1. Introduction
Brugada syndrome (BrS) is a rare heritable form of cardiac arrhythmia, which often clinically manifests itself with syncope or (resuscitated) cardiac arrest due to either polymorphic ventricular tachycardia (VT) or ventricular fibrillation (VF). Typically, these clinical situations occur at night or at rest in young adults without cardiac structural abnormalities [
1]. BrS is characterized by a coved-type ST-segment elevation in the right precordial leads V1 through V3 of the electrocardiogram (ECG) and an increased risk of sudden cardiac death (SCD) [
2]. With an estimated variable prevalence of 0–0.1% in Europe/USA and 0–0.94% in Southeast Asia, where it is the leading cause of death in apparently healthy young men, BrS is responsible for 4% of all SCDs and up to 12% of sudden death worldwide in individuals with structurally normal hearts [
3,
4]. BrS has a complex physiopathology and cannot be defined as a monogenic disease [
5,
6]. Nevertheless, the sodium voltage-gated channel 5A (
SCN5A) gene, which encodes the pore-forming α-subunit of the cardiac voltage-gated sodium channel Nav1.5, was the first gene to be associated with BrS in 1998 by Chen and colleagues [
7]. Since then, rare variants of more than 20 other genes have been found in BrS patients, but loss-of-function mutations of Nav1.5 still account for 20% to 30% of all genetically diagnosed BrS cases [
8,
9].
SCN5A was also recently assessed as the only undisputed BrS-related gene by the Clinical Genome Resource initiative, while all the other genes were reclassified as disputed [
10]. Nav1.5 is the molecular determinant of the inward sodium current (I
Na) in the heart and underlines the fast depolarization of the cardiac action potential of working myocytes in both the atria and the ventricles [
11]. To date, more than 300 Nav1.5 BrS-related mutations have been described, localized throughout the whole protein structure, and associated with a broad spectrum of disease severity [
1,
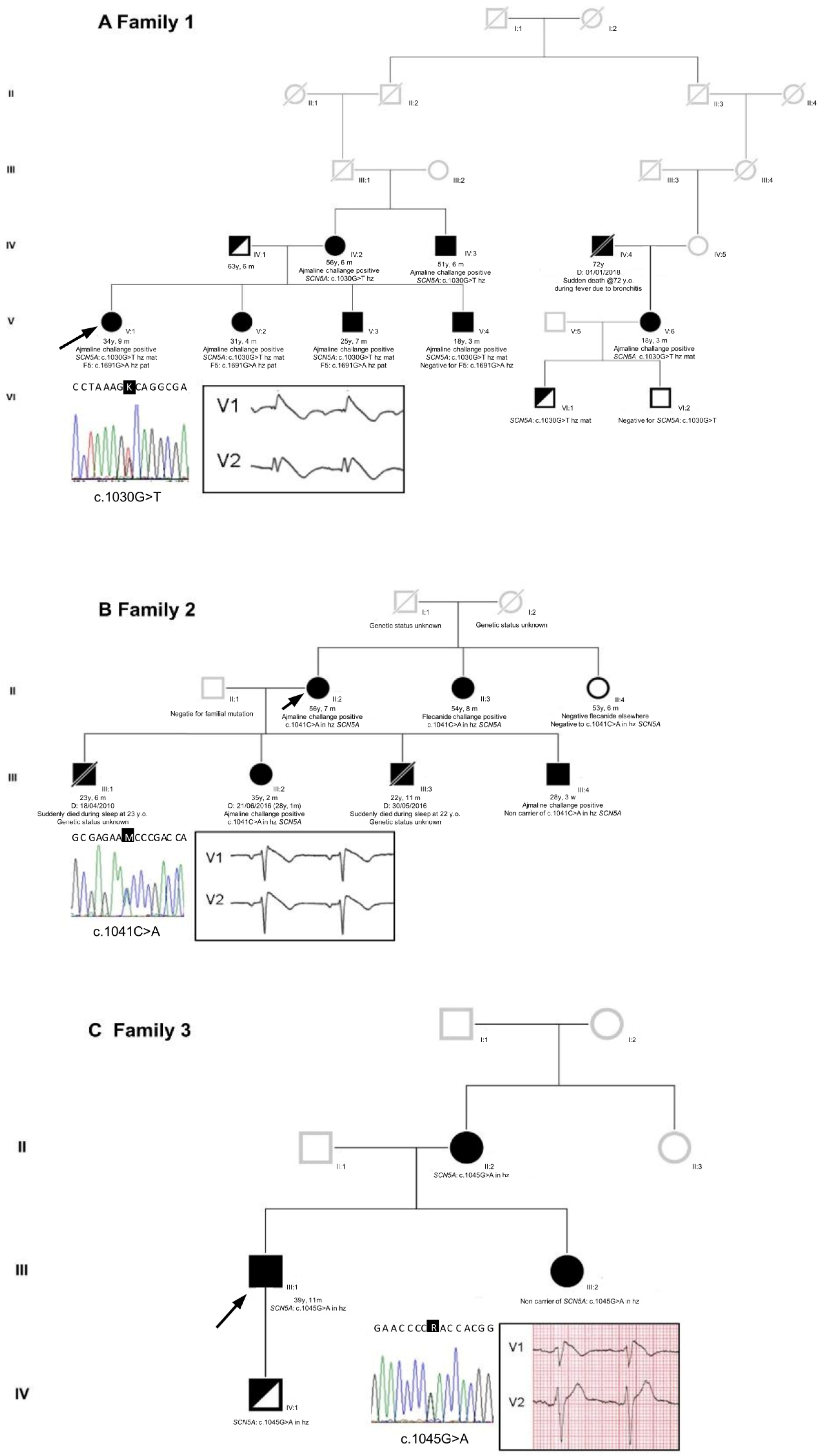
12]. Here, we identified and functionally characterized three novel
SCN5A missense mutations, namely c.1030 G>T (p.A344S), c.1041 C>A (p.N347K), and c.1045 G>A (p.D349N), found in three unrelated BrS patients and their relatives. Given the loss-of-function effect revealed from the patch clamp approach, the effect of chronic exposure to mexiletine was challenged to explore the possibility of a functional rescue. Finally, as all the three mutations are located within the P-loop comprised between the S5 and S6 segments of domain I of the channel, we inquired into their structural significance, shedding lights on these residues’ roles in Nav1.5 and their potential impact on channel function.
