
Updates on C3 Glomerulopathy in Kidney Transplantation: Pathogenesis and Treatment Options

Abstract
:1. Introduction
2. C3 Glomerulopathy: Pathogenesis and Clinical Features
3. C3 Glomerulopathy and Infections
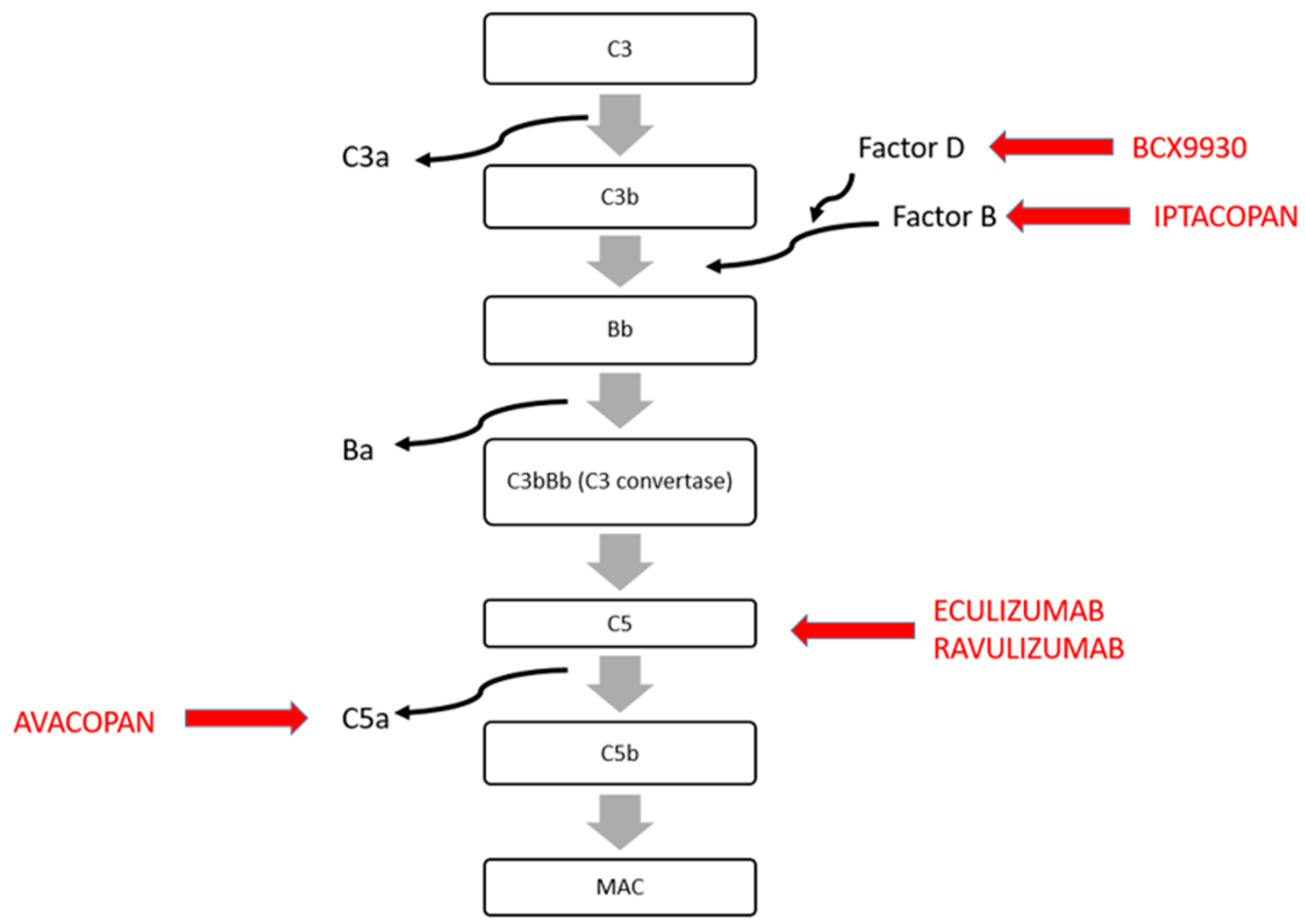
4. Treatment of C3 Glomerulopathy Recurrence

{kind=link}
{kind=link}
| Treatment | Target | Mechanism of Action | Os/Ev | Status | References |
|---|---|---|---|---|---|
| Eculizumab | Anti-C5 monoclonal antibody | Block the formation of MAC | Ev (every 2 weeks) | Approved for PNH, aHUS | Regunathan-Shenk R. et al., 2019 [19] Gurkan et al., 2013 [47] Gonzalez Suarez et al., 2020 [48] Kaartinen et al., 2018 [56] Hillmen et al., 2020 [49] Fakhouri et al., 2020 [50] Naseer et al., 2022 [57] |
| Ravalizumab | Anti-C5 humanized monoclonal antibody | Block the formation of MAC | Ev (every 8 weeks) | Approved for aHUS/Ongoing IgAN, LN | ALXN1210-aHUS-311 60–63 |
| Avacopan (CCX168) | C5a inhibitor | Block the binding of C5a-C5Ar1 | Os | Approved for ANCA-associated vasculitis/Ongoing for GPA, MPA | ACCOLADE trial Zotta et al., 2023 [52] |
| Iptacopan | Selective Factor B inhibitor | Block the formation of C3 convertase | Os | Approved for PNH/Ongoing for complement disease | APPEAR-C3G |
| BCX9930 | Factor D inhibitor | Block the formation of C3 convertase | Os | Ongoing for C3GN, IgAN, MN | NCT05162066 |
5. C3 Glomerulopathy and Monoclonal Gammopathy: Description and Treatment
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaballo, M.A.; Canney, M.; O’Kelly, P.; Williams, Y.; O’Seaghdha, C.M.; Conlon, P.J. A comparative analysis of survival of patients on dialysis and after kidney transplantation. Clin. Kidney J. 2018, 11, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic review: Kidney transplantation compared with dialysis in clinically relevant outcomes. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2011, 11, 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Ison, M.G.; Danziger-Isakov, L. Long-Term Infectious Complications of Kidney Transplantation. Clin. J. Am. Soc. Nephrol. 2022, 17, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Sellarés, J.; De Freitas, D.G.; Mengel, M.; Reeve, J.; Einecke, G.; Sis, B.; Hidalgo, L.G.; Famulski, K.; Matas, A.; Halloran, P.F. Understanding the Causes of Kidney Transplant Failure: The Dominant Role of Antibody-Mediated Rejection and Nonadherence. Am. J. Transplant. 2012, 12, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.; Astor, B.C.; Zhong, W.; Mandelbrot, D.A.; Maursetter, L.; Panzer, S.E. The association of acute rejection vs recurrent glomerular disease with graft outcomes after kidney transplantation. Clin. Transplant. 2019, 33, e13738. [Google Scholar] [CrossRef] [PubMed]
- Cosio, F.G.; El Ters, M.; Cornell, L.D.; Schinstock, C.A.; Stegall, M.D. Changing Kidney Allograft Histology Early Posttransplant: Prognostic Implications of 1-Year Protocol Biopsies. Am. J. Transplant. 2016, 16, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Cosio, F.G.; Cattran, D.C. Recent advances in our understanding of recurrent primary glomerulonephritis after kidney transplantation. Kidney Int. 2017, 91, 304–314. [Google Scholar] [CrossRef]
