Abstract
This systematic review was conducted to gather evidence of preeclampsia occurring before the 20th week of gestation, additionally considering the role of PLGF and sFlt-1 in the development of the disease. In the three cases of preeclampsia before the 20th week of gestation presented in the authors’ material, all pregnancies ended up with IUFD, and the SFlt-1/PLGF ratios were significantly elevated in all women. Eligible publications were identified with searches in the PubMed, Embase, Scopus, and Web of Science databases. No date or language restrictions were made. All original peer-reviewed scientific reports were included. A total of 30 publications were included in the final report, including case reports and case series. No other publication types regarding this issue were identified. In the literature, 34 cases of preeclampsia with onset occurring before the 20th week of gestation were identified, for a final total of 37 cases. Live births were reported in 5 cases (10.52%), and there were 9 intrauterine fetal demises (24.32%), and 23 terminations of pregnancy (62.16%). Preeclampsia before the 20th week of gestation is rare but can occur. We collected all available evidence regarding this phenomenon, with 37 cases reported worldwide. We call for large-scale cohort or register-based studies to establish revised definitions or develop new ones regarding the currently unrecognized very early onset preeclampsia.
1. Introduction
Preeclampsia (PE) is a known obstetric pathology, the definition of which, due to the ongoing process of understanding its pathogenesis, is still evolving. Originally, it was known as a condition of hypertension and proteinuria, but then the definition was expanded to include liver and kidney dysfunctions, thrombocytopenia, and fetal growth restriction. In 2018, the International Society of the Study of Hypertension in Pregnancy published a definition of preeclampsia. The diagnostic criteria include newly onset hypertension ≥20 weeks of gestation, additional proteinuria, and maternal organ dysfunction or uteroplacental dysfunction [1].
The process of trophoblast invasion begins at the early stages of pregnancy. The most intense transformations take place before the 18th week of gestation. In the primary period, a structure called a cytotrophoblast shell is created, the task of which is to protect the embryo from the harmful effects of oxygen and provide nourishment without the contribution of all the mother’s blood [2,3].
After the dilatation of the spiral arteries after about 12 weeks of pregnancy, the mother’s blood flows into the uteroplacental space around the chorionic villi for the first time. A further transformation of the spiral vessels occurs, which extends from the central parts of the placenta to its peripheral parts. Moreover, the surfaces of the villi keep enlarging, thanks to which the exchange capacity of the uteroplacental compartment is constantly increasing. This process is inextricably linked to the increasing demands of the fetus [2,4,5].
Nowadays, the diagnosis of early preeclampsia is associated with the simultaneous occurrence of increased resistance in the blood flow of uterine arteries and disturbances in the angiogenesis process, which, to some extent, can be monitored using angiogenesis placental markers, such as soluble FMS-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PLGF). SFlt-1 and PLGF demonstrate altered values 6–8 weeks before clinical diagnosis [6].
Still, a criterion for the diagnosis of preeclampsia is its occurrence after the 20th week of gestation. With a better understanding of what causes this pathology, we decided that we should question this criterion and assess if a new definition of preeclampsia should be elaborated. The aim of this systematic review was to collect and assess all data regarding preeclampsia with onset before the 20th week of gestation.
It has been accepted to define preeclampsia as a condition developing after the 20th week of pregnancy. Do the symptoms of placental insufficiency really only occur in the second half of pregnancy? If the clinical picture completely coincides with preeclampsia in the first half of pregnancy, with reasonable suspicion or certainty of chorionic villi damage and features of placental insufficiency, should we not recognize that we are dealing with preeclampsia? This review aimed to investigate whether we should again modify its definition.
PLGF and sFlt-1
Placental development is a sequence of events. It starts soon after the blastocyst implantation in the maternal decidua. Sysytiotrofoblast forms the lacune, which is later filled with maternal blood. Simultaneously, extravillous trophoblast starts to invade the maternal spiral arteries, forming plugs that stop the maternal blood flow and replace the maternal muscular cells in the zona intima of the vessels and, temporally, the maternal endothelium. Arterial remodeling is controlled vastly by the immune system, namely uNK and Treg cells. What is interesting is that uNK cells have the ability to secrete angiogenic factors, including PLGF, which plays role in uNK proliferation [7]. Higher PLGF expression in uNK cells was confirmed in high-risk pregnancies by high-resistance flow in the uterine arteries [8]. A high expression of PLGF is observed in arrested implantation sites. One of the explanations for the dual role of PLGF in the development of abnormal vasculature and failed implantation may be an insufficient expression of VEGF in those cases, with the role of PLGF switching from angiogenesis to inflammation [9].
Altered arterial remodeling or arterial plug resolution leads to oxidative stress of the syncytiotrophoblasts, resulting in decreased PLGF production. Degenerative syncytiotrophoblastic cells, or syncytial knots, are known to produce large amounts of sFlt-1 [7]. The fates of 237 patients with extremely high PLGF/sFlt-1 ratio (>655) have been investigated. At inclusion, 185 of them had preeclampsia (78.1%), and the remaining mostly suffered from FGR (82.7% of the rest). The maternal complications observed were severe hypertension (19.5% with PE, 5.8% without PE), oliguria (8.1% with PE, 0% without PE), and placental abruption (8.7% with PE, 21.2% without PE) [10].
PLGF is a member of the vascular endothelial growth factor (VEGF) family. PLGF is secreted as a homodimer but can also form a heterodimer PLGF/VEGF. Members of the VEGF family are potent vascular growth factors [11].