3. Discussion
From a clinical viewpoint, in the context of BrS, the three families described in this work are heterogeneous and present several possibilities. Family 1 is quite large, and all the seven members harboring the c.1030G>T (p.A344S) mutation tested positive for ajmaline, revealing complete penetrance. Notably, the ajmaline challenge has not been performed yet/has still to be performed on one pediatric carrier (the son of the proband’s third-grade cousin).
Concerning the c.1041C>A (p.N347K) mutation, as already reported by our group [
18], our data indicate that one BrS patient within the family does not carry the mutation. Given the maternal inheritance of the c.1041C>A mutation in the
SCN5A gene, it is possible that this specific mutation is not the one and only cause of BrS in this family. Therefore, it can be speculated that BrS might be caused by a different mutation only in this family member (for example, via a de novo mutation) or that c.1041C>A acts as a genetic modifier, able to worsen the clinical presentation of Brugada in all carriers. At the moment, the
SCN5A c.1041C>A mutation is the only mutation that has been found in this family, considering the panel of 37 genes described in the literature regarding BrS.
Regarding the c.1045G>A (p.D349N) mutation, as also reported previously [
18], the family is small with a confirmed pattern of inheritance. Unfortunately, the son of the proband, positive for the presence of the mutation, is not keen to collaborate for further analysis.
