
Head and Neck Cancer Patients’ Survival According to HPV Status, miRNA Profiling, and Tumour Features—A Cohort Study
 ,
,  ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Patient and Tumour Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 76) | HPV-Positive (n = 18) | HPV-Negative (n = 58) | |
|---|---|---|---|---|
| Gender | F | 20 (26.3%) | 4 (22.2%) | 16 (27.6%) |
| M | 56 (73.7%) | 14 (77.8%) | 42 (72.4%) | |
| Age | Mean ± SD | 61.7 ± 11.6 | 59.6 ± 15.5 | 62.4 ± 10.1 |
| Median | 61 | 61.5 | 61 | |
| Range | 31–87 | 31–87 | 42–85 | |
| 0–64 | 46 (60.5%) | 11 (61.1%) | 35 (60.3%) | |
| 65+ | 30 (39.5%) | 7 (38.9%) | 23 (39.7%) | |
| Lifestyle | NSmND | 26 (34.2%) | 8 (44.4%) | 18 (31%) |
| Sm | 5 (6.6%) | 1 (5.6%) | 4 (6.9%) | |
| SmD | 45 (59.2%) | 9 (50%) | 36 (62.1%) | |
| Tumour site | Oral cavity | 60 (78.9%) | 12 (66.7%) | 48 (82.8%) |
| gingiva | 17 (22.4%) | 3 (16.7%) | 14 (24.1%) | |
| oral tongue | 16 (21.1%) | 2 (11.1%) | 14 (24.1%) | |
| sublingual area | 16 (21.1%) | 5 (27.8%) | 11 (19%) | |
| retromolar | 9 (11.8%) | 2 (11.1%) | 7 (12.1%) | |
| buccal mucosa | 2 (2.6%) | 0 (0%) | 2 (3.4%) | |
| Oropharynx | 16 (21.1%) | 6 (33.3%) | 10 (17.2%) | |
| base of tongue | 8 (10.5%) | 1 (5.6%) | 7 (12.1%) | |
| tonsil | 7 (9.2%) | 5 (27.8%) | 2 (3.4%) | |
| posterior pharyngeal wall | 1 (1.3%) | 0 (0%) | 1 (1.7%) | |
| cT stage | 1 | 6 (7.9%) | 2 (11.1%) | 4 (6.9%) |
| 2 | 26 (34.2%) | 5 (27.8%) | 21 (36.2%) | |
| 3 | 21 (27.6%) | 5 (27.8%) | 16 (27.6%) | |
| 4a | 23 (30.3%) | 6 (33.3%) | 17 (29.3%) | |
| cN stage | 0 | 35 (46.1%) | 7 (38.9%) | 28 (48.3%) |
| 1 | 20 (26.3%) | 5 (27.8%) | 15 (25.9%) | |
| 2 | 17 (22.4%) | 5 (27.8%) | 12 (20.7%) | |
| 3 | 4 (5.3%) | 1 (5.6%) | 3 (5.2%) | |
| Overall clinical stage | Stage I–II | 21 (27.6%) | 2 (11.1%) | 19 (32.8%) |
| I | 3 (3.9%) | 0 (0%) | 3 (5.2%) | |
| II | 18 (23.7%) | 2 (11.1%) | 16 (27.6%) | |
| Stage III | 19 (25%) | 6 (33.3%) | 13 (22.4%) | |
| Stage IV | 36 (47.4%) | 10 (55.6%) | 26 (44.8%) | |
| IVa | 32 (42.1%) | 9 (50%) | 23 (39.7%) | |
| IVb | 4 (5.3%) | 1 (5.6%) | 3 (5.2%) | |
| HPV | Positive | 18 (23.7%) | 18 | |
| Negative | 58 (76.3%) | 58 | ||
| Therapy | Surgery | 45 (59.2%) | 10 (55.6%) | 35 (60.3%) |
| Surgery + RT | 31 (40.8%) | 8 (44.4%) | 23 (39.7%) | |
| Follow-up | Survival overall | 38 (50%) | 10 (55.6%) | 28 (48.3%) |