PLGF is coded by the PGF gene, located on chromosome 14q24.3 [12]. Currently, there are four known isoforms of the PLGF: PLGF-1 contains 149 amino acids, PLGF-2 contains an additional heparin binding sequence with 21 amino acids, PLGF-3 has an in-frame insertion loop with 72amino acids, PLGF-4 has both the additional 72-amino-acid sequence of PLGF-3 and the 21-amino-acid heparin binding sequence. PLGF-1 and PLGF-3 bind primarily to VEGFR1 (Flt-1), while the PLGF-2 main receptor is the neuropilin-1 receptor (NRP). PLGF-4 may be a cell membrane-associated variant, with autocrine abilities. Isoforms-1, -2, and -3 have confirmed the ability to bind to sFlt-1 [12,13].
PLGF levels are undetectable in most healthy tissues. On the other hand, they have a role in angiogenesis in pathological conditions, such as inflammation or ischemia. Under typical conditions, PLGF expression is upregulated by hypoxia, inflammatory cytokine growth factors, and hormones—all those present during implantation and placenta development. However, hypoxia during placentation downregulates PLGF expression and upregulates sFlt-1 expression. What is more, PLGF expression in the placenta is independent of the activity of the hypoxia-induced factor (HIF)-1. The trophoblast is the main source of PLGF. Its production in the trophoblast is strongly upregulated in early pregnancy [14].
The PLGF homodimer binds to the FLT-1 (VEGFR-1). FLT-1 suppresses angiogenic signals and modulates the behavior of immune cells. It increases the proliferation, survival, and migration of the macrophages. It also promotes the expressions of cytokines, assuming a role in decidualization [14].
FLT-1 (VEGFR-1) has a higher affinity to VEGF and PLGF but lower kinase activity than VEGFR-2. VERFR-2 has lower affinity but much higher activity. VEGFR-1, therefore, plays a dual role as a weak promoter of angiogenesis via its kinase activity while depleting the pool of available VEGF for VEGFR-2 and, therefore, having an antiangiogenic effect [15]. PLGF has a binding potential to VEGFR-1 but not VEGFR-2, displacing VEGF from VEGFR-1 and increasing the availability of VEGF to VEGFR-2 [9,16].
FLT-1 is a receptor for both VEGF and PLGF. It is coded by the FLT gene, a member of the src family, located on chromosome 13q12.3. The gene name comes from its close similarity to the FMS gene. Flt-1 possesses tyrosine kinase activity, controlling cell proliferation and differentiation. The soluble form of Flt-1 (sFlt-1) is a product of alternative splicing. SFlt-1 binds to PLGF and VEGF with high affinity, decreasing its bioavailability [17].
FLT-1 co-receptor neuropilin (NRP)-1 and NRP-2 are expressed in axons, vessels, and immune cells. NRP-1 is expressed mostly in dendritic cells (DCs) and T regulatory (Treg) cells. It is constitutively expressed by CD4+CD25high natural Treg cells. It promotes prolonged interaction between Tregs and immature DCs. This interaction probably slows DC maturation and therefore promotes immune tolerance. Conversely to the production of a soluble form of FLT-1 receptor—a soluble form of the NRP-1—the sNRP-1 is detected. SNRP-1 binds to both PLGL and VEGF, also decreasing its bioavailability [14].
Activation of the FLT-1 receptor has also a role in the immune response via transcription factor NF-κB. NF-κB has binding sites in the promoter region of PLGF and can modulate its expression. NF-κB is involved in immune response, angiogenesis, and hypoxia processes present at the formation of the placenta [14].
High levels of sFLT-1 are observed in post-partum cardiomyopathy and individuals with an altered myocardial performance index. Patten et al. suggested that a high level of sFlt-1 together with poor local pro-angiogenic defense in one heart may lead to the development of the disease [18]. An altered expression of Flt-1 may be one of the factors leading to fetal demise in malaria infection [19].
SFlt-1 has multiple splice variants, but two are predominant. SFlt-1-1 (sFlt1_v1, sFlt-1-i13) is expressed in several tissues, while sFlt-1-14 (sFlt-1-v2, sFlt-1 -e15a) is expressed exclusively in a placenta. The placental expression of the sFlt-1_1 is roughly three times larger than the sFlt-1-14 splice variant. In a preeclampsia expression of both variants is increased, but the sFlt-1-1 to a larger extent [20,21].
SFlt-1 expression is regulated by the renin–angiotensin system in the placenta, and angiotensin II is a stimulator of sFlt-1. Ex vivo studies have shown the potential role of the proton pump inhibitors (esomeprazole) in mitigating this effect. In ex vivo conditions, esomeprazole decreased the expression of the sFlt-1 mRNA and the concentration of sFlt-1 in the supernatant of a healthy and a preeclamptic placenta. The probable mechanism of action may be the inhibition of the uptake of angiotensinogen or (pro)renin transport [22]. Data on the use of proton pump inhibitors in preeclamptic women show varying results [23,24,25,26].
The treatment of hypertension with alphamethyldopa had different effects on PLGF and sFlt-1. The effect also varied between preeclamptic and gestational hypertension patients. Alphamethyldopa treatment did not change the levels of either factor in the gestational hypertension patients. In the preeclamptic patients, on the other hand, the levels of sFlt-1 decreased while the PLGF remained stable. The effect was visible both in the placenta and the serum, as changes in the serum were mirrored by changes in the placenta. It is speculated that this is the effect of the alphamethyldopa stimulation of the α2β-adrenoceptors on the placenta and the myometrium, and thus, directly influences sFlt-1 production [27]. On the other hand, data regarding the mechanism of action is scarce, and this effect has not been confirmed by an ex vivo study [28].
The association between the levels of the PLGF and sFlt-1 and placenta accreta spectrum (PAS) was recently summed up in a meta-analysis. The authors concluded that the PLGF levels did not change in PAS, but the results of the studies were conflicting. The sFlt-1 was significantly decreased and not dependent on the type of PAS, and these results were consistent among studies. A suitable cut-off value has to be established to include these promising findings in clinical practice [29].