It is therefore evident that the genotype–phenotype correlation among BrS patients is challenging, due to both its variability and clinical behavior. Another source of complexity is the attribution of pathogenicity, even in the case of the SCN5A variants, partially due to the oligogenic inheritance of BrS. Certainly, the genetic test can be beneficial for risk stratification among probands and family members, but the relevance of common variants cannot be underestimated. Thus, it is important to remark that not all the cases of BrS are caused by SCN5A mutations, and that the genetic incomplete penetrance does not completely rule out the relation between a mutation and the syndrome.
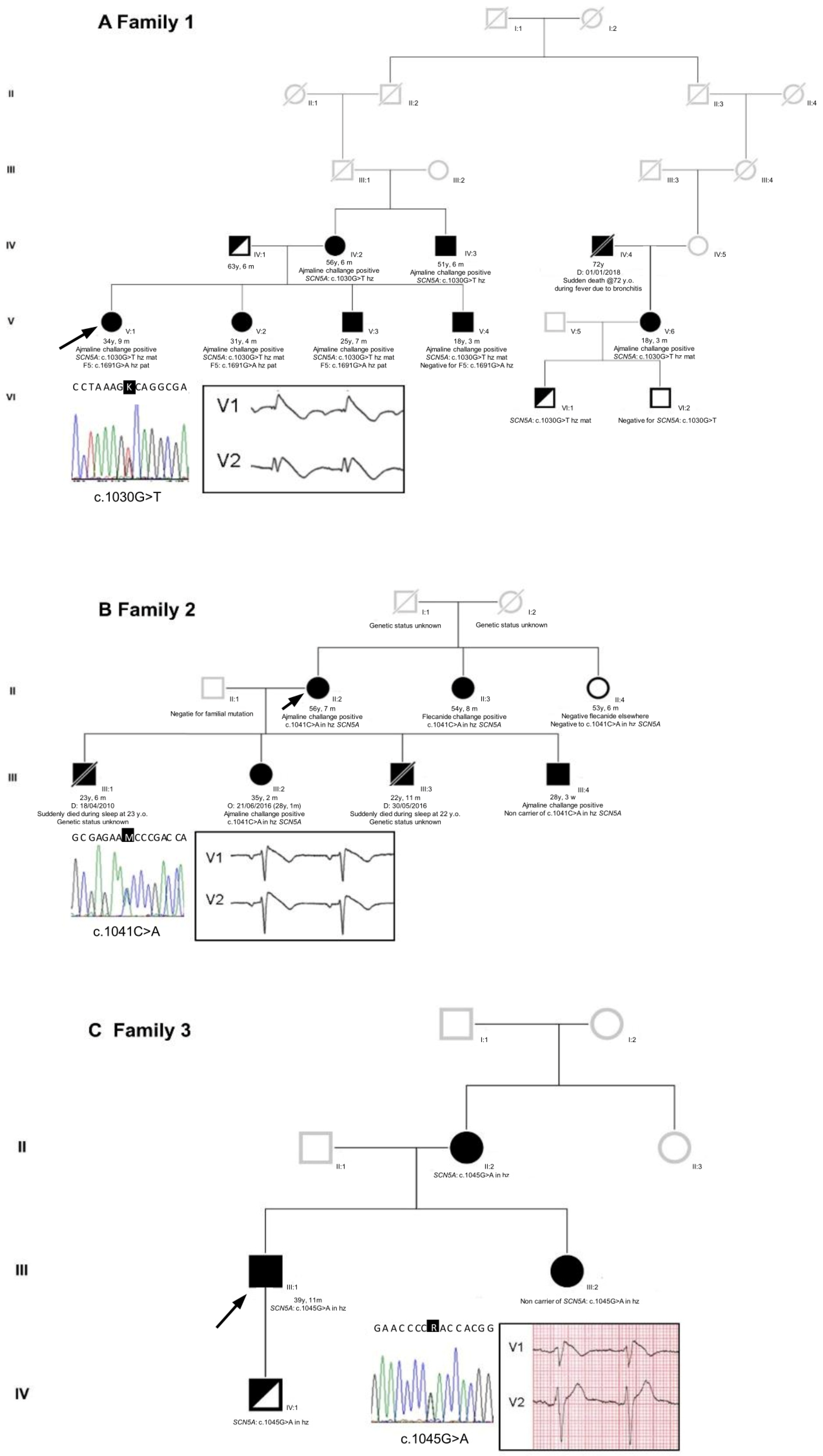
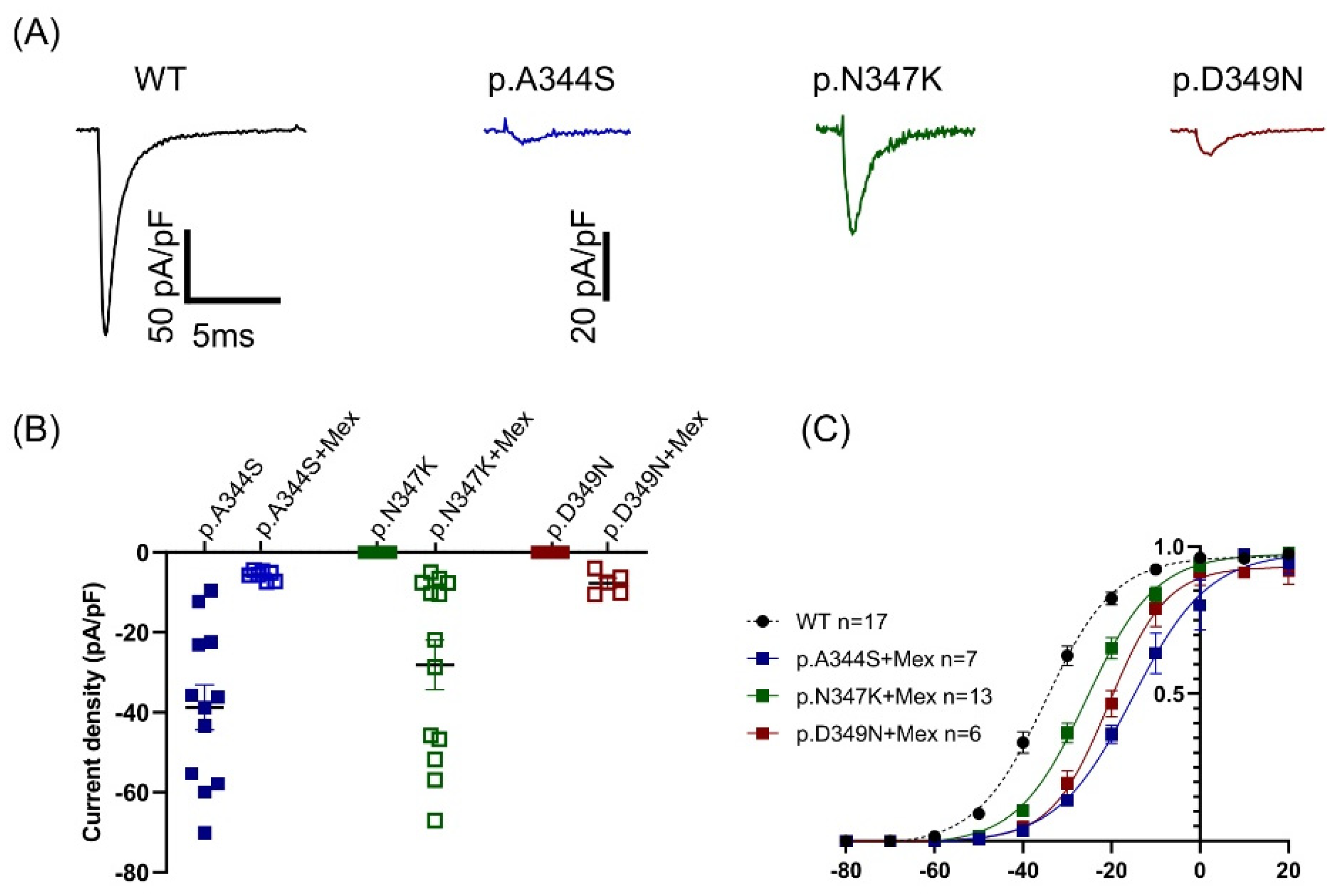
These clinical cases represented the opportunity to shed light on the biophysical and structural features of three novel mutations in Nav1.5 located very close to each other (positions p.344, p.347, and p.349). All of them resulted in a loss-of-function of the channel, in which the predominant effect is the reduction (p.A344S)/abolishment (p.N347K and p.D349N) of the I
Na, without showing a dominant-negative effect. Other biophysical properties, such as the subtle shift (4–5 mV) in the activation or inactivation curves, and the slowing in the kinetics of the fast inactivation process, could be quantitatively considered as less relevant. Notably, the three mutations fall in a region of the channel that is part of the P loop of domain I. This region extends from the aminoacidic residue p.M273 to p.S357, but already in the range between p.R340 and p.D356 (twenty-one residues long), five more mutations have been described (p.R340Q [
