
Comparing the HER2 Status of the Primary Tumor to That of Disseminated Tumor Cells in Early Breast Cancer

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. HER2 Status of PT and DTCs
2.3. Systemic Therapy and HER2 Status of DTCs
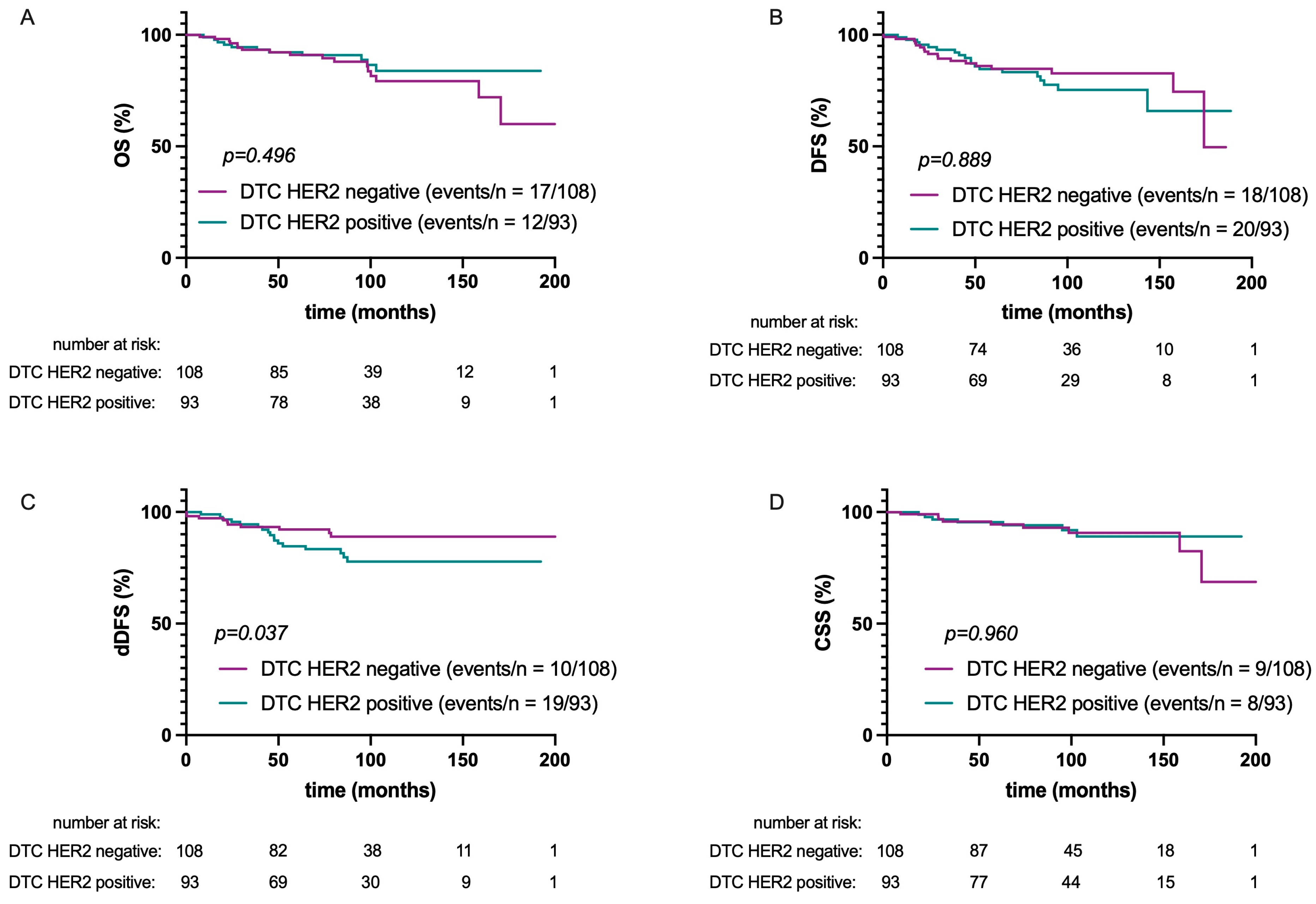
2.4. Survival Analysis
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Detection and Characterization of DTC
4.3. Evaluation of the HER2 Status of the PT
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Chan, P.S.; Lok, V.; Chen, X.; Ding, H.; Jin, Y.; Yuan, J.; Lao, X.Q.; Zheng, Z.J.; Wong, M.C. Global incidence and mortality of breast cancer: A trend analysis. Aging 2021, 13, 5748–5803. [Google Scholar] [CrossRef] [PubMed]
- Ponde, N.F.; Zardavas, D.; Piccart, M. Progress in adjuvant systemic therapy for breast cancer. Nat. Rev. Clin. Oncol. 2019, 16, 27–44. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Bertaglia, V.; Parati, M.C.; Borgonovo, K.; De Silva, P.; Luciani, A.; Novello, S.; Scartozzi, M.; Emens, L.A.; Solinas, C. Adjuvant chemotherapy for resected triple negative breast cancer patients: A network meta-analysis. Breast 2023, 67, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhang, X.; Chen, Y.; Li, P.; Zhang, J.; Xu, A.; Huang, N.; Liang, M.; Chen, Y.; Wang, K. Survival differences between HER2-0 and HER2-low-expressing breast cancer—A meta-analysis of early breast cancer patients. Crit. Rev. Oncol. Hematol. 2023, 185, 103962. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, H.; Obradovic, M.M.S.; Hoffmann, M.; Harper, K.L.; Sosa, M.S.; Werner-Klein, M.; Nanduri, L.K.; Werno, C.; Ehrl, C.; Maneck, M.; et al. Early dissemination seeds metastasis in breast cancer. Nature 2016, 540, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Hartkopf, A.D.; Brucker, S.Y.; Taran, F.A.; Harbeck, N.; von Au, A.; Naume, B.; Pierga, J.Y.; Hoffmann, O.; Beckmann, M.W.; Ryden, L.; et al. Disseminated tumour cells from the bone marrow of early breast cancer patients: Results from an international pooled analysis. Eur. J. Cancer 2021, 154, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Vogl, F.D.; Naume, B.; Janni, W.; Osborne, M.P.; Coombes, R.C.; Schlimok, G.; Diel, I.J.; Gerber, B.; Gebauer, G.; et al. A pooled analysis of bone marrow micrometastasis in breast cancer. N. Engl. J. Med. 2005, 353, 793–802. [Google Scholar] [CrossRef]
- Volmer, L.; Koch, A.; Matovina, S.; Dannehl, D.; Weiss, M.; Welker, G.; Hahn, M.; Engler, T.; Wallwiener, M.; Walter, C.B.; et al. Neoadjuvant Chemotherapy of Patients with Early Breast Cancer Is Associated with Increased Detection of Disseminated Tumor Cells in the Bone Marrow. Cancers 2022, 14, 635. [Google Scholar] [CrossRef]