| No evidence of disease | 36 (47.4%) | 9 (50%) | 27 (46.6%) | |
| Alive with disease | 2 (2.6%) | 1 (5.6%) | 1 (1.7%) | |
| Dead of other causes | 23 (30.3%) | 3 (16.7%) | 20 (34.5%) | |
| Dead of disease | 15 (19.7%) | 5 (27.8%) | 10 (17.2%) | |
| Follow-up events | Recurrence | 13 (17.1%) | 4 (22.2%) | 9 (15.5%) |
| Distant metastasis | 17 (22.4%) | 4 (22.2%) | 13 (22.4%) | |
| Secondary malignancy | 16 (21.1%) | 3 (16.7%) | 13 (22.4%) | |
| Median follow-up time (months) | 45.5 | 40.5 | 46 | |
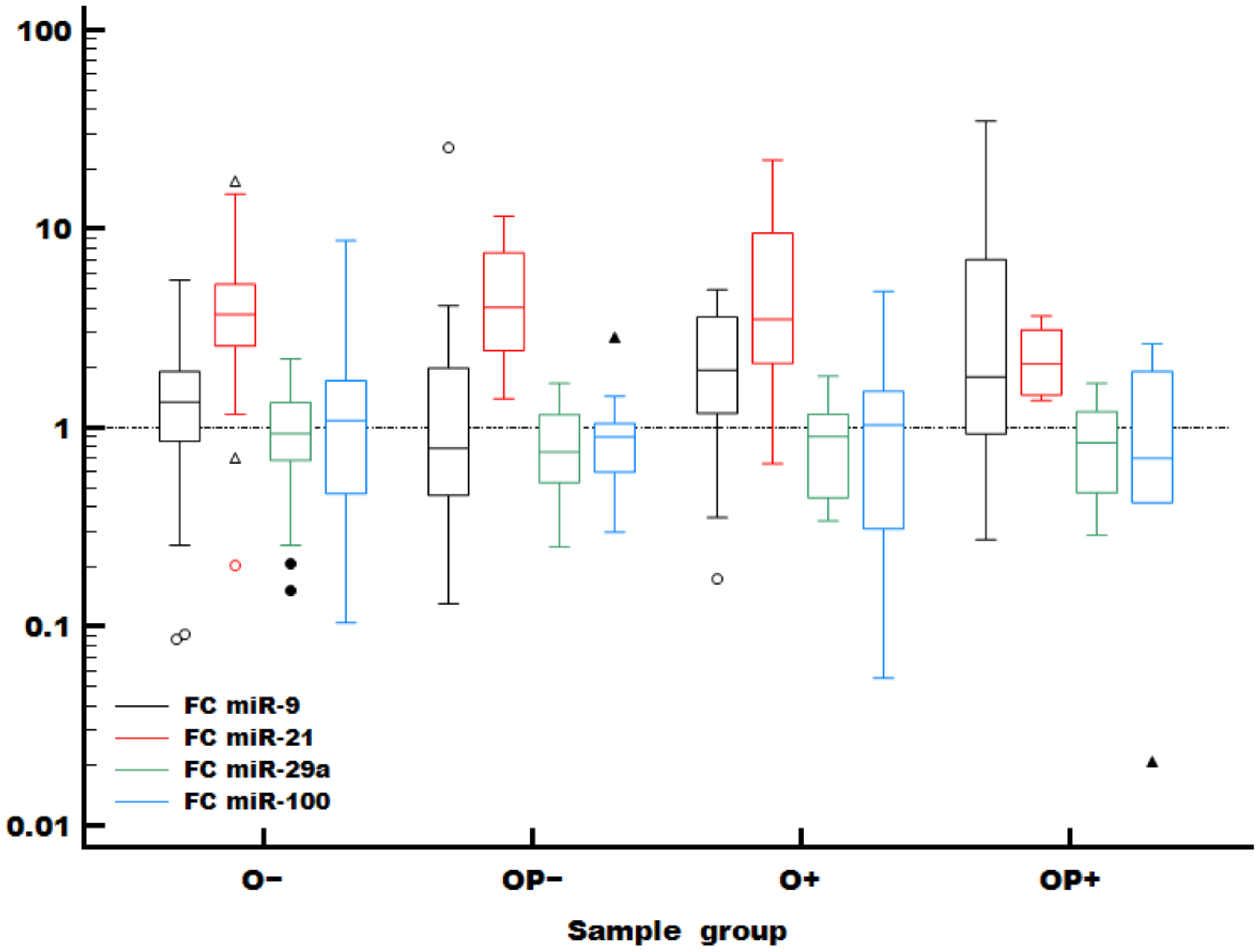
2.2. MiRNA Expression
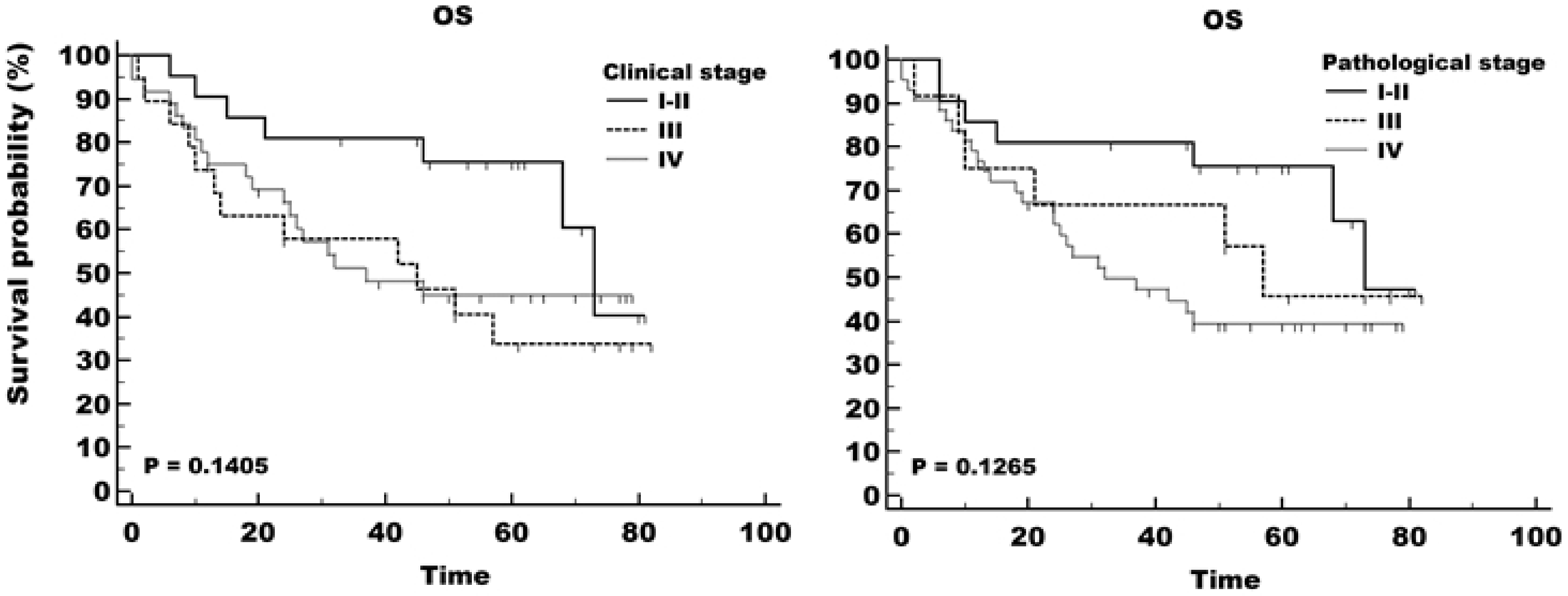
2.3. Overall Survival
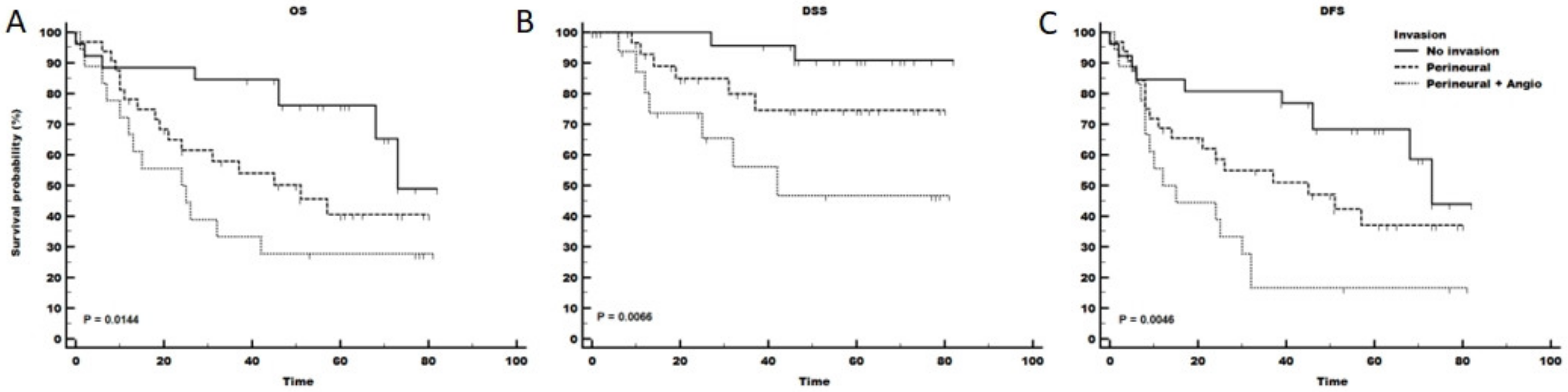
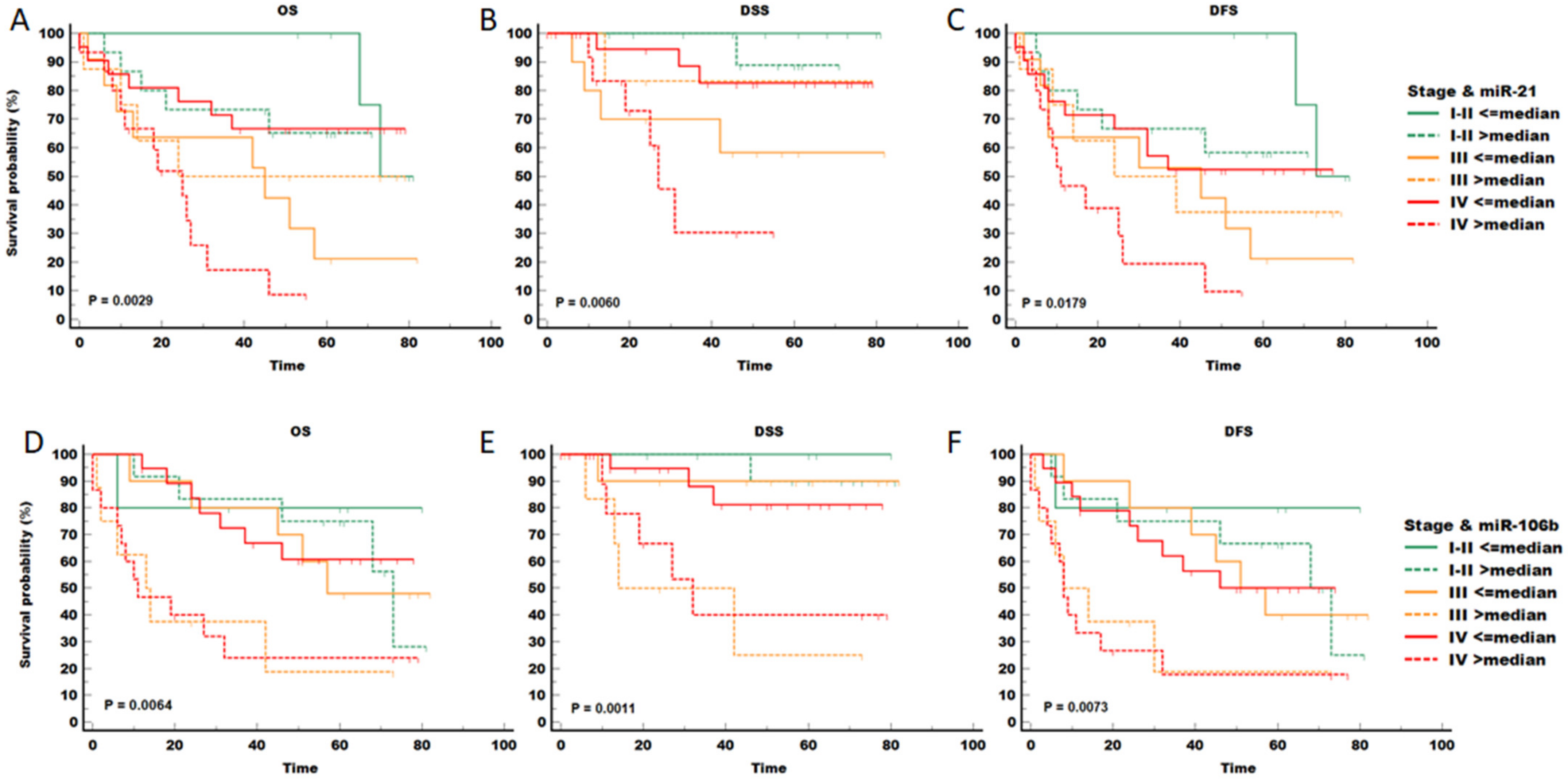
2.4. Risk Factors in HNSCC Patients
3. Discussion
4. Material and Methods
4.1. Patients and Tumour Samples
4.2. RNA and DNA Extraction and HPV Testing
4.3. MicroRNA Quantitation
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wyss, A.; Hashibe, M.; Chuang, S.-C.; Lee, Y.-C.A.; Zhang, Z.-F.; Yu, G.-P.; Winn, D.M.; Wei, Q.; Talamini, R.; Szeszenia-Dabrowska, N.; et al. Cigarette, Cigar, and Pipe Smoking and the Risk of Head and Neck Cancers: Pooled Analysis in the International Head and Neck Cancer Epidemiology Consortium. Am. J. Epidemiol. 2013, 178, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and Neck Squamous Cell Carcinoma. Nat. Rev. Dis. Prim. 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Tumban, E. A Current Update on Human Papillomavirus-Associated Head and Neck Cancers. Viruses 2019, 11, 922. [Google Scholar] [CrossRef] [PubMed]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-Associated Oropharyngeal Cancer: Epidemiology, Molecular Biology and Clinical Management. Nat. Rev. Clin. Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef]
- Luo, X.; Zheng, M.; Cao, M.; Zhang, W.; Huang, M.; Dai, L.; Tang, Y.; Liang, X. Distinguishable Prognostic MiRNA Signatures of Head and Neck Squamous Cell Cancer With or Without HPV Infection. Front. Oncol. 2021, 10, 614487. [Google Scholar] [CrossRef]
- Du, E.; Mazul, A.L.; Farquhar, D.; Brennan, P.; Anantharaman, D.; Abedi-Ardekani, B.; Weissler, M.C.; Hayes, D.N.; Olshan, A.F.; Zevallos, J.P. Long-term Survival in Head and Neck Cancer: Impact of Site, Stage, Smoking, and Human Papillomavirus Status. Laryngoscope 2019, 129, 2506–2513. [Google Scholar] [CrossRef]