19], p.G351V [
17], p.G351D [
8], p.T353I [
20,
21], and p.D356N [
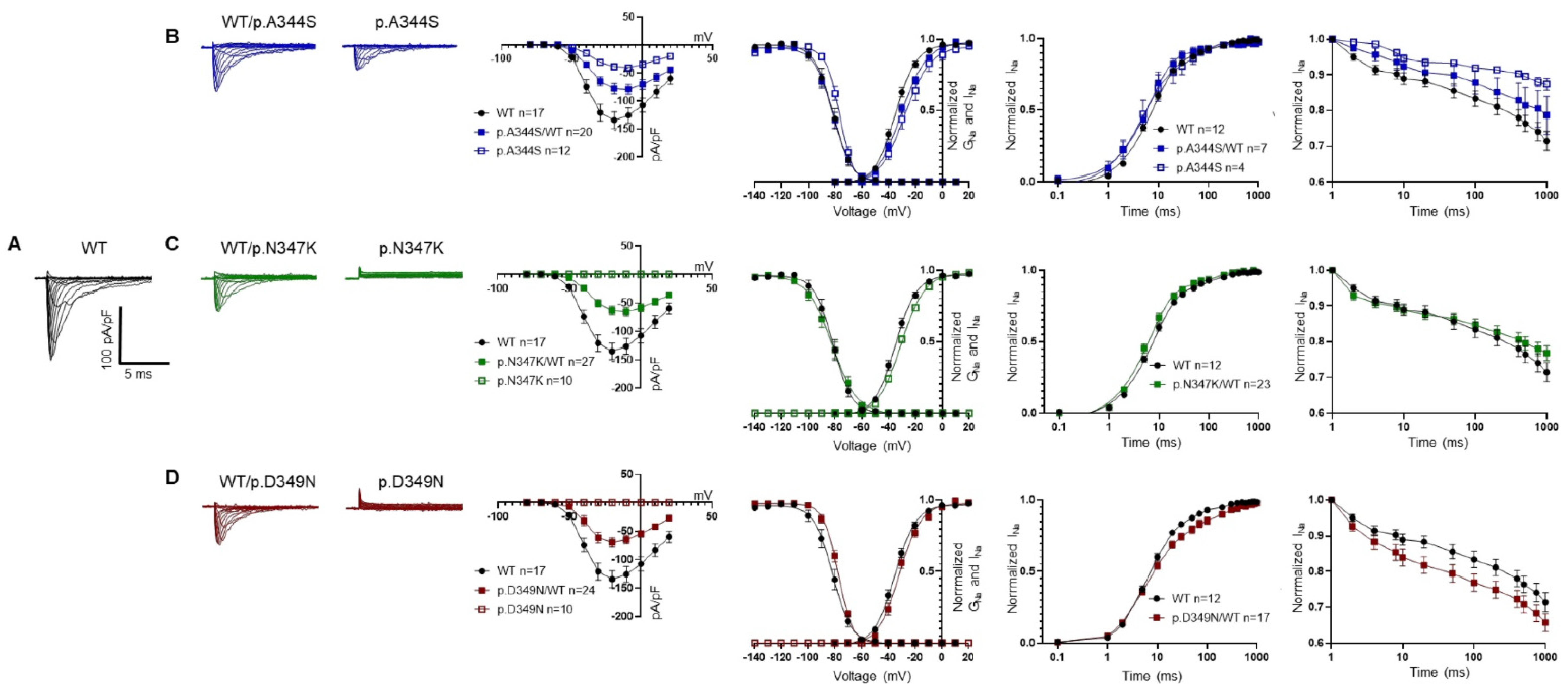
22]), suggesting its relevant role in the protein’s function and a possible mutational hot spot. All but one (p.R340Q) resulted in a protein loss-of-function, that most of the time, once again, corresponded to a significant reduction/abolishment in the current density. This effect is not surprising, since these mutations have been related to the BrS phenotype. The reduction in the current density has often been attributed to a trafficking defect. However, this assumption is questionable in the case of the three novel mutations we have described, as confocal images indicated the presence of the Nav1.5 channel on the plasma membrane. Despite the fact that it is important to recall the interpretive limitations associated with an image acquired through confocal microscopy (the analysis, in fact, remains only semi-quantitative, and even though the channel is visible in the plasma membrane, the possibility that the level of expression might be significantly diminished compared to the wild-type channel cannot be disregarded), such a result allowed for a deeper consideration in terms of the mechanism underlying the observed loss-of-function. In fact, p.A344S has the mildest effect on the Na
+ channel’s current; a behavior similar to the one published for p.C335R and p.P336L [
19,