- Hartkopf, A.D.; Taran, F.A.; Wallwiener, M.; Hahn, M.; Becker, S.; Solomayer, E.F.; Brucker, S.Y.; Fehm, T.N.; Wallwiener, D. Prognostic relevance of disseminated tumour cells from the bone marrow of early stage breast cancer patients—Results from a large single-centre analysis. Eur. J. Cancer 2014, 50, 2550–2559. [Google Scholar] [CrossRef]
- Rosin, J.; Svegrup, E.; Valachis, A.; Zerdes, I. Discordance of PIK3CA mutational status between primary and metastatic breast cancer: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2023, 201, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Nikas, I.P.; Lim, S.; Im, S.A.; Lee, K.H.; Lee, D.W.; Lee, H.; Ryu, H.S. Discrepancies in Hormone Receptor and HER2 Expression between Malignant Serous Effusions and Paired Tissues from Primary or Recurrent Breast Cancers. Pathobiology 2023. [Google Scholar] [CrossRef]
- Moreira-Dinzey, J.; Zhan, H.; Rozenblit, M.; Krishnamurti, U.; Harigopal, M.; Zhong, M.; Liang, Y. The correlation of ESR1 genetic aberrations with estrogen receptor and progesterone receptor status in metastatic and primary estrogen receptor-positive breast carcinomas. Hum. Pathol. 2023, 137, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Li, M.; Lv, H.; Zhou, S.; Xu, X.; Shui, R.; Yang, W. HER2-low breast cancer: Evolution of HER2 expression from primary tumor to distant metastases. BMC Cancer 2023, 23, 656. [Google Scholar] [CrossRef]
- Almstedt, K.; Krauthauser, L.; Kappenberg, F.; Wagner, D.C.; Heimes, A.S.; Battista, M.J.; Anic, K.; Krajnak, S.; Lebrecht, A.; Schwab, R.; et al. Discordance of HER2-Low between Primary Tumors and Matched Distant Metastases in Breast Cancer. Cancers 2023, 15, 1413. [Google Scholar] [CrossRef] [PubMed]
- Yeo, S.K.; Guan, J.L. Breast Cancer: Multiple Subtypes within a Tumor? Trends Cancer 2017, 3, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L.L.; Polyak, K. Breast tumor heterogeneity: Cancer stem cells or clonal evolution? Cell Cycle 2007, 6, 2332–2338. [Google Scholar] [CrossRef] [PubMed]
- Venizelos, A.; Engebrethsen, C.; Deng, W.; Geisler, J.; Geisler, S.; Iversen, G.T.; Aas, T.; Aase, H.S.; Seyedzadeh, M.; Steinskog, E.S.; et al. Clonal evolution in primary breast cancers under sequential epirubicin and docetaxel monotherapy. Genome Med. 2022, 14, 86. [Google Scholar] [CrossRef]
- Hartkopf, A.D.; Banys, M.; Meier-Stiegen, F.; Hahn, M.; Rohm, C.; Hoffmann, J.; Helms, G.; Taran, F.A.; Wallwiener, M.; Walter, C.; et al. The HER2 status of disseminated tumor cells in the bone marrow of early breast cancer patients is independent from primary tumor and predicts higher risk of relapse. Breast Cancer Res. Treat. 2013, 138, 509–517. [Google Scholar] [CrossRef]
