
High Filamin a Expression in Adrenocortical Carcinomas Is Associated with a Favourable Tumour Behaviour: A European Multicentric Study

 , , , ,
, , , ,  , , , ,
, , , ,  ,
,  ,
,  ,
,  , ,
, ,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
2. Results
2.1. Demographic, Clinical, and Histopathological Data
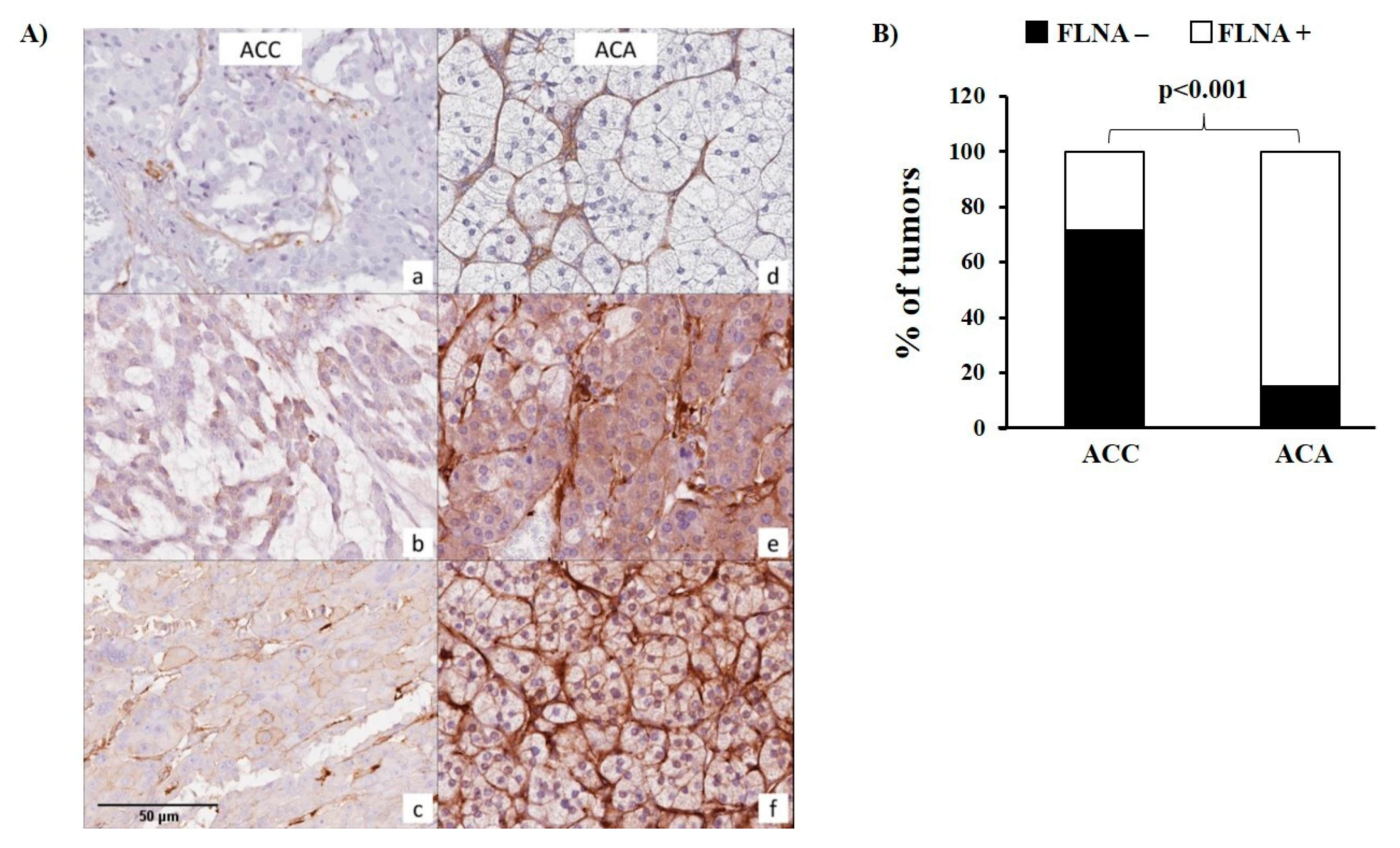
2.2. FLNA Expression in ACC and ACA
2.3. Association between the FLNA Expression and the Clinicopathological Features of ACCs
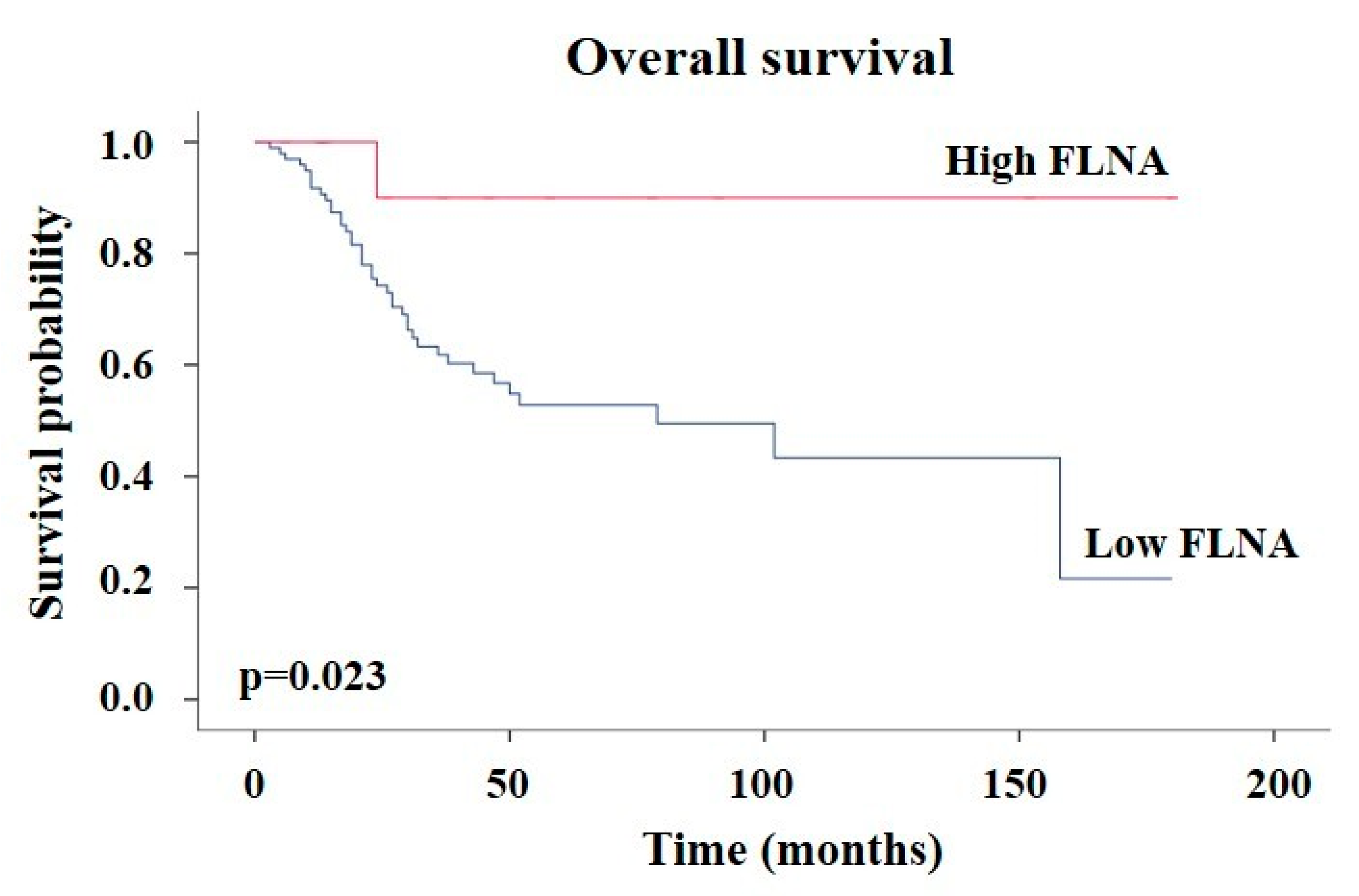
2.4. Association between FLNA Expression and the Clinical Outcome of ACCs
3. Discussion
4. Materials and Methods
4.1. Patients and Data Collection
4.2. Immunohistochemistry
4.3. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weiss, L.M. Comparative histologic study of 43 metastasizing and nonmetastasizing adrenocortical tumors. Am. J. Surg. Pathol. 1984, 8, 163–169. [Google Scholar] [CrossRef]
- Mizdrak, M. The Role of Biomarkers in Adrenocortical Carcinoma: A Review of Current Evidence and Future Perspectives. Biomedicines 2021, 9, 174. [Google Scholar] [CrossRef]
- Jain, M.; Zhang, L.; He, M.; Zhang, Y.-Q.; Shen, M.; Kebebew, E. TOP2A is overexpressed and is a therapeutic target for adrenocortical carcinoma. Endocr. Relat. Cancer 2013, 20, 361–370. [Google Scholar] [CrossRef]
- Fassnacht, M.; Allolio, B. Clinical management of adrenocortical carcinoma. Best. Pract. Res. Clin. Endocrinol. Metabol. 2009, 23, 273–289. [Google Scholar] [CrossRef]
- Crona, J.; Beuschlein, F. Adrenocortical carcinoma—Towards genomics guided clinical care. Nat. Rev. Endocrinol. 2019, 15, 548–560. [Google Scholar] [CrossRef]
- Fassnacht, M.; Johanssen, S.; Quinkler, M.; Bucsky, P.; Willenberg, H.S.; Beuschlein, F.; Terzolo, M.; Mueller, H.; Hahner, S.; Allolio, B.; et al. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: Proposal for a revised TNM classification. Cancer 2009, 115, 243–250. [Google Scholar] [CrossRef]
- Beuschlein, F.; Weigel, J.; Saeger, W.; Kroiss, M.; Wild, V.; Daffara, F.; Libé, R.; Ardito, A.; Al Ghuzlan, A.; Quinkler, M.; et al. Major Prognostic Role of Ki67 in Localized Adrenocortical Carcinoma After Complete Resection. J. Clin. Endocrinol. Metab. 2015, 100, 841–849. [Google Scholar] [CrossRef]