Female and male placentas have different expressions of angiogenic factors. The sex-dependent expression of a plethora of factors was found as early as the blastocyst stage. The same was confirmed for the sFlt-1 and the PLGF in the first trimester. The mothers of female fetuses had higher PLGF and sFlt-1 levels in the first trimester. This finding is concordant with the known richer vasculature of female placentas. As a result of such vasculature, female placentas have greater placental capacity [30].
2. Case Presentation
We present three cases of preeclampsia with onset before 20 weeks of gestation from our centers. Cases 1 and 2 were patients treated at the Pomeranian Medical University Hospital, in northwest Poland. The third case came from the “Zelazna” Medical Centre in Warsaw, Poland. Both hospitals are tertiary reference centers. The only inclusion criterium was the onset of the symptoms of preeclampsia before the 20th week of gestation, with no exclusion criteria (Table 1). According to Polish law, the presentation of anonymous retrospective patient data does not need bioethical committee supervision.

Table 1.
Presentation of cases. APS—antiphospholipid syndrome, FMF—Fetal Medicine Foundation, IUFD—intrauterine fetal demise, UtA—uterine artery, PI—pulsatility index, aCGH—array comparative genomic hybridization.
The results for the PE onset, comorbidities, and outcomes are presented in summary form, the presented cases, and a systematic review.
Of note, the angiogenesis markers and the uterine artery flow were markedly altered in all three cases. One woman had a high preeclampsia risk estimation, according to Fetal Medicine Foundation protocol, at the first-trimester examination (1:4).
3. Materials and Methods
The subject-related articles were processed according to Preferred Reporting Items in Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
All original scientific articles regarding the cases of atypical preeclampsia before the 20th week of gestation were assessed. We excluded letters to the editor, opinions, and non-peer-reviewed articles. All cases of preeclampsia that occurred after the 20th week of gestation were excluded.
The inclusion criteria were, similar to the classic definition, newly onset hypertension or worsening of chronic hypertension, and additional proteinuria, maternal organ dysfunction, or uteroplacental dysfunction.
On the 13 June 2021, we searched PubMed, Embase, Scopus, and Web of Science databases, using the search phrase. Search engine-specific options limiting the search to the title and abstract were used. No date or language restrictions were used. The articles we found that were eligible for this search were written in English and Spanish (languages of the authors ).
Each report was assessed independently by two authors. The PRISMA chart of the whole process is shown in Figure 1.
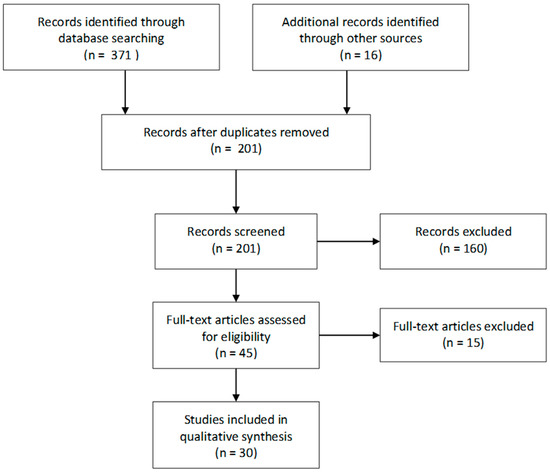
Figure 1.
PRISMA flow chart.
Two authors (IS and JPD) independently extracted data regarding atypical preeclampsia before 20 weeks of gestation. The data that were extracted from the full texts included the onset week of gestation when preeclampsia occurred, gravidity, parity, type of pregnancy (single, twin, partial molar, complete molar, or IVF), comorbidities, information on first-trimester prenatal screening, the evolution of blood pressure values, proteinuria, markers of angiogenesis, information on the uterine artery PI, and the pregnancy outcome. No missing information was assumed. All articles included in the review are case reports, and therefore, there was no risk of bias assessed.
4. Results
There were 30 papers describing 34 cases of atypical preeclampsia found in the reviewed literature that met the criteria for this systematic review. The earliest reported case of preeclampsia was at 14 weeks of gestation. The data on the onset of preeclampsia and the end of pregnancy are shown in Figure 2. There was no information on first-trimester preeclampsia screening. Most of the patients were admitted to the hospital with high blood pressure and proteinuria. Information about the post-pregnancy events was available for 12 cases—the blood pressure was normalized after pregnancy in all women who were not diagnosed with hypertension before the pregnancy. The angiogenesis markers reported in the three studies are shown in Table 2. In total, there were 23 terminations of pregnancy, 9 cases of intrauterine fetal demise, and 5 cases of preterm live deliveries, including two selective terminations of one fetus with the live birth of another twin/triplet. Two live births were cesarean sections. The majority of women had pre-pregnancy morbidities, predisposing them to the development of preeclampsia during pregnancy. The data on the outcome and maternal comorbidities are shown in Figure 3. A summary of the included studies is presented in Table 3. Rejected papers and reasons for rejection are presented in Table 4.
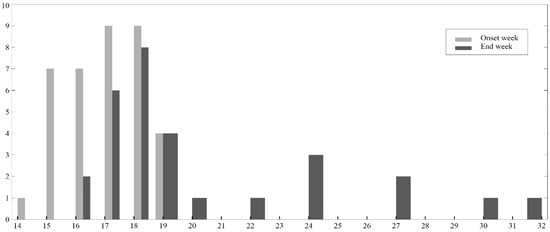
Figure 2.
Preeclampsia onset week and the week of the pregnancy end by the number of cases reported.
Table 2.
Reported angiogenesis markers. Soluble FMS-like tyrosine kinase-1 (sFlt-1)/Placental growth factor (PLGF).
