

Predictive Performances of Blood-Count-Derived Inflammatory Markers for Liver Fibrosis Severity in Psoriasis Vulgaris

 , and
, and 
Abstract
:1. Introduction
2. Results
2.1. Patients’ Clinical Profile
2.2. Serological Markers and Liver Fibrosis Scores
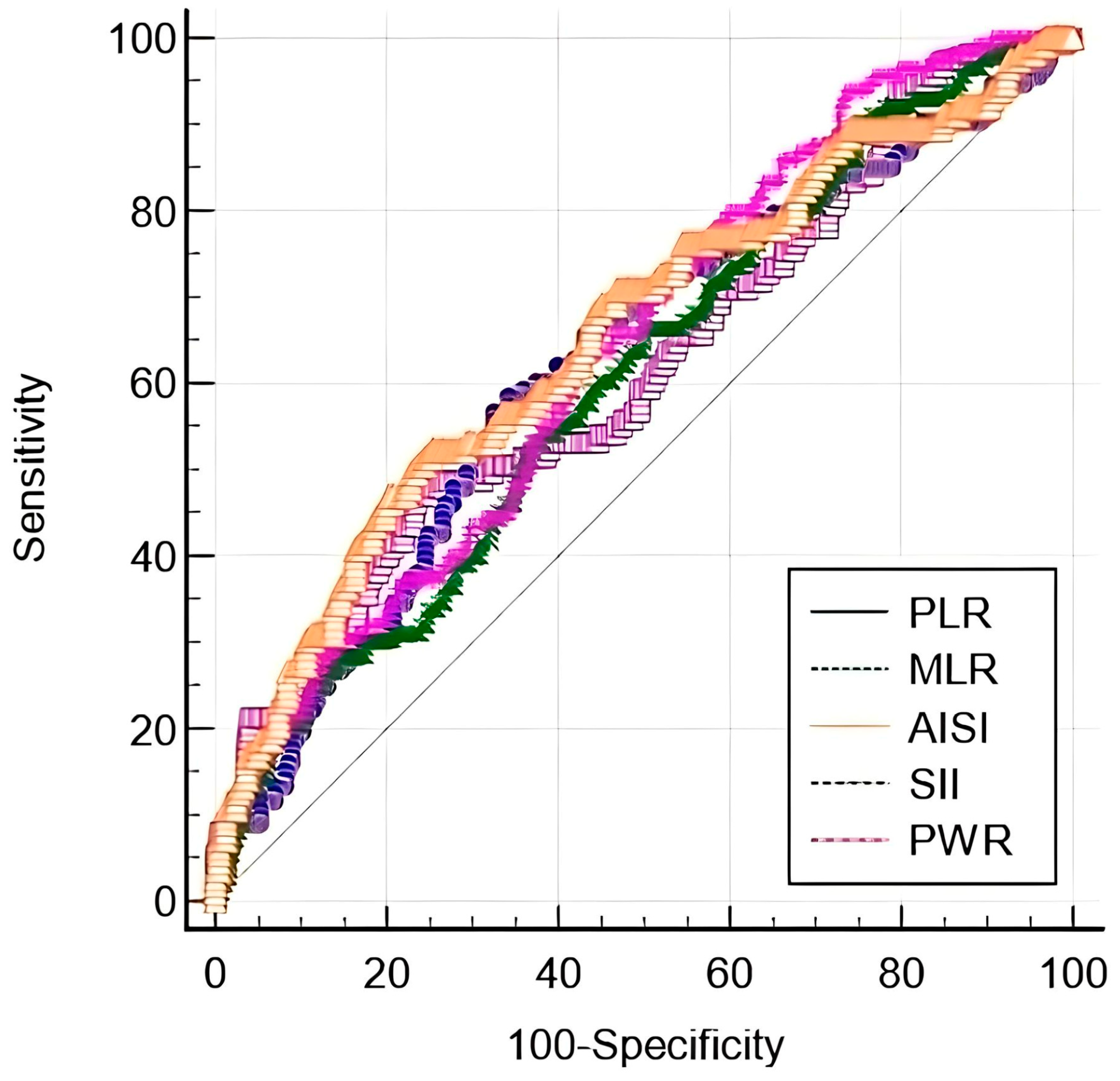
2.3. Performance of Inflammatory Biomarkers for the Evaluation of Liver Fibrosis
2.4. Performance of Hepatic NITs for the Evaluation of Liver Fibrosis
2.5. The Reliability of Blood-Count-Derived Markers for Predicting Liver Fibrosis Severity
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Data Collection
4.3. Biomarkers
4.4. Study Outcome
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Damiani, G.; Bragazzi, N.L.; Karimkhani Aksut, C.; Wu, D.; Alicandro, G.; McGonagle, D.; Guo, C.; Dellavalle, R.; Grada, A.; Wong, P.; et al. The Global, Regional, and National Burden of Psoriasis: Results and Insights from the Global Burden of Disease 2019 Study. Front. Med. 2021, 8, 743180. [Google Scholar] [CrossRef] [PubMed]
- Nicolescu, A.C.; Bucur, Ș.; Giurcăneanu, C.; Gheucă-Solovăstru, L.; Constantin, T.; Furtunescu, F.; Ancuța, I.; Constantin, M.M. Prevalence and Characteristics of Psoriasis in Romania—First Study in Overall Population. J. Pers. Med. 2021, 11, 523. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The association between psoriasis and hypertension: A systematic review and meta-analysis of observational studies. J. Hypertens. 2013, 31, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Friedland, R.; Kridin, K.; Cohen, A.D.; Landau, D.; Ben-Amitai, D. Psoriasis and Renal Disorders: A Large-Scale Population-Based Study in Children and Adults. Dermatology 2022, 238, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Ogdie, A.; Grewal, S.K.; Noe, M.H.; Shin, D.B.; Takeshita, J.; Chiesa Fuxench, Z.C.; Carr, R.M.; Gelfand, J.M. Risk of Incident Liver Disease in Patients with Psoriasis, Psoriatic Arthritis, and Rheumatoid Arthritis: A Population-Based Study. J. Investig. Dermatol. 2018, 138, 760–767. [Google Scholar] [CrossRef]
- Meng, F.; Wang, K.; Aoyama, T.; Grivennikov, S.I.; Paik, Y.; Scholten, D.; Cong, M.; Iwaisako, K.; Liu, X.; Zhang, M.; et al. Interleukin-17 Signaling in Inflammatory, Kupffer Cells, and Hepatic Stellate Cells Exacerbates Liver Fibrosis in Mice. Gastroenterology 2012, 143, 765–776.e3. [Google Scholar] [CrossRef] [PubMed]
- Menter, A.; Korman, N.J.; Elmets, C.A.; Feldman, S.R.; Gelfand, J.M.; Gordon, K.B.; Gottlieb, A.B.; Koo, J.Y.; Lebwohl, M.; Lim, H.W.; et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. J. Am. Acad. Dermatol. 2009, 61, 451–485. [Google Scholar] [CrossRef] [PubMed]
- Maybury, C.M.; Samarasekera, E.; Douiri, A.; Barker, J.N.; Smith, C.H. Diagnostic accuracy of noninvasive markers of liver fibrosis in patients with psoriasis taking methotrexate: A systematic review and meta-analysis. Br. J. Dermatol. 2014, 170, 1237–1247. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281.e4. [Google Scholar] [CrossRef]