- Lippert, J.; Appenzeller, S.; Liang, R.; Sbiera, S.; Kircher, S.; Altieri, B.; Nanda, I.; Weigand, I.; Gehrig, A.; Steinhauer, S.; et al. Targeted Molecular Analysis in Adrenocortical Carcinomas: A Strategy Toward Improved Personalized Prognostication. J. Clin. Endocrinol. Metab. 2018, 103, 4511–4523. [Google Scholar] [CrossRef]
- Elhassan, Y.S.; Altieri, B.; Berhane, S.; Cosentini, D.; Calabrese, A.; Haissaguerre, M.; Kastelan, D.; Fragoso, M.C.B.V.; Bertherat, J.; Al Ghuzlan, A.; et al. S-GRAS score for prognostic classification of adrenocortical carcinoma: An international, multicenter ENSAT study. Eur. J. Endocrinol. 2021, 186, 25–36. [Google Scholar] [CrossRef]
- Lippert, J.; Dischinger, U.; Appenzeller, S.; Prete, A.; Kircher, S.; Skordilis, K.; Elhassan, Y.S.; Altieri, B.; Fassnacht, M.; Ronchi, C.L. Performance of DNA-based biomarkers for classification of adrenocortical carcinoma: A prognostic study. Eur. J. Endocrinol. 2023, 189, 262–270. [Google Scholar] [CrossRef]
- Altieri, B.; Colao, A.; Faggiano, A. The role of insulin-like growth factor system in the adrenocortical tumors. Minerva Endocrinol. 2019, 44, 43–57. [Google Scholar] [CrossRef]
- Gicquel, C.; Bertagna, X.; Schneid, H.; Francillard-Leblond, M.; Luton, J.P.; Girard, F.; Le Bouc, Y. Rearrangements at the 11p15 locus and overexpression of insulin-like growth factor-II gene in sporadic adrenocortical tumors. J. Clin. Endocrinol. Metab. 1994, 78, 1444–1453. [Google Scholar] [CrossRef]
- Gicquel, C.; Raffin-Sanson, M.-L.; Gaston, V.; Bertagna, X.; Plouin, P.-F.; Schlumberger, M.; Louvel, A.; Luton, J.-P.; Le Bouc, Y. Structural and functional abnormalities at 11p15 are associated with the malignant phenotype in sporadic adrenocortical tumors: Study on a series of 82 tumors. J. Clin. Endocrinol. Metab. 1997, 82, 2559–2565. [Google Scholar] [CrossRef]
- Boulle, N.; Logié, A.; Gicquel, C.; Perin, L.; Le Bouc, Y. Increased levels of insulin-like growth factor II (IGF-II) and IGF-binding protein-2 are associated with malignancy in sporadic adrenocortical tumors. J. Clin. Endocrinol. Metab. 1998, 83, 1713–1720. [Google Scholar] [CrossRef][Green Version]