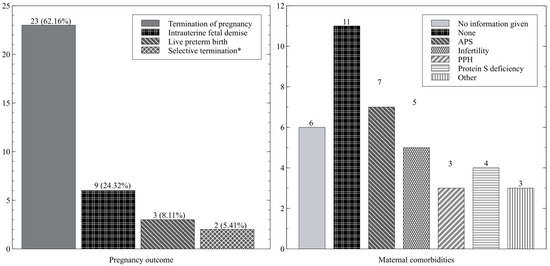
Figure 3.
Pregnancy outcome—number of cases (%); maternal comorbidities—number of cases. * Selective termination and live birth of other twin/triplets. APS—antiphospholipid syndrome, PPH—pre-pregnancy hypertension.
Table 3.
Presentation and summary of included cases. Papers (n = 30) and cases (n = 34) were included in the systematic review. HBD—hebdomas, weeks of pregnancy when pregnancy ended, IUFD—intrauterine fetal demise, LB—live birth, sFGR—selective fetal growth restriction, RDS—respiratory distress syndrome, TOP—termination of pregnancy.
Table 4.
Rejected after full-text review.
5. Discussion
The International Society of the Study of Hypertension in Pregnancy’s definition of preeclampsia excludes the possibility of preeclampsia before 20 weeks of gestation. In our work, we indicate that in all analyzed cases, preeclampsia occurred before the 20th week of pregnancy. Furthermore, we show that women can develop preeclampsia in normal and molar pregnancies.
The majority of the women who develop atypical PE had pre-existing co-morbidities, mainly anti-phospholipid syndrome, pre-pregnancy hypertension, and protein S deficiency. Infertility treatment may be a risk factor for atypical PE. This may be a factor worth considering in the development of the definition of atypical preeclampsia.
Five of the presented cases resulted in the delivery of a live-born preterm child. One may consider atypical preeclampsia as extremely severe; however, there is a chance of fetal survival.
In our presented cases, the women diagnosed with very early onset preeclampsia had severe angiogenesis imbalance, detectable by the sFlt-1/PLGF ratio. Data regarding the first-trimester preeclampsia screening were available for only one woman, with a risk of 1:4, but it would be reasonable to expect similarly high results for all women endangered with very early onset preeclampsia. The answer to the question of the effectiveness of acetylsalicylic acid prophylaxis in these cases is extremely interesting but beyond the scope of this review.
In light of the available evidence, it is not possible to assess the performance of first-trimester screening in the prediction of atypical preeclampsia. On the other hand, all our presented cases had high a highly altered PLGF/sFlt-1 index at the onset of the disease. PLGF is recommended in preeclampsia screening according to the Fetal Medicine Foundation, and therefore, we think that screening including all recommended maternal characteristics, blood pressure, uterine arteries flow, and biochemical markers, including the PLGF, may be enough to screen for atypical preeclampsia.
It should be noted that our review includes case reports only. Therefore, the assessment of study bias was impossible. We also cannot exclude publication bias. Moreover, presented cases do not fit the common definition, and therefore, it may be that some cases have not been reported due to misdiagnosis. The results of our study are affected by these limitations, but in our opinion, they rather underestimate the occurrence of atypical preeclampsia.
We performed an extensive search in four databases with very few limitations. The identified studies were inconsistent with the reported data. The extraction of some predefined data was therefore impossible, including information on first-trimester perinatal screening, markers of angiogenesis, and measures of uterine artery perfusion. To our knowledge, this is the first systematic review regarding this topic.
Based on our review, we cannot determine new criteria for the preeclampsia definition before the 20th week of pregnancy. The reviewed studies lack uterine artery Doppler flow, angiogenesis placental markers, and first-trimester preeclampsia screening data, which may become a part of the definition. A comprehensive cohort or a large-scale database study should be conducted to deliver the data required to extend the preeclampsia definition to cases before the 20th week of pregnancy.
6. Conclusions
Preeclampsia before the 20th week of gestation is rare but it can occur. We collected all available evidence regarding this phenomenon, with 37 cases reported worldwide. We call for large-scale cohort or register-based studies to establish revised definitions or develop new ones regarding the currently unrecognized very early onset preeclampsia.