- Menter, A.; Gelfand, J.M.; Connor, C.; Armstrong, A.W.; Cordoro, K.M.; Davis, D.M.R.; Elewski, B.E.; Gordon, K.B.; Gottlieb, A.B.; Kaplan, D.H.; et al. Joint American Academy of Dermatology–National Psoriasis Foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies. J. Am. Acad. Dermatol. 2020, 82, 1445–1486. [Google Scholar] [CrossRef]
- Larmann, J.; Handke, J.; Scholz, A.S.; Dehne, S.; Arens, C.; Gillmann, H.J.; Uhle, F.; Motsch, J.; Weigand, M.A.; Janssen, H. Preoperative neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are associated with major adverse cardiovascular and cerebrovascular events in coronary heart disease patients undergoing non-cardiac surgery. BMC Cardiovasc. Disord. 2020, 20, 230. [Google Scholar] [CrossRef] [PubMed]
- Durmus, E.; Kivrak, T.; Gerin, F.; Sunbul, M.; Sari, I.; Erdogan, O. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio are Predictors of Heart Failure. Arq. Bras. Cardiol. 2015, 105, 606–613. [Google Scholar] [CrossRef]
- Ye, Z.; Hu, T.; Wang, J.; Xiao, R.; Liao, X.; Liu, M.; Sun, Z. Systemic immune-inflammation index as a potential biomarker of cardiovascular diseases: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2022, 9, 933913. [Google Scholar] [CrossRef] [PubMed]
- Modica, R.; Minotta, R.; Liccardi, A.; Cannavale, G.; Benevento, E.; Colao, A. Evaluation of Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Systemic Immune–Inflammation Index (SII) as Potential Biomarkers in Patients with Sporadic Medullary Thyroid Cancer (MTC). J. Pers. Med. 2023, 13, 953. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.Q.; Ma, C.; Cao, W.Z.; Ning, Z.; Tan, G. Prognostic Significance of NLR, PLR, LMR and Tumor Infiltrating T Lymphocytes in Patients Undergoing Surgical Resection for Hilar Cholangiocarcinoma. Front. Oncol. 2022, 12, 908907. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, C.; Mongardini, F.M.; Paolicelli, M.; Bentivoglio, D.; Cozzolino, G.; Ruggiero, R.; Pizza, A.; Tolone, S.; del Genio, G.; Parisi, S.; et al. Role of Inflammatory Biomarkers (NLR, LMR, PLR) in the Prognostication of Malignancy in Indeterminate Thyroid Nodules. Int. J. Mol. Sci. 2023, 24, 6466. [Google Scholar] [CrossRef] [PubMed]
- Kovács, A.R.; Sulina, A.; Kovács, K.S.; Lukács, L.; Török, P.; Lampé, R. Prognostic Significance of Preoperative NLR, MLR, and PLR Values in Predicting the Outcome of Primary Cytoreductive Surgery in Serous Epithelial Ovarian Cancer. Diagnostics 2023, 13, 2268. [Google Scholar] [CrossRef] [PubMed]
- Maloney, S.; Pavlakis, N.; Itchins, M.; Arena, J.; Mittal, A.; Hudson, A.; Colvin, E.; Sahni, S.; Diakos, C.; Chan, D.; et al. The Prognostic and Predictive Role of the Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Lymphocyte-to-Monocyte Ratio (LMR) as Biomarkers in Resected Pancreatic Cancer. J. Clin. Med. 2023, 12, 1989. [Google Scholar] [CrossRef]
