
The Addition of Hydroxyapatite Nanoparticles on Implant Surfaces Modified by Zirconia Blasting and Acid Etching to Enhance Peri-Implant Bone Healing

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Structural Characterization
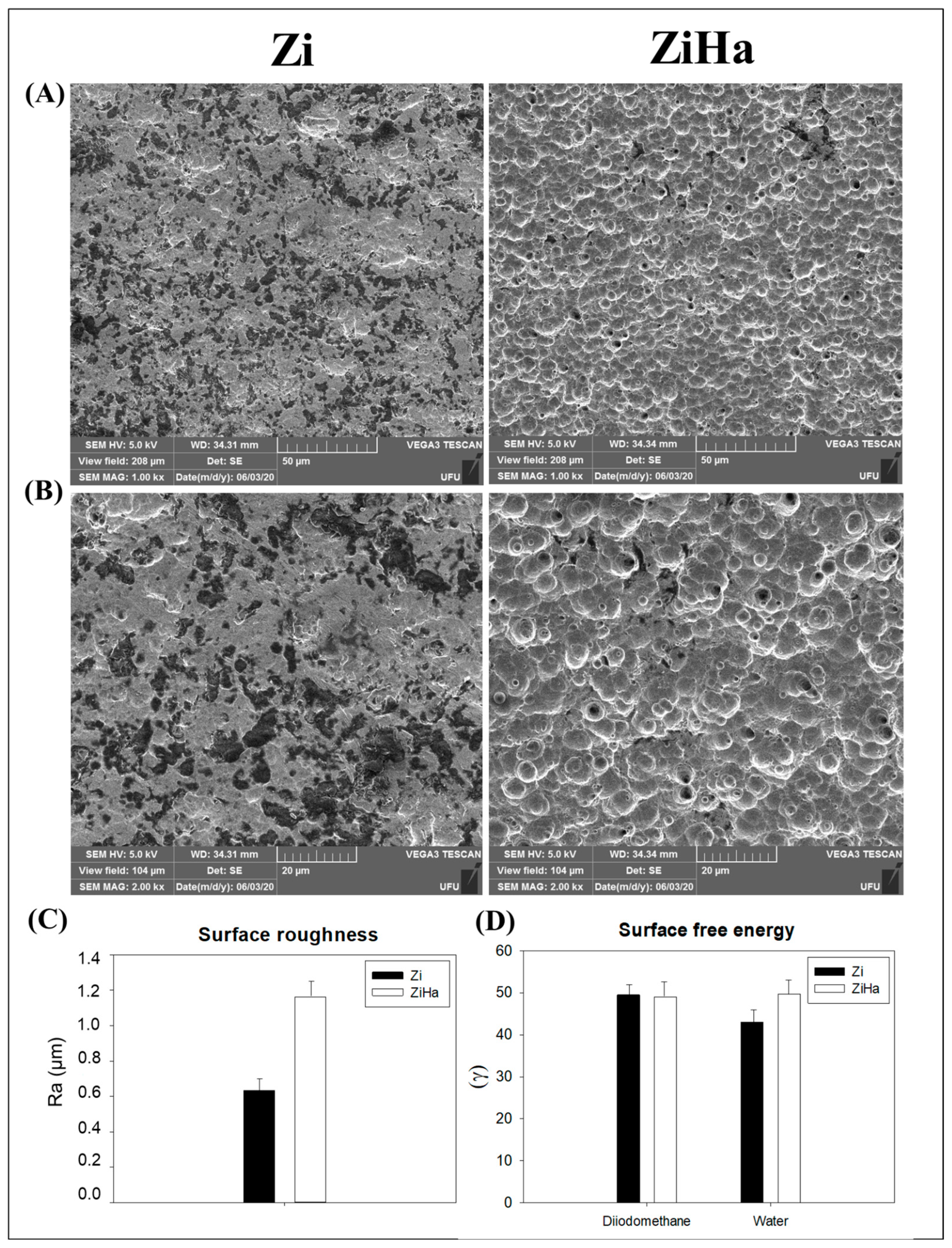
2.1.1. Scanning Electron Microscopy (SEM)
2.1.2. Profilometry—Surface Roughness Analysis
2.1.3. Surface Free Energy
2.2. Histological Analysis
2.3. Immunohistochemistry
2.4. Biomechanical Analysis (Reverse Torque)
2.5. Histometry
3. Discussion
4. Materials and Methods
4.1. Implants/Discs Coating by Zirconia Blasting and Acid Etching with the Addition of Hydroxyapatite Nanoparticles
4.2. Structural Characterization
4.2.1. Scanning Electron Microscopy (SEM)
4.2.2. Profilometry—Analysis of Surface Roughness
4.2.3. Surface Free Energy
4.3. In Vivo Study: Experimental Design
4.4. Ovariectomy Procedure
4.5. Implant Surgery Sequence
4.6. Peri-Implant Bone Healing Assessment
4.6.1. Analyses for Decalcified Tissues
Histological Analysis
Immunohistochemical Reactions
4.6.2. Analyses for Calcified Tissues
Biomechanical Analysis of Implants (Reverse Torque)
Histometric Analysis
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alghamdi, H.S.; Jansen, J.A. The development and future of dental implants. Dent. Mater. J. 2020, 39, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Ahn, T.-K.; Lee, D.H.; Kim, T.-S.; Jang, G.C.; Choi, S.; Oh, J.B.; Ye, G.; Lee, S. Modification of Titanium Implant and Titanium Dioxide for Bone Tissue Engineering. In Novel Biomaterials for Regenerative Medicine; Chun, H.J., Park, K., Kim, C.-H., Khang, G., Eds.; Springer: Singapore, 2018; pp. 355–368. [Google Scholar] [CrossRef]
- Gittens, R.A.; Olivares-Navarrete, R.; Schwartz, Z.; Boyan, B.D. Implant osseointegration and the role of microroughness and nanostructures: Lessons for spine implants. Acta Biomater. 2014, 10, 3363–3371. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Jansen, J.A.; Walboomers, X.F.; van den Beucken, J.J. Mechanical aspects of dental implants and osseointegration: A narrative review. J. Mech. Behav. Biomed. Mater. 2020, 103, 103574. [Google Scholar] [CrossRef] [PubMed]
- Chai, W.L.; Razali, M.; Moharamzadeh, K.; Zafar, M.S. 10—The hard and soft tissue interfaces with dental implants. In Dental Implants; Zafar, M.S., Khurshid, Z., Khan, A.S., Najeeb, S., Sefat, F., Eds.; Woodhead Publishing: Sawston, UK, 2020; pp. 173–201. [Google Scholar] [CrossRef]
- De Bruyn, H.; Christiaens, V.; Doornewaard, R.; Jacobsson, M.; Cosyn, J.; Jacquet, W.; Vervaeke, S. Implant surface roughness and patient factors on long-term peri-implant bone loss. Periodontology 2000 2017, 73, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Hatamleh, M.M.; Wu, X.; Alnazzawi, A.; Watson, J.; Watts, D. Surface characteristics and biocompatibility of cranioplasty titanium implants following different surface treatments. Dent. Mater. 2018, 34, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Rupp, F.; Liang, L.; Geis-Gerstorfer, J.; Scheideler, L.; Hüttig, F. Surface characteristics of dental implants: A review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, G.; Francetti, L.; Barbaro, B.; del Fabbro, M. Novel surfaces and osseointegration in implant dentistry. J. Investig. Clin. Dent. 2018, 9, e12349. [Google Scholar] [CrossRef] [PubMed]