- Zanoni, F.; Khairallah, P.; Kiryluk, K.; Batal, I. Glomerular Diseases of the Kidney Allograft: Toward a Precision Medicine Approach. Semin. Nephrol. 2022, 42, 29–43. [Google Scholar] [CrossRef]
- Allen, P.J.; Chadban, S.J.; Craig, J.C.; Lim, W.H.; Allen, R.D.M.; Clayton, P.A.; Teixeira-Pinto, A.; Wong, G. Recurrent glomerulonephritis after kidney transplantation: Risk factors and allograft outcomes. Kidney Int. 2017, 92, 461–469. [Google Scholar] [CrossRef]
- Uffing, A.; Hullekes, F.; Riella, L.V.; Hogan, J.J. Recurrent Glomerular Disease after Kidney Transplantation: Diagnostic and Management Dilemmas. Clin. J. Am. Soc. Nephrol. 2021, 16, 1730–1742. [Google Scholar] [CrossRef]
- Ponticelli, C.; Glassock, R.J. Posttransplant recurrence of primary glomerulonephritis. Clin. J. Am. Soc. Nephrol. CJASN 2010, 5, 2363–2372. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.H.; Shingde, M.; Wong, G. Recurrent and de novo Glomerulonephritis After Kidney Transplantation. Front. Immunol. 2019, 10, 1944. [Google Scholar] [CrossRef] [PubMed]
- Morozumi, K.; Takeda, A.; Otsuka, Y.; Horike, K.; Gotoh, N.; Watarai, Y. Recurrent glomerular disease after kidney transplantation: An update of selected areas and the impact of protocol biopsy. Nephrol. Carlton Vic. 2014, 19 (Suppl. S3), 6–10. [Google Scholar] [CrossRef] [PubMed]
- Infante, B.; Rossini, M.; Leo, S.; Troise, D.; Netti, G.S.; Ranieri, E.; Gesualdo, L.; Castellano, G.; Stallone, G. Recurrent Glomerulonephritis after Renal Transplantation: The Clinical Problem. Int. J. Mol. Sci. 2020, 21, 5954. [Google Scholar] [CrossRef] [PubMed]
- Pickering, M.C.; D’Agati, V.D.; Nester, C.M.; Smith, R.J.; Haas, M.; Appel, G.B.; Alpers, C.E.; Bajema, I.M.; Bedrosian, C.; Braun, M.; et al. C3 glomerulopathy: Consensus report. Kidney Int. 2013, 84, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Caravaca-Fontán, F.; Lucientes, L.; Cavero, T.; Praga, M. Update on C3 Glomerulopathy: A Complement-Mediated Disease. Nephron 2020, 144, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Eddy, A.; Sibley, R.; Mauer, S.M.; Kim, Y. Renal allograft failure due to recurrent dense intramembranous deposit disease. Clin. Nephrol 1984, 21, 305–313. [Google Scholar] [PubMed]
- Salvadori, M.; Bertoni, E. Complement related kidney diseases: Recurrence after transplantation. World J. Transplant. 2016, 6, 632–645. [Google Scholar] [CrossRef] [PubMed]
- Regunathan-Shenk, R.; Avasare, R.S.; Ahn, W.; Canetta, P.A.; Cohen, D.J.; Appel, G.B.; Bomback, A.S. Kidney Transplantation in C3 Glomerulopathy: A Case Series. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2019, 73, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Caravaca-Fontán, F.; Polanco, N.; Villacorta, B.; Buxeda, A.; Coca, A.; Ávila, A.; Martínez-Gallardo, R.; Galeano, C.; Valero, R.; Ramos, N.; et al. Recurrence of immune complex and complement-mediated membranoproliferative glomerulonephritis in kidney transplantation. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc—Eur. Ren. Assoc. 2023, 38, 222–235. [Google Scholar] [CrossRef]
