
Disease-Modifying Effects of Lenvatinib, a Multiple Receptor Tyrosine Kinase Inhibitor, on Posttraumatic Osteoarthritis of the Knee

 , , and
, , and
Abstract
:
1. Introduction
2. Results
2.1. Preliminary Experiment
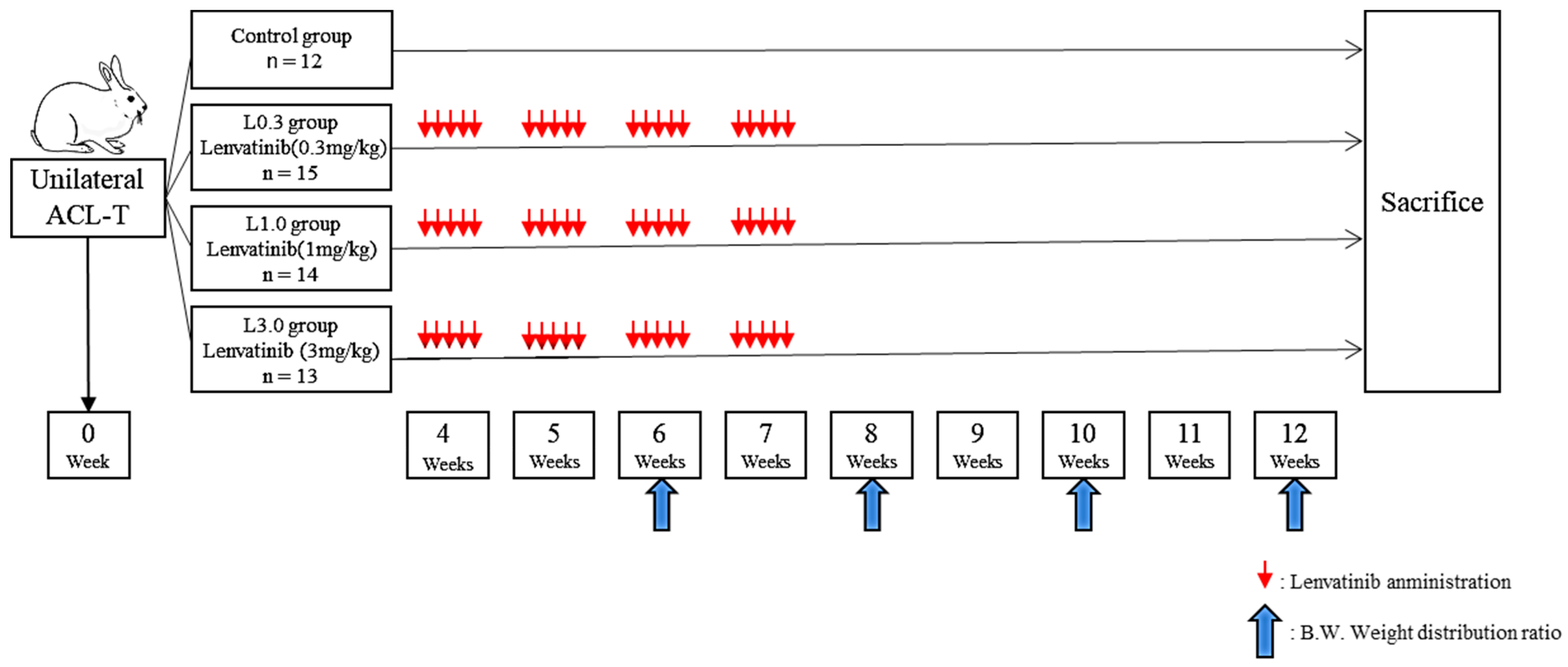
2.2. Application of Lenvatinib on ACLT-Induced Osteoarthritis Model in Rabbit
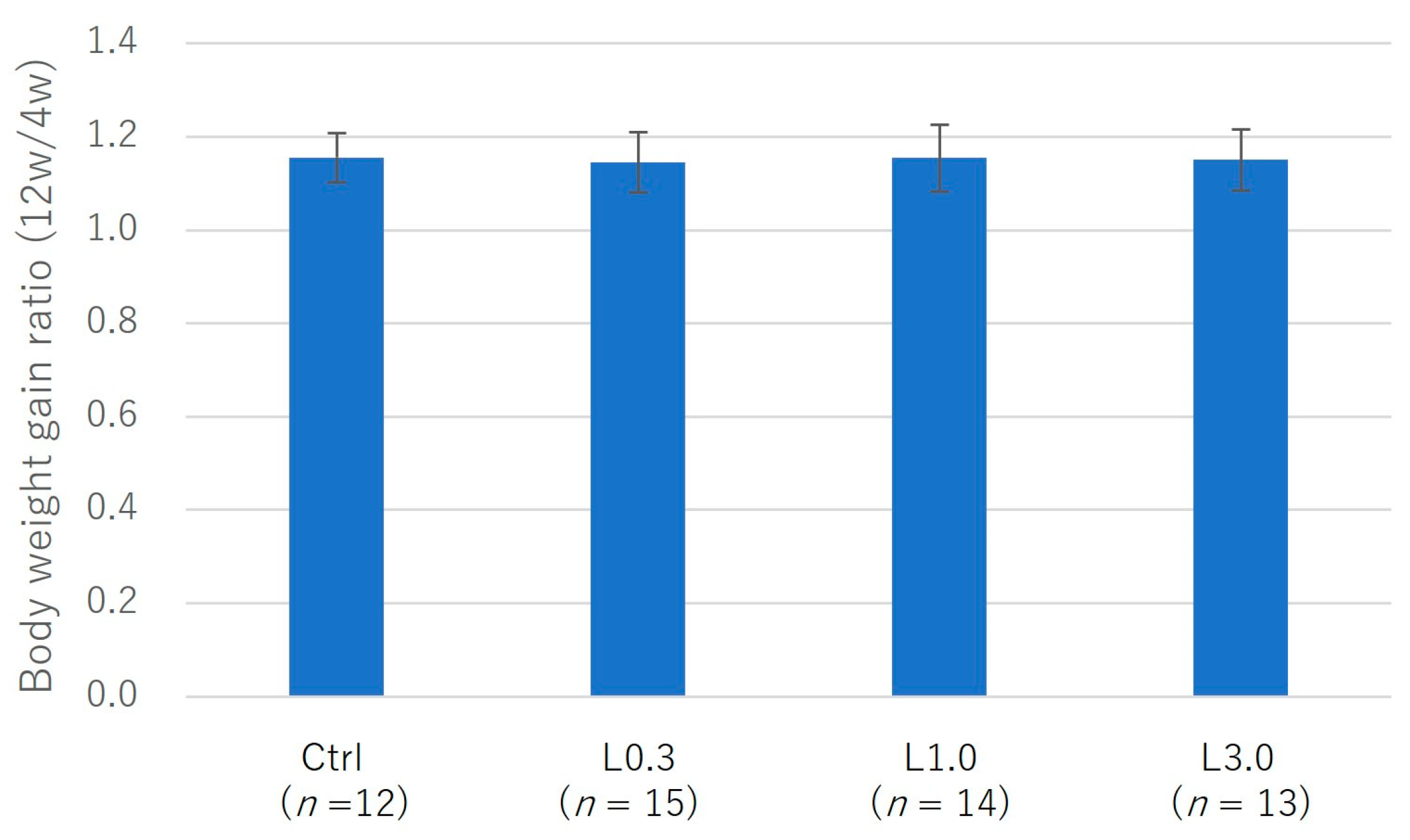
2.2.1. Adverse Events
2.2.2. Pain Evaluation
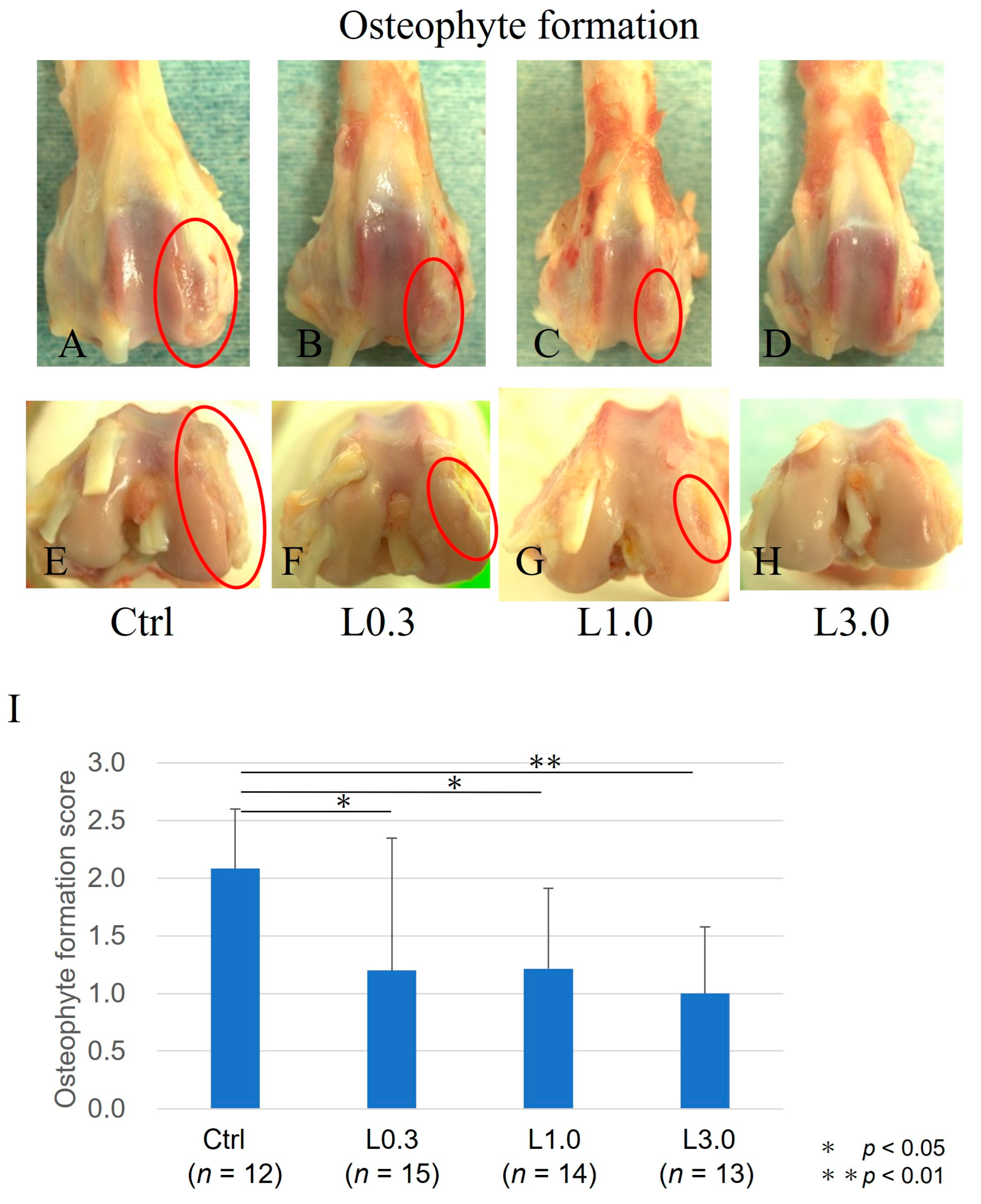
2.2.3. Comparison of Osteophyte Formation
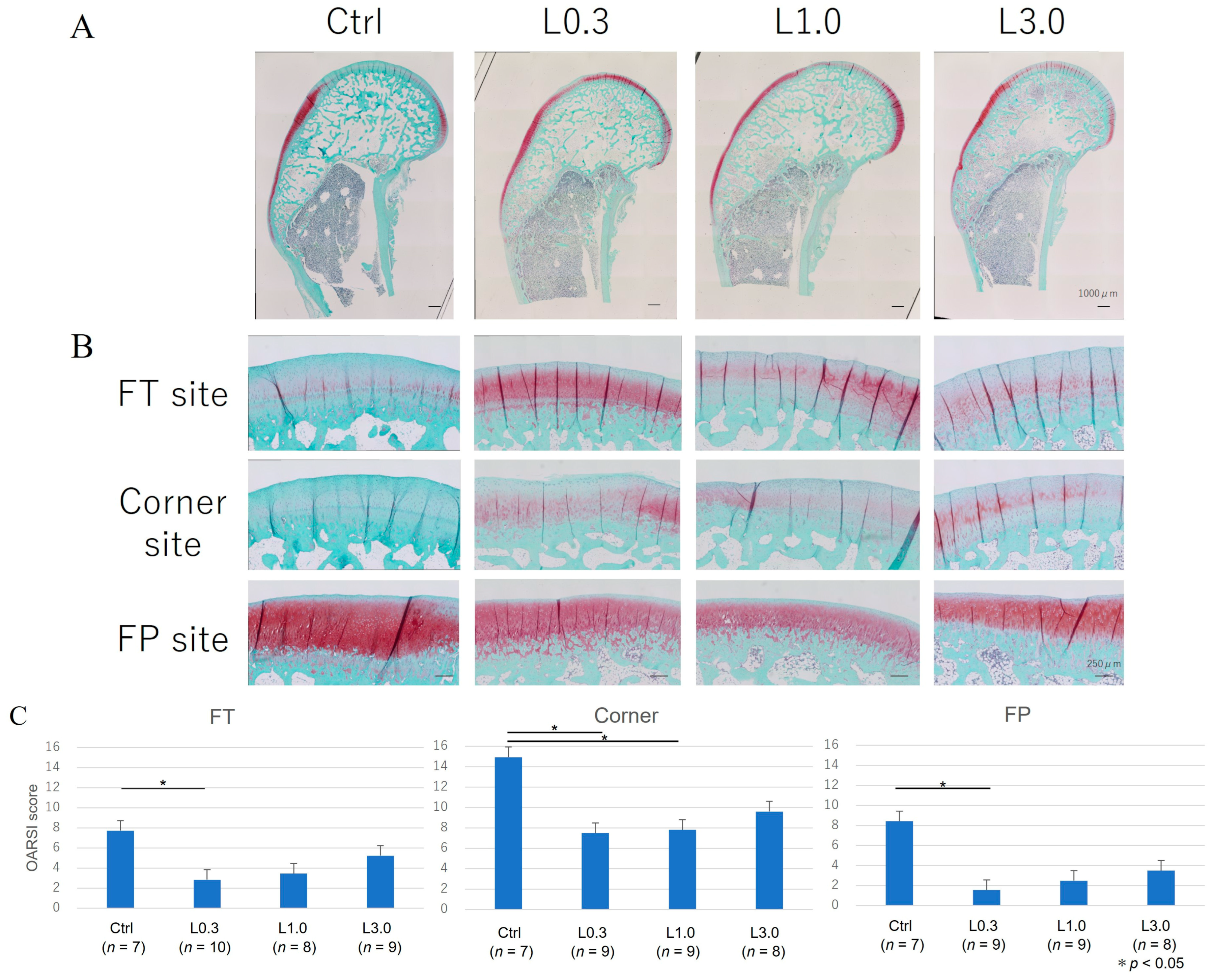
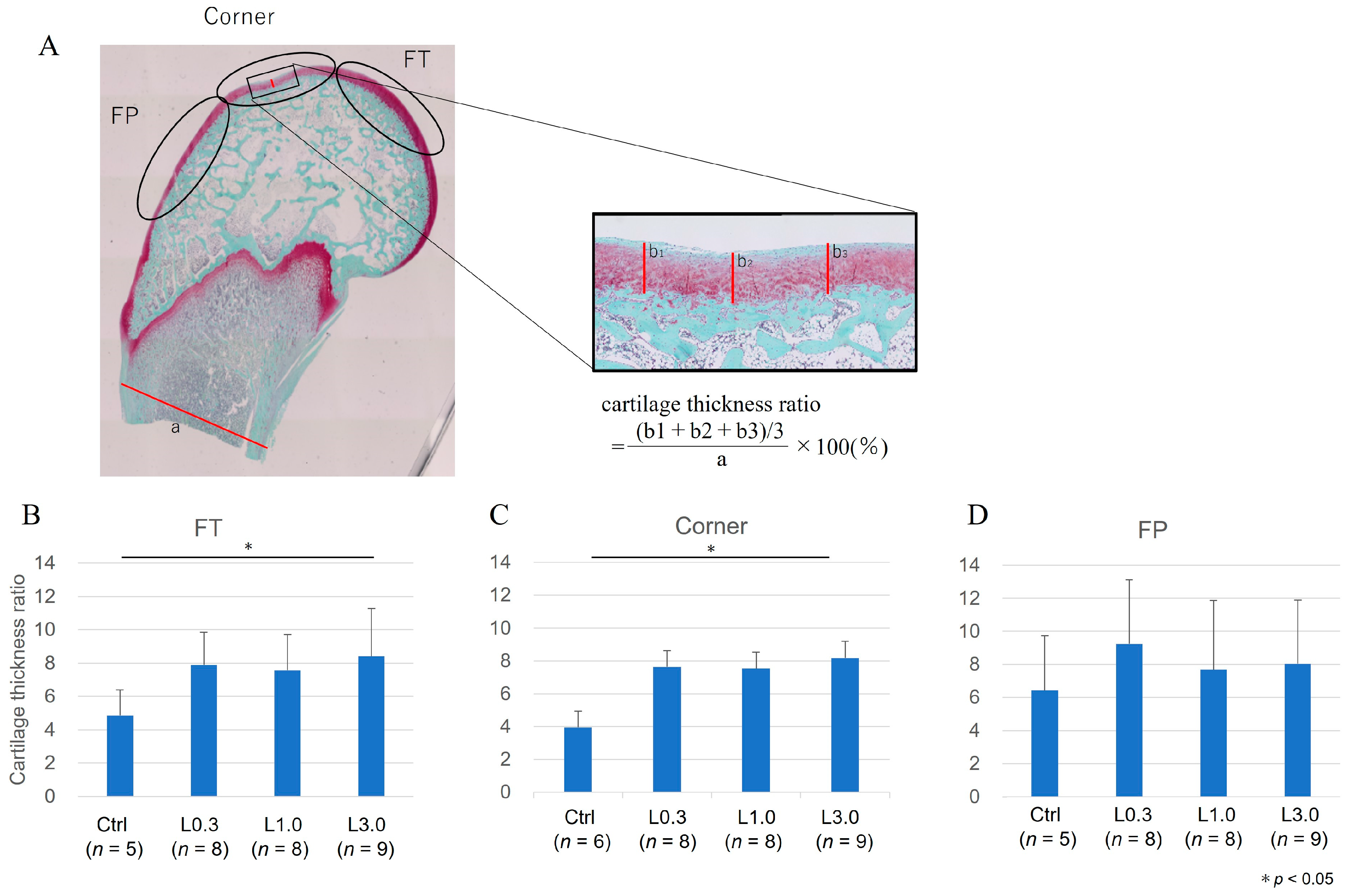
2.2.4. Histological Evaluation of the Articular Cartilage
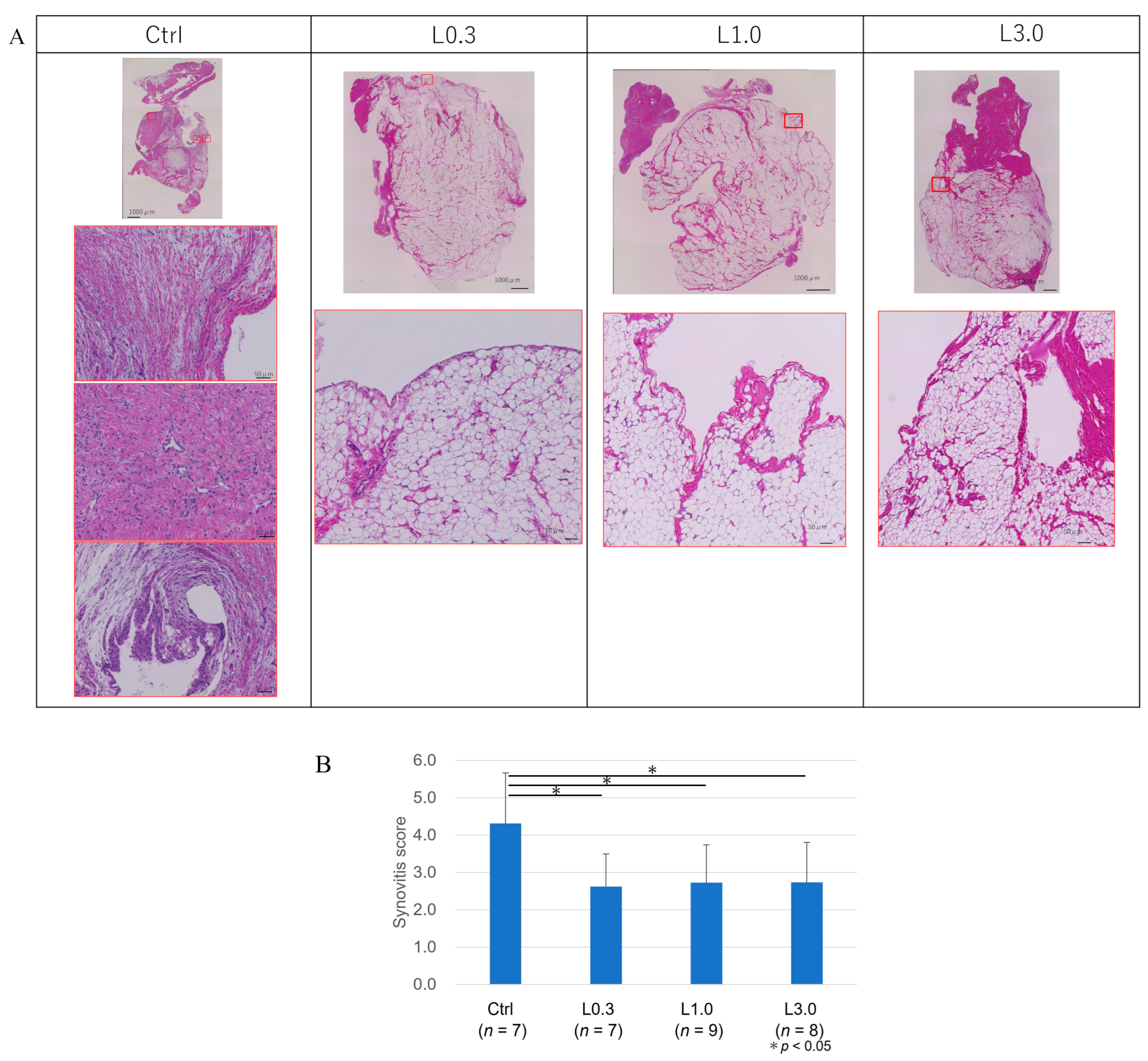
2.2.5. Histological Evaluation of the Synovium
2.2.6. Gene Expression in Articular Cartilage
3. Discussion
Limitations
4. Materials and Methods
4.1. Animals and Surgical Procedures
4.2. Lenvatinib Dose
4.3. Oral Administration of Lenvatinib
4.4. Experimental Design
4.5. Morphology of Osteophyte Formation
4.6. Histological Examination
4.7. Pain Evaluation
4.8. Gene Expression Analysis by Real-Time Polymerase Chain Reaction (PCR)
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawrence, R.C.; Helmick, C.G.; Arnett, F.C.; Deyo, R.A.; Felson, D.T.; Giannini, E.H.; Heyse, S.P.; Hirsch, R.; Hochberg, M.C.; Hunder, G.G.; et al. Estimates of the Prevalence of Arthritis and Selected Musculoskeletal Disorders in the United States. Arthritis Rheum. 1998, 41, 778–799. [Google Scholar] [CrossRef] [PubMed]
- Poole, A.R. Osteoarthritis as a whole joint disease. HSS J. 2012, 8, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Valdes, A.M.; Spector, T.D. Genetic epidemiology of hip and knee osteoarthritis. Nat. Rev. Rheumatol. 2011, 7, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Issa, S.N.; Sharma, L. Epidemiology of osteoarthritis: An update. Curr. Rheumatol. Rep. 2006, 8, 7–15. [Google Scholar] [CrossRef]
