
A Plasma Pyrophosphate Cutoff Value for Diagnosing Pseudoxanthoma Elasticum

 , , , and
, , , and
Abstract
1. Introduction
2. Results
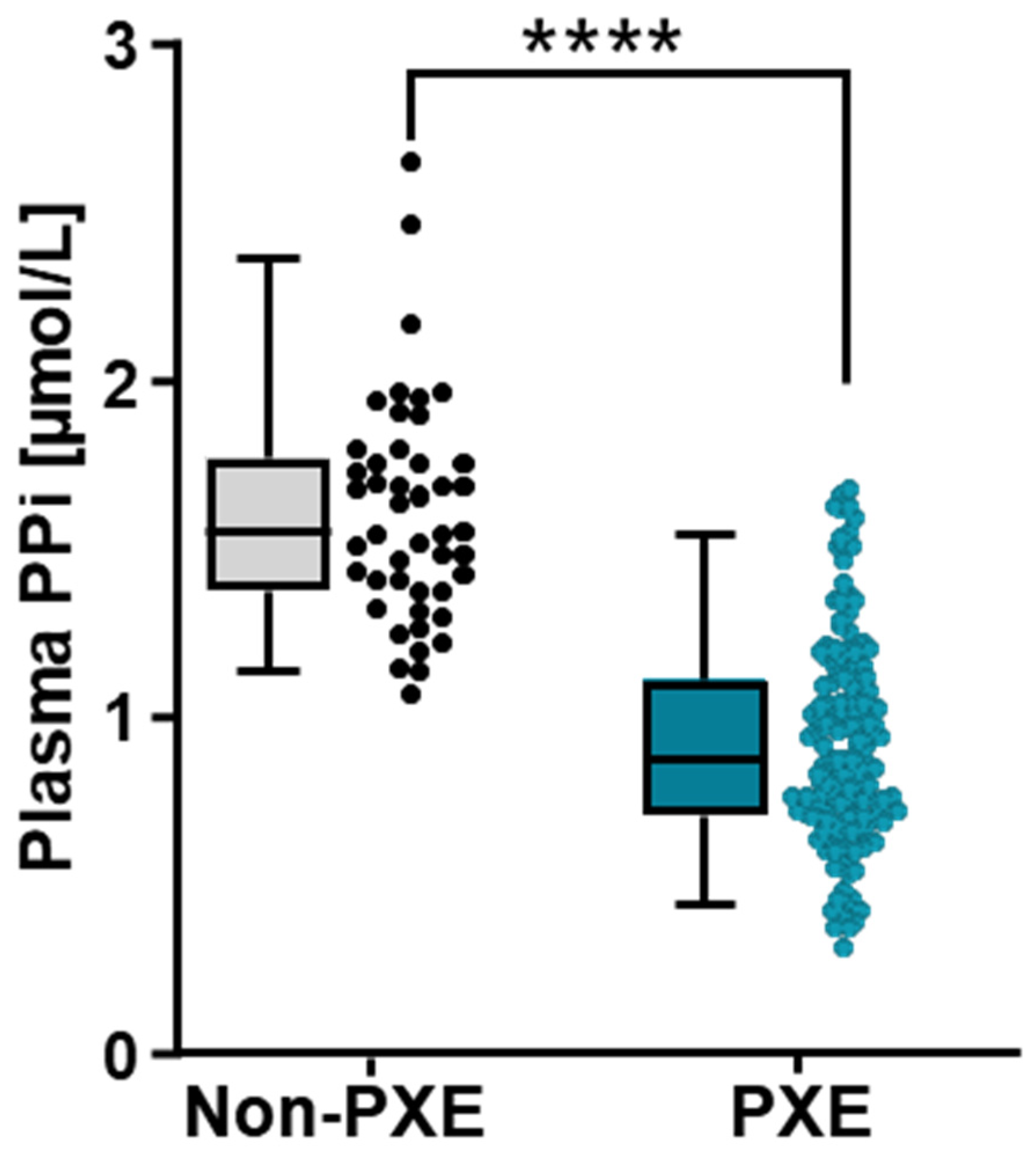
2.1. A Significant Decrease of Plasma PPi Concentration in a PXE Cohort
2.2. Determination of a PPi Cutoff Value for PXE Diagnosis



{kind=link}
{kind=link}
{kind=link}
| Threshold | Overall Patients | Patients Aged under 50 Years (<50 y.o.) | ||||||
|---|---|---|---|---|---|---|---|---|
| Train (n = 148) | Test (n = 51) | Train (n = 78) | Test (n = 27) | |||||
| Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | |
| <1.70 | 100.0 | 44.1 | 100.0 | 33.3 | 100.0 | 33.3 | 100.0 | 37.5 |
| <1.20 | 83.3 | 91.1 | 92.3 | 91.7 | 92.6 | 95.8 | 100.0 | 100.0 |
| <1.10 | 69.3 | 100.0 | 79.5 | 100.0 | 85.2 | 100.0 | 89.5 | 100.0 |
2.3. Influence of Sex on the PPi Cutoff for PXE Diagnosis
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Preanalytical Preparation of Blood Samples
4.3. Plasma PPi Concentration Measurement
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Le Saux, O.; Urban, Z.; Tschuch, C.; Csiszar, K.; Bacchelli, B.; Quaglino, D.; Pasquali-Ronchetti, I.; Pope, F.M.; Richards, A.; Terry, S.; et al. Mutations in a Gene Encoding an ABC Transporter Cause Pseudoxanthoma Elasticum. Nat. Genet. 2000, 25, 223–227. [Google Scholar] [CrossRef]
- Germain, D.P. Pseudoxanthoma Elasticum. Orphanet J. Rare Dis. 2017, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.; Neldner, K.; Pope, F.M.; De Paepe, A.; Christiano, A.M.; Boyd, C.D.; Uitto, J.; McKusick, V.A. Classification of Pseudoxanthoma Elasticum: Report of a Consensus Conference. J. Am. Acad. Dermatol. 1994, 30, 103–107. [Google Scholar] [CrossRef]
- Uitto, J.; Jiang, Q.; Váradi, A.; Bercovitch, L.G.; Terry, S.F. Pseudoxanthoma Elasticum: Diagnostic features, classification, and treatment options. Expert Opin. Orphan Drugs 2014, 2, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Plomp, A.S.; Toonstra, J.; Bergen, A.A.; van Dijk, M.R.; de Jong, P.T. Proposal for Updating the Pseudoxanthoma Elasticum Classification System and a Review of the Clinical Findings. Am. J. Med. Genet. A 2010, 152A, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Vanakker, O.M.; Leroy, B.P.; Coucke, P.; Bercovitch, L.G.; Uitto, J.; Viljoen, D.; Terry, S.F.; Van Acker, P.; Matthys, D.; Loeys, B.; et al. Novel Clinico-Molecular Insights in Pseudoxanthoma Elasticum Provide an Efficient Molecular Screening Method and a Comprehensive Diagnostic Flowchart. Hum. Mutat. 2008, 29, 205. [Google Scholar] [CrossRef] [PubMed]
- Ralph, D.; Nitschke, Y.; Levine, M.A.; Caffet, M.; Wurst, T.; Saeidian, A.H.; Youssefian, L.; Vahidnezhad, H.; Terry, S.F.; Rutsch, F.; et al. ENPP1 Variants in Patients with GACI and PXE Expand the Clinical and Genetic Heterogeneity of Heritable Disorders of Ectopic Calcification. PLoS Genet. 2022, 18, e1010192. [Google Scholar] [CrossRef]