Author Contributions
Title and abstract searches were conducted by J.M. and S.F. The full-text review was conducted by I.S. and J.P.-D. All discrepancies were solved by a third viewer (A.K.—inclusion, J.M.—full-text review). Conceptualization, J.M., A.K. and S.K.; methodology, J.M. and I.S.; software, J.P.-D., I.S., K.M.-P. and A.B.; validation, J.M., I.S., M.B.-J. and J.P.-D.; formal analysis, S.F.; investigation, A.C.-P., E.K. and A.B.; resources, I.S., J.P.-D. and K.M.-P.; data curation, I.S., J.P.-D., K.M.-P. and A.B.; writing—original draft preparation, J.M.; writing—review and editing, A.K. and S.K.; visualization, M.B.-J.; supervision, A.K.; project administration, S.K.; funding acquisition, S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
According to Polish law, the presentation of anonymous retrospective patient data does not need bioethical committee supervision.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Gómez, T.; Castillo-Marco, N.; Cordero, T.; Simón, C. Decidualization resistance in the origin of preeclampsia. Am. J. Obstet. Gynecol. 2022, 226, S886–S894. [Google Scholar] [CrossRef] [PubMed]
- Pijnenborg, R.; Vercruysse, L.; Hanssens, M. The Uterine Spiral Arteries In Human Pregnancy: Facts and Controversies. Placenta 2006, 27, 939–958. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.; Kim, S.H.; Cha, D.H.; Park, H.J. Defective Uteroplacental Vascular Remodeling in Preeclampsia: Key Molecular Factors Leading to Long Term Cardiovascular Disease. Int. J. Mol. Sci. 2021, 22, 11202. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.; Woods, A.; Jauniaux, E.; Kingdom, J. Rheological and Physiological Consequences of Conversion of the Maternal Spiral Arteries for Uteroplacental Blood Flow during Human Pregnancy. Placenta 2009, 30, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Cerdeira, A.S.; Redman, C.; Vatish, M. Meta-Analysis and Systematic Review to Assess the Role of Soluble FMS-Like Tyrosine Kinase-1 and Placenta Growth Factor Ratio in Prediction of Preeclampsia. Hypertension 2018, 71, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Kosińska-Kaczyńska, K. Placental Syndromes—A New Paradigm in Perinatology. Int. J. Environ. Res. Public Health 2022, 19, 7392. [Google Scholar] [CrossRef]
- Wallace, A.E.; Fraser, R.; Gurung, S.; Goulwara, S.S.; Whitley, G.S.; Johnstone, A.P.; Cartwright, J.E. Increased angiogenic factor secretion by decidual natural killer cells from pregnancies with high uterine artery resistance alters trophoblast function. Hum. Reprod. 2014, 29, 652–660. [Google Scholar] [CrossRef]
- Nejabati, H.R.; Latifi, Z.; Ghasemnejad, T.; Fattahi, A.; Nouri, M. Placental growth factor (PlGF) as an angiogenic/inflammatory switcher: Lesson from early pregnancy losses. Gynecol. Endocrinol. 2017, 33, 668–674. [Google Scholar] [CrossRef]
- Villalain, C.; Herraiz, I.; Valle, L.; Mendoza, M.; Delgado, J.L.; Vazquez-Fernandez, M.; Martinez-Uriarte, J.; Melchor, I.; Caamiña, S.; Fernandez-Oliva, A.; et al. Maternal and Perinatal Outcomes Associated With Extremely High Values for the sFlt-1 (Soluble fms-Like Tyrosine Kinase 1)/PlGF (Placental Growth Factor) Ratio. J. Am. Heart Assoc. 2020, 9, e015548. [Google Scholar] [CrossRef]
- Vuorela, P.; Hatva, E.; Lymboussaki, A.; Kaipainen, A.; Joukov, V.; Persico, M.G.; Alitalo, K.; Halmesmäki, E. Expression of Vascular Endothelial Growth Factor and Placenta Growth Factor in Human Placenta1. Biol. Reprod. 1997, 56, 489–494. [Google Scholar] [CrossRef] [PubMed]
- MIM Number: 601121: Updated 20/02/2015, access 01/01/2023. In Online Mendelian Inheritance in Man, OMIM®; Johns Hopkins University: Baltimore, MD, USA, 2015.
- Frang, H.; Hurskainen, P.; Nicolaides, K.; Sairanen, M. PlGF isoform 3 in maternal serum and placental tissue. Pregnancy Hypertens. 2019, 18, 9–13. [Google Scholar] [CrossRef]
- Albonici, L.; Benvenuto, M.; Focaccetti, C.; Cifaldi, L.; Miele, M.T.; Limana, F.; Manzari, V.; Bei, R. PlGF Immunological Impact during Pregnancy. Int. J. Mol. Sci. 2020, 21, 8714. [Google Scholar] [CrossRef] [PubMed]
- Shibuya, M. Vascular endothelial growth factor receptor-1 (VEGFR-1/Flt-1): A dual regulator for angiogenesis. Angiogenesis 2006, 9, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Chen, H.H.; Winer, J.; Houck, K.A.; Ferrara, N. Placenta growth factor. Potentiation of vascular endothelial growth factor bioactivity, in vitro and in vivo, and high affinity binding to Flt-1 but not to Flk-1/KDR. J. Biol. Chem. 1994, 269, 25646–25654. [Google Scholar] [CrossRef]
- MIM Number: 165070: Updated 24/09/2018, access 01/01/2023. In Online Mendelian Inheritance in Man, OMIM®; Johns Hopkins University: Baltimore, MD, USA, 2018.