- De Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide Burden of Cancer Attributable to HPV by Site, Country and HPV Type: Worldwide Burden of Cancer Attributable to HPV. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Sullivan, D.C.; Jessup, J.M.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Cham, Switzerland, 2018; ISBN 978-3-319-40617-6. [Google Scholar]
- Gartagani, Z.; Doumas, S.; Kyriakopoulou, A.; Economopoulou, P.; Psaltopoulou, T.; Kotsantis, I.; Sergentanis, T.N.; Psyrri, A. Lymph Node Ratio as a Prognostic Factor in Neck Dissection in Oral Cancer Patients: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 4456. [Google Scholar] [CrossRef]
- Xing, Y.; Zhang, J.; Lin, H.; Gold, K.A.; Sturgis, E.M.; Garden, A.S.; Lee, J.J.; William, W.N. Relationship between Level of Lymph Node Metastasis and Survival in Locally Advanced Head and Neck Squamous Cell Carcinoma. Cancer 2016, 122, 534–545. [Google Scholar] [CrossRef]
- Salehi, M.; Sharifi, M. Exosomal MiRNAs as Novel Cancer Biomarkers: Challenges and Opportunities. J. Cell. Physiol. 2018, 233, 6370–6380. [Google Scholar] [CrossRef] [PubMed]
- Thomaidou, A.C.; Batsaki, P.; Adamaki, M.; Goulielmaki, M.; Baxevanis, C.N.; Zoumpourlis, V.; Fortis, S.P. Promising Biomarkers in Head and Neck Cancer: The Most Clinically Important MiRNAs. Int. J. Mol. Sci. 2022, 23, 8257. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Croce, C.M. The Role of MicroRNAs in Human Cancer. Signal Transduct. Target. Ther. 2016, 1, 15004. [Google Scholar] [CrossRef] [PubMed]
- Lubov, J.; Maschietto, M.; Ibrahim, I.; Mlynarek, A.; Hier, M.; Kowalski, L.P.; Alaoui-Jamali, M.A.; da Silva, S.D. Meta-Analysis of MicroRNAs Expression in Head and Neck Cancer: Uncovering Association with Outcome and Mechanisms. Oncotarget 2017, 8, 55511–55524. [Google Scholar] [CrossRef]
- Ganju, A.; Khan, S.; Hafeez, B.B.; Behrman, S.W.; Yallapu, M.M.; Chauhan, S.C.; Jaggi, M. MiRNA Nanotherapeutics for Cancer. Drug Discov. Today 2017, 22, 424–432. [Google Scholar] [CrossRef]
- Hersi, H.M.; Raulf, N.; Gaken, J.; Folarin, N.; Tavassoli, M. MicroRNA-9 Inhibits Growth and Invasion of Head and Neck Cancer Cells and Is a Predictive Biomarker of Response to Plerixafor, an Inhibitor of Its Target CXCR. Mol. Oncol. 2018, 12, 2023–2041. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Network. Comprehensive Genomic Characterization of Head and Neck Squamous Cell Carcinomas. Nature 2015, 517, 576–582. [Google Scholar] [CrossRef]