- Kligman, S.; Ren, Z.; Chung, C.-H.; Perillo, M.A.; Chang, Y.-C.; Koo, H.; Zheng, Z.; Li, C. The Impact of Dental Implant Surface Modifications on Osseointegration and Biofilm Formation. J. Clin. Med. 2021, 10, 1641. [Google Scholar] [CrossRef] [PubMed]
- Jemat, A.; Ghazali, M.J.; Razali, M.; Otsuka, Y. Surface Modifications and Their Effects on Titanium Dental Implants. BioMed Res. Int. 2015, 2015, 791725. [Google Scholar] [CrossRef] [PubMed]
- Thormann, U.; El Khawassna, T.; Ray, S.; Duerselen, L.; Kampschulte, M.; Lips, K.; von Dewitz, H.; Heinemann, S.; Heiss, C.; Szalay, G.; et al. Differences of bone healing in metaphyseal defect fractures between osteoporotic and physiological bone in rats. Injury 2014, 45, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, N.T.; Guastaldi, F.P.; Perrotti, V.; Hochuli-Vieira, E.; Guastaldi, A.C.; Piattelli, A.; Iezzi, G. Biomedical Ti-Mo alloys with surface machined and modified by laser beam: Biomechanical, histological, and histometric analysis in rabbits. Clin. Implant. Dent. Relat. Res. 2013, 15, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, T.P.; Souza, F.Á.; Guastaldi, A.C.; Margonar, R.; Garcia-Júnior, I.R.; Hochuli-Vieira, E. Commercially pure titanium implants with surfaces modified by laser beam with and without chemical deposition of apatite. Biomechanical and topographical analysis in rabbits. Clin. Oral Implant. Res. 2013, 24, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Mendes, M.W.; Ágreda, C.G.; Bressiani, A.H.; Bressiani, J.C. A new titanium based alloy Ti–27Nb–13Zr produced by powder metallurgy with biomimetic coating for use as a biomaterial. Mater. Sci. Eng. C 2016, 63, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Souza, F.A.; Queiroz, T.P.; Guastaldi, A.C.; Garcia-Júnior, I.R.; Magro-Filho, O.; Nishioka, R.S.; Sisti, K.E.; Sonoda, C.K. Comparative in vivo study of commercially pure Ti implants with surfaces modified by laser with and without silicate deposition: Biomechanical and scanning electron microscopy analysis. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101B, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Lee, J. Nanoscale hydroxyapatite particles for bone tissue engineering. Acta Biomater. 2011, 7, 2769–2781. [Google Scholar] [CrossRef] [PubMed]
- Poinern, G.E.; Brundavanam, R.K.; Mondinos, N.; Jiang, Z.-T. Synthesis and characterisation of nanohydroxyapatite using an ultrasound assisted method. Ultrason. Sonochem. 2009, 16, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Souza, J.C.M.; Sordi, M.B.; Kanazawa, M.; Ravindran, S.; Henriques, B.; Silva, F.S.; Aparicio, C.; Cooper, L.F. Nano-scale modification of titanium implant surfaces to enhance osseointegration. Acta Biomater. 2019, 94, 112–131. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Barrena, E.; Rosset, P.; Lozano, D.; Stanovici, J.; Ermthaller, C.; Gerbhard, F. Bone fracture healing: Cell therapy in delayed unions and nonunions. Bone 2015, 70, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Lupsa, B.C.; Insogna, K. Bone Health and Osteoporosis. Endocrinol. Metab. Clin. N. Am. 2015, 44, 517–530. [Google Scholar] [CrossRef]