- Brito, G.M.C.; Fontenele, A.M.M.; Carneiro, E.C.R.L.; Nogueira, I.A.L.; Cavalcante, T.B.; Vale, A.A.M.; Monteiro, S.C.M.; Filho, N.S. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in Nondialysis Chronic Kidney Patients. Int. J. Inflamm. 2021, 2021, 6678960. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines 2022, 10, 1272. [Google Scholar] [CrossRef] [PubMed]
- Hayran, Y. Elevated neutrophil to lymphocyte ratio as an indicator of secondary erythema nodosum, a retrospective observational study. Turk. J. Med. Sci. 2019, 49, 624–634. [Google Scholar] [CrossRef] [PubMed]
- Rifaioglu, E.N.; Bülbül Şen, B.; Ekiz, Ö.; Cigdem Dogramaci, A. Neutrophil to lymphocyte ratio in Behçet’s disease as a marker of disease activity. Acta Dermatovenerol. Alp. Pannonica Adriat. 2014, 23, 65–67. [Google Scholar] [PubMed]
- Korkmaz, C.; Demircioglu, S. The Association of Neutrophil/Lymphocyte and Platelet/Lymphocyte Ratios and Hematological Parameters with Diagnosis, Stages, Extrapulmonary Involvement, Pulmonary Hypertension, Response to Treatment, and Prognosis in Patients with Sarcoidosis. Can. Respir. J. 2020, 2020, 1696450. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.M.; Wu, C.; Gao, Y.M.; Li, F.; Yu, X.L.; Jin, H.Z. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and other hematological parameters in psoriasis patients. BMC Immunol. 2021, 22, 64. [Google Scholar] [CrossRef] [PubMed]
- Yorulmaz, A.; Hayran, Y.; Akpinar, U.; Yalcin, B. Systemic Immune-Inflammation Index (SII) Predicts Increased Severity in Psoriasis and Psoriatic Arthritis. Curr. Health Sci. J. 2020, 46, 352–357. [Google Scholar]
- Aktaş Karabay, E.; Demir, D.; Aksu Çerman, A. Evaluation of monocyte to high-density lipoprotein ratio, lymphocytes, monocytes, and platelets in psoriasis. An. Bras. Dermatol. 2020, 95, 40–45. [Google Scholar] [CrossRef]
- Amalia, L.; Dalimonthe, N.Z. Clinical significance of Platelet-to-White Blood Cell Ratio (PWR) and National Institute of Health Stroke Scale (NIHSS) in acute ischemic stroke. Heliyon 2020, 6, e05033. [Google Scholar] [CrossRef]
- Abdulhadi, B.; Naranjo, M.; Krishnamoorthy, P.; Rangaswami, J. White blood cell count to platelet ratio: A novel biomarker for predicting outcomes in patients on circulatory support devices. J. Am. Coll. Cardiol. 2018, 71, A810. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, S.E.; Song, D.S.; Kim, H.Y.; Yoon, E.; Kim, T.H.; Jung, Y.K.; Suk, K.T.; Jun, B.G.; Yim, H.J.; et al. Platelet-to-White Blood Cell Ratio Is Associated with Adverse Outcomes in Cirrhotic Patients with Acute Deterioration. J. Clin. Med. 2022, 11, 2463. [Google Scholar] [CrossRef]
- Yu, K.; Du, Z.; Li, Q.; Cheng, Q.; Huang, C.; Shi, G.; Li, N. Comparison of non-invasive models for predicting liver damage in chronic hepatitis B patients. Gastroenterol. Hepatol. 2019, 42, 281–288. [Google Scholar] [CrossRef]