- Tiwana, M.S.; Wu, J.; Hay, J.; Wong, F.; Cheung, W.; Olson, R.A. 25 Year Survival Outcomes for Squamous Cell Carcinomas of the Head and Neck: Population-Based Outcomes from a Canadian Province. Oral Oncol. 2014, 50, 651–656. [Google Scholar] [CrossRef]
- Panarese, I.; Aquino, G.; Ronchi, A.; Longo, F.; Montella, M.; Cozzolino, I.; Roccuzzo, G.; Colella, G.; Caraglia, M.; Franco, R. Oral and Oropharyngeal Squamous Cell Carcinoma: Prognostic and Predictive Parameters in the Etiopathogenetic Route. Expert Rev. Anticancer. Ther. 2019, 19, 105–119. [Google Scholar] [CrossRef]
- Gatta, G.; Botta, L.; Sánchez, M.J.; Anderson, L.A.; Pierannunzio, D.; Licitra, L.; Hackl, M.; Zielonke, N.; Oberaigner, W.; Van Eycken, E.; et al. Prognoses and Improvement for Head and Neck Cancers Diagnosed in Europe in Early 2000s: The EUROCARE-5 Population-Based Study. Eur. J. Cancer 2015, 51, 2130–2143. [Google Scholar] [CrossRef]
- D’Souza, G.; Dempsey, A. The Role of HPV in Head and Neck Cancer and Review of the HPV Vaccine. Prev. Med. 2011, 53, S5–S11. [Google Scholar] [CrossRef]
- Weiss, B.G.; Anczykowski, M.Z.; Küffer, S.; Spiegel, J.L.; Bertlich, M.; Canis, M.; Ihler, F.; Kitz, J.; Jakob, M. Prognostic Impact of Additional HPV Diagnostics in 102 Patients with P16-Stratified Advanced Oropharyngeal Squamous Cell Carcinoma. Eur. Arch. Otorhinolaryngol. 2021, 278, 1983–2000. [Google Scholar] [CrossRef]
- Ko, H.C.; Harari, P.M.; Sacotte, R.M.; Chen, S.; Wieland, A.M.; Yu, M.; Baschnagel, A.M.; Bruce, J.Y.; Kimple, R.J.; Witek, M.E. Prognostic Implications of Human Papillomavirus Status for Patients with Non-Oropharyngeal Head and Neck Squamous Cell Carcinomas. J. Cancer Res. Clin. Oncol. 2017, 143, 2341–2350. [Google Scholar] [CrossRef] [PubMed]
- Wookey, V.B.; Appiah, A.K.; Kallam, A.; Ernani, V.; Smith, L.M.; Ganti, A.K. HPV Status and Survival in Non-Oropharyngeal Squamous Cell Carcinoma of the Head and Neck. Anticancer Res. 2019, 39, 1907–1914. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human Papillomavirus Types in Head and Neck Squamous Cell Carcinomas Worldwide: A Systematic Review. Cancer Epidemiol. Biomark. Prev. 2005, 14, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Descamps, G.; Karaca, Y.; Lechien, J.R.; Kindt, N.; Decaestecker, C.; Remmelink, M.; Larsimont, D.; Andry, G.; Hassid, S.; Rodriguez, A.; et al. Classical Risk Factors, but Not HPV Status, Predict Survival after Chemoradiotherapy in Advanced Head and Neck Cancer Patients. J. Cancer Res. Clin. Oncol. 2016, 142, 2185–2196. [Google Scholar] [CrossRef]