- Grisa, A.; Veitz-Keenan, A. Is osteoporosis a risk factor for implant survival or failure? Evid.-Based Dent. 2018, 19, 51–52. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Yu, Q. Primary osteoporosis in postmenopausal women. Chronic Dis. Transl. Med. 2015, 1, 9–13. [Google Scholar] [CrossRef] [PubMed]
- MacKnight, J.M. Osteopenia and Osteoporosis in Female Athletes. Clin. Sports Med. 2017, 36, 687–702. [Google Scholar] [CrossRef]
- Tella, S.H.; Gallagher, J.C. Prevention and treatment of postmenopausal osteoporosis. J. Steroid Biochem. Mol. Biol. 2014, 142, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Faverani, L.P.; Barão, V.A.R.; Ramalho-Ferreira, G.; Ferreira, M.B.; Garcia-Júnior, I.R.; Assunção, W.G. Effect of bleaching agents and soft drink on titanium surface topography. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Ramalho-Ferreira, G.; Faverani, L.P.; Grossi-Oliveira, G.A.; Okamoto, T.; Okamoto, R. Alveolar bone dynamics in osteoporotic rats treated with raloxifene or alendronate: Confocal microscopy analysis. J. Biomed. Opt. 2015, 20, 038003. [Google Scholar] [CrossRef] [PubMed]
- Harrasser, N.; Gorkotte, J.; Obermeier, A.; Feihl, S.; Straub, M.; Slotta-Huspenina, J.; von Eisenhart-Rothe, R.; Moser, W.; Gruner, P.; de Wild, M.; et al. A new model of implant-related osteomyelitis in the metaphysis of rat tibiae. BMC Musculoskelet. Disord. 2016, 17, 152. [Google Scholar] [CrossRef] [PubMed]
- Polo, T.O.B.; Silva, W.P.P.; Momesso, G.A.C.; Lima-Neto, T.J.; Barbosa, S.; Cordeiro, J.M.; Hassumi, J.S.; da Cruz, N.C.; Okamoto, R.; Barão, V.A.R.; et al. Plasma Electrolytic Oxidation as a Feasible Surface Treatment for Biomedical Applications: An in vivo study. Sci. Rep. 2020, 10, 10000. [Google Scholar] [CrossRef] [PubMed]
- Marques, I.S.V.; Nilson, C.C.; Landers, R.; Yuan, J.C.C.; Mesquita, M.F.; Sukotjo, C.; Mathew, T.; Barao, V.A.D. Incorporation of Ca, P, and Si on bioactive coatings produced by plasma electrolytic oxidation: The role of electrolyte concentration and treatment duration. Biointerphases 2015, 10, 41002. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Van Duyn, C.; Cohen, D.J.; Schwartz, Z.; Boyan, B.D. Strategies for Improving Impaired Osseointegration in Compromised Animal Models. J. Dent. Res. 2024, 103, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Louropoulou, A.; Slot, D.E.; Van der Weijden, F. Influence of mechanical instruments on the biocompatibility of titanium dental implants surfaces: A systematic review. Clin. Oral Implant. Res. 2015, 26, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Bone and Bone Graft Healing. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Prideaux, M.; Findlay, D.M.; Atkins, G.J. Osteocytes: The master cells in bone remodelling. Curr. Opin. Pharmacol. 2016, 28, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Dempster, D.W.; Compston, J.E.; Drezner, M.K.; Glorieux, F.H.; Kanis, J.A.; Malluche, H.; Meunier, P.J.; Ott, S.M.; Recker, R.R.; Parfitt, A.M. Standardized nomenclature, symbols, and units for bone histomorphometry: A 2012 update of the report of the ASBMR Histomorphometry Nomenclature Committee. J. Bone Miner. Res. 2013, 28, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Voumard, B.; Maquer, G.; Heuberger, P.; Zysset, P.K.; Wolfram, U. Peroperative estimation of bone quality and primary dental implant stability. J. Mech. Behav. Biomed. Mater. 2019, 92, 24–32. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Choi, N.-R.; Kim, Y.-D. The factors that influence postoperative stability of the dental implants in posterior edentulous maxilla. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 2. [Google Scholar] [CrossRef] [PubMed]
- Bacchelli, B.; Giavaresi, G.; Franchi, M.; Martini, D.; De Pasquale, V.; Trirè, A.; Fini, M.; Giardino, R.; Ruggeri, A. Influence of a zirconia sandblasting treated surface on peri-implant bone healing: An experimental study in sheep. Acta Biomater. 2009, 5, 2246–2257. [Google Scholar] [CrossRef] [PubMed]
- Franchi, M.; Orsini, E.; Triré, A.; Quaranta, M.; Martini, D.; Piccari, G.G.; Ruggeri, A.; Ottani, V. Osteogenesis and morphology of the peri-implant bone facing dental implants. Sci. World J. 2004, 4, 1083–1095. [Google Scholar] [CrossRef]
- Franchi, M.; Bacchelli, B.; Giavaresi, G.; De Pasquale, V.; Martini, D.; Fini, M.; Giardino, R.; Ruggeri, A. Influence of Different Implant Surfaces on Peri-Implant Osteogenesis: Histomorphometric Analysis in Sheep. J. Periodontol. 2007, 78, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Homa, K.; Zakrzewski, W.; Dobrzyński, W.; Piszko, P.J.; Piszko, A.; Matys, J.; Wiglusz, R.J.; Dobrzyński, M. Surface Functionalization of Titanium-Based Implants with a Nanohydroxyapatite Layer and Its Impact on Osteoblasts: A Systematic Review. J. Funct. Biomater. 2024, 15, 45. [Google Scholar] [CrossRef] [PubMed]
- Faverani, L.P.; Assunçao, W.G.; de Carvalho, P.S.P.; Yuan, J.C.C.; Sukotjo, C.; Mathew, M.T.; Barao, V.A. Effects of Dextrose and Lipopolysaccharide on the Corrosion Behavior of a Ti-6Al-4V Alloy with a Smooth Surface or Treated with Double-Acid-Etching. PLoS ONE 2014, 9, e93377. [Google Scholar] [CrossRef] [PubMed]
- Barão, V.A.R.; Mathew, M.T.; Assunção, W.G.; Yuan, J.C.; Wimmer, M.A.; Sukotjo, C. Stability of cp-Ti and Ti-6Al-4V alloy for dental implants as a function of saliva pH—An electrochemical study. Clin. Oral Implant. Res. 2012, 23, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Jalota, S.; Bhaduri, S.B.; Tas, A.C. Effect of carbonate content and buffer type on calcium phosphate formation in SBF solutions. J. Mater. Sci. Mater. Med. 2006, 17, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Faverani, L.P.; Barao, V.A.R.; Pires, M.F.A.; Yuan, J.C.