- De Paula, L.C.; Mazzali, M.; De Sousa, M.V. Recurrent Membranoproliferative Glomerulonephritis After Kidney Transplantation: Risk Factors and Impact on Graft Survival. Ann. Transplant. 2023, 28, e940502-1. [Google Scholar] [CrossRef] [PubMed]
- Perea-Ortega, L.; León-Fradejas, M.; Alonso-Titos, J.; Cabello-Díaz, M.; Toledo-Rojas, R.; Sola-Moyano, E.; Martín-Reyes, G.; López-Jiménez, V.; Burgos-Rodríguez, D.; Hernández-Marrero, D. Likely Recurrence of C3 Glomerulonephritis in Kidney Transplantation: An Entity to Bear in Mind: Case Report. Transplant. Proc. 2015, 47, 2669–2671. [Google Scholar] [CrossRef] [PubMed]
- Frangou, E.; Varnavidou-Nicolaidou, A.; Petousis, P.; Soloukides, A.; Theophanous, E.; Savva, I.; Michael, N.; Toumasi, E.; Georgiou, D.; Stylianou, G.; et al. Clinical course and outcome after kidney transplantation in patients with C3 glomerulonephritis due to CFHR5 nephropathy. Nephrol. Dial. Transplant. 2019, 34, 1780–1788. [Google Scholar] [CrossRef] [PubMed]
- Garg, N.; Zhang, Y.; Nicholson-Weller, A.; Khankin, E.V.; Borsa, N.G.; Meyer, N.C.; McDermott, S.; Stillman, I.E.; Rennke, H.G.; Smith, R.J.; et al. C3 glomerulonephritis secondary to mutations in factors H and I: Rapid recurrence in deceased donor kidney transplant effectively treated with eculizumab. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc—Eur. Ren. Assoc. 2018, 33, 2260–2265. [Google Scholar] [CrossRef] [PubMed]
- Boyer, O.; Noël, L.-H.; Balzamo, E.; Guest, G.; Biebuyck, N.; Charbit, M.; Salomon, R.; Frémeaux-Bacchi, V.; Niaudet, P. Complement factor H deficiency and posttransplantation glomerulonephritis with isolated C3 deposits. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2008, 51, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Lomax-Browne, H.J.; Medjeral-Thomas, N.R.; Barbour, S.J.; Gisby, J.; Han, H.; Bomback, A.S.; Fervenza, F.C.; Cairns, T.H.; Szydlo, R.; Tan, S.-J.; et al. Association of Histologic Parameters with Outcome in C3 Glomerulopathy and Idiopathic Immunoglobulin-Associated Membranoproliferative Glomerulonephritis. Clin. J. Am. Soc. Nephrol. CJASN 2022, 17, 994–1007. [Google Scholar] [CrossRef] [PubMed]
- Caravaca-Fontán, F.; Praga, M. Prognostication for C3 Glomerulopathy and Idiopathic Immunoglobulin-Associated Membranoproliferative Glomerulonephritis. Clin. J. Am. Soc. Nephrol. CJASN 2022, 17, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2018, 18, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Aubert, O.; Higgins, S.; Bouatou, Y.; Yoo, D.; Raynaud, M.; Viglietti, D.; Rabant, M.; Hidalgo, L.; Glotz, D.; Legendre, C.; et al. Archetype Analysis Identifies Distinct Profiles in Renal Transplant Recipients with Transplant Glomerulopathy Associated with Allograft Survival. J. Am. Soc. Nephrol. JASN 2019, 30, 625–639. [Google Scholar] [CrossRef] [PubMed]
- Filippone, E.J.; McCue, P.A.; Farber, J.L. Transplant glomerulopathy. Mod. Pathol. Off. J. U S Can. Acad. Pathol. Inc. 2018, 31, 235–252. [Google Scholar] [CrossRef]