- Lai, Y.-H.; Su, C.-C.; Wu, S.-Y.; Hsueh, W.-T.; Wu, Y.-H.; Chen, H.H.W.; Hsiao, J.-R.; Liu, C.-H.; Tsai, Y.-S. Impact of Alcohol and Smoking on Outcomes of HPV-Related Oropharyngeal Cancer. J. Clin. Med. 2022, 11, 6510. [Google Scholar] [CrossRef] [PubMed]
- Božinović, K.; Sabol, I.; Rakušić, Z.; Jakovčević, A.; Šekerija, M.; Lukinović, J.; Prgomet, D.; Grce, M. HPV-Driven Oropharyngeal Squamous Cell Cancer in Croatia—Demography and Survival. PLoS ONE 2019, 14, e0211577. [Google Scholar] [CrossRef]
- Stathopoulos, P.; Smith, W.P. Analysis of Survival Rates Following Primary Surgery of 178 Consecutive Patients with Oral Cancer in a Large District General Hospital. J. Maxillofac. Oral Surg. 2017, 16, 158–163. [Google Scholar] [CrossRef]
- Sabatini, M.E.; Chiocca, S. Human Papillomavirus as a Driver of Head and Neck Cancers. Br. J. Cancer 2020, 122, 306–314. [Google Scholar] [CrossRef]
- Chen, Z.; Jin, Y.; Yu, D.; Wang, A.; Mahjabeen, I.; Wang, C.; Liu, X.; Zhou, X. Down-Regulation of the MicroRNA-99 Family Members in Head and Neck Squamous Cell Carcinoma. Oral Oncol. 2012, 48, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Božinović, K.; Sabol, I.; Dediol, E.; Milutin Gašperov, N.; Manojlović, S.; Vojtechova, Z.; Tachezy, R.; Grce, M. Genome-Wide MiRNA Profiling Reinforces the Importance of MiR-9 in Human Papillomavirus Associated Oral and Oropharyngeal Head and Neck Cancer. Sci. Rep. 2019, 9, 2306. [Google Scholar] [CrossRef] [PubMed]
- Resnick, R.M.; Cornelissen, M.T.E.; Wright, D.K.; Eichinger, G.H.; Fox, H.; Ter Schegget, J.; Manos, M.M. Detection and Typing of Human Papillomavirus in Archival Cervical Cancer Specimens by DNA Amplification With Consensus Primers. Gynecol. Oncol. 1990, 82, 1477–1484. [Google Scholar] [CrossRef] [PubMed]
- Gravitt, P.E.; Peyton, C.L.; Alessi, T.Q.; Wheeler, C.M.; Coutlée, F.; Hildesheim, A.; Schiffman, M.H.; Scott, D.R.; Apple, R.J. Improved Amplification of Genital Human Papillomaviruses. J. Clin. Microbiol. 2000, 38, 357–361. [Google Scholar] [CrossRef]