- Ko, D.G.; Park, J.W.; Kim, J.H.; Jung, J.H.; Kim, H.S.; Suk, K.T.; Jang, M.K.; Park, S.H.; Lee, M.S.; Kim, D.J.; et al. Platelet-to-White Blood Cell Ratio: A Feasible Biomarker for Pyogenic Liver Abscess. Diagnostics 2022, 12, 2556. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.L.; Liang, S.; Li, J.; Napierata, L.; Brown, T.; Benoit, S.; Senices, M.; Gill, D.; Dunussi-Joannopoulos, K.; Collins, M.; et al. IL-22 is required for Th17 cell-mediated pathology in a mouse model of psoriasis-like skin inflammation. J. Clin. Investig. 2008, 118, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.R.; Blumenschein, W.; Murphy, E.; Diveu, C.; Wiekowski, M.; Abbondanzo, S.; Lucian, L.; Geissler, R.; Brodie, S.; Kimball, A.B.; et al. IL-23 stimulates epidermal hyperplasia via TNF and IL-20R2-dependent mechanisms with implications for psoriasis pathogenesis. J. Exp. Med. 2006, 203, 2577–2587. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Guttman-Yassky, E.; Suarez-Farinas, M.; Nograles, K.E.; Tian, S.; Cardinale, I.; Chimenti, S.; Krueger, J.G. Integrative Responses to IL-17 and TNF-alpha in Human Keratinocytes Account for Key Inflammatory Pathogenic Circuits in Psoriasis. J. Investig. Dermatol. 2011, 131, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Danilenko, D.M.; Valdez, P.; Kasman, I.; Eastham-Anderson, J.; Wu, J.; Ouyang, W. Interleukin-22, a T(H)17 cytokine, mediates IL-23-induced dermal inflammation and acanthosis. Nature 2007, 445, 648–651. [Google Scholar] [CrossRef]
- Arican, O.; Aral, M.; Sasmaz, S.; Ciragil, P. Serum levels of TNF-alpha, IFN-gamma, IL-6, IL-8, IL-12, IL-17 and IL-18 in patients with active psoriasis and correlation with disease severity. Mediat. Inflamm. 2005, 2005, 273–279. [Google Scholar] [CrossRef]
- Tsoi, L.C.; Spain, S.L.; Knight, J.; Ellinghaus, E.; Stuart, P.E.; Capon, F.; Ding, J.; Li, Y.; Tejasvi, T.; Gudjonsson, J.E.; et al. Identification of 15 new psoriasis susceptibility loci highlights the role of innate immunity. Nat. Genet. 2012, 44, 1341–1348. [Google Scholar] [CrossRef]
- Sugimoto, E.; Matsuda, H.; Shibata, S.; Mizuno, Y.; Koyama, A.; Li, L.; Taira, H.; Ito, Y.; Awaji, K.; Yamashita, T.; et al. Impact of Pretreatment Systemic Inflammatory Markers on Treatment Persistence with Biologics and Conventional Systemic Therapy: A Retrospective Study of Patients with Psoriasis Vulgaris and Psoriatic Arthritis. J. Clin. Med. 2023, 12, 3046. [Google Scholar] [CrossRef]
- Asahina, A.; Kubo, N.; Umezawa, Y.; Honda, H.; Yanaba, K.; Nakagawa, H. Neutrophil-lymphocyte ratio, platelet-lymphocyte ratio and mean platelet volume in Japanese patients with psoriasis and psoriatic arthritis: Response to therapy with biologics. J Dermatol. 2017, 44, 1112–1121. [Google Scholar] [CrossRef]
- Annen, S.; Horiguchi, G.; Teramukai, S.; Ichiyama, S.; Ito, M.; Hoashi, T.; Kanda, N.; Saeki, H. Association of Transition of Laboratory Markers with Transition of Disease Activity in Psoriasis Patients Treated with Biologics. J. Nippon. Med. Sch. 2022, 89, 587–593. [Google Scholar] [CrossRef]