- Panzer, S.E.; Joachim, E.; Parajuli, S.; Zhong, W.; Astor, B.C.; Djamali, A. Glomerular C3 Deposition Is an Independent Risk Factor for Allograft Failure in Kidney Transplant Recipients With Transplant Glomerulopathy. Kidney Int. Rep. 2019, 4, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Duong, M.D.; Reidy, K.J. Acute Postinfectious Glomerulonephritis. Pediatr. Clin. North. Am. 2022, 69, 1051–1078. [Google Scholar] [CrossRef] [PubMed]
- Chauvet, S.; Berthaud, R.; Devriese, M.; Mignotet, M.; Vieira Martins, P.; Robe-Rybkine, T.; Miteva, M.A.; Gyulkhandanyan, A.; Ryckewaert, A.; Louillet, F.; et al. Anti-Factor B Antibodies and Acute Postinfectious GN in Children. J. Am. Soc. Nephrol. JASN 2020, 31, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Fervenza, F.C.; Zhang, Y.; Zand, L.; Meyer, N.C.; Borsa, N.; Nasr, S.H.; Smith, R.J.H. Atypical postinfectious glomerulonephritis is associated with abnormalities in the alternative pathway of complement. Kidney Int. 2013, 83, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Khalighi, M.A.; Wang, S.; Henriksen, K.J.; Bock, M.; Keswani, M.; Meehan, S.M.; Chang, A. Revisiting post-infectious glomerulonephritis in the emerging era of C3 glomerulopathy. Clin. Kidney J. 2016, 9, 397–402. [Google Scholar] [CrossRef]
- Andresdottir, M.B.; Assmann, K.J.; Hilbrands, L.B.; Wetzels, J.F. Type I membranoproliferative glomerulonephritis in a renal allograft: A recurrence induced by a cytomegalovirus infection? Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2000, 35, E6. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK Patients in Hospital with COVID-19 Using the ISARIC WHO Clinical Characterisation Protocol: Prospective Observational Cohort Study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L.; et al. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef]
- Ahmadian, E.; Hosseiniyan Khatibi, S.M.; Razi Soofiyani, S.; Abediazar, S.; Shoja, M.M.; Ardalan, M.; Zununi Vahed, S. COVID-19 and kidney injury: Pathophysiology and molecular mechanisms. Rev. Med. Virol. 2021, 31, e2176. [Google Scholar] [CrossRef] [PubMed]
- Pfister, F.; Vonbrunn, E.; Ries, T.; Jäck, H.-M.; Überla, K.; Lochnit, G.; Sheriff, A.; Herrmann, M.; Büttner-Herold, M.; Amann, K.; et al. Complement Activation in Kidneys of Patients With COVID-19. Front. Immunol. 2020, 11, 594849. [Google Scholar] [CrossRef]
- Wen, J.; Wang, W.; Xu, F.; Sun, J.; Chen, J.; Ni, X. C3 glomerulonephritis and thrombotic microangiopathy of renal allograft after pulmonary infection in a male with concomitant two complement factor I gene variations: A case report. BMC Nephrol. 2018, 19, 148. [Google Scholar] [CrossRef]
- Lim, J.-H.; Shin, S.-W.; Kim, M.-S.; Han, M.-H.; Kim, Y.-J.; Jung, H.-Y.; Choi, J.-Y.; Cho, J.-H.; Park, S.-H.; Kim, Y.-L.; et al. Recurrent C3 Glomerulonephritis along with BK-Virus-Associated Nephropathy after Kidney Transplantation: A Case Report. Med. Kaunas. Lith. 2023, 59, 1308. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.B.; Bomback, A.S. C3 Glomerulopathy: Pathogenesis and Treatment. Adv. Chronic Kidney Dis. 2020, 27, 104–110. [Google Scholar] [CrossRef]
- Caravaca-Fontán, F.; Díaz-Encarnación, M.M.; Lucientes, L.; Cavero, T.; Cabello, V.; Ariceta, G.; Quintana, L.F.; Marco, H.; Barros, X.; Ramos, N.; et al. Mycophenolate Mofetil in C3 Glomerulopathy and Pathogenic Drivers of the Disease. Clin. J. Am. Soc. Nephrol. 2020, 15, 1287–1298. [Google Scholar] [CrossRef]
