
Metabolomics and Cardiovascular Risk in Patients with Heart Failure: A Systematic Review and Meta-Analysis

 , , , and
, , , and 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Screening
2.4. Data Collection Process and Data Items
2.5. Data Aggregation Approach
2.6. Risk of Bias
2.7. Data Analysis
3. Results
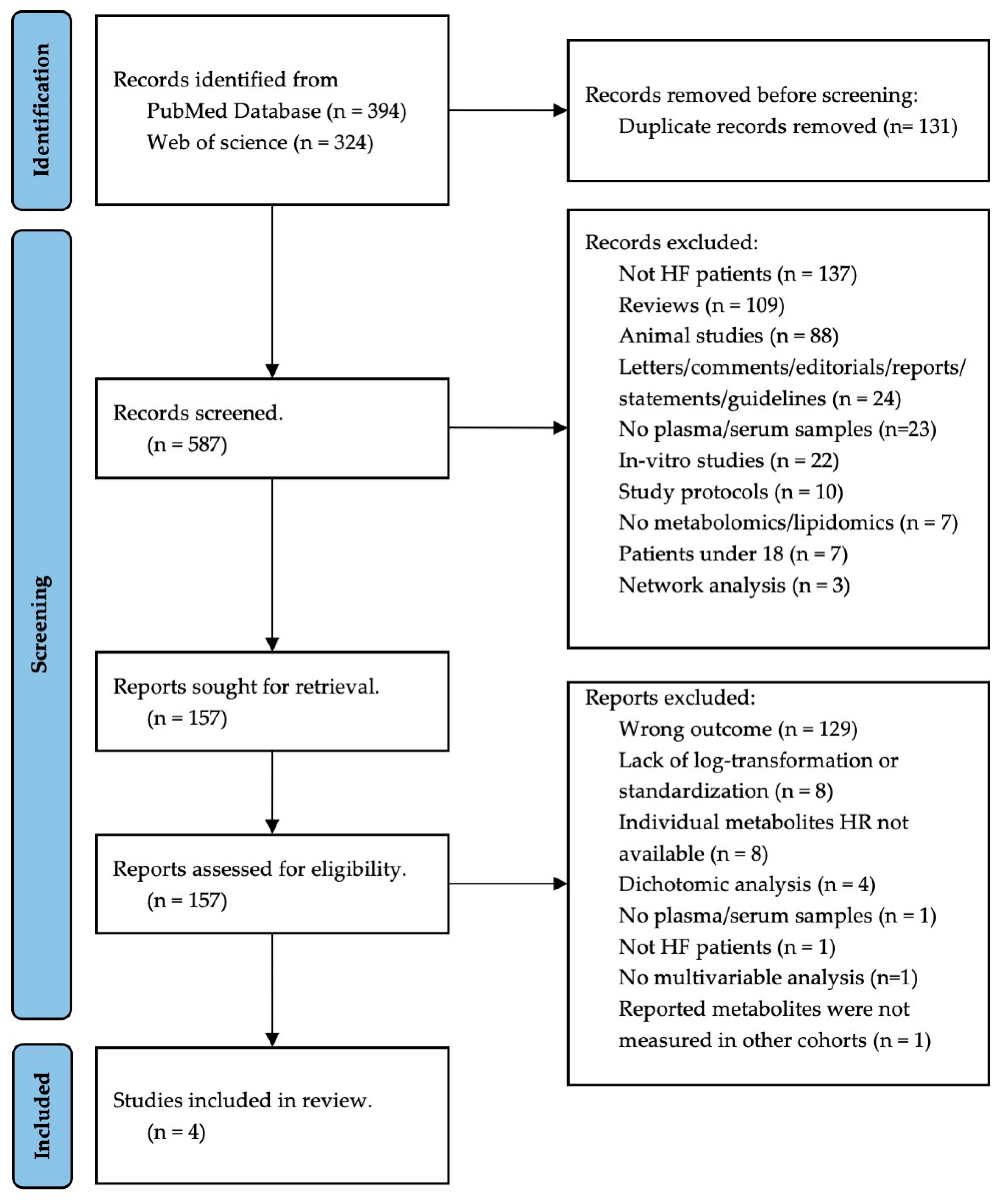
3.1. Study Selection
3.2. Study Endpoints
3.3. Patients’ Characteristics
3.4. Metabolomics Characteristics
3.5. Explored Metabolites
3.6. Risk of Bias in Studies
3.7. Data Pre-Processing
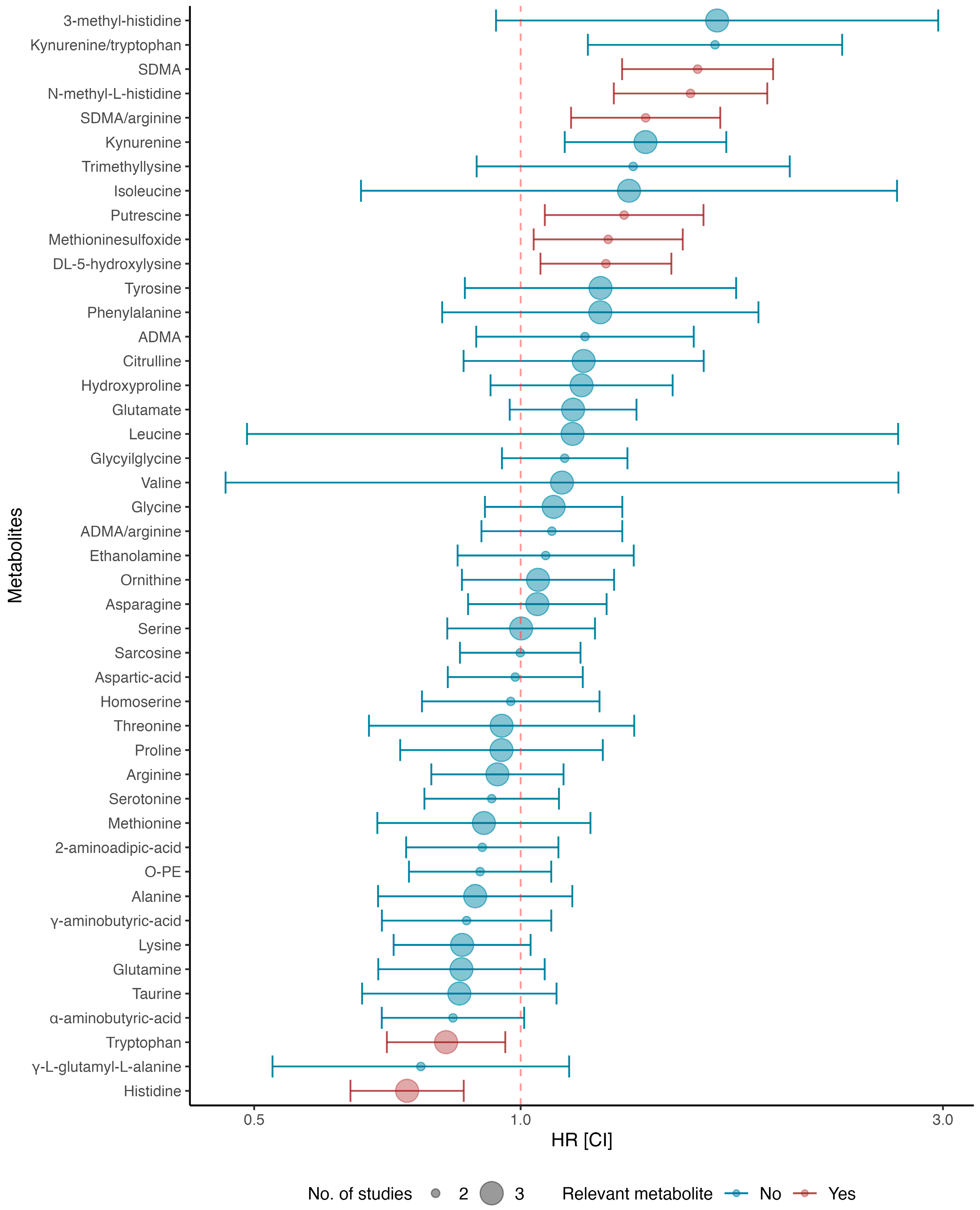
3.8. Primary Analysis
4. Discussion
4.1. Symmetric Dimethylarginine (SDMA) and SDMA/Arginine
4.2. Putrescine
4.3. N-Methyl-Histidine
4.4. Hydroxylysine
4.5. Methionine Sulfoxide
4.6. Histidine
4.7. Tryptophan
4.8. Taking Metabolomics to a Clinical Setting
4.9. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Norhammar, A.; Bodegard, J.; Vanderheyden, M.; Tangri, N.; Karasik, A.; Maggioni, A.P.; Sveen, K.A.; Taveira-Gomes, T.; Botana, M.; Hunziker, L.; et al. Prevalence, Outcomes and Costs of a Contemporary, Multinational Population with Heart Failure. Heart 2023, 109, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global Burden of Heart Failure: A Comprehensive and Updated Review of Epidemiology. Cardiovasc. Res. 2023, 118, 3272–3287. [Google Scholar] [CrossRef] [PubMed]
- Tsutsui, H.; Albert, N.M.; Coats, A.J.S.; Anker, S.D.; Bayes-Genis, A.; Butler, J.; Chioncel, O.; Defilippi, C.R.; Drazner, M.H.; Felker, G.M.; et al. Natriuretic Peptides: Role in the Diagnosis and Management of Heart Failure: A Scientific Statement from the Heart Failure Association of the European Society of Cardiology, Heart Failure Society of America and Japanese Heart Failure Society. Eur. J. Heart Fail. 2023, 25, 616–631. [Google Scholar] [CrossRef] [PubMed]
- Buchan, T.A.; Ching, C.; Foroutan, F.; Malik, A.; Daza, J.F.; Hing, N.N.F.; Siemieniuk, R.; Evaniew, N.; Orchanian-Cheff, A.; Ross, H.J.; et al. Prognostic Value of Natriuretic Peptides in Heart Failure: Systematic Review and Meta-Analysis. Heart Fail. Rev. 2022, 27, 645–654. [Google Scholar] [CrossRef]