- De Roda Husman, A.M.; Walboomers, J.M.; van den Brule, A.J.; Meijer, C.J.; Snijders, P.J. The use of general primers GP5 and GP6 elongated at their 3’ ends with adjacent highly conserved sequences improves human papillomavirus detection by PCR. J. Gen. Virol. 1995, 76, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, H.; Kawana, T.; Kitagawa, K.; Mizuno, M.; Yoshikura, H.; Iwamoto, A. Detection and Typing of Multiple Genital Human Papillomaviruses by DNA Amplification with Consensus Primers. Jpn. J. Cancer Res. 1991, 82, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Soler, C.; Allibert, P.; Chardonnet, Y.; Cros, P.; Mandrand, B.; Thivolet, J. Detection of human papillomavirus types 6, 11, 16 and 18 in mucosal and cutaneous lesions by the multiplex polymerase chain reaction. J. Virol. Methods 1991, 35, 143–157. [Google Scholar] [CrossRef]
- Smeets, S.J.; Hesselink, A.T.; Speel, E.-J.M.; Haesevoets, A.; Snijders, P.J.; Pawlita, M.; Meijer, C.J.; Braakhuis, B.J.; Leemans, C.R.; Brakenhoff, R.H. A novel algorithm for reliable detection of human papillomavirus in paraffin embedded head and neck cancer specimen. Int. J. Cancer 2007, 121, 2465–2472. [Google Scholar] [CrossRef]
- Chandrashekar, D.S.; Karthikeyan, S.K.; Korla, P.K.; Patel, H.; Shovon, A.R.; Athar, M.; Netto, G.J.; Qin, Z.S.; Kumar, S.; Manne, U.; et al. UALCAN: An update to the integrated cancer data analysis platform. Neoplasia 2022, 25, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Chandrashekar, D.S.; Bashel, B.; Balasubramanya, S.A.H.; Creighton, C.J.; Ponce-Rodriguez, I.; Chakravarthi, B.V.S.K.; Varambally, S. UALCAN: A portal for facilitating tumor subgroup gene expression and survival analyses. Neoplasia 2017, 19, 649–658. [Google Scholar] [CrossRef]




| Characteristics | Total (n = 76) | HPV-Positive (n = 18) | HPV-Negative (n = 58) | |
|---|---|---|---|---|
| pT stage | 1 | 6 (7.9%) | 2 (11.1%) | 4 (6.9%) |
| 2 | 30 (39.5%) | 5 (27.8%) | 25 (43.1%) | |
| 3 | 15 (19.7%) | 3 (16.7%) | 12 (20.7%) | |
| 4a | 25 (32.9%) | 8 (44.4%) | 17 (29.3%) | |
| pN stage | X | 11 (14.5%) | 5 (27.8%) | 6 (10.3%) |
| 0 | 27 (35.5%) | 3 (16.7%) | 24 (41.4%) | |
| 1 | 8 (10.5%) | 1 (5.6%) | 7 (12.1%) | |
| 2 | 21 (27.6%) | 5 (27.8%) | 16 (27.6%) | |
| 3 | 9 (11.8%) | 4 (22.2%) | 5 (8.6%) | |
| Overall pathological stage | Stage I–II | 21 (27.6%) | 3 (16.7%) | 18 (31%) |
| I | 4 (5.3%) | 1 (5.6%) | 3 (5.2%) | |
| II | 17 (22.4%) | 2 (11.1%) | 15 (25.9%) | |
| Stage III | 12 (15.8%) | 3 (16.7%) | 9 (15.5%) | |