- Gurkan, S.; Fyfe, B.; Weiss, L.; Xiao, X.; Zhang, Y.; Smith, R.J. Eculizumab and recurrent C3 glomerulonephritis. Pediatr. Nephrol. 2013, 28, 1975–1981. [Google Scholar] [CrossRef]
- Gonzalez Suarez, M.L.; Thongprayoon, C.; Hansrivijit, P.; Kovvuru, K.; Kanduri, S.R.; Aeddula, N.R.; Pivovarova, A.I.; Chewcharat, A.; Bathini, T.; Mao, M.A.; et al. Treatment of C3 Glomerulopathy in Adult Kidney Transplant Recipients: A Systematic Review. Med. Sci. Basel Switz. 2020, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Hillmen, P.; Young, N.S.; Schubert, J.; Brodsky, R.A.; Socié, G.; Muus, P.; Röth, A.; Szer, J.; Elebute, M.O.; Nakamura, R.; et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N. Engl. J. Med. 2006, 355, 1233–1243. [Google Scholar] [CrossRef]
- Fakhouri, F.; Zuber, J.; Frémeaux-Bacchi, V.; Loirat, C. Haemolytic uraemic syndrome. Lancet Lond. Engl. 2017, 390, 681–696. [Google Scholar] [CrossRef]
- Werion, A.; Rondeau, E. Application of C5 inhibitors in glomerular diseases in 2021. Kidney Res. Clin. Pract. 2022, 41, 412–421. [Google Scholar] [CrossRef]
- Zotta, F.; Diomedi-Camassei, F.; Gargiulo, A.; Cappoli, A.; Emma, F.; Vivarelli, M. Successful treatment with avacopan [CCX168] in a pediatric patient with C3 glomerulonephritis. Pediatr. Nephrol. 2023, 38, 4197–4201. [Google Scholar] [CrossRef]
- Bomback, A.S.; Kavanagh, D.; Vivarelli, M.; Meier, M.; Wang, Y.; Webb, N.J.A.; Trapani, A.J.; Smith, R.J.H. Alternative Complement Pathway Inhibition With Iptacopan for the Treatment of C3 Glomerulopathy-Study Design of the APPEAR-C3G Trial. Kidney Int. Rep. 2022, 7, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Barbour, S.; Gill, J.S. Advances in the understanding of complement mediated glomerular disease: Implications for recurrence in the transplant setting. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2015, 15, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, E.C.; Sethi, S.; Leung, N.; Dispenzieri, A.; Fervenza, F.C.; Cosio, F.G. Recurrent membranoproliferative glomerulonephritis after kidney transplantation. Kidney Int. 2010, 77, 721–728. [Google Scholar] [CrossRef]
- Kaartinen, K.; Martola, L.; Räisänen-Sokolowski, A.; Meri, S. Recurrent allograft C3 glomerulonephritis and unsuccessful eculizumab treatment. Clin. Immunol. Orlando Fla. 2018, 187, 104–106. [Google Scholar] [CrossRef]
- Naseer, M.S.; Singh, A.; Singh, N. Repository Corticotropin in Treating de novo C3 Glomerulonephritis after Transplantation. Glomerular Dis. 2022, 2, 100–105. [Google Scholar] [CrossRef]
- Lindskog, A.; Ebefors, K.; Johansson, M.E.; Stefánsson, B.; Granqvist, A.; Arnadottir, M.; Berg, A.-L.; Nyström, J.; Haraldsson, B. Melanocortin 1 receptor agonists reduce proteinuria. J. Am. Soc. Nephrol. JASN 2010, 21, 1290–1298. [Google Scholar] [CrossRef] [PubMed]
- Gong, R. The renaissance of corticotropin therapy in proteinuric nephropathies. Nat. Rev. Nephrol. 2011, 8, 122–128. [Google Scholar] [CrossRef]