- Xue, Y.; Clopton, P.; Peacock, W.F.; Maisel, A.S. Serial Changes in High-sensitive Troponin I Predict Outcome in Patients with Decompensated Heart Failure. Eur. J. Heart Fail. 2011, 13, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Castiglione, V.; Borrelli, C.; Saccaro, L.F.; Franzini, M.; Masi, S.; Emdin, M.; Giannoni, A. Oxidative Stress and Inflammation in the Evolution of Heart Failure: From Pathophysiology to Therapeutic Strategies. Eur. J. Prev. Cardiol. 2020, 27, 494–510. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.L.; Grodin, J.L.; Wu, Y.; Hernandez, A.F.; Butler, J.; Metra, M.; Felker, G.M.; Voors, A.A.; McMurray, J.J.; Armstrong, P.W.; et al. Increased Mortality with Elevated Plasma Endothelin-1 in Acute Heart Failure: An ASCEND-HF Biomarker Substudy: Endothelin-1 in Acute HF. Eur. J. Heart Fail. 2016, 18, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Zile, M.R.; DeSantis, S.M.; Baicu, C.F.; Stroud, R.E.; Thompson, S.B.; McClure, C.D.; Mehurg, S.M.; Spinale, F.G. Plasma Biomarkers That Reflect Determinants of Matrix Composition Identify the Presence of Left Ventricular Hypertrophy and Diastolic Heart Failure. Circ. Heart Fail. 2011, 4, 246–256. [Google Scholar] [CrossRef]
- Nymo, S.H.; Aukrust, P.; Kjekshus, J.; McMurray, J.J.V.; Cleland, J.G.F.; Wikstrand, J.; Muntendam, P.; Wienhues-Thelen, U.; Latini, R.; Askevold, E.T.; et al. Limited Added Value of Circulating Inflammatory Biomarkers in Chronic Heart Failure. JACC-Heart Fail. 2017, 5, 256–264. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Shah, S.H.; Corwin, E.J.; Fiehn, O.; Fitzgerald, R.L.; Gerszten, R.E.; Illig, T.; Rhee, E.P.; Srinivas, P.R.; Wang, T.J.; et al. Potential Impact and Study Considerations of Metabolomics in Cardiovascular Health and Disease: A Scientific Statement from the American Heart Association. Circ.-Cardiovasc. Gene 2017, 10, e000032. [Google Scholar] [CrossRef]
- McGarrah, R.W.; Crown, S.B.; Zhang, G.-F.; Shah, S.H.; Newgard, C.B. Cardiovascular Metabolomics. Circ. Res. 2018, 122, 1238–1258. [Google Scholar] [CrossRef]
- Xie, H.; Zhang, B.; Xie, M.; Li, T. Circulating Metabolic Signatures of Heart Failure in Precision Cardiology. Precis. Clin. Med. 2023, 6, pbad005. [Google Scholar] [CrossRef]
- Bayes-Genis, A.; Liu, P.P.; Lanfear, D.E.; De Boer, R.A.; González, A.; Thum, T.; Emdin, M.; Januzzi, J.L. Omics Phenotyping in Heart Failure: The next Frontier. Eur. Heart J. 2020, 41, 3477–3484. [Google Scholar] [CrossRef] [PubMed]