23], which precede it in sequence. On the other hand, for both p.N347K and p.D349N, probably due to their deeper positions and their interactions, the effect is more profound, as also suggested by the score assigned via the in silico prediction. In fact, in these two constructs, the inward current was completely absent, as it was described for the closely located p.G351-, p.T353-, and p.D356-mutated residues [
8,
17,
20,
21,
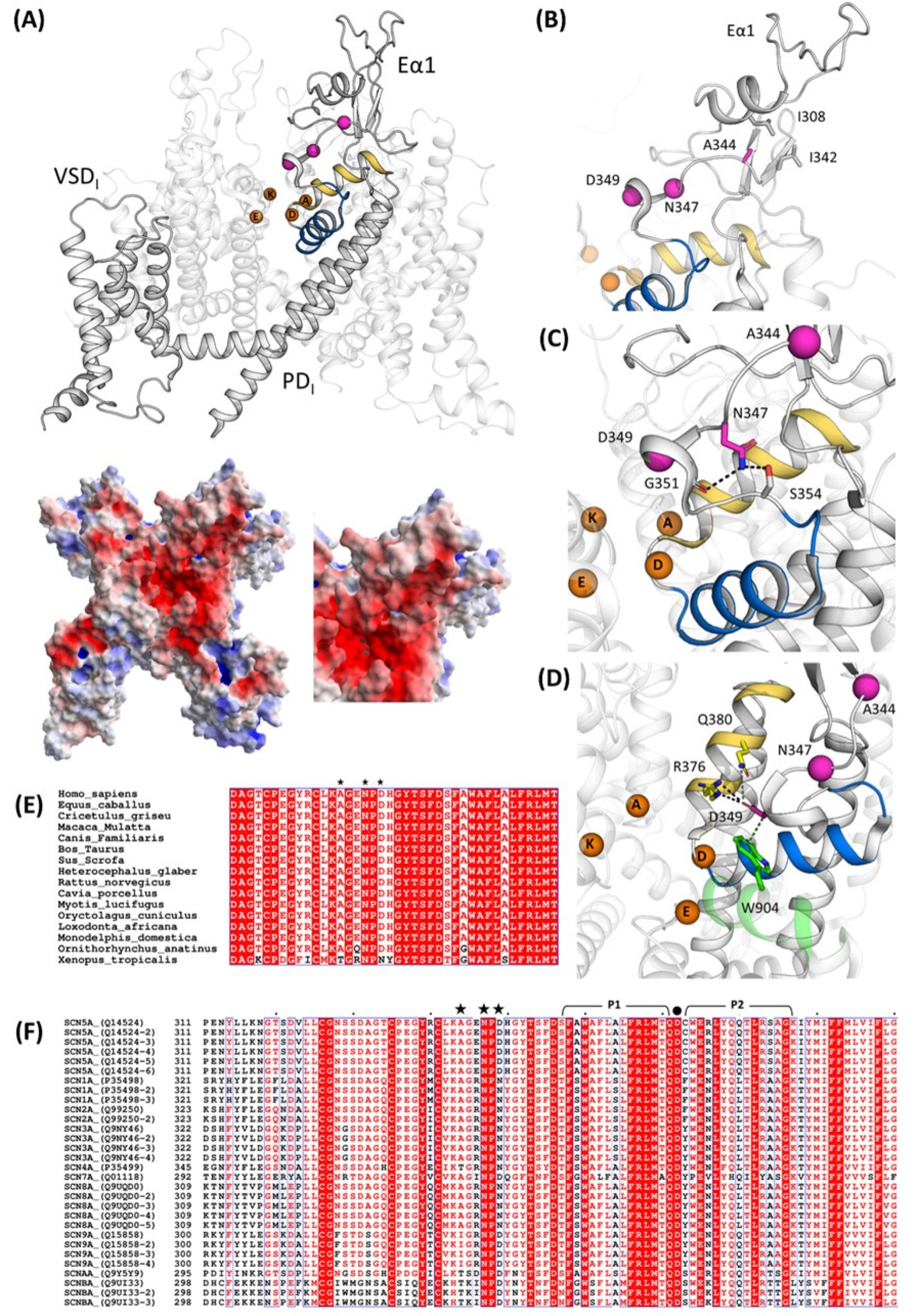
22]. Indeed, the structural analysis suggested that the position p.A344, being more external, is quite far from the selectivity filter, while p.N347 is located deeper in the funnel-like region of the channel, and the introduction of a positive charge (K) may impair the correct orientation of the selectivity filter and of the two helices supporting the pore (the P1-SF-P2 motif). Finally, the p.D349 residue is in very close proximity to the selectivity filter, and, with its network of interactions, concurs to correctly place two out of four elements of the DEKA filter. Moreover, again, being part of a negative area, its substitution with a residue with an uncharged polar side chain (from D to N) may affect such a network and account for the dramatic effect. Thus, in general, and specifically for the p.A344S mutation, it cannot be excluded that the reduction in the current density may be explained via a decreased expression level at the plasma membrane (although no data are available at the moment); for the other two mutations, the destabilization of the selectivity filter seems to be one more aspect to be considered among the causes of the abolishment of the sodium current, despite the presence of the channel at the membrane.