- Richette, P.; Poitou, C.; Garnero, P.; Vicaut, E.; Bouillot, J.L.; Lacorte, J.M.; Basdevant, A.; Clément, K.; Bardin, T.; Chevalier, X. Benefits of massive weight loss on symptoms, systemic inflammation, and cartilage turnover in obese patients with knee osteoarthritis. Ann. Rheum. Dis. 2011, 70, 139–144. [Google Scholar] [CrossRef]
- Brown, T.D.; Johnston, R.C.; Saltzman, C.L.; Marsh, J.; Buckwalter, J.A. Posttraumatic osteoarthritis: A first estimate of incidence, prevalence, and disease burden. J. Orthop. Trauma. 2006, 20, 739–744. [Google Scholar] [CrossRef]
- Srikanth, V.K.; Fryer, J.L.; Zhai, G.; Winzenberg, T.M.; Hosmer, D.; Jones, G. A Meta-Analysis of Sex Differences Prevalence, Incidence and Severity of Osteoarthritis. Osteoarthr. Cartil. 2005, 13, 769–781. [Google Scholar] [CrossRef]
- Tanamas, S.; Hanna, F.S.; Cicuttini, F.M.; Wluka, A.E.; Berry, P.; Urquhart, D.M. Does knee malalignment increase the risk of development and progression of knee osteoarthritis? A systematic review. Arthritis Care Res. 2009, 61, 459–467. [Google Scholar] [CrossRef]
- Roseti, L.; Desando, G.; Cavallo, C.; Petretta, M.; Grigolo, B. Articular cartilage regeneration in osteoarthritis. Cells 2019, 8, 1305. [Google Scholar] [CrossRef]
- Bonnet, C.S.; Walsh, D.A. Osteoarthritis, angiogenesis, and inflammation. Rheumatology 2005, 44, 7–16. [Google Scholar] [CrossRef]
- Mapp, P.I.; Walsh, D.A. Mechanisms and targets of angiogenesis and nerve growth in osteoarthritis. Nat. Rev. Rheumatol. 2012, 8, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Favero, M.; El-Hadi, H.; Belluzzi, E.; Granzotto, M.; Porzionato, A.; Sarasin, G.; Rambaldo, A.; Iacobellis, C.; Cigolotti, A.; Fontanella, C.G.; et al. Infrapatellar Fat Pad Features in Osteoarthritis: A Histopathological and Molecular Study. Rheumatol. (Oxf. ) 2017, 56, 1784–1793. [Google Scholar] [CrossRef] [PubMed]