- An, I.; Ucmak, D.; Ozturk, M. The effect of biological agent treatment on neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, mean platelet volume, and C-reactive protein in psoriasis patients. Adv. Dermatol. Allergol. 2020, 37, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Albayrak, H. Neutrophil-to-Lymphocyte Ratio, Neutrophil-to-Monocyte Ratio, Platelet-to-Lymphocyte Ratio, and Systemic Immune-Inflammation Index in Psoriasis Patients: Response to Treatment with Biological Drugs. J. Clin. Med. 2023, 12, 5452. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.S.B.; Kvist-Hansen, A.; Siewertsen, M.; Enevold, C.; Hansen, P.R.; Kaur-Knudsen, D.; Zachariae, C.; Nielsen, C.H.; Loft, N.; Skov, L. Blood Cell Biomarkers of Inflammation and Cytokine Levels as Predictors of Response to Biologics in Patients with Psoriasis. Int. J. Mol. Sci. 2023, 24, 6111. [Google Scholar] [CrossRef] [PubMed]
- Ataseven, A.; Temiz, S.A.; Eren, G.; Özer, İ.; Dursun, R. Comparison of anti-TNF and IL-inhibitors treatments in patients with psoriasis in terms of response to routine laboratory parameter dynamics. J. Dermatol. Treat. 2022, 33, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Taha, M.M.; Al-Asady, Z.T.S. Evaluation of the Effectiveness of Antioxidants and TNF-α in Iraqi Patients with Psoriasis treated with Etanercept. Res. J. Pharm. Technol. 2019, 12, 665–668. [Google Scholar] [CrossRef]
- Olejniczak-Staruch, I.; Narbutt, J.; Bednarski, I.; Woźniacka, A.; Sieniawska, J.; Kraska-Gacka, M.; Śmigielski, J.; Lesiak, A. Interleukin 22 and 6 serum concentrations decrease under long-term biologic therapy in psoriasis. Postep. Dermatol. Alergol. 2020, 37, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Pastore, S.; Mariani, V.; Lulli, D.; Gubinelli, E.; Raskovic, D.; Mariani, S.; Stancato, A.; de Luca, C.; Pecorelli, A.; Valacchi, G.; et al. Glutathione peroxidase activity in the blood cells of psoriatic patients correlates with their responsiveness to Efalizumab. Free Radic. Res. 2011, 45, 585–599. [Google Scholar] [CrossRef] [PubMed]
- Becatti, M.; Urban, M.L.; Taurisano, G.; Mannucci, A.; Barygina, V.; Pescitelli, L.; Prignano, F.; Silvestri, E.; Taddei, N.; Lotti, T.; et al. Secukinumab reduces plasma oxidative stress in psoriasis: A case-based experience. Dermatol. Ther. 2018, 31, e12675. [Google Scholar] [CrossRef]
- Campanati, A.; Orciani, M.; Gorbi, S.; Regoli, F.; Di Primio, R.; Offidani, A. Effect of biologic therapies targeting tumour necrosis factor-α on cutaneous mesenchymal stem cells in psoriasis: Modifications of MSCs in psoriatic patients receiving TNF-α inhibitors. Br. J. Dermatol. 2012, 167, 68–76. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Papadavid, E.; Makavos, G.; Andreadou, I.; Varoudi, M.; Gravanis, K.; Theodoropoulos, K.; Pavlidis, G.; Triantafyllidi, H.; Moutsatsou, P.; et al. Lowering Interleukin-12 Activity Improves Myocardial and Vascular Function Compared with Tumor Necrosis Factor-a Antagonism or Cyclosporine in Psoriasis. Circ. Cardiovasc. Imaging 2017, 10, e006283. [Google Scholar] [CrossRef]