- Giordano, T.J.; Thomas, D.G.; Kuick, R.; Lizyness, M.; Misek, D.E.; Smith, A.L.; Sanders, D.; Aljundi, R.T.; Gauger, P.G.; Thompson, N.W.; et al. Distinct Transcriptional profiles of adrenocortical tumors uncovered by DNA microarray analysis. Am. J. Pathol. 2003, 162, 521–531. [Google Scholar] [CrossRef]
- de Fraipont, F.; El Atifi, M.; Cherradi, N.; Le Moigne, G.; Defaye, G.; Houlgatte, R.; Bertherat, J.; Bertagna, X.; Plouin, P.-F.; Baudin, E.; et al. Gene Expression Profiling of Human Adrenocortical Tumors Using Complementary Deoxyribonucleic Acid Microarrays Identifies Several Candidate Genes as Markers of Malignancy. J. Clin. Endocrinol. Metab. 2005, 90, 1819–1829. [Google Scholar] [CrossRef]
- Almeida, M.Q.; Fragoso, M.C.B.V.; Lotfi, C.F.P.; Santos, M.G.; Nishi, M.Y.; Costa, M.H.S.; Lerario, A.M.; Maciel, C.C.; Mattos, G.E.; Jorge, A.A.L.; et al. Expression of Insulin-Like Growth Factor-II and Its Receptor in Pediatric and Adult Adrenocortical Tumors. J. Clin. Endocrinol. Metab. 2008, 93, 3524–3531. [Google Scholar] [CrossRef]
- Barlaskar, F.M.; Spalding, A.C.; Heaton, J.H.; Kuick, R.; Kim, A.C.; Thomas, D.G.; Giordano, T.J.; Ben-Josef, E.; Hammer, G.D. Preclinical Targeting of the Type I Insulin-Like Growth Factor Receptor in Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2009, 94, 204–212. [Google Scholar] [CrossRef]
- Catalano, R.; Giardino, E.; Treppiedi, D.; Mangili, F.; Morelli, V.; Elli, F.; Serban, A.; Luconi, M.; Mannelli, M.; Spada, A.; et al. The cytoskeleton actin binding protein filamin A impairs both IGF2 mitogenic effects and the efficacy of IGF1R inhibitors in adrenocortical cancer cells. Cancer Lett. 2021, 497, 77–88. [Google Scholar] [CrossRef]
- Nakamura, F.; Stossel, T.P.; Hartwig, J.H. The filamins: Organizers of cell structure and function. Cell Adhes. Migr. 2011, 5, 160–169. [Google Scholar] [CrossRef]
- Bedolla, R.G.; Wang, Y.; Asuncion, A.; Chamie, K.; Siddiqui, S.; Mudryj, M.M.; Prihoda, T.J.; Siddiqui, J.; Chinnaiyan, A.M.; Mehra, R.; et al. Nuclear versus Cytoplasmic Localization of Filamin A in Prostate Cancer: Immunohistochemical Correlation with Metastases. Clin. Cancer Res. 2009, 15, 788–796. [Google Scholar] [CrossRef]