- Lanfear, D.E.; Gibbs, J.J.; Li, J.; She, R.; Petucci, C.; Culver, J.A.; Tang, W.H.W.; Pinto, Y.M.; Williams, L.K.; Sabbah, H.N.; et al. Targeted Metabolomic Profiling of Plasma and Survival in Heart Failure Patients. JACC Heart Fail. 2017, 5, 823–832. [Google Scholar] [CrossRef]
- McGranaghan, P.; Düngen, H.; Saxena, A.; Rubens, M.; Salami, J.; Radenkovic, J.; Bach, D.; Apostolovic, S.; Loncar, G.; Zdravkovic, M.; et al. Incremental Prognostic Value of a Novel Metabolite-based Biomarker Score in Congestive Heart Failure Patients. ESC Heart Fail. 2020, 7, 3029–3039. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wishart, D.S.; Guo, A.; Oler, E.; Wang, F.; Anjum, A.; Peters, H.; Dizon, R.; Sayeeda, Z.; Tian, S.; Lee, B.L.; et al. HMDB 5.0: The Human Metabolome Database for 2022. Nucleic Acids. Res. 2022, 50, D622–D631. [Google Scholar] [CrossRef]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 20 October 2023).
- Higgins, J.P.T. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- R Core Team. R. A Language and Environment for Stastistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.r-project.org/ (accessed on 20 May 2024).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Truby, L.K.; Regan, J.A.; Giamberardino, S.N.; Ilkayeva, O.; Bain, J.; Newgard, C.B.; O’Connor, C.M.; Felker, G.M.; Kraus, W.E.; McGarrah, R.W.; et al. Circulating Long Chain Acylcarnitines and Outcomes in Diabetic Heart Failure: An HF-ACTION Clinical Trial Substudy. Cardiovasc. Diabetol. 2021, 20, 161. [Google Scholar] [CrossRef] [PubMed]
- Cediel, G.; Teis, A.; Codina, P.; Julve, J.; Domingo, M.; Santiago-Vacas, E.; Castelblanco, E.; Amigó, N.; Lupón, J.; Mauricio, D.; et al. GlycA and GlycB as Inflammatory Markers in Chronic Heart Failure. Am. J. Cardiol. 2022, 181, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-H.; Cheng, M.-L.; Liu, M.-H.; Shiao, M.-S.; Hsu, K.-H.; Huang, Y.-Y.; Lin, C.-C.; Lin, J.-F. Increased P-Cresyl Sulfate Level Is Independently Associated with Poor Outcomes in Patients with Heart Failure. Heart Vessel. 2016, 31, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Hofbauer, T.M.; Distelmaier, K.; Muqaku, B.; Spinka, G.; Seidl, V.; Arfsten, H.T.; Hagn, G.; Meier-Menches, S.; Bartko, P.E.; Pavo, N.; et al. Metabolomics Implicate Eicosanoids in Severe Functional Mitral Regurgitation. ESC Heart Fail. 2023, 10, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-H.; Cheng, M.-L.; Liu, M.