- Rutsch, F.; Ruf, N.; Vaingankar, S.; Toliat, M.R.; Suk, A.; Höhne, W.; Schauer, G.; Lehmann, M.; Roscioli, T.; Schnabel, D.; et al. Mutations in ENPP1 Are Associated with “idiopathic” Infantile Arterial Calcification. Nat. Genet. 2003, 34, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Vanakker, O.M.; Martin, L.; Gheduzzi, D.; Leroy, B.P.; Loeys, B.L.; Guerci, V.I.; Matthys, D.; Terry, S.F.; Coucke, P.J.; Pasquali-Ronchetti, I.; et al. Pseudoxanthoma Elasticum-like Phenotype with Cutis Laxa and Multiple Coagulation Factor Deficiency Represents a Separate Genetic Entity. J. Investig. Dermatol. 2007, 127, 581–587. [Google Scholar] [CrossRef]
- Jansen, R.S.; Küçükosmanoglu, A.; de Haas, M.; Sapthu, S.; Otero, J.A.; Hegman, I.E.M.; Bergen, A.A.B.; Gorgels, T.G.M.F.; Borst, P.; van de Wetering, K. ABCC6 Prevents Ectopic Mineralization Seen in Pseudoxanthoma Elasticum by Inducing Cellular Nucleotide Release. Proc. Natl. Acad. Sci. USA 2013, 110, 20206–20211. [Google Scholar] [CrossRef] [PubMed]
- Pomozi, V.; Brampton, C.; van de Wetering, K.; Zoll, J.; Calio, B.; Pham, K.; Owens, J.B.; Marh, J.; Moisyadi, S.; Varadi, A.; et al. Pyrophosphate Supplementation Prevents Chronic and Acute Calcification in ABCC6-Deficient Mice. Am. J. Pathol. 2017, 187, 1258–1272. [Google Scholar] [CrossRef]
- Kauffenstein, G.; Yegutkin, G.G.; Khiati, S.; Pomozi, V.; Le Saux, O.; Leftheriotis, G.; Lenaers, G.; Henrion, D.; Martin, L. Alteration of Extracellular Nucleotide Metabolism in Pseudoxanthoma Elasticum. J. Investig. Dermatol. 2018, 138, 1862–1870. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.S.; Duijst, S.; Mahakena, S.; Sommer, D.; Szeri, F.; Varadi, A.; Plomp, A.; Bergen, A.A.; Oude Elferink, R.P.; Borst, P.; et al. ABCC6-Mediated ATP Secretion by the Liver Is the Main Source of the Mineralization Inhibitor Inorganic Pyrophosphate in the Systemic Circulation-Brief Report. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1985–1989. [Google Scholar] [CrossRef]
- Kozák, E.; Bartstra, J.W.; de Jong, P.A.; Mali, W.P.T.M.; Fülöp, K.; Tőkési, N.; Pomozi, V.; Risseeuw, S.; Norel, J.O.; van Leeuwen, R.; et al. Plasma Level of Pyrophosphate Is Low in Pseudoxanthoma Elasticum Owing to Mutations in the ABCC6 Gene, but It Does Not Correlate with ABCC6 Genotype. J. Clin. Med. 2023, 12, 1047. [Google Scholar] [CrossRef] [PubMed]
- Leftheriotis, G.; Navasiolava, N.; Clotaire, L.; Duranton, C.; Le Saux, O.; Bendahhou, S.; Laurain, A.; Rubera, I.; Martin, L. Relationships between Plasma Pyrophosphate, Vascular Calcification and Clinical Severity in Patients Affected by Pseudoxanthoma Elasticum. J. Clin. Med. 2022, 11, 2588. [Google Scholar] [CrossRef]
- Sánchez-Tévar, A.M.; García-Fernández, M.; Murcia-Casas, B.; Rioja-Villodres, J.; Carrillo, J.L.; Camacho, M.; Van Gils, M.; Sánchez-Chaparro, M.A.; Vanakker, O.; Valdivielso, P. Plasma Inorganic Pyrophosphate and Alkaline Phosphatase in Patients with Pseudoxanthoma Elasticum. Ann. Transl. Med. 2019, 7, 798. [Google Scholar] [CrossRef] [PubMed]