- Alper, O.; Stetler-Stevenson, W.G.; Harris, L.N.; Leitner, W.W.; Özdemirli, M.; Hartmann, D.; Raffeld, M.; Abu-Asab, M.; Byers, S.; Zhuang, Z.; et al. Novel anti-filamin-A antibody detects a secreted variant of filamin-A in plasma from patients with breast carcinoma and high-grade astrocytoma. Cancer Sci. 2009, 100, 1748–1756. [Google Scholar] [CrossRef]
- Tian, H.-M.; Liu, X.-H.; Han, W.; Zhao, L.-L.; Yuan, B.; Yuan, C.-J. Differential expression of filamin A and its clinical significance in breast cancer. Oncol. Lett. 2013, 6, 681–686. [Google Scholar] [CrossRef]
- Uramoto, H.; Akyürek, L.M.; Hanagiri, T. A positive relationship between filamin and VEGF in patients with lung cancer. Anticancer Res. 2010, 30, 3939–3944. [Google Scholar]
- Kamochi, N.; Nakashima, M.; Aoki, S.; Uchihashi, K.; Sugihara, H.; Toda, S.; Kudo, S. Irradiated fibroblast-induced bystander effects on invasive growth of squamous cell carcinoma under cancer-stromal cell interaction. Cancer Sci. 2008, 99, 2417–2427. [Google Scholar] [CrossRef]
- Guedj, N.; Zhan, Q.; Perigny, M.; Rautou, P.-E.; Degos, F.; Belghiti, J.; Farges, O.; Bedossa, P.; Paradis, V. Comparative protein expression profiles of hilar and peripheral hepatic cholangiocarcinomas. J. Hepatol. 2009, 51, 93–101. [Google Scholar] [CrossRef]
- Storvall, S.; Leijon, H.; Ryhänen, E.M.; Vesterinen, T.; Heiskanen, I.; Schalin-Jäntti, C.; Arola, J. Filamin A and parafibromin expression in parathyroid carcinoma. Eur. J. Endocrinol. 2021, 185, 803–812. [Google Scholar] [CrossRef]
- Wang, A.; Liu, L.; Yuan, M.; Han, S.; You, X.; Zhang, H.; Lei, F.; Zhang, Y. Role and mechanism of FLNa and UCP2 in the development of cervical cancer. Oncol. Rep. 2020, 44, 2656–2668. [Google Scholar] [CrossRef]
- Vitali, E.; Boemi, I.; Rosso, L.; Cambiaghi, V.; Novellis, P.; Mantovani, G.; Spada, A.; Alloisio, M.; Veronesi, G.; Ferrero, S.; et al. FLNA is implicated in pulmonary neuroendocrine tumors aggressiveness and progression. Oncotarget 2017, 8, 77330–77340. [Google Scholar] [CrossRef]