- Belluzzi, E.; Macchi, V.; Fontanella, C.G.; Carniel, E.L.; Olivotto, E.; Filardo, G.; Sarasin, G.; Porzionato, A.; Granzotto, M.; Pozzuoli, A.; et al. Infrapatellar Fat Pad Gene Expression and Protein Production in Patients with and without Osteoarthritis. Int. J. Mol. Sci. 2020, 21, 6016. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.L.; Nagao, M.; Levine, B.R.; Chen, D.; Olsen, B.R.; Im, H.J. Targeting VEGF and its receptors for the treatment of osteoarthritis and associated pain. J. Bone Miner. Res. 2016, 31, 911–924. [Google Scholar] [CrossRef]
- Mabey, T.; Honsawek, S.; Saetan, N.; Poovorawan, Y.; Tanavalee, A.; Yuktanandana, P. Angiogenic Cytokine Expression Profiles in Plasma and Synovial Fluid of Primary Knee Osteoarthritis. Int. Orthop. 2014, 38, 1885–1892. [Google Scholar] [CrossRef]
- Nagai, T.; Sato, M.; Kutsuna, T.; Kokubo, M.; Ebihara, G.; Ohta, N.; Mochida, J. Intravenous administration of anti-vascular endothelial growth factor humanized monoclonal antibody bevacizumab improves articular cartilage repair. Arthritis Res. Ther. 2010, 12, R178. [Google Scholar] [CrossRef]
- Nagai, T.; Sato, M.; Kobayashi, M.; Yokoyama, M.; Tani, Y.; Mochida, J. Bevacizumab, an anti-vascular endothelial growth factor antibody, inhibits osteoarthritis. Arthritis Res. Ther. 2014, 16, 427. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, T.; Naganuma, A.; Kakizaki, S. Lenvatinib for hepatocellular carcinoma: A literature review. Pharmaceuticals 2021, 14, 36. [Google Scholar] [CrossRef]
- Yan, Z.; Yang, M.; Lai, C.L. Clinical efficacy of lenvatinib for the treatment of radioiodine-refractory thyroid carcinoma: A systematic review and meta-analysis of clinical trials. Clin. Endocrinol. 2021, 95, 478–488. [Google Scholar] [CrossRef]