Another interesting issue is related to the role of mexiletine in rescuing channel function. Mexiletine, classified as a class Ib antiarrhythmic drug, has been recognized for its binding to Nav1.5 channels at a local anesthetic-binding site within the fourth homologous domain’s sixth transmembrane segment. Beyond its use-dependent sodium channel blocking capability, it is also considered a pharmacological chaperone. Notably, mexiletine exhibits a certain level of tonic block, gauged as a first-pulse block, before close-state inactivation [
24]. This implies an inherent affinity of mexiletine for the local anesthetic receptor site and, more broadly, for Nav1.5 channels, that may account for its escort activity. In this view, mexiletine’s contribution to the recovery of the I
Na is related to its capacity for inducing a conformational shift in misfolded channels that will appear normal to the quality control mechanism, thus permitting export from the endoplasmic reticulum (ER) and restoring membrane trafficking. The same impact on trafficking has not only been proposed for just Nav1.5 channels, but also to the hHERG channel and its blockers, which hinder anterograde channel delivery or facilitate rescue surface expression [
25,
26]. Regarding mexiletine’s application, a previous paper reported concentrations ranging from 10 µM (within clinical levels) to 500 µM that have been employed for 24–48 h of in vitro incubation. While not all mutations respond positively to this drug [
27], those that do are located in different portions within the channel. They may be situated within a transmembrane helix, P-loop, linker between domains, or the C-terminus of the protein [
13,
28,
29]. Notably, peak current recovery might coincide with significant shifts towards more negative potentials for both activation and inactivation voltage dependencies [
13]. In contrast, for the first time, the p.A344S mutation demonstrated an 85% mexiletine-dependent peak current reduction, possibly linked to a 20 mV rightward shift in the activation curve. In contrast, the mutations p.N347K and p.D349N showcased the expected current recovery, similar to the effects seen with p.V1378M and p.G1743R, which are located in comparable positions between S5 and S6 of the third and fourth domains, but, again, with a positive shift in the gating properties [
27,
30]. It is also remarkable that p.N347K and p.D349N Nav1.5 were present on the cell membrane, despite the absence of an inward current, indicating a dysfunctional rather than completely impaired trafficking channel. A plausible rationale for the mexiletine-driven rescue is its potential to stabilize the selectivity filter’s position within the protein and counteract mutation-induced conformational alterations. However, translating this pharmacological in vitro rescue into a mutation-specific pharmacotherapy necessitates further exploration. Yet, the activation curve shift resulting from prolonged mexiletine exposure may pose risks of window current alterations, potentially affecting the action potential’s repolarization phase. Thus, paraphrasing the results obtained in this study, by treating the mutated channels for a considered chronic duration, the therapeutic intervention should be led by the consideration of which effect is prevalent, and the question that the clinician would be able to answer is: is the current density rescued by mexiletine enough to sustain phase 0 of the action potential, and thus the action potential upstroke velocity, but still not enough to alter the window current (that typically involves a minor fraction of the non-inactivated Nav1.5 channels)? In other words, is it possible to establish a threshold for the safety and efficacy of certain drugs among BrS patients in correlation with the presence of
SCN5A mutations? The answer may avoid potentially harmful consequences [
28].
Limitations of the Study
While the presented study has shed light on the role of SCN5A mutations in BrS, we acknowledge limitations stemming from a relatively small patient cohort. Expanding genetic sequencing to encompass a broader range of genes and a more diverse BrS patient population is crucial. This approach promises deeper insights into the clinical significance of SCN5A mutations, potential genotype–phenotype correlations, and a more comprehensive understanding of BrS genetics. Due to BrS’s genetic complexity, we recognize the need for a broader multi-genomic exploration to uncover additional gene mutations or disease-associated factors. This comprehensive approach is essential for a more holistic understanding of BrS pathogenesis.
Moreover, our current research primarily relies on cellular and molecular studies. The incorporation of BrS animal models or induced pluripotent stem cell (iPSC)-derived cardiomyocytes in these kind of studies would enhance the validation of the impacts of specific mutations or therapeutic interventions within a more intricate biological system. These models can provide valuable in vivo and functional data, bridging the gap between genetic findings and their clinical implications.
Finally, in terms of deciphering the functional implications of mutations at the atomic level, experimental techniques, like X-ray crystallography and cryo-electron microscopy (cryo-EM), primarily provide the atomic coordinates of a protein’s structure. Of course, each approach has its own strengths and weaknesses: X-ray crystallography provides high-resolution structures, but requires protein crystallization, which can be difficult for some samples; cryo-EM offers high-resolution imaging and versatility, but the preparation of samples can be technically challenging, and there is a risk of generating structural artifacts or sample damage during the process. Electrostatic potential calculations, in spite of being limited by approximations, are computationally efficient and relatively fast; they provide enough information, and are cost-effective compared to our experimental methods; thus, they are useful for initial structural assessments and screening.
4. Materials and Methods
4.1. Subjects
Patients and relatives were evaluated in our Department of Arrhythmology and Electrophysiology at the hospital Policlinico San Donato. This study was conducted in accordance with the Declaration of Helsinki and written informed consent of human subjects was obtained for their participation in the study and for publication. The procedures employed were reviewed and approved by the local Ethics Committee (approver number: M-EC-006/A, rev. 1 March 2013).
4.2. DNA Extraction and Genetic Analysis
Genomic DNA was extracted from the peripheral blood of the probands and relatives using the Maxwell 16 Blood DNA Purification kit (Promega Italia, Milan, Italy). Their quality and concentration were determined using Nanodrop and Qbit (Thermo Fisher Scientific Italia, Monza, Italy). The samples were enriched using the Tru Sight One Sequencing kit (Clinical exome, Illumina, San Diego, CA, USA) and sequenced on the NextSeq500 platform (Illumina). The sequences were analyzed according to GATK Best Practice criteria, exploiting pipelines based on BWA, the Smith–Waterman algorithm, freebayes, SnpSift-SnpEFF, and BaseSpace Onsite. The next-generation sequencing (NGS) panel was only used for the three probands of each family, while all other family members were studied with Sanger sequencing. This panel contained 37 genes that have been described in the BrS research literature (ABCC9, ACTC1, AKAP9, CACNA1C, CACNA2D1, CACNB2, DSC2, DSG2, DSP, FLNC, GPD1L, HCN4, JUP, KCND2, KCND3, KCNE1L, KCNE3, KCNE5, KCNH2, KCNJ8, MOG1/RANGRF, MYBPC3, MYH7, MYL2, MYL3, PKP2, PLN, SCN10A, SCN1B, SCN2B, SCN3B, SCN5A, SEMA3A, TNNI3, TNNT2, TPM1, and TRPM4). The mean coverage of the sequenced regions was 123×. The analyzed regions covering <20× include the regions 91708393–91708423 (chromosome 7, gene AKAP9, transcript NM_005751), 2791187–2191220 (chromosome 12, gene CACNA1C, transcript NM_199460), and 150644885–150644904 (chromosome 7, gene KCNH2, transcript NM_000238).