- Patten, I.S.; Rana, S.; Shahul, S.; Rowe, G.C.; Jang, C.; Liu, L.; Hacker, M.R.; Rhee, J.S.; Mitchell, J.; Mahmood, F.; et al. Cardiac Angiogenic Imbalance Leads to Peri-partum Cardiomyopathy. Nature 2012, 485, 333–338. [Google Scholar] [CrossRef]
- Muehlenbachs, A.; Fried, M.; Lachowitzer, J.; Mutabingwa, T.K.; Duffy, P.E. Natural selection of FLT1 alleles and their association with malaria resistance in utero. Proc. Natl. Acad. Sci. USA 2008, 105, 14488–14491. [Google Scholar] [CrossRef]
- Jebbink, J.; Keijser, R.; Veenboer, G.; van der Post, J.; Ris-Stalpers, C.; Afink, G. Expression of Placental FLT1 Transcript Variants Relates to Both Gestational Hypertensive Disease and Fetal Growth. Hypertension 2011, 58, 70–76. [Google Scholar] [CrossRef]
- Souders, C.A.; Maynard, S.E.; Yan, J.; Wang, Y.; Boatright, N.K.; Sedan, J.; Balyozian, D.; Cheslock, P.S.; Molrine, D.C.; Simas, T.A.M. Circulating Levels of sFlt1 Splice Variants as Predictive Markers for the Development of Preeclampsia. Int. J. Mol. Sci. 2015, 16, 12436–12453. [Google Scholar] [CrossRef]
- Sun, Y.; Tan, L.; Neuman, R.; Broekhuizen, M.; Schoenmakers, S.; Lu, X.; Danser, A. Megalin, Proton Pump Inhibitors and the Renin–Angiotensin System in Healthy and Pre-Eclamptic Placentas. Int. J. Mol. Sci. 2021, 22, 7407. [Google Scholar] [CrossRef]
- Neuman, R.I.; Baars, M.D.; Saleh, L.; Broekhuizen, M.; Nieboer, D.; Cornette, J.; Schoenmakers, S.; Verhoeven, M.; Koch, B.C.; Russcher, H.; et al. Omeprazole Administration in Preterm Preeclampsia: A Randomized Controlled Trial to Study Its Effect on sFlt-1 (Soluble Fms-Like Tyrosine Kinase-1), PlGF (Placental Growth Factor), and ET-1 (Endothelin-1). Hypertension 2022, 79, 1297–1307. [Google Scholar] [CrossRef]
- Cluver, C.A.; Hannan, N.J.; van Papendorp, E.; Hiscock, R.; Beard, S.; Mol, B.W.; Theron, G.B.; Hall, D.R.; Decloedt, E.H.; Stander, M.; et al. Esomeprazole to treat women with preterm preeclampsia: A randomized placebo controlled trial. Am. J. Obstet. Gynecol. 2018, 219, 388.e1–388.e17. [Google Scholar] [CrossRef]
- Hastie, R.; Bergman, L.; Cluver, C.A.; Wikman, A.; Hannan, N.J.; Walker, S.P.; Wikström, A.-K.; Tong, S.; Hesselman, S. Proton Pump Inhibitors and Preeclampsia Risk Among 157 720 Women. Hypertension 2019, 73, 1097–1103. [Google Scholar] [CrossRef]
- de Alwis, N.; Fato, B.R.; Beard, S.; Binder, N.K.; Kaitu’U-Lino, T.J.; Onda, K.; Hannan, N.J. Assessment of the Proton Pump Inhibitor, Esomeprazole Magnesium Hydrate and Trihydrate, on Pathophysiological Markers of Preeclampsia in Preclinical Human Models of Disease. Int. J. Mol. Sci. 2022, 23, 9533. [Google Scholar] [CrossRef]
- Khalil, A.; Muttukrishna, S.; Harrington, K.; Jauniaux, E. Effect of Antihypertensive Therapy with Alpha Methyldopa on Levels of Angiogenic Factors in Pregnancies with Hypertensive Disorders. PLoS ONE 2008, 3, e2766. [Google Scholar] [CrossRef]
- Gangooly, S.; Muttukrishna, S.; Jauniaux, E. In-Vitro Study of the Effect of Anti-Hypertensive Drugs on Placental Hormones and Angiogenic Proteins Synthesis in Pre-Eclampsia. PLoS ONE 2014, 9, e107644. [Google Scholar] [CrossRef]
- Alzoubi, O.; Maaita, W.; Madain, Z.; Alzoubi, M.; Sweis, J.J.G.; Arar, A.R.; Sweis, N.W.G. Association between placenta accreta spectrum and third-trimester serum levels of vascular endothelial growth factor, placental growth factor, and soluble Fms-like tyrosine kinase-1: A meta-analysis. J. Obstet. Gynaecol. Res. 2022, 48, 2363–2376. [Google Scholar] [CrossRef]
- Meakin, A.; Cuffe, J.; Darby, J.; Morrison, J.; Clifton, V. Let’s Talk about Placental Sex, Baby: Understanding Mechanisms That Drive Female- and Male-Specific Fetal Growth and Developmental Outcomes. Int. J. Mol. Sci. 2021, 22, 6386. [Google Scholar] [CrossRef] [PubMed]
- Imasawa, T.; Nishiwaki, T.; Nishimura, M.; Shikama, N.; Matsumura, R.; Nagai, M.; Soyama, A.; Koike, K.; Kitamura, H.; Joh, K. A Case of “Pure” Preeclampsia With Nephrotic Syndrome Before 15 Weeks of Gestation in a Patient Whose Renal Biopsy Showed Glomerular Capillary Endotheliosis. Am. J. Kidney Dis. 2006, 48, 495–501. [Google Scholar] [CrossRef]
- Suzuki, T.; Ichikawa, D.; Nakata, M.; Watanabe, S.; Han, W.; Kohatsu, K.; Shirai, S.; Imai, N.; Koike, J.; Shibagaki, Y. Nephrotic syndrome due to preeclampsia before 20 weeks of gestation: A case report. BMC Nephrol. 2020, 21, 240. [Google Scholar] [CrossRef]