-H. Simplified Plasma Essential Amino Acid-Based Profiling Provides Metabolic Information and Prognostic Value Additive to Traditional Risk Factors in Heart Failure. Amino Acids. 2018, 50, 1739–1748. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Shui, B.; Zhao, Q.; Hu, Z.; Shu, Q.; Su, M.; Zhang, Y.; Ni, Y. Quantitative Metabolomics Reveals Heart Failure with Midrange Ejection Fraction as a Distinct Phenotype of Heart Failure. Can. J. Cardiol. 2021, 37, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Nayak, A.; Liu, C.; Mehta, A.; Ko, Y.; Tahhan, A.S.; Dhindsa, D.S.; Uppal, K.; Jones, D.P.; Butler, J.; Morris, A.A.; et al. N8-Acetylspermidine: A Polyamine Biomarker in Ischemic Cardiomyopathy with Reduced Ejection Fraction. J. Am. Heart Assoc. 2020, 9, e016055. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Li, Y.; Wang, Y.; You, H.; Hui, P.; Zheng, Y.; Du, J. Increased Branched-Chain Amino Acid Levels Are Associated with Long-Term Adverse Cardiovascular Events in Patients with STEMI and Acute Heart Failure. Life Sci. 2018, 209, 167–172. [Google Scholar] [CrossRef]
- Zhang, Y.; Blasco-Colmenares, E.; Harms, A.C.; London, B.; Halder, I.; Singh, M.; Dudley, S.C.; Gutmann, R.; Guallar, E.; Hankemeier, T.; et al. Serum Amine-Based Metabolites and Their Association with Outcomes in Primary Prevention Implantable Cardioverter-Defibrillator Patients. Europace 2016, 18, 1383–1390. [Google Scholar] [CrossRef]
- Zhang, Y.; Guallar, E.; Blasco-Colmenares, E.; Harms, A.C.; Vreeken, R.J.; Hankemeier, T.; Tomaselli, G.F.; Cheng, A. Serum-Based Oxylipins Are Associated with Outcomes in Primary Prevention Implantable Cardioverter Defibrillator Patients. PLoS ONE 2016, 11, e0157035. [Google Scholar] [CrossRef] [PubMed]
- Kouzu, H.; Katano, S.; Yano, T.; Ohori, K.; Nagaoka, R.; Inoue, T.; Takamura, Y.; Ishigo, T.; Watanabe, A.; Koyama, M.; et al. Plasma Amino Acid Profiling Improves Predictive Accuracy of Adverse Events in Patients with Heart Failure. ESC Heart Fail. 2021, 8, 5045–5056. [Google Scholar] [CrossRef] [PubMed]
- Karaman, I. Preprocessing and Pretreatment of Metabolomics Data for Statistical Analysis. In Metabolomics: From Fundamentals to Clinical Applications; Sussulini, A., Ed.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2017; Volume 965, pp. 145–161. [Google Scholar]