4.3. Plasmid Generation
Wild-type (WT) SCN5A complementary DNA (cDNA) was subcloned into the pcDNA3.1 plasmid, with a tandem twin Strep tag and FLAG tag at the N terminus of Nav1.5. The mutations were engineered via site-directed mutagenesis through the QuikChange II site-directed mutagenesis kit (Agilent Technologies Italia, Milan, Italy), according to the manufacturer’s instructions. The oligonucleotides used for the three mutations were: c.1030 G>T, forward 5′-GCTACCGGTGCCTAAAGTCAGGCGAGAACC-3′, reverse 5′-GGTTCTCGCCTGACTTTAGGCACCGGTAGC-3′; c.1041 C>A, forward 5′-AAAGGCAGGCGAGAAACCCGACCACGGCTAC-3′, reverse 5′-GTAGCCGTGGTCGGGTTTCTCGCCTGCCTTT-3′; and c.1045 G>A, forward 5′- CAGGCGAGAACCCCAACCACGGCTACACC-3′, reverse 5′-GGTGTAGCCGTGGTTGGGGTTCTCGCCTG-3′. Sanger sequencing was then performed to confirm the accurate incorporation of the mutation and validate the sequence’s integrity. The SCN1B gene, which encodes for the human cardiac β1 subunit, was inserted into a pIRES vector that was engineered to contain EGFP as a reporter gene (a kind gift from Prof. Hugues Abriel, University of Bern, Bern, Switzerland).
4.4. Cell Culture and Transfection
The HEK293 (human embryonic kidney 293) cell line was obtained from ATCC. Cells were cultured in a controlled environment (5% CO
2, 37 °C) and maintained in an appropriate medium (DMEM/F12; Gibco-Thermo Fisher Scientific Italia, Monza, Italy) supplemented with 10% fetal bovine serum (FBS, FBS; Sigma-Aldrich—Merk Life Science, Milan, Italy), 2 mM L-Glutamine, 100 U/mL, and 100 μg/mL Pen/Strep (Euroclone, Pero, Italy). Equal amounts of
SCN5A (0.5 µg, WT or mutant channel) and
SCN1B subunits cDNA (1:1 ratio) were transiently transfected using the jetPRIME reagent (PolyPlus transfection, Euroclone, Pero, Italy), according to the manufacturer’s instructions. In order to mimic the genetic balance of affected individuals, 0.25 µg of the WT and 0.25 µg of the variant alpha subunit-encoding plasmid, as well as 0.5 µg of the beta 1 subunit, were co-transfected (0.5:0.5:1 ratio). Following this step, 48 h after transfection, the cells were dispersed using a trypsin/EDTA solution (Gibco-Thermo Fisher Scientific Italia, Monza, Italy), gently centrifuged at room temperature (RT) at a speed of 200×
g for 5 min, and resuspended. For experiments focused on the rescue of the I
Na, transfected cells were incubated overnight with mexiletine (mexiletine hydrochloride, Sigma-Aldrich - Merk Life Science, Milan, Italy ) at a concentration of 0.1 mM [
20].
4.5. Functional Analysis
4.5.1. Automated Patch Clamp
Automated patch clamp recordings were performed at room temperature (RT) using the Nanion Patchliner platform (Nanion Technologies, Munich, Germany). The transfected cells, after dispersion in trypsin and centrifugation, were then resuspended in an external solution at a final concentration of 500,000 cells/mL. The cells were allowed to recover at 4 °C for 20 min before proceeding with the automated recordings. According to company recommendations, single-hole medium resistance (1.8–3 MΩ) NPC-16 chips were used to record the Na
+ current. Pulse generation and data collection were performed using PatchControl v3.01.19 (Nanion Technologies, Munich, Germany ) and PatchMaster v2X92 (Heka, Multi Channel Systems MCS GmbH, Reutlingen, Germany) software. Whole-cell currents were filtered at 10 KHz, the sampling rate was set to 20 µs, and series resistances were automatically compensated. The external recording solution contained (mM): 80 NaCl, 60 NMDG, 4 KCl, 2 CaCl
2, 1 MgCl
2, 5 D-Glucose monohydrate, and 10 Hepes, (pH 7.4 with HCl, osmolarity adjusted to 289 mOsm/Kg). The internal solution was composed of the following (mM): 110 CsF, 10 NaCl, 10 CsCl, 10 Hepes, and 10 EGTA (pH 7.2 with CsOH, osmolarity > 280 mOsm/kg). To achieve high-resistance seals, a seal enhancer solution was added, containing (mM): 80 NaCl, 60 NMDG, 4 KCl, 10 CaCl
2, 1 MgCl
2, 5 D-Glucose monohydrate, and 10 Hepes, (pH 7.4 with HCl, osmolarity adjusted to 313 mOsm/Kg). The holding potential was −120 mV. Steady-state activation was studied pulsing from −80 mV to +20 mV (+5 mV increments, 25 ms duration), while the steady-state inactivation protocol had an initial 500 ms duration step (from −140 mV to +10 mV, increments of +10 mV), followed by a −10 mV test pulse (20 ms durations). Steady-state activation and availability curves were fitted with a Boltzmann function: y = 1/(1 + exp((V − V
1/2)/k)), where y is the relative current, V is the membrane potential, V
1/2 is the half-maximal voltage, and k is the slope factor. The onset of the fast inactivation process was studied, fitting the decay of the peak current traces elicited by a 25 ms depolarizing pulse from −120 to +20 mV with a bi-exponential function (the data in
Table 1 only show the value of the τ fast @ −20 mV).