- Elango, T.; Dayalan, H.; Gnanaraj, P.; Malligarjunan, H.; Subramanian, S. Impact of methotrexate on oxidative stress and apoptosis markers in psoriatic patients. Clin. Exp. Med. 2014, 14, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Rademaker, M. Monitoring methotrexate-induced liver fibrosis in patients with psoriasis: Utility of transient elastography. Psoriasis Targets Ther. 2018, 8, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J. Comparison of Noninvasive Markers of Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Ülger, Y. Is neutrophil lymphocyte ratio a useful biomarker in predicting fibrosis in chronic hepatitis C infection? Eastern J. Med. 2021, 26, 123–127. [Google Scholar] [CrossRef]
- Kara, M.; Dogru, T.; Genc, H.; Sertoglu, E.; Celebi, G.; Gurel, H.; Kayadibi, H.; Cicek, A.F.; Ercin, C.N.; Sonmez, A. Neutrophil-to-lymphocyte ratio is not a predictor of liver histology in patients with nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2015, 27, 1144–1148. [Google Scholar] [CrossRef]
- Lu, W.; Zhang, Y.; Zhu, H.; Zhang, T.; Zhang, L.; Gao, N.; Chang, D.; Yin, J.; Zhou, X.; Li, M.; et al. Evaluation and comparison of the diagnostic performance of routine blood tests in predicting liver fibrosis in chronic hepatitis B infection. Br. J. Biomed. Sci. 2019, 76, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Ding, R.; Zhou, X.; Huang, D.; Wang, Y.; Li, X.; Yan, L.; Lu, W.; Yang, Z.; Zhang, Z. Predictive Performances of Blood Parameter Ratios for Liver Inflammation and Advanced Liver Fibrosis in Chronic Hepatitis B Infection. BioMed Res. Int. 2021, 2021, 6644855. [Google Scholar] [CrossRef]
- Sigal, S.; Mitchell, O.; Feldman, D.; Diakow, M. The pathophysiology of thrombocytopenia in chronic liver disease. Hepatic Med. Évid. Res. 2016, 8, 39–50. [Google Scholar] [CrossRef]
- Wai, C. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef]
- Giannini, E.; Risso, D.; Botta, F.; Chiarbonello, B.; Fasoli, A.; Malfatti, F.; Romagnoli, P.; Testa, E.; Ceppa, P.; Testa, R. Validity and Clinical Utility of the Aspartate Aminotransferase–Alanine Aminotransferase Ratio in Assessing Disease Severity and Prognosis in Patients with Hepatitis C Virus–Related Chronic Liver Disease. Arch. Intern. Med. 2003, 163, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Cross, T.J.S.; Rizzi, P.; Berry, P.A.; Bruce, M.; Portmann, B.; Harrison, P.M. King’s Score: An accurate marker of cirrhosis in chronic hepatitis C. Eur. J. Gastroenterol. Hepatol. 2009, 21, 730–738. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | All Patients | LR-SF (n = 246) | HR-SF (n = 113) | p-Value |