- McGranaghan, P.; Saxena, A.; Rubens, M.; Radenkovic, J.; Bach, D.; Schleußner, L.; Pieske, B.; Edelmann, F.; Trippel, T.D. Predictive Value of Metabolomic Biomarkers for Cardiovascular Disease Risk: A Systematic Review and Meta-Analysis. Biomarkers 2020, 25, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Canela, M.; Hruby, A.; Clish, C.B.; Liang, L.; Martínez-González, M.A.; Hu, F.B. Comprehensive Metabolomic Profiling and Incident Cardiovascular Disease: A Systematic Review. J. Am. Heart Assoc. 2017, 6, e005705. [Google Scholar] [CrossRef] [PubMed]
- Morales, Y.; Cáceres, T.; May, K.; Hevel, J.M. Biochemistry and Regulation of the Protein Arginine Methyltransferases (PRMTs). Arch. Biochem. Biophys. 2016, 590, 138–152. [Google Scholar] [CrossRef] [PubMed]
- Tain, Y.; Hsu, C. Toxic Dimethylarginines: Asymmetric Dimethylarginine (ADMA) and Symmetric Dimethylarginine (SDMA). Toxins 2017, 9, 92. [Google Scholar] [CrossRef] [PubMed]
- Bode-Böger, S.M.; Scalera, F.; Kielstein, J.T.; Martens-Lobenhoffer, J.; Breithardt, G.D.; Fobker, M.; Reinecke, H. Symmetrical Dimethylarginine: A New Combined Parameter for Renal Function and Extent of Coronary Artery Disease. J. Am. Soc. Nephrol. 2006, 17, 1128–1134. [Google Scholar]
- Rastaldo, R.; Pagliaro, P.; Cappello, S.; Penna, C.; Mancardi, D.; Westerhof, N.; Losano, G. Nitric Oxide and Cardiac Function. Life Sci. 2007, 81, 779–793. [Google Scholar] [CrossRef]
- Schlesinger, S.; Sonntag, S.R.; Lieb, W.; Maas, R. Asymmetric and Symmetric Dimethylarginine as Risk Markers for Total Mortality and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Studies. PLoS ONE 2016, 11, e0165811. [Google Scholar] [CrossRef]
- Potočnjak, I.; Radulović, B.; Degoricija, V.; Trbušić, M.; Pregartner, G.; Berghold, A.; Meinitzer, A.; Frank, S. Serum Concentrations of Asymmetric and Symmetric Dimethylarginine Are Associated with Mortality in Acute Heart Failure Patients. Int. J. Cardiol. 2018, 261, 109–113. [Google Scholar] [CrossRef]
- Flamigni, F.; Rossoni, C.; Stefanelli, C.; Caldarera, C. Polyamine Metabolism and Function in the Heart. J. Mol. Cell. Cardiol. 1986, 18, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Pegg, A.E. Mammalian Polyamine Metabolism and Function. IUBMB Life 2009, 61, 880–894. [Google Scholar] [CrossRef] [PubMed]
- Moinard, C.; Cynober, L.; Debandt, J. Polyamines: Metabolism and Implications in Human Diseases. Clin. Nutr. 2005, 24, 184–197. [Google Scholar] [CrossRef] [PubMed]