- Casanovas, O.; Hicklin, D.J.; Bergers, G.; Hanahan, D. Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer Cell. 2005, 8, 299–309. [Google Scholar] [CrossRef]
- Tibesku, C.O.; Szuwart, T.; Ocken, S.A.; Skwara, A.; Fuchs, S. Increase in the expression of the transmembrane surface receptor CD44v6 on chondrocytes in animals with osteoarthritis. Arthritis Rheum. 2005, 52, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Pritzker, K.P.; Gay, S.; Jimenez, S.A.; Ostergaard, K.; Pelletier, J.P.; Revell, P.A.; Salter, D.; Van den Berg, W.B. Osteoarthritis cartilage histopathology: Grading and staging. Osteoarthr. Cartil. 2006, 14, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Krenn, V.; Morawietz, L.; Burmester, G.R.; Kinne, R.W.; Mueller-Ladner, U.; Muller, B.; Haupl, T. Synovitis score: Discrimination between chronic low-grade and high-grade synovitis. Histopathology 2006, 49, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Emmi, A.; Stocco, E.; Boscolo-Berto, R.; Contran, M.; Belluzzi, E.; Favero, M.; Macchi, V. Infrapatellar fat pad-synovial membrane anatomo-fuctional unit: Microscopic basis for Piezo1/2 mechanosensors involvement in osteoarthritis pain. Front. Cell Dev. Biol. 2022, 10, 886604. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, A.I.; Beekhuizen, M.; t Hart, M.C.; Radstake, T.R.; Dhert, W.J.; Saris, D.B.; van Osch, G.J.; Creemers, L.B. Cytokine profiles in the joint depend on pathology, but are different between synovial fluid, cartilage tissue and cultured chondrocytes. Arthritis Res. Ther. 2014, 16, 441. [Google Scholar] [CrossRef] [PubMed]
- Franses, R.E.; McWilliams, D.F.; Mapp, P.I.; Walsh, D.A. Osteochondral angiogenesis and increased protease inhibitor expression in OA. Osteoarthr. Cartil. 2010, 18, 563–571. [Google Scholar] [CrossRef]