| Stage IV | 43 (56.6%) | 12 (66.7%) | 31 (53.4%) | |
| IVa | 34 (44.7%) | 8 (44.4%) | 26 (44.8%) | |
| IVb | 9 (11.8%) | 4 (22.2%) | 5 (8.6%) | |
| Grade | 1 | 29 (38.2%) | 5 (27.8%) | 24 (41.4%) |
| 2 | 35 (46.1%) | 8 (44.4%) | 27 (46.6%) | |
| 3 | 12 (15.8%) | 5 (27.8%) | 7 (12.1%) | |
| Resection margins | Clean (≥5 mm) | 25 (32.9%) | 6 (33.3%) | 19 (32.8%) |
| Clean (NS) | 21 (27.6%) | 4 (22.2%) | 17 (29.3%) | |
| Close (<5 mm) | 30 (39.5%) | 8 (44.4%) | 22 (37.9%) | |
| Invasion | No invasion | 26 (34.2%) | 6 (33.3%) | 20 (34.5%) |
| Perineural | 32 (42.1%) | 8 (44.4%) | 24 (41.4%) | |
| Perineural + Angio | 18 (23.7%) | 4 (22.2%) | 14 (24.1%) | |
| Lymph node yield | 0 | 10 (13.2%) | 4 (22.2%) | 6 (10.3%) |
| 1–10 | 8 (10.5%) | 1 (5.6%) | 7 (12.1%) | |
| 11–20 | 17 (22.4%) | 2 (11.1%) | 15 (25.9%) | |
| 21+ | 41 (53.9%) | 11 (61.1%) | 30 (51.7%) | |
| Lymph node positivity | 0 | 38 (50%) | 8 (44.4%) | 30 (51.7%) |
| 1–2 | 22 (28.9%) | 5 (27.8%) | 17 (29.3%) | |
| 3–4 | 9 (11.8%) | 3 (16.7%) | 6 (10.3%) | |
| 5+ | 7 (9.2%) | 2 (11.1%) | 5 (8.6%) | |
| Lymph node ratio | ≤0.05 | 35 (46.1%) | 7 (38.9%) | 28 (48.3%) |
| >0.05 | 31 (40.8%) | 7 (38.9%) | 24 (41.4%) | |
| No lymph nodes evaluated | 10 (13.2%) | 4 (22.2%) | 6 (10.3%) | |
| Extranodal spread | No | 24 (31.6%) | 4 (22.2%) | 20 (34.5%) |
| Yes | 14 (18.4%) | 6 (33.3%) | 8 (13.8%) | |
| No positive LNs | 38 (50%) | 8 (44.4%) | 30 (51.7%) | |
| miRNA | Total (n = 76) | HPV-Negative (n = 58) | HPV-Positive (n = 18) | O Total (n = 60) | OP Total (n = 16) | O− (n = 48) | O+ (n = 12) | OP− (n = 10) | OP+ (n = 6) |
|---|---|---|---|---|---|---|---|---|---|
| miR-9 | 1.4 (0.8–2.6) | 1.2 (0.7–1.9) | 1.8 (1–4.2) | 1.4 (0.9–2.6) | 0.9 (0.5–3.1) | 1.3 (0.9–1.9) | 2 (1.2–3.6) | 0.8 (0.5–2) | 1.8 (0.9–7) |
| miR-21 | 3.6 (2.3–5.5) | 3.8 (2.5–5.5) | 3 (1.7–7.5) | 3.7 (2.5–5.6) | 3.3 (1.9–4.3) | 3.7 (2.6–5.3) | 3.5 (2.1–9.7) | 4 (2.4–7.6) | 2.2 (1.5–3.1) |
| mir-29a | 0.9 (0.6–1.3) | 0.9 (0.7–1.3) | 0.9 (0.5–1.2) | 0.9 (0.7–1.3) | 0.8 (0.5–1.2) | 0.9 (0.7–1.3) | 0.9 (0.4–1.2) | 0.8 (0.5–1.2) | 0.9 (0.5–1.2) |
| miR-100 | 1 (0.4–1.6) | 1 (0.5–1.6) | 0.9 (0.3–1.6) | 1 (0.4–1.7) | 0.9 (0.5–1.2) | 1.1 (0.5–1.7) | 1 (0.3–1.5) | 0.9 (0.6–1.1) | 0.7 (0.4–1.9) |
| Overall Survival | Disease-Specific Survival | Disease-Free Survival | ||||
|---|---|---|---|---|---|---|
| Events | 38/76 | 14/69 * | 43/76 | |||