4.5.2. Manual Patch Clamp
After dispersion with trypsin and centrifugation, the cells were plated onto 35 mm plastic Petri dishes and used for whole-cell patch clamp experiments a few hours later to allow attachment. Voltage clamp experiments were conducted at RT, and only GFP-expressing (green) cells were selected for recording. The internal and external solutions used for the recordings were the same solutions that were adopted for automated patch clamp analysis. Borosilicate glass patch pipettes (2–3 MΩ) were pulled with a P-1000 Flaming-Brown micropipette puller (Sutter Instrument). Series resistance (Rs) were compensated, and the compensation was readjusted before each protocol. Recovery from inactivation was studied through a two-step protocol at −10 mV (500 ms and 20 ms duration, respectively), separated by a −120 mV pulse of increasing duration from 0.1 ms to 1 s. Also, the time dependence of the onset of intermediate and slow inactivation was measured with a two-pulse protocol: the first pulse, P1, stepped from the holding potential of −120 mV to −20 mV (increasing duration from 1 to 1000 ms), followed by a step back to −120 mV for 20 ms to let the channels recover from the fast inactivation, and the second pulse, P2, to −20 mV (duration 20 ms) enables the recording of the sodium current. The resulting P2/P1 ratio was normalized and plotted against the P1 duration [
31,
32]. Data were acquired with a Multiclamp 700B amplifier and Digidata 1550B and pClamp 10.3 software, and analyzed with Clampfit 10.7 software (all Axon Instruments, Molecular Devices, San Jose, CA, USA).
4.5.3. Statistical Analysis
Functional data are presented as the mean ± SEM of at least three independent experiments; n denotes the number of cells. A two-way ANOVA was performed for multiple comparisons, followed by a modified t-test with Fisher’s correction (OriginPro 8; OriginLab Corporation, Northampton, MA, USA ). Values of p < 0.05 were considered significant, and indicated with * or # in the figures and table.
4.6. Immunofluorescence Staining
For the immunofluorescence staining experiments, the SCN1B gene was subcloned in a pCDNA3.1 vector devoid of the GFP reporter gene in order to prevent the overlapping fluorescence of the GFP and the secondary antibody used. HEK293 cells were plated on a glass slide coated with gelatin 0.1% in PBS; following this step, 48 h after transfection, they were fixed using PFA 4% in PBS for 15 min at RT. Three washes of 5 min each at RT in PBS high salt buffer (PBS-HS) were performed. Before antibody staining, the cells were incubated with the permeabilization solution (gelatin 0.4% Triton X-100 0.6%, phosphate buffer 40 mM, NaCl 0.9 M, and saponin 0.1%) for 15 min at RT. Two washes were then conducted with the PBS-HS solution. The non-specific binding sites of the primary antibody were blocked with PBS + 0.5% bovine serum albumin (BSA) for 1 h at RT. The excess was removed with two 5 min washes in PBS-HS. The cells were incubated with permeabilization buffer (20 mM PBS pH 6.8, 2% gelatin, 0.1% Triton X-100 solution, 0.45 mM NaCl, 1% albumin, and 0.1% saponin) for 15 min at RT. The primary (Anti.Nav1.5 Rabbit monoclonal antibody, Cell Signaling Europe, Leiden The Netherlands, Catalogue # 14421, diluted 1:400) and secondary (Donkey Anti-rabbit Alexa Fluor 488, Thermo Fisher Scientific Italia, Monza, Italy, Catalogue # A-21206, diluted 1:600) antibodies were incubated overnight (o/n) at 4 °C, and for 1 h at RT in the dark, respectively, in permeabilization solution. The excess antibodies were then removed with two washes (5 min, RT) in PBS-HS and two washes in PBS low salt (LS). The slides were coverslipped with DAKO fluorescence mounting medium. The Zeiss LSM710 confocal microscope, equipped with a 63× oil immersion objective, was used for image acquisition as a single optical section. Zeiss ZEN Microscope Lite software version and ImageJ 1.48V were used for image processing.
4.7. Structural Analysis
Nav1.5 structural data were retrieved from wwPDB (PDB ID: 7DTC, 6LQA). Electrostatic potential calculations and figures were generated using PyMOL (Schrödinger, LLC, Munich, Germany. The PyMOL Molecular Graphics System, Version 2.5.6). The electrostatic potential was calculated using the Adaptive Poisson–Boltzmann Solver (APBS) method [
33]. The sequences of human SCN genes (UniProt accession No. P35498, P35499, Q01118, Q14524, Q15858, Q99250, Q9NY46, Q9UI33, Q9UQD0, and Q9Y5Y9) were retrieved from UniProt and aligned in MEGA 11 [
34] using the MUSCLE algorithm [
35]. The multiple sequence alignment presented (
Figure 5) was generated with ESPript [
36].

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}