|---|---|---|---|---|
| Age | 54.76 ± 16.36 | 50.07 ± 16.10 | 64.98 ± 11.63 | <0.001 |
| Gender | ||||
| Male | 216 (60.17%) | 141 (57.32%) | 75 (66.37%) | 0.100 |
| Female | 143 (39.83%) | 105 (42.68%) | 38 (33.63%) | |
| Disease severity | ||||
| Mild | 177 (49.30%) | 132 (53.66%) | 45 (39.82%) | 0.015 |
| Moderate-severe | 182 (50.70%) | 114 (46.34%) | 68 (60.18%) | |
| AST | 19 [18–20.56] | 16 [15–17] | 31 [26–37] | <0.001 |
| ALT | 22 [21–24] | 21 [19–22.86] | 28 [23.61–33] | 0.001 |
| GGT | 30 [27–32] | 24.5 [20.14–28] | 48 [36–68.40] | <0.001 |
| Platelets | 238.02 [228.90–243.00] | 270.44 [261.67–279.21] | 188.67 [178.59–198.75] | <0.001 |
| WBC | 7.50 [7.17–7.85] | 7.73 [7.37–8.09] | 6.84 [6.43–7.67] | 0.001 |
| Neutrophils | 4.44 [4.23–4.75] | 4.53 [4.28–4.88] | 4.12 [3.77–4.66] | 0.02 |
| Lymphocytes | 2.08 [1.97–2.23] | 2.22 [2.08–2.30] | 1.85 [1.67–2.00] | <0.001 |
| Monocytes | 0.50 [0.48–0.53] | 0.49 [0.46–0.52] | 0.53 [0.48–0.56] | 0.33 |
| PLR | 115.19 [110.12–120.96] | 117.49 [112.46–153.81] | 102.51 [89.95–117.91] | <0.001 |
| NLR | 2.05 [1.91–2.21] | 2.04 [1.82–2.23] | 2.08 [1.95–2.32] | 0.58 |
| d-NLR | 1.56 [1.44–1.66] | 1.55 [1.42–1.67] | 1.60 [1.44–1.73] | 0.96 |
| MLR | 0.24 [0.22–0.25] | 0.22 [0.21–0.23] | 0.28 [0.26–0.30] | <0.001 |
| ESR | 15 [12.74–17.26] | 14.26 [12.47–16.53] | 17 [13.63–20] | 0.07 |
| SII | 480.22 [453.86–524.81] | 526.07 [480.15–570.06] | 431.53 [387.45–462.05] | <0.001 |
| SIRI | 1.04 [0.94–1.11] | 0.99 [0.90–1.11] | 1.07 [0.98–1.28] | 0.42 |
| AISI | 258.40 [231.92–274] | 273.26 [248.12–285.65] | 214.55 [187.50–250.25] | 0.001 |
| APRI | 0.22 [0.20–0.23] | 0.18 [0.16–0.19] | 0.49 [0.41–0.55] | <0.001 |
| AAR | 0.88 [0.82–0.93] | 0.75 [0.70–0.81] | 1.10 [1.02–1.25] | <0.001 |
| PWR | 32.86 [30.99–33.98] | 34.49 [22.05–36.53] | 27.40 [25.39–31.12] | <0.001 |
| GPR | 0.12 [0.11–0.13] | 0.09 [0.08–0.10] | 0.24 [0.20–0.33] | <0.001 |
| Marker | r | p-Value | Marker | r | p-Value |
|---|---|---|---|---|---|
| AST | 0.49 | <0.001 | MLR | 0.20 | <0.001 |
| ALT | 0.21 | <0.001 | SII | −0.22 | <0.001 |
| GGT | 0.39 | <0.001 | AISI | −0.17 | <0.001 |
| Platelets | −0.546 | <0.001 | PWR | −0.25 | <0.001 |
| WBC | −0.17 | 0.001 | APRI | 0.63 | <0.001 |
| Lymphocytes | −0.20 | <0.001 | AAR | 0.44 | <0.001 |
| PLR | −0.19 | <0.001 | GPR | 0.46 | <0.001 |
| AUC (95% CI) | p-Value | Cut-Off | Se (%) | Sp (%) | Youden Index J | p-Value * | |
|---|---|---|---|---|---|---|---|
| PLR | 0.618 (0.565–0.668) | <0.001 | 94.68 | 46.90 | 76.42 | 0.23 | 0.19 |
| MLR | 0.624 (0.571–0.674) | <0.001 | 0.26 | 58.41 | 65.85 | 0.24 | 0.44 |
| SII | 0.640 (0.588–0.690) | <0.001 | 828.77 | 93.81 | 26.42 | 0.20 | 0.71 |
| AISI | 0.607 (0.555–0.658) | <0.001 | 273.09 | 66.37 | 50.00 | 0.16 | 0.33 |
| PWR | 0.657 (0.606–0.706) | <0.001 | 27.59 | 52.21 | 74.80 | 0.27 | - |
| AUC (95% CI) | p-Value | Cut-Off | Se (%) | Sp (%) | Youden Index J | p-Value * | |
