucosa -Leathery appearance | -Sub-epithelial fibrosis and hyalinization -Epithelial atypia | -Chronic use of betel quid -Spicy food | Sex: Female > Male Age: young adult |
| Actinic keratosis (AK) | -Vermilion border -Lower lip | -Rough, scaly patches | -Epithelial atrophy -Ortho/Para keratinization -Atypia -Individual cell keratinization -Pseudo acanthosis | Sunlight | Sex Male > Female Middle age White skin |
| Nicotinic stomatitis | -Palate | -Thickened white plaques -Mucosal nodularity -Erythema -Ulceration | -Hyperkeratosis -Acanthosis -Squamous metaplasia -Salivary gland ducts hyperplasia | Reverse smoking | India Caribbean Islands Latin America Sardinia |
| Oral lupus erythematosus (OLE) | -Buccal mucosa -Palate -Lips | -Central circular zone of atrophic mucosa -White striae on borders | -Atrophic to hyperkeratotic epithelium -Sub-epithelial lymphocytic infiltration. -Basal cell degeneration -Thickening of the basement membrane | -Subtype of lupus erythematosus | Sex: Female > Male Age: First diagnosis 20–40 years |
| Dyskeratosis congenita (DKC) | -Tongue -Buccal mucosa -Soft palate | -White patch -Papillary projections | -Dyskeratotic cells -Epithelial atrophy -Acanthosis -Dysplasia -Hyperplasia -Hyperkeratosis | -Genetic disorder Zinsser-Cole-Engman syndrome | Young age |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khamis, A.; Salzer, L.; Schiegnitz, E.; Stauber, R.H.; Gül, D. The Magic Triangle in Oral Potentially Malignant Disorders: Vitamin D, Vitamin D Receptor, and Malignancy. Int. J. Mol. Sci. 2023, 24, 15058. https://doi.org/10.3390/ijms242015058
Khamis A, Salzer L, Schiegnitz E, Stauber RH, Gül D. The Magic Triangle in Oral Potentially Malignant Disorders: Vitamin D, Vitamin D Receptor, and Malignancy. International Journal of Molecular Sciences. 2023; 24(20):15058. https://doi.org/10.3390/ijms242015058
Chicago/Turabian StyleKhamis, Aya, Lara Salzer, Eik Schiegnitz, Roland H. Stauber, and Désirée Gül. 2023. "The Magic Triangle in Oral Potentially Malignant Disorders: Vitamin D, Vitamin D Receptor, and Malignancy" International Journal of Molecular Sciences 24, no. 20: 15058. https://doi.org/10.3390/ijms242015058
APA StyleKhamis, A., Salzer, L., Schiegnitz, E., Stauber, R. H., & Gül, D. (2023). The Magic Triangle in Oral Potentially Malignant Disorders: Vitamin D, Vitamin D Receptor, and Malignancy. International Journal of Molecular Sciences, 24(20), 15058. https://doi.org/10.3390/ijms242015058