- Rondeau, E.; Scully, M.; Ariceta, G.; Barbour, T.; Cataland, S.; Heyne, N.; Miyakawa, Y.; Ortiz, S.; Swenson, E.; Vallee, M.; et al. The long-acting C5 inhibitor, Ravulizumab, is effective and safe in adult patients with atypical hemolytic uremic syndrome naïve to complement inhibitor treatment. Kidney Int. 2020, 97, 1287–1296. [Google Scholar] [CrossRef]
- Menne, J. Is ravulizumab the new treatment of choice for atypical hemolytic uremic syndrome [aHUS]? Kidney Int. 2020, 97, 1106–1108. [Google Scholar] [CrossRef] [PubMed]
- Barbour, T.; Scully, M.; Ariceta, G.; Cataland, S.; Garlo, K.; Heyne, N.; Luque, Y.; Menne, J.; Miyakawa, Y.; Yoon, S.-S.; et al. Long-Term Efficacy and Safety of the Long-Acting Complement C5 Inhibitor Ravulizumab for the Treatment of Atypical Hemolytic Uremic Syndrome in Adults. Kidney Int. Rep. 2021, 6, 1603–1613. [Google Scholar] [CrossRef] [PubMed]
- Ariceta, G.; Dixon, B.P.; Kim, S.H.; Kapur, G.; Mauch, T.; Ortiz, S.; Vallee, M.; Denker, A.E.; Kang, H.G.; Greenbaum, L.A.; et al. The long-acting C5 inhibitor, ravulizumab, is effective and safe in pediatric patients with atypical hemolytic uremic syndrome naïve to complement inhibitor treatment. Kidney Int. 2021, 100, 225–237. [Google Scholar] [CrossRef]
- Pickering, M.C.; Cook, H.T.; Warren, J.; Bygrave, A.E.; Moss, J.; Walport, M.J.; Botto, M. Uncontrolled C3 activation causes membranoproliferative glomerulonephritis in mice deficient in complement factor, H. Nat. Genet. 2002, 31, 424–428. [Google Scholar] [CrossRef]
- Pickering, M.C.; Warren, J.; Rose, K.L.; Carlucci, F.; Wang, Y.; Walport, M.J.; Cook, H.T.; Botto, M. Prevention of C5 activation ameliorates spontaneous and experimental glomerulonephritis in factor H-deficient mice. Proc. Natl. Acad. Sci. USA 2006, 103, 9649–9654. [Google Scholar] [CrossRef]
- Nasr, S.H.; Markowitz, G.S.; Stokes, M.B.; Seshan, S.V.; Valderrama, E.; Appel, G.B.; Aucouturier, P.; D’Agati, V.D. Proliferative glomerulonephritis with monoclonal IgG deposits: A distinct entity mimicking immune-complex glomerulonephritis. Kidney Int. 2004, 65, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Leung, N.; Bridoux, F.; Hutchison, C.A.; Nasr, S.H.; Cockwell, P.; Fermand, J.-P.; Dispenzieri, A.; Song, K.W.; Kyle, R.A. Monoclonal gammopathy of renal significance: When MGUS is no longer undetermined or insignificant. Blood 2012, 120, 4292–4295. [Google Scholar] [CrossRef]
- Bridoux, F.; Leung, N.; Hutchison, C.A.; Touchard, G.; Sethi, S.; Fermand, J.-P.; Picken, M.M.; Herrera, G.A.; Kastritis, E.; Merlini, G.; et al. Diagnosis of monoclonal gammopathy of renal significance. Kidney Int. 2015, 87, 698–711. [Google Scholar] [CrossRef] [PubMed]
- Zand, L.; Kattah, A.; Fervenza, F.C.; Smith, R.J.H.; Nasr, S.H.; Zhang, Y.; Vrana, J.A.; Leung, N.; Cornell, L.D.; Sethi, S. C3 glomerulonephritis associated with monoclonal gammopathy: A case series. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2013, 62, 506–514. [Google Scholar] [CrossRef]
- Meri, S.; Koistinen, V.; Miettinen, A.; Törnroth, T.; Seppälä, I.J. Activation of the alternative pathway of complement by monoclonal lambda light chains in membranoproliferative glomerulonephritis. J. Exp. Med. 1992, 175, 939–950. [Google Scholar] [CrossRef]