- Mai, N.; Abuhadra, N.; Jhaveri, K. Molecularly Targeted Therapies for Triple Negative Breast Cancer: History, Advances, and Future Directions. Clin. Breast Cancer 2023, 23, 784–799. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B.; et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N. Engl. J. Med. 2021, 384, 1529–1541. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Nicolo, E.; Tarantino, P.; Curigliano, G. Biology and Treatment of HER2-Low Breast Cancer. Hematol. Oncol. Clin. N. Am. 2023, 37, 117–132. [Google Scholar] [CrossRef]
- Krawczyk, N.; Banys, M.; Neubauer, H.; Solomayer, E.F.; Gall, C.; Hahn, M.; Becker, S.; Bachmann, R.; Wallwiener, D.; Fehm, T. HER2 status on persistent disseminated tumor cells after adjuvant therapy may differ from initial HER2 status on primary tumor. Anticancer Res. 2009, 29, 4019–4024. [Google Scholar] [PubMed]
- Becker, S.; Becker-Pergola, G.; Fehm, T.; Wallwiener, D.; Solomayer, E.F. Her2 expression on disseminated tumor cells from bone marrow of breast cancer patients. Anticancer Res. 2005, 25, 2171–2175. [Google Scholar] [PubMed]
- Solomayer, E.F.; Becker, S.; Pergola-Becker, G.; Bachmann, R.; Kramer, B.; Vogel, U.; Neubauer, H.; Wallwiener, D.; Huober, J.; Fehm, T.N. Comparison of HER2 status between primary tumor and disseminated tumor cells in primary breast cancer patients. Breast Cancer Res. Treat. 2006, 98, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, M.; Porta, F.M.; D’Ercole, M.; Pescia, C.; Sajjadi, E.; Cursano, G.; De Camilli, E.; Pala, O.; Mazzarol, G.; Venetis, K.; et al. Standardized pathology report for HER2 testing in compliance with 2023 ASCO/CAP updates and 2023 ESMO consensus statements on HER2-low breast cancer. Virchows. Arch. 2024, 484, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Hartkopf, A.D.; Wallwiener, M.; Kommoss, S.; Taran, F.A.; Brucker, S.Y. Detection of disseminated tumor cells from the bone marrow of patients with early breast cancer is associated with high 21-gene recurrence score. Breast Cancer Res. Treat. 2016, 156, 91–95. [Google Scholar] [CrossRef]
- Braun, S.; Schlimok, G.; Heumos, I.; Schaller, G.; Riethdorf, L.; Riethmuller, G.; Pantel, K. ErbB2 overexpression on occult metastatic cells in bone marrow predicts poor clinical outcome of stage I-III breast cancer patients. Cancer Res. 2001, 61, 1890–1895. [Google Scholar]
- Pestrin, M.; Bessi, S.; Galardi, F.; Truglia, M.; Biggeri, A.; Biagioni, C.; Cappadona, S.; Biganzoli, L.; Giannini, A.; Di Leo, A. Correlation of HER2 status between primary tumors and corresponding circulating tumor cells in advanced breast cancer patients. Breast Cancer Res. Treat. 2009, 118, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Mu, Z.; Ye, Z.; Zhang, Z.; Abu-Khalaf, M.M.; Silver, D.P.; Palazzo, J.P.; Jagannathan, G.; Fellin, F.M.; Bhattacharya, S.; et al. Prognostic value of HER2 status on circulating tumor cells in advanced-stage breast cancer patients with HER2-negative tumors. Breast Cancer Res. Treat. 