| Overall model fit | p < 0.001 | p = 0.028 | p < 0.001 | |||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Age 65+ vs <65 | - | - | - | - | 3 (1.4–6.4) | 0.0042 |
| Gender M vs F | 3.1 (1.1–8.7) | 0.027 | - | - | - | - |
| Sm vs NSmND | 2.1 (0.4–10.7) | 0.360 | - | - | - | 0 |
| SmD vs NSND | 1.7 (0.7–4.1) | 0.206 | - | - | - | 0 |
| Stage III vs I–II | 1.6 (0.5–4.9) | 0.419 | 3.9 (0.4–38.6) | 0.244 | 1.2 (0.5–3.3) | 0.674 |
| Stage IV vs I–II | 1.1 (0.4–3.5) | 0.839 | 3.5 (0.4–31.9) | 0.265 | 1.4 (0.6–3.7) | 0.464 |
| Perivascular vs no invasion | 2.8 (0.8–9.6) | 0.099 | 3.9 (0.5–30.5) | 0.192 | 2.8 (1–8) | 0.049 |
| Both invasions vs no invasion | 4.3 (1.4–13.6) | 0.014 | 3.9 (0.6–27.8) | 0.169 | 4 (1.5–10.9) | 0.007 |
| Resection edge Not reported vs Clean (>5 mm) | 4.5 (1.5–13.6) | 0.008 | 8.3 (0.7–96.1) | 0.089 | 3.1 (1.2–8) | 0.019 |
| Resection edge Close (<5 mm) vs Clean (>5 mm) | 1.9 (0.7–4.7) | 0.190 | 5 (0.6–42.1) | 0.143 | 1.5 (0.6–3.7) | 0.345 |
| LN yield 1–10 vs 0 | 11.6 (1.2–9.7) | 0.033 | - | - | 10 (1.8–54.2) | 0.008 |
| LN yield 11–20 vs 0 | 5.3 (0.6–46.9) | 0.134 | - | - | 2.7 (0.6–13.4) | 0.216 |
| LN yield 21+ vs 0 | 4.7 (0.6–40.1) | 0.156 | - | - | 5 (1.1–23.7) | 0.041 |
| FC_miR-21 | 1.1 (1–1.2) | 0.011 | - | - | 1.1 (1–1.2) | 0.002 |
| FC miR-106b * | - | - | 1.3 (0.8–1.9) | 0.269 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šimić, I.; Božinović, K.; Milutin Gašperov, N.; Kordić, M.; Pešut, E.; Manojlović, L.; Grce, M.; Dediol, E.; Sabol, I. Head and Neck Cancer Patients’ Survival According to HPV Status, miRNA Profiling, and Tumour Features—A Cohort Study. Int. J. Mol. Sci. 2023, 24, 3344. https://doi.org/10.3390/ijms24043344
Šimić I, Božinović K, Milutin Gašperov N, Kordić M, Pešut E, Manojlović L, Grce M, Dediol E, Sabol I. Head and Neck Cancer Patients’ Survival According to HPV Status, miRNA Profiling, and Tumour Features—A Cohort Study. International Journal of Molecular Sciences. 2023; 24(4):3344. https://doi.org/10.3390/ijms24043344
Chicago/Turabian StyleŠimić, Ivana, Ksenija Božinović, Nina Milutin Gašperov, Mario Kordić, Ena Pešut, Luka Manojlović, Magdalena Grce, Emil Dediol, and Ivan Sabol. 2023. "Head and Neck Cancer Patients’ Survival According to HPV Status, miRNA Profiling, and Tumour Features—A Cohort Study" International Journal of Molecular Sciences 24, no. 4: 3344. https://doi.org/10.3390/ijms24043344