- Chauvet, S.; Roumenina, L.T.; Aucouturier, P.; Marinozzi, M.-C.; Dragon-Durey, M.-A.; Karras, A.; Delmas, Y.; Le Quintrec, M.; Guerrot, D.; Jourde-Chiche, N.; et al. Both Monoclonal and Polyclonal Immunoglobulin Contingents Mediate Complement Activation in Monoclonal Gammopathy Associated-C3 Glomerulopathy. Front. Immunol. 2018, 9, 2260. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Rajkumar, S.V. Monoclonal gammopathy-associated proliferative glomerulonephritis. Mayo Clin. Proc. 2013, 88, 1284–1293. [Google Scholar] [CrossRef] [PubMed]
- Heybeli, C.; Alexander, M.P.; Bentall, A.J.; Amer, H.; Buadi, F.K.; Dean, P.G.; Dingli, D.; Dispenzieri, A.; El Ters, M.; Gertz, M.A.; et al. Kidney Transplantation in Patients With Monoclonal Gammopathy of Renal Significance [MGRS] -Associated Lesions: A Case Series. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2022, 79, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fuentes, M.C.; Caba-Molina, M.; Polo-Moyano, A.; Palomares-Bayo, M.; Galindo-Sacristan, P.; De Gracia-Guindo, C. A 78-Year-Old Man with Chronic Kidney Disease and Monoclonal Gammopathy Who Developed Post-Transplant C3 Glomerulopathy—Recurrence or De Novo? A Case Report and Literature Review. Am. J. Case Rep. 2023, 24, e939726. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, A.; Fervenza, F.C.; Smith, R.J.H.; Sethi, S. C3 glomerulopathy associated with monoclonal Ig is a distinct subtype. Kidney Int. 2018, 94, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, I.E.; Gallan, A.; Huston, H.K.; Raphael, K.L.; Miller, D.V.; Revelo, M.P.; Khalighi, M.A. C3 glomerulopathy in adults: A distinct patient subset showing frequent association with monoclonal gammopathy and poor renal outcome. Clin. Kidney J. 2016, 9, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Said, S.M.; Cosio, F.G.; Valeri, A.M.; Leung, N.; Sethi, S.; Salameh, H.; Cornell, L.D.; Fidler, M.E.; Alexander, M.P.; Fervenza, F.C.; et al. Proliferative glomerulonephritis with monoclonal immunoglobulin G deposits is associated with high rate of early recurrence in the allograft. Kidney Int. 2018, 94, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Albawardi, A.; Satoskar, A.; Von Visger, J.; Brodsky, S.; Nadasdy, G.; Nadasdy, T. Proliferative glomerulonephritis with monoclonal IgG deposits recurs or may develop de novo in kidney allografts. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2011, 58, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Unagami, K.; Okumi, M.; Kakuta, Y.; Horita, S.; Ishida, H.; Koike, J.; Honda, K.; Tanabe, K.; Nitta, K. A case of recurrent proliferative glomerulonephritis with monoclonal IgG deposits or de novo C3 glomerulonephritis after kidney transplantation. Nephrol. Carlton Vic. 2018, 23 (Suppl. S2), 76–80. [Google Scholar] [CrossRef]
- Serra, N.; Facundo, C.; Canal, C.; Arce, Y.; Ayasreh, N.; Vila, A.; Bardají, B.; Silva, I.; López, V.; Benito, S.; et al. Three cases of monoclonal gammopathy of renal significance after kidney transplantation. De novo C3 glomerulopathy. Nefrologia 2019, 39, 198–201. [Google Scholar] [CrossRef]