- Lambert, C.; Mathy-Hartert, M.; Dubuc, J.E.; Montell, E.; Vergés, J.; Munaut, C.; Noël, A.; Henrotin, Y. Characterization of synovial angiogenesis in osteoarthritis patients and its modulation by chondroitin sulfate. Arthritis Res. Ther. 2012, 14, R58. [Google Scholar] [CrossRef] [PubMed]
- Haywood, L.; McWilliams, D.F.; Pearson, C.I.; Gill, S.E.; Ganesan, A.; Wilson, D.; Walsh, D.A. Inflammation and angiogenesis in osteoarthritis. Arthritis Rheum. 2003, 48, 2173–2177. [Google Scholar] [CrossRef] [PubMed]
- Sohn, D.; Sokolove, J.; Sharpe, O.; Erhart, J.C.; Chandra, P.E.; Lahey, L.J.; Lindstrom, T.M.; Hwang, I.; Boyer, K.A.; Andriacchi, T.P.; et al. Plasma proteins present in osteoarthritic synovial fluid can stimulate cytokine production via Toll-like receptor 4. Arthritis Res. Ther. 2012, 14, R7. [Google Scholar] [CrossRef] [PubMed]
- Corrado, A.; Neve, A.; Cantatore, F.P. Expression of vascular endothelial growth factor in normal, osteoarthritic and osteoporotic osteoblasts. Clin. Exp. Med. 2013, 13, 81–84. [Google Scholar] [CrossRef]
- Saetan, N.; Honsawek, S.; Tanavalee, A.; Yuktanandana, P.; Meknavin, S.; Ngarmukos, S.; Tanpowpong, T.; Parkpian, V. Relationship of plasma and synovial fluid vascular endothelial growth factor with radiographic severity in primary knee osteoarthritis. Int. Orthop. 2014, 38, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.Y.; Hao, Y.R.; Wang, Z.; Zhou, J.L.; Jia, Q.X.; Qiu, B. The effect of vascular endothelial growth factor on aggrecan and type II collagen expression in rat articular chondrocytes. Rheumatol. Int. 2012, 32, 3359–3364. [Google Scholar] [CrossRef] [PubMed]
- Sotozawa, M.; Kumagai, K.; Ishikawa, K.; Yamada, S.; Inoue, Y.; Inaba, Y. Bevacizumab suppressed degenerative changes in articular cartilage explants from patients with osteoarthritis of the knee. J. Orthop. Surg. Res. 2023, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Nagao, M.; Hamilton, J.L.; Kc, R.; Berendsen, A.D.; Duan, X.; Cheong, C.W.; Li, X.; Im, H.; Olsen, B.R. Vascular Endothelial Growth Factor in Cartilage Development and Osteoarthritis. Sci. Rep. 2017, 7, 13027. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.; Singh, G.; Wang, J.; O-Sullivan, I.; Votta-Velis, G.; Bruce, B.; Anbazhagan, A.N.; Wijnen, A.J.; Im, H. Targeting Vascular Endothelial Growth Factor Receptors as a Therapeutic Strategy for Osteoarthritis and Associated Pain. Int. J. Biol. Sci. 2023, 19, 675–690. [Google Scholar] [CrossRef]
- Abdullah, S.E.; Perez-Soler, R. Mechanisms of resistance to vascular endothelial growth factor blockade. Cancer 2012, 118, 3455–3467. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Ellman, M.B.; Kroin, J.S.; Chen, D.; Yan, D.; Mikecz, K.; Ranjan, K.C.; Xiao, G.; Stein, G.S.; Kim, S.G.; et al. Species-specific biological effects of FGF-2 in articular cartilage: Implication for distinct roles within the FGF receptor family. J. Cell. Biochem. 2012, 113, 2532–2542. [Google Scholar] [CrossRef] [PubMed]
- Ellman, M.B.; Yan, D.; Ahmadinia, K.; Chen, D.; An, H.S.; Im, H.J. Fibroblast growth factor control of cartilage homeostasis. J. Cell. Biochem. 2013, 114, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.M.G.; Beier, F.; Pest, M.A. Recent developments in emerging therapeutic targets of osteoarthritis. Curr. Opin. Rheumatol. 2017, 29, 96. [Google Scholar] [CrossRef]
- Capozzi, M.; De Divitiis, C.; Ottaiano, A.; von Arx, C.; Scala, S.; Tatangelo, F.; Delrio, P.; Tafuto, S. Lenvatinib, a molecule with versatile application: From preclinical evidence to future development in anti-cancer treatment. Cancer Manag Res. 2018, 11, 3847–3860. [Google Scholar] [CrossRef]
- Vadala, G.; Ambrosio, L.; Cattani, C.; Cattani, C.; Bernardini, R.; Giacalone, A.; Papalia, R.; Denaro, V. Bevacizumab arrests osteoarthritis progression in a rabbit model: A dose-escalation study. J. Clin. Med. 2021, 10, 2825. [Google Scholar] [CrossRef]