- Xu, C.; Yu, X.; Zhu, Y.; Cai, Z.; Yu, L.; Lin, Y.; Yu, H.; Xue, Z.; Zhou, L. Overexpression of calpain-1 predicts poor outcome in patients with colorectal cancer and promotes tumor cell progression associated with downregulation of FLNA. Oncol. Rep. 2019, 41, 3424–3434. [Google Scholar] [CrossRef]
- Wang, Z.; Li, C.; Jiang, M.; Chen, J.; Yang, M.; Pu, J. Filamin A (FLNA) regulates autophagy of bladder carcinoma cell and affects its proliferation, invasion and metastasis. Int. Urol. Nephrol. 2018, 50, 263–273. [Google Scholar] [CrossRef]
- Sun, G.G.; Lu, Y.F.; Cheng, Y.J.; Hu, W.N. Absent expression of FLNA is correlated with poor prognosis of nasopharyngeal cancer. Tumor Biol. 2014, 35, 2967–2974. [Google Scholar] [CrossRef]
- Sun, G.G.; Sheng, S.H.; Jing, S.W.; Hu, W.N. An antiproliferative gene FLNA regulates migration and invasion of gastric carcinoma cell in vitro and its clinical significance. Tumor Biol. 2014, 35, 2641–2648. [Google Scholar] [CrossRef]
- Duregon, E.; Volante, M.; Bollito, E.; Goia, M.; Buttigliero, C.; Zaggia, B.; Berruti, A.; Scagliotti, G.V.; Papotti, M. Pitfalls in the diagnosis of adrenocortical tumors: A lesson from 300 consultation cases. Hum. Pathol. 2015, 46, 1799–1807. [Google Scholar] [CrossRef]
- Elsayes, K.M.; Elmohr, M.M.; Javadi, S.; Menias, C.O.; Remer, E.M.; Morani, A.C.; Shaaban, A.M. Mimics, pitfalls, and misdiagnoses of adrenal masses on CT and MRI. Abdom. Radiol. 2020, 45, 982–1000. [Google Scholar] [CrossRef]
- Wong, C.-L.; Fok, C.-K.; Chan, Y.-K.; Tam, V.H.-K.; Fung, L.-M. Was It an Adrenocortical Adenoma or an Adrenocortical Carcinoma? Limitation of the Weiss Scoring System in Determining the Malignant Potential of Adrenocortical Tumor: Report on Two Cases. Case Rep. Endocrinol. 2022, 2022, 7395050. [Google Scholar] [CrossRef]
- Faillot, S.; Assie, G. ENDOCRINE TUMOURS: The genomics of adrenocortical tumors. Eur. J. Endocrinol. 2016, 174, R249–R265. [Google Scholar] [CrossRef]
- Ozsari, L.; Kutahyalioglu, M.; Elsayes, K.M.; Vicens, R.A.; Sircar, K.; Jazaerly, T.; Waguespack, S.G.; Busaidy, N.L.; Cabanillas, M.E.; Dadu, R.; et al. Preexisting adrenal masses in patients with adrenocortical carcinoma: Clinical and radiological factors contributing to delayed diagnosis. Endocrine 2016, 51, 351–359. [Google Scholar] [CrossRef]