- Nasr, S.H.; Sethi, S.; Cornell, L.D.; Fidler, M.E.; Boelkins, M.; Fervenza, F.C.; Cosio, F.G.; D’Agati, V.D. Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft. Clin. J. Am. Soc. Nephrol. 2011, 6, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Chauvet, S.; Frémeaux-Bacchi, V.; Petitprez, F.; Karras, A.; Daniel, L.; Burtey, S.; Choukroun, G.; Delmas, Y.; Guerrot, D.; François, A.; et al. Treatment of B-cell disorder improves renal outcome of patients with monoclonal gammopathy-associated C3 glomerulopathy. Blood 2017, 129, 1437–1447. [Google Scholar] [CrossRef] [PubMed]
- Moog, P.; Jost, P.J.; Büttner-Herold, M. Eculizumab as salvage therapy for recurrent monoclonal gammopathy-induced C3 glomerulopathy in a kidney allograft. BMC Nephrol. 2018, 19, 106. [Google Scholar] [CrossRef] [PubMed]
- Guiard, E.; Karras, A.; Plaisier, E.; Duong Van Huyen, J.-P.; Fakhouri, F.; Rougier, J.-P.; Noel, L.-H.; Callard, P.; Delahousse, M.; Ronco, P. Patterns of noncryoglobulinemic glomerulonephritis with monoclonal Ig deposits: Correlation with IgG subclass and response to rituximab. Clin. J. Am. Soc. Nephrol. CJASN 2011, 6, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Rudnicki, M. Rituximab for Treatment of Membranoproliferative Glomerulonephritis and C3 Glomerulopathies. BioMed Res. Int. 2017, 2017, 2180508. [Google Scholar] [CrossRef] [PubMed]
- AlSahow, A.; Al-Muhaiteeb, A.; Nawar, H.; AlHelal, B.; AlYousef, A.; Abdallah, E.; AbuShall, A.; Elmekawi, S.; Meshal, B.; AlQallaf, A.; et al. Use of Rituximab as an Off-Label Medication in Glomerular Diseases: Clinical Perspective. Med. Princ. Pract. 2022, 31, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Voora, S.; Adey, D.B. Management of Kidney Transplant Recipients by General Nephrologists: Core Curriculum 2019. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2019, 73, 866–879. [Google Scholar] [CrossRef] [PubMed]
- Obata, S.; Vaz de Castro, P.A.S.; Riella, L.V.; Cravedi. Recurrent C3 glomerulopathy after kidney transplantation. P. Transplant. Rev. 2024, 38, 100839. [Google Scholar] [CrossRef] [PubMed]
- Ponticelli, C.; Calatroni, M.; Moroni, G. C3 glomerulopathies: Dense deposit disease and C3 glomerulonephritis. Front. Med. 2023, 10, 1289812. [Google Scholar] [CrossRef] [PubMed]
- Tarragon Estebanez, B.; Bomback, A.S. C3 Glomerulopathy: Novel Treatment Paradigms. Kidney Int. Rep. 2023, 9, 569–579. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartoli, G.; Dello Strologo, A.; Grandaliano, G.; Pesce, F. Updates on C3 Glomerulopathy in Kidney Transplantation: Pathogenesis and Treatment Options. Int. J. Mol. Sci. 2024, 25, 6508. https://doi.org/10.3390/ijms25126508
Bartoli G, Dello Strologo A, Grandaliano G, Pesce F. Updates on C3 Glomerulopathy in Kidney Transplantation: Pathogenesis and Treatment Options. International Journal of Molecular Sciences. 2024; 25(12):6508. https://doi.org/10.3390/ijms25126508
Chicago/Turabian StyleBartoli, Giulia, Andrea Dello Strologo, Giuseppe Grandaliano, and Francesco Pesce. 2024. "Updates on C3 Glomerulopathy in Kidney Transplantation: Pathogenesis and Treatment Options" International Journal of Molecular Sciences 25, no. 12: 6508. https://doi.org/10.3390/ijms25126508