- Perin, A.; Sessa, A.; Desiderio, M.A. Polyamine Levels and Diamine Oxidase Activity in Hypertrophic Heart of Spontaneously Hypertensive Rats and of Rats Treated with Isoproterenol. BBA-Gen. Subj. 1983, 755, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Meana, C.; Rubín, J.M.; Bordallo, C.; Suárez, L.; Bordallo, J.; Sánchez, M. Correlation between Endogenous Polyamines in Human Cardiac Tissues and Clinical Parameters in Patients with Heart Failure. J. Cell. Mol. Med. 2016, 20, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Sadoshima, J. Mechanisms of Physiological and Pathological Cardiac Hypertrophy. Nat. Rev. Cardiol. 2018, 15, 387–407. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Daitoku, H.; Uetake, T.; Kako, K.; Fukamizu, A. Histidine Nτ-Methylation Identified as a New Posttranslational Modification in Histone H2A at His-82 and H3 at His-39. J. Biol. Chem. 2023, 299, 105131. [Google Scholar] [CrossRef] [PubMed]
- Davydova, E.; Shimazu, T.; Schuhmacher, M.K.; Jakobsson, M.E.; Willemen, H.L.D.M.; Liu, T.; Moen, A.; Ho, A.Y.Y.; Małecki, J.; Schroer, L.; et al. The Methyltransferase METTL9 Mediates Pervasive 1-Methylhistidine Modification in Mammalian Proteomes. Nat. Commun. 2021, 12, 891. [Google Scholar] [CrossRef] [PubMed]
- Razavi, A.C.; Bazzano, L.A.; He, J.; Whelton, S.P.; Rebholz, C.M.; Fernandez, C.; Krousel-Wood, M.; Li, C.; Shi, M.; Nierenberg, J.L.; et al. Race Modifies the Association between Animal Protein Metabolite 1-Methylhistidine and Blood Pressure in Middle-Aged Adults: The Bogalusa Heart Study. J. Hypertens. 2020, 38, 2435–2442. [Google Scholar] [CrossRef]
- Razavi, A.C.; Bazzano, L.A.; He, J.; Fernandez, C.; Whelton, S.P.; Krousel-Wood, M.; Li, S.; Nierenberg, J.L.; Shi, M.; Li, C.; et al. Novel Findings from a Metabolomics Study of Left Ventricular Diastolic Function: The Bogalusa Heart Study. J. Am. Heart Assoc. 2020, 9, e015118. [Google Scholar] [CrossRef]
- Hakuno, D.; Hamba, Y.; Toya, T.; Adachi, T. Plasma Amino Acid Profiling Identifies Specific Amino Acid Associations with Cardiovascular Function in Patients with Systolic Heart Failure. PLoS ONE 2015, 10, e0117325. [Google Scholar] [CrossRef] [PubMed]
- 55. In Junqueira’s Basic Histology, 15th ed.; McGraw-Hill: New York, NY, USA, 2018; pp. 103–108.