- Lee, J.S.; Guo, P.; Klett, K.; Hall, M.; Sinha, K.; Ravuri, S.; Huard, J.; Murphy, W.L. VEGF-attenuated platelet-rich plasma improves therapeutic effect on cartilage repair. Biomater. Sci. 2022, 10, 2172–2181. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving Bioscience Research Reporting: The ARRIVE Guidelines for Reporting Animal Research. PLoS Biol. 2010, 8, e1000412. [Google Scholar] [CrossRef]
- Yudoh, K.; Shishido, K.; Murayama, H.; Yano, M.; Matsubayashi, K.; Takada, H.; Nakamura, H.; Masuko, K.; Kato, T.; Nishioka, K. Water-soluble C60 fullerene prevents degeneration of articular cartilage in osteoarthritis via down-regulation of chondrocyte catabolic activity and inhibition of cartilage degeneration during disease development. Arthritis Rheum. 2007, 56, 3307–3318. [Google Scholar] [CrossRef]
- Dubbelman, A.C.; Rosing, H.; Nijenhuis, C.; Huitema, A.D.; Mergui-Roelvink, M.; Gupta, A.; Verbel, D.; Thompson, G.; Shumaker, R.; Schellens, J.H.; et al. Pharmacokinetics and excretion of 14C-lenvatinib in patients with advanced solid tumors or lymphomas. Invest. New Drugs 2015, 33, 233–240. [Google Scholar] [CrossRef]
- Motzer, R.J.; Taylor, M.H.; Evans, T.R.J.; Okusaka, T.; Glen, H.; Lubiniecki, G.M.; Dutcus, C.; Smith, A.D.; Okpara, C.E.; Hussein, Z.; et al. Lenvatinib dose, efficacy, and safety in the treatment of multiple malignancies. Expert Rev. Anticancer Ther. 2022, 22, 383–400. [Google Scholar] [CrossRef]
- Inoue, K.; Asai, N.; Mizuo, H.; Fukuda, K.; Kusano, K.; Yoshimura, T. Unique metabolic pathway of [14C] lenvatinib after oral administration to male cynomolgus monkey. Drug Metab. Dispos. 2012, 40, 662–670. [Google Scholar] [CrossRef]