- Luconi, M.; Cantini, G.; van Leeuwaarde, R.S.; Roebaar, R.; Fei, L.; Propato, A.P.; Santi, R.; Ercolino, T.; Mannelli, M.; Canu, L.; et al. Prognostic Value of Microscopic Tumor Necrosis in Adrenal Cortical Carcinoma. Endocr. Pathol. 2023, 34, 224–233. [Google Scholar] [CrossRef]
- Zhang, K.; Zhu, T.; Gao, D.; Zhang, Y.; Zhao, Q.; Liu, S.; Su, T.; Bernier, M.; Zhao, R. Filamin A expression correlates with proliferation and invasive properties of human metastatic melanoma tumors: Implications for survival in patients. J. Cancer Res. Clin. Oncol. 2014, 140, 1913–1926. [Google Scholar] [CrossRef]
- Chen, M. In situ phosphorylation of platelet actin-binding protein by cAMP-dependent protein kinase stabilizes it against proteolysis by calpain. J. Biol. Chem. 1989, 264, 14282–14289. [Google Scholar] [CrossRef]
- Jay, D.; García, E.J.; Lara, J.E.; Medina, M.A.; de la Luz Ibarra, M. Determination of a cAMP-dependent protein kinase phosphorylation site in the C-terminal region of human endothelial actin-binding protein. Arch. Biochem. Biophys. 2000, 377, 80–84. [Google Scholar] [CrossRef]
- Jay, D.; García, E.J.; de la Luz Ibarra, M. In situ determination of a PKA phosphorylation site in the C-terminal region of filamin. Mol. Cell Biochem. 2004, 260, 49–53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ACC (n = 119) | ACA (n = 26) | ||
|---|---|---|---|
| Number (%) | Number (%) | p Value | |
| Sex | |||
| Female/Male (%) | 76/43 (63.9/36.1) | 15/11 (57.7/42.3) | 0.55 * |
| Age | |||
| ≥50 years | 60 (50.4) | 17 (81.0) | 0.02 − |
| Hormonal overproduction | |||
| Inactive | 36 (35.3) | 2 (8.0) | 0.0001 − |
| Single hormone | 38 (37.3) | 19 (76.0) | |
| More than one hormone | 28 (27.4) | 4 (16.0) | |
| ENSAT tumour stage | |||
| 1 | 17 (14.4) | / | |
| 2 | 44 (37.3) | / | |
| 3 | 40 (33.9) | / | |
| 4 | 17 (14.4) | / | |
| Ki67 | |||
| 0–9% | 30 (27.0) | / | |
| 10–19% | 38 (34.2) | / | |
| ≥20% | 43 (38.7) | / | |
| Weiss score | |||
| <6 | 40 (44.0) | / | |
| ≥6 | 51 (56.0) | / | |
| Resection status | |||
| R0 | 47 (66.2) | / | |
| R1 | 7 (9.9) | / | |
| R2 | 9 (12.7) | / | |
| RX | 8 (11.3) | / | |
| S-GRAS score | |||
| 0–1 | 8 (14.5) | / | |