- Krane, S.M.; Kantrowitz, F.G.; Byrne, M.; Pinnell, S.R.; Singer, F.R. Urinary Excretion of Hydroxylysine and Its Glycosides as an Index of Collagen Degradation. J. Clin. Investig. 1977, 59, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Lijnen, P.J.; Maharani, T.; Finahari, N.; Prihadi, J.S. Serum Collagen Markers and Heart Failure. Cardiovasc. Haematol. Disord. -Drug Targets 2012, 12, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Moskovitz, J.; Smith, A. Methionine Sulfoxide and the Methionine Sulfoxide Reductase System as Modulators of Signal Transduction Pathways: A Review. Amino Acids 2021, 53, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Kodera, Y.; Saito, T.; Fujimoto, K.; Momozono, A.; Hayashi, A.; Kamata, Y.; Shichiri, M. Methionine Sulfoxides in Serum Proteins as Potential Clinical Biomarkers of Oxidative Stress. Sci. Rep. 2016, 6, 38299. [Google Scholar] [CrossRef] [PubMed]
- Picot, C.R.; Perichon, M.; Lundberg, K.C.; Friguet, B.; Szweda, L.I.; Petropoulos, I. Alterations in Mitochondrial and Cytosolic Methionine Sulfoxide Reductase Activity during Cardiac Ischemia and Reperfusion. Exp. Gerontol. 2006, 41, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Holeček, M. Histidine in Health and Disease: Metabolism, Physiological Importance, and Use as a Supplement. Nutrients 2020, 12, 848. [Google Scholar] [CrossRef]
- Hartman, P.E.; Hartman, Z.; Ault, K.T. Scavenging of singlet molecular oxygen by imidazole compounds: High and sustained activities of carboxy terminal histidine dipeptides and exceptional activity of imidazole-4-acetic acid. Photochem. Photobiol. 1990, 51, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Edelman, J.J.B.; Seco, M.; Dunne, B.; Matzelle, S.J.; Murphy, M.; Joshi, P.; Yan, T.D.; Wilson, M.K.; Bannon, P.G.; Vallely, M.P.; et al. Custodiol for Myocardial Protection and Preservation: A Systematic Review. Ann. Cardiothorac. Surg. 2013, 2, 717–728. [Google Scholar]
- Liu, C.; Li, R.; Liu, Y.; Li, Z.; Sun, Y.; Yin, P.; Huang, R. Characteristics of Blood Metabolic Profile in Coronary Heart Disease, Dilated Cardiomyopathy and Valvular Heart Disease Induced Heart Failure. Front. Cardiovasc. Med. 2021, 7, 622236. [Google Scholar] [CrossRef]
- Anguita, E.; Chaparro, A.; Candel, F.J.; Ramos-Acosta, C.; Martínez-Micaelo, N.; Amigó, N.; Torrejón, M.J.; Llopis-García, G.; Suárez-Cadenas, M.D.M.; Matesanz, M.; et al. Biomarkers of Stable and Decompensated Phases of Heart Failure with Preserved Ejection Fraction. Int. J. Cardiol. 2022, 361, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Grifka-Walk, H.M.; Jenkins, B.R.; Kominsky, D.J. Amino Acid Trp: The Far Out Impacts of Host and Commensal Tryptophan Metabolism. Front. Immunol. 2021, 12, 653208. [Google Scholar] [CrossRef] [PubMed]
- Lund, A.; Nordrehaug, J.E.; Slettom, G.; Solvang, S.-E.H.; Pedersen, E.K.; Midttun, Ø.; Ulvik, A.; Ueland, P.M.; Nygård, O.; Giil, L.M. Correction: Plasma Kynurenines and Prognosis in Patients with Heart Failure. PLoS ONE 2020, 15, e0230056. [Google Scholar] [CrossRef]
- Razquin, C.; Ruiz-Canela, M.; Toledo, E.; Hernández-Alonso, P.; Clish, C.B.; Guasch-Ferré, M.; Li, J.; Wittenbecher, C.; Dennis, C.; Alonso-Gómez, A.; et al. Metabolomics of the Tryptophan–Kynurenine Degradation Pathway and Risk of Atrial Fibrillation and Heart Failure: Potential Modification Effect of Mediterranean Diet. Am. J. Clin. Nutr. 2021, 114, 1646–1654. [Google Scholar] [CrossRef] [PubMed]