- Stefos, T.; Plachouras, N.; Mari, G.; Cosmi, E.; Lolis, D. A case of partial mole and atypical type I triploidy associated with severe HELLP syndrome at 18 weeks’ gestation. Ultrasound Obstet. Gynecol. 2002, 20, 403–404. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, N.; Shiozaki, A.; Miura, K.; Yonezawa, R.; Takemura, K.; Yoneda, S.; Masuzaki, H.; Saito, S. A triploid partial mole placenta from paternal isodisomy with a diploid fetus derived from one sperm and one oocyte may have caused angiogenic imbalance leading to preeclampsia-like symptoms at 19 weeks of gestation. Placenta 2013, 34, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Myer, E.; Hill, J. First trimester hemolysis, elevated liver enzymes, low platelets syndrome in a surrogate pregnancy. AJP Rep. 2015, 5, e212–e214. [Google Scholar] [CrossRef] [PubMed]
- Hazra, S.; Waugh, J.; Bosio, P. “Pure” pre-eclampsia before 20 weeks of gestation: A unique entity. Int. J. Obstet. Gynaecol. 2003, 110, 1034–1035. [Google Scholar] [CrossRef]
- Bornstein, E.; Barnhard, Y.; Atkin, R.; Divon, M.Y. HELLP syndrome: A rare, early presentation at 17 weeks of gestation. Obstet. Gynecol. 2007, 110, 525–527. [Google Scholar] [CrossRef]
- Alsulyman, O.M.; Amescastro, M.; Zuckerman, E.; McGehee, W.; Murphygoodwin, T. Preeclampsia and liver infarction in early pregnancy associated with the antiphospholipid syndrome. Obstet. Gynecol. 1996, 88, 644–646. [Google Scholar] [CrossRef]
- Stillman, I.E.; Karumanchi, S.A. The Glomerular Injury of Preeclampsia. J. Am. Soc. Nephrol. 2007, 18, 2281–2284. [Google Scholar] [CrossRef]
- Parrott, J.; Fields, T.A.; Parrish, M. Previable Preeclampsia Diagnosed by Renal Biopsy in Setting of Novel Diagnosis of C4 Glomerulopathy. Case Rep. Obstet. Gynecol. 2017, 2017, 8698670. [Google Scholar] [CrossRef]
- Tanaka, M.; Tsujimoto, Y.; Goto, K.; Kumahara, K.; Onishi, S.; Iwanari, S.; Fumihara, D.; Miki, S.; Ikeda, M.; Sato, K.; et al. Preeclampsia before 20 weeks of gestation: A case report and review of the literature. CEN Case Rep. 2015, 4, 55–60. [Google Scholar] [CrossRef][Green Version]
- Maya, I.D. Hypertension and proteinuria in a 17-year-old at 19 weeks’ gestation. Am. J. Kidney Dis. 2008, 51, 155–159. [Google Scholar] [CrossRef]
- Mayer-Pickel, K.; Stern, C.; Cervar-Zivkovic, M.; Schöll, W.; Moertl, M. Preeclampsia before fetal viability in women with primary antiphospholipid syndrome- materno-fetal outcomes in a series of 7 cases. J. Reprod. Immunol. 2020, 138, 103101. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.N.; Nelson, D.B.; Spong, C.Y.; McIntire, D.D.; Reddy, M.; Cunningham, F.G. 1012 Acute kidney injury in pregnancies complicated by preeclampsia with severe features. Am. J. Obstet. Gynecol. 2021, 224, S627. [Google Scholar] [CrossRef]
- Romero-Arauz, J.F.; Carranco-Salinas, C.; Leaños-Miranda, A.; Martínez-Rodríguez, O.A. Atypical preeclampsia: Case report. Ginecol. Obstet. Mex. 2014, 82, 354–360. [Google Scholar] [PubMed]
- Konstantopoulos, A.; Sfakianoudis, K.; Simopoulou, M.; Kontogeorgi, A.; Rapani, A.; Grigoriadis, S.; Pantou, A.; Bathrellos, N.; Grammatis, A.; Pantos, K. Early Onset Preeclampsia Diagnosis Prior to the 20th Week of Gestation in a Twin Pregnancy Managed via Selective Reduction of an Intrauterine Growth Restriction Fetus: A Case Report and Literature Review. Diagnostics 2020, 10, 531. [Google Scholar] [CrossRef]
- Khan, B.S.A.; Sharma, Y.; Soman, S.S.; Jandali, H.A.; Reddy, S. In vitro fertilization (IVF): Early-onset preeclampsia before 16 weeks’ gestation. J. Am. Soc. Nephrol. 2019, 30, 861. [Google Scholar]
- Thomas, W.; Griffiths, M.; Nelson-Piercy, C.; Sinnamon, K. Pre-eclampsia before 20-week gestation: Diagnosis, investigation and management. Clin. Kidney J. 2012, 5, 597–599. [Google Scholar] [CrossRef]
- Craig, K.; Pinette, M.G.; Blackstone, J.; Chard, R.; Cartin, A. Highly abnormal maternal inhibin and β-human chorionic gonadotropin levels along with severe HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome at 17 weeks’ gestation with triploidy. Am. J. Obstet. Gynecol. 2000, 182, 737–739. [Google Scholar] [CrossRef]
- Nwosu, E.C.; Ferriman, E.; McCormack, M.J.; Williams, J.H.; Gosden, C.M. Partial hydatidiform mole and hypertension associated with a live fetus—Variable presentation in two cases. Hum. Reprod. 1995, 10, 2459–2462. [Google Scholar] [CrossRef]
- Billieux, M.-H.; Petignat, P.; Fior, A.; Mhawech, P.; Blouin, J.-L.; Dahoun, S.; Vassilakos, P. Pre-eclampsia and peripartum cardiomyopathy in molar pregnancy: Clinical implication for maternally imprinted genes. Ultrasound Obstet. Gynecol. 2004, 23, 398–401. [Google Scholar] [CrossRef]
- Brittain, P.C.; Bayliss, P. Partial Hydatidiform Molar Pregnancy Presenting with Severe Preeclampsia Prior to Twenty Weeks Gestation: A Case Report and Review of the Literature. Mil. Med. 1995, 160, 42–44. [Google Scholar] [CrossRef]
- Saad, O.E.; Tanouti, S.; Bkiyar, H.; Mimouni, A.; Housni, B. Near death 18 weeks preeclampsia in molar pregnancy. Int. J. Reprod. Contracept. Obstet. Gynecol. 2020, 9, 877. [Google Scholar] [CrossRef]