|---|---|---|---|---|---|---|---|
| APRI | 0.889 (0.852–0.920) | <0.001 | 0.22 | 91.15 | 69.11 | 0.60 | - |
| AAR | 0.774 (0.727–0.816) | <0.001 | 0.89 | 75.22 | 66.67 | 0.42 | <0.001 |
| GPR | 0.786 (0.740–0.828) | <0.001 | 0.14 | 74.34 | 73.98 | 0.48 | <0.001 |
| Parameter | OR | 95% CI | p-Value |
|---|---|---|---|
| Demographic characteristics | |||
| Age > 50 years old | 4.63 | 2.57–8.36 | <0.001 |
| Male sex | 0.78 | 0.48–1.27 | 0.127 |
| Moderate-severe psoriasis | 1.70 | 1.06–2.73 | 0.028 |
| Inflammatory markers | |||
| PLR | 1.02 | 0.99–1.06 | 0.097 |
| MLR | 3.51 | 1.69–7.29 | <0.001 |
| PWR | 0.94 | 0.99–1.02 | <0.001 |
| SII | 0.99 | 0.99–1.01 | 0.150 |
| AISI | 0.98 | 0.98–0.99 | 0.009 |
| Hepatic NITs | |||
| APRI | 11.68 | 7.44–18.32 | <0.001 |
| AAR | 13.26 | 5.37–32.78 | <0.001 |
| GPR | 4.54 | 0.70–29.43 | 0.110 |
| Marker | Formula |
|---|---|
| NLR | Neutrophil count/lymphocyte count [×103/μL] |
| d-NLR | Neutrophil count/(WBC-neutrophil count) [×103/μL] |
| PLR | Platelet count/lymphocyte count [×103/μL] |
| MLR | Monocyte count/lymphocyte count [×103/μL] |
| SII | (Neutrophil count × platelet count)/lymphocyte count [×103/μL] |
| SIRI | (Neutrophil count × monocyte count)/lymphocyte count [×103/μL] |
| AISI | (Neutrophil count × monocyte count × platelet count)/lymphocyte count [×103/μL] |
| PWR | Platelet count/WBC [×103/μL] |
| FIB-4 | (Age [years] × AST [U/L])/(platelet count [×103/μL] × √ALT [U/L]) |
| APRI | [(AST/upper limit of the normal AST range) × 100]/platelet count [×103/μL] |
| AAR | AST/ALT [U/L] |
| GPR | GGT [U/L]/platelet count [×103/μL] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiucă, O.M.; Morariu, S.H.; Mariean, C.R.; Tiucă, R.A.; Nicolescu, A.C.; Cotoi, O.S. Predictive Performances of Blood-Count-Derived Inflammatory Markers for Liver Fibrosis Severity in Psoriasis Vulgaris. Int. J. Mol. Sci. 2023, 24, 16898. https://doi.org/10.3390/ijms242316898
Tiucă OM, Morariu SH, Mariean CR, Tiucă RA, Nicolescu AC, Cotoi OS. Predictive Performances of Blood-Count-Derived Inflammatory Markers for Liver Fibrosis Severity in Psoriasis Vulgaris. International Journal of Molecular Sciences. 2023; 24(23):16898. https://doi.org/10.3390/ijms242316898
Chicago/Turabian StyleTiucă, Oana Mirela, Silviu Horia Morariu, Claudia Raluca Mariean, Robert Aurelian Tiucă, Alin Codrut Nicolescu, and Ovidiu Simion Cotoi. 2023. "Predictive Performances of Blood-Count-Derived Inflammatory Markers for Liver Fibrosis Severity in Psoriasis Vulgaris" International Journal of Molecular Sciences 24, no. 23: 16898. https://doi.org/10.3390/ijms242316898
APA StyleTiucă, O. M., Morariu, S. H., Mariean, C. R., Tiucă, R. A., Nicolescu, A. C., & Cotoi, O. S. (2023). Predictive Performances of Blood-Count-Derived Inflammatory Markers for Liver Fibrosis Severity in Psoriasis Vulgaris. International Journal of Molecular Sciences, 24(23), 16898. https://doi.org/10.3390/ijms242316898