2020, 181, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Munzone, E.; Nole, F.; Goldhirsch, A.; Botteri, E.; Esposito, A.; Zorzino, L.; Curigliano, G.; Minchella, I.; Adamoli, L.; Cassatella, M.C.; et al. Changes of HER2 status in circulating tumor cells compared with the primary tumor during treatment for advanced breast cancer. Clin. Breast Cancer 2010, 10, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Roetger, A.; Merschjann, A.; Dittmar, T.; Jackisch, C.; Barnekow, A.; Brandt, B. Selection of potentially metastatic subpopulations expressing c-erbB-2 from breast cancer tissue by use of an extravasation model. Am. J. Pathol. 1998, 153, 1797–1806. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.; Fong, C.; Luthra, A.; Smith, S.A.; DiNatale, R.G.; Nandakumar, S.; Walch, H.; Chatila, W.K.; Madupuri, R.; Kundra, R.; et al. Genomic characterization of metastatic patterns from prospective clinical sequencing of 25,000 patients. Cell 2022, 185, 563–575.e511. [Google Scholar] [CrossRef]
- Harper, K.L.; Sosa, M.S.; Entenberg, D.; Hosseini, H.; Cheung, J.F.; Nobre, R.; Avivar-Valderas, A.; Nagi, C.; Girnius, N.; Davis, R.J.; et al. Mechanism of early dissemination and metastasis in Her2(+) mammary cancer. Nature 2016, 540, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, D.; Uenosono, Y.; Arigami, T.; Yanagita, S.; Okubo, K.; Kijima, T.; Miyazono, F.; Hamanoue, M.; Hokita, S.; Nakashima, S.; et al. Clinical significance of circulating tumor cells in the response to trastuzumab for HER2-negative metastatic gastric cancer. Cancer Chemother. Pharmacol. 2021, 87, 789–797. [Google Scholar] [CrossRef]
- Jacot, W.; Cottu, P.; Berger, F.; Dubot, C.; Venat-Bouvet, L.; Lortholary, A.; Bourgeois, H.; Bollet, M.; Servent, V.; Luporsi, E.; et al. Actionability of HER2-amplified circulating tumor cells in HER2-negative metastatic breast cancer: The CirCe T-DM1 trial. Breast Cancer Res. 2019, 21, 121. [Google Scholar] [CrossRef] [PubMed]
- Parsons, H.A.; Macrae, E.R.; Guo, H.; Li, T.; Barry, W.T.; Tayob, N.; Wulf, G.M.; Isakoff, S.J.; Krop, I.E. Phase II Single-Arm Study to Assess Trastuzumab and Vinorelbine in Advanced Breast Cancer Patients With HER2-Negative Tumors and HER2-Positive Circulating Tumor Cells. JCO Precis. Oncol. 2021, 5, 896–903. [Google Scholar] [CrossRef]
- Lewis, G.D.; Li, G.; Guo, J.; Yu, S.F.; Fields, C.T.; Lee, G.; Zhang, D.; Dragovich, P.S.; Pillow, T.; Wei, B.; et al. The HER2-directed antibody-drug conjugate DHES0815A in advanced and/or metastatic breast cancer: Preclinical characterization and phase 1 trial results. Nat. Commun. 2024, 15, 466. [Google Scholar] [CrossRef]
- Trastuzumab Deruxtecan (T-DXd) Alone or in Sequence with THP, Versus Standard Treatment (ddAC-THP), in HER2-Positive Early Breast Cancer. NCT05113251. Available online: https://clinicaltrials.gov/study/NCT05113251 (accessed on 28 March 2024).