- Van Gils, M.; Depauw, J.; Coucke, P.J.; Aerts, S.; Verschuere, S.; Nollet, L.; Vanakker, O.M. Inorganic Pyrophosphate Plasma Levels Are Decreased in Pseudoxanthoma Elasticum Patients and Heterozygous Carriers but Do Not Correlate with the Genotype or Phenotype. J. Clin. Med. 2023, 12, 1893. [Google Scholar] [CrossRef] [PubMed]
- Bartstra, J.W.; Risseeuw, S.; de Jong, P.A.; van Os, B.; Kalsbeek, L.; Mol, C.; Baas, A.F.; Verschuere, S.; Vanakker, O.; Florijn, R.J.; et al. Genotype-Phenotype Correlation in Pseudoxanthoma Elasticum. Atherosclerosis 2021, 324, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Legrand, A.; Cornez, L.; Samkari, W.; Mazzella, J.-M.; Venisse, A.; Boccio, V.; Auribault, K.; Keren, B.; Benistan, K.; Germain, D.P.; et al. Mutation Spectrum in the ABCC6 Gene and Genotype-Phenotype Correlations in a French Cohort with Pseudoxanthoma Elasticum. Genet. Med. 2017, 19, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Centre Hospitalier Universitaire de Nice. Efficacy of PyROphosPHate Supplementation to Fight ECtopIc Calcification in PseudoXanthoma Elasticum—PROPHECI-PPI Study. 13 December 2022. Available online: https://classic.clinicaltrials.gov/ct2/show/NCT04868578 (accessed on 3 May 2021).
- R Core Team. R A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.scirp.org/(S(lz5mqp453ed%20snp55rrgjct55))/reference/referencespapers.aspx?referenceid=3456808 (accessed on 30 October 2023).
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An Open-Source Package for R and S+ to Analyze and Compare ROC Curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubera, I.; Clotaire, L.; Laurain, A.; Destere, A.; Martin, L.; Duranton, C.; Leftheriotis, G. A Plasma Pyrophosphate Cutoff Value for Diagnosing Pseudoxanthoma Elasticum. Int. J. Mol. Sci. 2024, 25, 6502. https://doi.org/10.3390/ijms25126502
Rubera I, Clotaire L, Laurain A, Destere A, Martin L, Duranton C, Leftheriotis G. A Plasma Pyrophosphate Cutoff Value for Diagnosing Pseudoxanthoma Elasticum. International Journal of Molecular Sciences. 2024; 25(12):6502. https://doi.org/10.3390/ijms25126502
Chicago/Turabian StyleRubera, Isabelle, Laetitia Clotaire, Audrey Laurain, Alexandre Destere, Ludovic Martin, Christophe Duranton, and Georges Leftheriotis. 2024. "A Plasma Pyrophosphate Cutoff Value for Diagnosing Pseudoxanthoma Elasticum" International Journal of Molecular Sciences 25, no. 12: 6502. https://doi.org/10.3390/ijms25126502
APA StyleRubera, I., Clotaire, L., Laurain, A., Destere, A., Martin, L., Duranton, C., & Leftheriotis, G. (2024). A Plasma Pyrophosphate Cutoff Value for Diagnosing Pseudoxanthoma Elasticum. International Journal of Molecular Sciences, 25(12), 6502. https://doi.org/10.3390/ijms25126502