| 2–3 | 22 (40.0) | / | |
| 4–5 | 14 (25.5) | / | |
| 6–9 | 11 (20.0) | / | |
| Post-surgical therapy | |||
| No medical treatment | 17 (14.9) | / | |
| Mitotane | 40 (35.1) | / | |
| Mitotane + chemotherapy | 57 (50.0) | / |
| Low FLNA (n = 103) | High FLNA (n = 16) | p Value | |
|---|---|---|---|
| Female (%) | 62.1 | 75.0 | 0.32 * |
| Age | 49.7 ± 14.8 | 50.9 ± 14.9 | 0.76 + |
| ≥50 years (%) | 49.5 | 56.3 | 0.62 * |
| ENSAT stage (1–2) (%) | 48.0 | 75.0 | 0.04 * |
| ENSAT stage (3–4) (%) | 52.0 | 25.0 | |
| Ki67 | 18.8 ± 16.4 | 13.0 ± 10.6 | 0.20 + |
| Ki67 < 10 (%) | 24.7 | 42.9 | 0.15 * |
| Ki67 ≥ 10 (%) | 75.3 | 57.1 | |
| Weiss < 6 (%) | 39.0 | 71.4 | 0.02 * |
| Weiss ≥ 6 (%) | 61.0 | 28.6 | |
| Resection status (%) | |||
| R0 | 62.3 | 90.0 | 0.02 − |
| R1 | 11.5 | 0.0 | |
| R2 | 14.8 | 0.0 | |
| RX | 11.5 | 10.0 | |
| S-GRAS 0–1 (%) | 10.6 | 37.5 | 0.02 − |
| S-GRAS 2–3 (%) | 40.4 | 37.5 | |
| S-GRAS > 3 (%) | 48.9 | 25.0 | |
| Secreting tumours (%) | 64.4 | 66.7 | 0.86 * |
| Non-secreting tumours (%) | 35.6 | 33.3 | |
| Mitotane chemotherapy (%) | 49.0 | 56.3 | 0.24 * |
| Histological Weiss Criteria | Low FLNA (%) | High FLNA (%) | p Value |
|---|---|---|---|
| Nuclear grade | |||
| High | 20.8 | 25.0 | 1.00 |
| Low | 79.2 | 75.0 | |
| Mitoses | |||
| ≤5 per 50 high-power fields | 16.7 | 75.0 | 0.04 |
| >5 per 50 high-power fields | 83.3 | 25.0 | |
| Atypical mitoses | |||
| No | 70.8 | 75.0 | 1.00 |
| Yes | 29.2 | 25.0 | |
| Clear cells | |||
| >25% | 8.3 | 0.0 | 1.00 |
| ≤25% | 91.7 | 100.0 | |
| Diffuse architecture | |||
| ≤33% surface | 4.2 | 0.0 | 1.00 |
| >33% surface | 95.8 | 100.0 | |
| Confluent necrosis | |||
| No | 33.3 | 75.0 | 0.27 |
| Yes | 66.7 | 25.0 | |
| Venous invasion | |||
| No | 62.5 | 75.0 | 1.00 |
| Yes | 37.5 | 25.0 | |
| Sinusoidal invasion | |||
| No | 41.7 | 75.0 | 0.31 |
| Yes | 58.3 | 25.0 | |
| Capsular infiltration | |||
| No | 29.2 | 75.0 | 0.12 |
| Yes | 70.8 | 25.0 |
| Variable | Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|
| n | HR | 95%CI | p | n | HR | 95%CI | p | |
| FLNA expression | 112 | 0.2 | [0.2–1.0] | 0.05 | 55 | 0.2 | [0.2–1.3] | 0.09 |
| Low | 98 | 47 | ||||||
| High | 14 | 8 | ||||||