- Thill, M.; Kolberg-Liedtke, C.; Albert, U.S.; Banys-Paluchowski, M.; Bauerfeind, I.; Blohmer, J.U.; Budach, W.; Dall, P.; Ditsch, N.; Fallenberg, E.M.; et al. AGO Recommendations for the Diagnosis and Treatment of Patients with Locally Advanced and Metastatic Breast Cancer: Update 2023. Breast Care 2023, 18, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften. Interdisziplinäre S3-Leitlinie für die Früherkennung, Diagnostik, Therapie und Nachsorge des Mammakarzinoms. Langversion 4.4—Juni 2021. 2021. Available online: https://register.awmf.org/assets/guidelines/032-045OLl_S3_Mammakarzinom_2021-07.pdf (accessed on 28 March 2024).
- Curigliano, G.; Burstein, H.J.; Gnant, M.; Loibl, S.; Cameron, D.; Regan, M.M.; Denkert, C.; Poortmans, P.; Weber, W.P.; Thurlimann, B.; et al. Understanding breast cancer complexity to improve patient outcomes: The St Gallen International Consensus Conference for the Primary Therapy of Individuals with Early Breast Cancer 2023. Ann. Oncol. 2023, 34, 970–986. [Google Scholar] [CrossRef] [PubMed]
- Fehm, T.; Braun, S.; Muller, V.; Janni, W.; Gebauer, G.; Marth, C.; Schindlbeck, C.; Wallwiener, D.; Borgen, E.; Naume, B.; et al. A concept for the standardized detection of disseminated tumor cells in bone marrow from patients with primary breast cancer and its clinical implementation. Cancer 2006, 107, 885–892. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| All Patients n | DTC HER2-Positive n (%) | p-Value * | |
|---|---|---|---|
| 201 | 93 (46.2) | ||
| Mean age at diagnosis (years) | 59.9 | 60.0 | 0.891 |
| Menopausal status | 0.544 | ||
| premenopausal | 64 | 32 (50.0) | |
| postmenopausal | 137 | 61 (44.5) | |
| Histological type | |||
| NST | 144 | 70 (49.6) | 0.058 |
| ILC | 39 | 12 (30.8) | |
| other | 18 | 11 (61.1) | |
| pT | 0.948 | ||
| T1 | 121 | 56 (46.3) | |
| T2–4 | 80 | 37 (46.3) | |
| pN | |||
| N0 | 128 | 59 (46.1) | 1.000 |
| N+ | 73 | 34 (46.6) | |
| ER status | |||
| positive | 166 | 75 (45.2) | 0.706 |
| negative | 34 | 17 (50.0) | |
| Grading | |||
| G1 | 24 | 11 (45.8) | 0.968 |
| G2–3 | 175 | 81 (46.3) |
| Patients HER2 Classification | Total n | DTC HER2-Positive n (%) | DTC HER2-Negative n (%) | p-Value * |
|---|---|---|---|---|
| HER2 “classical” | 0.214 | |||
| Negative | 173 | 77 (44.5) | 96 (55.5) | |
| Positive | 28 | 16 (57.1) | 12 (42.9) | |
| HER2 “modern” | ||||
| Negative | 69 | 22 (31.9) | 47 (68.1) | 0.012 |
| Low | 103 | 54 (52.4) | 49 (47.6) | |
| High | 28 | 16 (57.1) | 12 (42.9) |
| Parameter | dDFS | DFS | OS | CSS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | Univariate | Multivariate | Univariate | Multivariate | |||||||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Estrogen receptor status | ||||||||||||||||