- Bruheim, S.; Kristian, A.; Uenaka, T.; Suo, Z.; Tsuruoka, A.; Nesland, J.M.; Fodstad, Ø. Antitumour activity of oral E7080, a novel inhibitor of multiple tyrosine kinases, in human sarcoma xenografts. Int. J. Cancer 2011, 129, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Hsia, A.W.; Emami, A.J.; Tarke, F.D.; Cunningham, H.C.; Tjandra, P.M.; Wong, A.; Christiansen, B.A.; Collette, N.M. Osteophytes and Fracture Calluses Share Developmental Milestones and Are Diminished by Unloading. J. Orthop. Res. 2018, 36, 699–710. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Gene | Primer Sequence: Forward | Primer Sequence: Reverse |
|---|---|---|
| GAPDH | 5′-AAGGTCGGAGTGAACGGATT-3′ | 5′-TGGCGACAACATCCACTTTG-3′ |
| MMP3 | 5′-ACACCGGATCTGCCAAGAGA-3′ | 5′-CTGGAGAACGTGAGTGGAGTCA-3′ |
| MMP13 | 5′-GATGCCATTACCAGTCTCC-3′ | 5′-GCTGTATTCAAACTGTATGG-3′ |
| VEGFA | 5′-TGCCCACCGAGGAGTTCA-3′ | 5′-GGCCCTGGTGAGGTTTGAT-3′ |
| ADAMTS-5 | 5′-GACAAGAGCCTGGAGGTGAG-3′ | 5′-AGGCATCGATACTGGTGAGG-3′ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sogo, Y.; Toyoda, E.; Nagai, T.; Takahashi, T.; Takizawa, D.; Watanabe, M.; Sato, M. Disease-Modifying Effects of Lenvatinib, a Multiple Receptor Tyrosine Kinase Inhibitor, on Posttraumatic Osteoarthritis of the Knee. Int. J. Mol. Sci. 2024, 25, 6514. https://doi.org/10.3390/ijms25126514
Sogo Y, Toyoda E, Nagai T, Takahashi T, Takizawa D, Watanabe M, Sato M. Disease-Modifying Effects of Lenvatinib, a Multiple Receptor Tyrosine Kinase Inhibitor, on Posttraumatic Osteoarthritis of the Knee. International Journal of Molecular Sciences. 2024; 25(12):6514. https://doi.org/10.3390/ijms25126514
Chicago/Turabian StyleSogo, Yasuyuki, Eriko Toyoda, Toshihiro Nagai, Takumi Takahashi, Daichi Takizawa, Masahiko Watanabe, and Masato Sato. 2024. "Disease-Modifying Effects of Lenvatinib, a Multiple Receptor Tyrosine Kinase Inhibitor, on Posttraumatic Osteoarthritis of the Knee" International Journal of Molecular Sciences 25, no. 12: 6514. https://doi.org/10.3390/ijms25126514