- Rahimpanah, F.; Smoleniec, J. Partial mole, triploidy and proteinuric hypertension: Two case reports. Aust. N. Z. J. Obstet. Gynaecol. 2000, 40, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Nugent, C.E.; Punch, M.R.; Barr, M.; LeBlanc, L.; Johnson, M.P.; Evans, M.I. Persistence of partial molar placenta and severe preeclampsia after selective termination in a twin pregnancy. Obstet. Gynecol. 1996, 87, 829–831. [Google Scholar]
- Prasannan-Nair, C.; Reynolds, S.F.; Budden, G. Partial molar pregnancy with severe pre-eclampsia at 19 weeks’ gestation. J. Obstet. Gynaecol. 2006, 26, 817. [Google Scholar] [CrossRef]
- Sherer, D.M.; Dalloul, M.; Stimphil, R.; Hellmann, M.; Khoury-Collado, F.; Osho, J.; Fomitcheva, L.; Brennan, K.J.; Abulafia, O. Acute Onset of Severe Hemolysis, Elevated Liver Enzymes, and Low Platelet Count Syndrome in a Patient with a Partial Hydatidiform Mole at 17 Weeks Gestation. Am. J. Perinatol. 2006, 23, 163–166. [Google Scholar] [CrossRef]
- Haram, K.; Trovik, J.; Sandset, P.M.; Hordnes, K. Severe syndrome of hemolysis, elevated liver enzymes and low platelets (HELLP) in the 18th week of pregnancy associated with the antiphospholipid–antibody syndrome. Acta Obstet. Gynecol. Scand. 2003, 82, 679–680. [Google Scholar] [CrossRef]
- McMahon, L.P.; Smith, J. The HELLP Syndrome at 16 weeks’Gestation: Possible Association with the Antiphospholipid Syndrome. Aust. N. Z. J. Obstet. Gynaecol. 1997, 37, 313–314. [Google Scholar] [CrossRef]
- De Weg, J.B.; De Groot, C.; Pajkrt, E.; De Vries, H.; De Boer, M. 143. Recovery of second trimester preeclampsia in triplet after foetal reduction; a case history and review of the literature. Pregnancy Hypertens. 2018, 13, S84. [Google Scholar] [CrossRef]
- Stevens, A.B.; Brasuell, D.M.; Higdon, R.N. Atypical preeclampsia—Gestational proteinuria. J. Fam. Med. Prim. Care 2017, 6, 669–671. [Google Scholar] [CrossRef]
- Albayrak, M.; Özdemir, I.; Demiraran, Y.; Dikici, S. Atypical preeclampsia and eclampsia: Report of four cases and review of the literature. J. Turk. Ger. Gynecol. Assoc. Artemis 2010, 11, 115–117. [Google Scholar] [CrossRef]
- Castelazo-Morales, E.; Monzalbo-Núñez, D.E.; López-Rioja, M.J.; Castelazo-Alatorre, S. Atypical preeclampsia and perinatal success: A case report. Ginecol. Obstet. Mex. 2014, 82, 70–74. [Google Scholar]
- Ditisheim, A.; Boulvain, M.; Irion, O.; Pechère-Bertschi, A. Atypical presentation of preeclampsia. Rev. Med. Suisse. 2015, 11, 1655–1658. [Google Scholar] [PubMed]
- Quintero-Loaiza, C.A.; Parra-Saavedra, M.; Molina-Giraldo, S.; Figueras, F.; Rojas-Arias, J.L.; Ortiz-López, L.D.; Orduña-Aparicio, W.J.; Acuña-Osorio, E.; Franco-Hernández, A. Characterization of atypical preeclampsia. Fetal Diagn. Ther. 2015, 38, 119–125. [Google Scholar] [CrossRef]
- Valle Tejero, A.; Monfort, I.R.; Calvo, P.; Aguilar, A.; Romero, A.; Diago, V.; Perales, A. Classic vs Atipic HELLP sydrome. Obstetric and perinatal results. J. Perinat. Med. 2015, 43, 432–1299. [Google Scholar] [CrossRef]
- Sibai, B.M.; Stella, C.L. Diagnosis and management of atypical preeclampsia-eclampsia. Am. J. Obstet. Gynecol. 2009, 200, 481.e1–481.e7. [Google Scholar] [CrossRef]
- van Scheltinga, J.A.T.; Krabbendam, I.; Spaanderman, M.E. Differentiating between gestational and chronic hypertension; An explorative study. Acta Obstet. Gynecol. Scand. 2013, 92, 312–317. [Google Scholar] [CrossRef]
- Van Scheltinga, J.A.T.; Krabbendam, I.; Lotgering, F.K.; Spaanderman, M.E.A. Hypertension before 20 weeks gestation and chronic hypertension. Reprod. Sci. 2010, 17, 238A. [Google Scholar] [CrossRef]
- Seguro, F.; Duly Bouhanick, B.; Chamontin, B.; Amar, J. Management of arterial hypertension before 20 weeks gestation in pregnant women. Presse. Med. 2016, 45, 627–630. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, H.; Long, Y.; Ma, Q.; Chen, R. Plasma Level of Placenta-Derived Macrophage-Stimulating Protein -Chain in Preeclampsia before 20 Weeks of Pregnancy. PLoS ONE 2016, 11, e0161626. [Google Scholar] [CrossRef]
- Sáez Cantero, V.L.C. Preeclampsia and eclampsia with atypical presentation. Prog. Obstet. Ginecol. 2012, 55, 326–328. [Google Scholar] [CrossRef]
- Stella, C.L.; Sibai, B.M. Preeclampsia: Diagnosis and management of the atypical presentation. J. Matern. Fetal. Neonatal. Med. 2006, 19, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Sibai, B.M.; Abdella, T.H.; Taylor, H.A. Eclampsia in the first half of pregnancy. A report of three cases and review of the literature. J. Reprod. Med. 1982, 27, 706–708. [Google Scholar] [PubMed]
- Garland, J.S.; Smith, G.N.; Moran, S.M. TMA in pregnancy before 20 weeks gestation: Is this preeclampsia or primary TMA? Can. J. Kidney Health Dis. 2020, 7, 8–9. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).