| neg. vs. pos | 3.8 (1.8–8.2) | 0.001 | 15.7 (5.6–44.1) | <0.001 | 3.4 (1.7–6.7) | <0.001 | 3.8 (1.9–7.5) | <0.001 | 1.8 (0.8–4.1) | 0.034 | 2.6 (1.1–6.3) | 0.036 | 3.5 (1.3–9.3) | 0.015 | 19.4 (4.9–77.2) | <0.001 |
| Nodal status | ||||||||||||||||
| pos. vs. neg. | 4.5 (2.0–10.2) | <0.001 | 9.8 (3.3–28.9) | <0.001 | 3.3 (1.7–6.4) | <0.001 | 3.0 (1.4–6.1) | 0.003 | 3.0 (1.4–6.4) | 0.004 | 4.5 (1.9–10.5) | <0.001 | 4.9 (1.7–14.3) | 0.003 | 17.2 (3.7–79.4) | <0.001 |
| HER2 status PT | ||||||||||||||||
| pos. vs. neg. | 2.7 (0.6–11.4) | 0.032 | 12.9 (2.4–48.7) | 0.003 | 1.1 (0.4–2.8) | 0.087 | 0.191 | 1.3 (0.4–3.8) | 0.061 | 0.111 | 3.6 (0.5–28.4) | 0.097 | 34.9 (3.1–397.6) | 0.004 | ||
| HER2 status DTCs | ||||||||||||||||
| pos. vs. neg. | 2.3 (1.1–5.2) | 0.037 | 2.6 (1.2–5.9) | 0.021 | 1.2 (0.6–2.2) | 0.064 | 0.837 | 1.3 (0.6–2.7) | 0.094 | 0.346 | 1.0 (0.4–2.7) | 0.096 | 0.934 | |||
| Tumor size | ||||||||||||||||
| T1 vs. T2–4 | 4.0 (1.8–8.8) | <0.001 | 0.062 | 3.3 (1.7–6.5) | <0.001 | 0.5 (0.22–0.98) | 0.04 | 2.3 (1.1–4.9) | 0.022 | 0.114 | 2.7 (1.0–7.1) | 0.047 | 0.613 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volmer, L.L.; Dannehl, D.; Matovina, S.; Taran, F.-A.; Walter, C.B.; Wallwiener, M.; Brucker, S.Y.; Hartkopf, A.D.; Engler, T. Comparing the HER2 Status of the Primary Tumor to That of Disseminated Tumor Cells in Early Breast Cancer. Int. J. Mol. Sci. 2024, 25, 5910. https://doi.org/10.3390/ijms25115910
Volmer LL, Dannehl D, Matovina S, Taran F-A, Walter CB, Wallwiener M, Brucker SY, Hartkopf AD, Engler T. Comparing the HER2 Status of the Primary Tumor to That of Disseminated Tumor Cells in Early Breast Cancer. International Journal of Molecular Sciences. 2024; 25(11):5910. https://doi.org/10.3390/ijms25115910
Chicago/Turabian StyleVolmer, Léa Louise, Dominik Dannehl, Sabine Matovina, Florin-Andrei Taran, Christina Barbara Walter, Markus Wallwiener, Sara Yvonne Brucker, Andreas Daniel Hartkopf, and Tobias Engler. 2024. "Comparing the HER2 Status of the Primary Tumor to That of Disseminated Tumor Cells in Early Breast Cancer" International Journal of Molecular Sciences 25, no. 11: 5910. https://doi.org/10.3390/ijms25115910
APA StyleVolmer, L. L., Dannehl, D., Matovina, S., Taran, F.-A., Walter, C. B., Wallwiener, M., Brucker, S. Y., Hartkopf, A. D., & Engler, T. (2024). Comparing the HER2 Status of the Primary Tumor to That of Disseminated Tumor Cells in Early Breast Cancer. International Journal of Molecular Sciences, 25(11), 5910. https://doi.org/10.3390/ijms25115910