-C.; Sukotjo, C.; Mathew, M.T.; Assunção, W.G. Corrosion kinetics and topography analysis of Ti–6Al–4V alloy subjected to different mouthwash solutions. Mater. Sci. Eng. C 2014, 43, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Combe, E. A protocol for determining the surface free energy of dental materials. Dent. Mater. 2004, 20, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Momesso, G.A.C.; Santos, A.M.d.S.; e Santos, J.M.F.; da Cruz, N.C.; Okamoto, R.; Barão, V.A.R.; Siroma, R.S.; Shibli, J.A.; Faverani, L.P. Comparison between Plasma Electrolytic Oxidation Coating and Sandblasted Acid-Etched Surface Treatment: Histometric, Tomographic, and Expression Levels of Osteoclastogenic Factors in Osteoporotic Rats. Materials 2020, 13, 1604. [Google Scholar] [CrossRef] [PubMed]
- Luvizuto, E.R.; Dias, S.S.; Okamoto, T.; Dornelles, R.C.; Okamoto, R. Raloxifene therapy inhibits osteoclastogenesis during the alveolar healing process in rats. Arch. Oral Biol. 2011, 56, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Hassumi, J.S.; Mulinari-Santos, G.; Fabris, A.L.d.S.; Jacob, R.G.M.; Gonçalves, A.; Rossi, A.C.; Freire, A.R.; Faverani, L.P.; Okamoto, R. Alveolar bone healing in rats: Micro-CT, immunohistochemical and molecular analysis. J. Appl. Oral Sci. 2018, 26, e20170326. [Google Scholar] [CrossRef] [PubMed]
- Luvizuto, E.R.; Queiroz, T.P.; Dias, S.M.D.; Okamoto, T.; Dornelles, R.C.M.; Garcia, I.R.; Okamoto, R. Histomorphometric analysis and immunolocalization of RANKL and OPG during the alveolar healing process in female ovariectomized rats treated with oestrogen or raloxifene. Arch. Oral Biol. 2010, 55, 52–59. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toscano, R.A.; Barbosa, S.; Campos, L.G.; de Sousa, C.A.; Dallazen, E.; Mourão, C.F.; Shibli, J.A.; Ervolino, E.; Faverani, L.P.; Assunção, W.G. The Addition of Hydroxyapatite Nanoparticles on Implant Surfaces Modified by Zirconia Blasting and Acid Etching to Enhance Peri-Implant Bone Healing. Int. J. Mol. Sci. 2024, 25, 7321. https://doi.org/10.3390/ijms25137321
Toscano RA, Barbosa S, Campos LG, de Sousa CA, Dallazen E, Mourão CF, Shibli JA, Ervolino E, Faverani LP, Assunção WG. The Addition of Hydroxyapatite Nanoparticles on Implant Surfaces Modified by Zirconia Blasting and Acid Etching to Enhance Peri-Implant Bone Healing. International Journal of Molecular Sciences. 2024; 25(13):7321. https://doi.org/10.3390/ijms25137321
Chicago/Turabian StyleToscano, Ricardo Alves, Stéfany Barbosa, Larissa Gabriele Campos, Cecília Alves de Sousa, Eduardo Dallazen, Carlos Fernando Mourão, Jamil Awad Shibli, Edilson Ervolino, Leonardo P. Faverani, and Wirley Goncalves Assunção. 2024. "The Addition of Hydroxyapatite Nanoparticles on Implant Surfaces Modified by Zirconia Blasting and Acid Etching to Enhance Peri-Implant Bone Healing" International Journal of Molecular Sciences 25, no. 13: 7321. https://doi.org/10.3390/ijms25137321