- Konishi, M.; Ebner, N.; Springer, J.; Schefold, J.C.; Doehner, W.; Dschietzig, T.B.; Anker, S.D.; Von Haehling, S. Impact of Plasma Kynurenine Level on Functional Capacity and Outcome in Heart Failure—Results from Studies Investigating Co-Morbidities Aggravating Heart Failure (SICA-HF). Circ. J. 2017, 81, 52–61. [Google Scholar] [CrossRef]
- Trifonova, O.P.; Maslov, D.L.; Balashova, E.E.; Lokhov, P.G. Current State and Future Perspectives on Personalized Metabolomics. Metabolites 2023, 13, 67. [Google Scholar] [CrossRef]
- Fiehn, O.; Robertson, D.; Griffin, J.; Van Der Werf, M.; Nikolau, B.; Morrison, N.; Sumner, L.W.; Goodacre, R.; Hardy, N.W.; Taylor, C.; et al. The Metabolomics Standards Initiative (MSI). Metabolomics 2007, 3, 175–178. [Google Scholar] [CrossRef]
- Salek, R.M.; Neumann, S.; Schober, D.; Hummel, J.; Billiau, K.; Kopka, J.; Correa, E.; Reijmers, T.; Rosato, A.; Tenori, L.; et al. COordination of Standards in MetabOlomicS (COSMOS): Facilitating Integrated Metabolomics Data Access. Metabolomics 2015, 11, 1587–1597. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Study Design and Name | Population | Primary Outcome | No. of Events/ No. of Patients | Median Follow-Up (Years) | Platform | Sample | Ref. |
|---|---|---|---|---|---|---|---|
| Cohort | Patients > 18 years with first-time STEMI, presented within 12 h of onset of chest pain, and AHF. Exclusion criteria were as follows:
| All-cause mortality or heart failure hospitalization | 53/138 | 2.04 | LC-MS | Plasma | [31] |
| GRADE cohort | Patients > 18 years with the following:
| All-cause mortality | 39/240 | 3.7 | UPLC-MS/MS | serum | [32] |
| PROSE-ICD cohort | Patients 18–80 years of age referred for primary prevention ICD implantation who met one of the following criteria:
| All-cause mortality | 120/402 | 5.5 | UPLC-MS/MS | serum | [32] |
| PROSE-ICD cohort | Patients 18–80 years of age referred for primary prevention ICD implantation who met one of the following criteria:
| All-cause mortality | 161/479 | 6.3 | LC-MS | serum | [33] |
| Retrospective Cohort | HF patients diagnosed according to the 2016 ESC Guidelines. Exclusion criteria were as follows:
| All-cause death orunscheduled readmission due to worsening HF or lethal arrhythmia | 40/301 | 1.04 * | UPLC | Plasma | [34] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neves, L.S.; Saraiva, F.; Ferreira, R.; Leite-Moreira, A.; Barros, A.S.; Diaz, S.O. Metabolomics and Cardiovascular Risk in Patients with Heart Failure: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2024, 25, 5693. https://doi.org/10.3390/ijms25115693
Neves LS, Saraiva F, Ferreira R, Leite-Moreira A, Barros AS, Diaz SO. Metabolomics and Cardiovascular Risk in Patients with Heart Failure: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2024; 25(11):5693. https://doi.org/10.3390/ijms25115693
Chicago/Turabian StyleNeves, Leonel Sousa, Francisca Saraiva, Rita Ferreira, Adelino Leite-Moreira, António S. Barros, and Sílvia O. Diaz. 2024. "Metabolomics and Cardiovascular Risk in Patients with Heart Failure: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 25, no. 11: 5693. https://doi.org/10.3390/ijms25115693