| Variables | Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|---|
| n | HR | 95%CI | p | n | HR | 95%CI | p | |
| FLNA expression | 112 | 0.2 | [0.2–1.0] | 0.05 | 105 | 0.2 | [0.2–1.2] | 0.08 |
| Low | 98 | 92 | ||||||
| High | 14 | 13 | ||||||
| ENSAT stage | 111 | 3.9 | [2.0–7.7] | <0.001 | 105 | 4.6 | [2.2–9.6] | <0.001 |
| 1–3 | 96 | 93 | ||||||
| 4 | 15 | 12 | ||||||
| Ki67 | 105 | 4.5 | [1.6–12.8] | 0.005 | 105 | 3.0 | [1.0–8.7] | 0.04 |
| <10 | 30 | 30 | ||||||
| ≥10 | 75 | 75 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalano, R.; Altieri, B.; Angelousi, A.; Arosio, M.; Bravi, F.; Canu, L.; Croci, G.A.; Detomas, M.; Esposito, E.; Ferrante, E.; et al. High Filamin a Expression in Adrenocortical Carcinomas Is Associated with a Favourable Tumour Behaviour: A European Multicentric Study. Int. J. Mol. Sci. 2023, 24, 16573. https://doi.org/10.3390/ijms242316573
Catalano R, Altieri B, Angelousi A, Arosio M, Bravi F, Canu L, Croci GA, Detomas M, Esposito E, Ferrante E, et al. High Filamin a Expression in Adrenocortical Carcinomas Is Associated with a Favourable Tumour Behaviour: A European Multicentric Study. International Journal of Molecular Sciences. 2023; 24(23):16573. https://doi.org/10.3390/ijms242316573
Chicago/Turabian StyleCatalano, Rosa, Barbara Altieri, Anna Angelousi, Maura Arosio, Francesca Bravi, Letizia Canu, Giorgio A. Croci, Mario Detomas, Emanuela Esposito, Emanuele Ferrante, and et al. 2023. "High Filamin a Expression in Adrenocortical Carcinomas Is Associated with a Favourable Tumour Behaviour: A European Multicentric Study" International Journal of Molecular Sciences 24, no. 23: 16573. https://doi.org/10.3390/ijms242316573
APA StyleCatalano, R., Altieri, B., Angelousi, A., Arosio, M., Bravi, F., Canu, L., Croci, G. A., Detomas, M., Esposito, E., Ferrante, E., Ferrero, S., Fuss, C. T., Kaltsas, G., Kimpel, O., Landwehr, L.-S., Luconi, M., Morelli, V., Nesi, G., Nozza, E., ... Peverelli, E. (2023). High Filamin a Expression in Adrenocortical Carcinomas Is Associated with a Favourable Tumour Behaviour: A European Multicentric Study. International Journal of Molecular Sciences, 24(23), 16573. https://doi.org/10.3390/ijms242316573