
The Combination of Chitosan-Based Biomaterial and Cellular Therapy for Successful Treatment of Diabetic Foot—Pilot Study
 , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Isolation of MSC from Bone Marrow
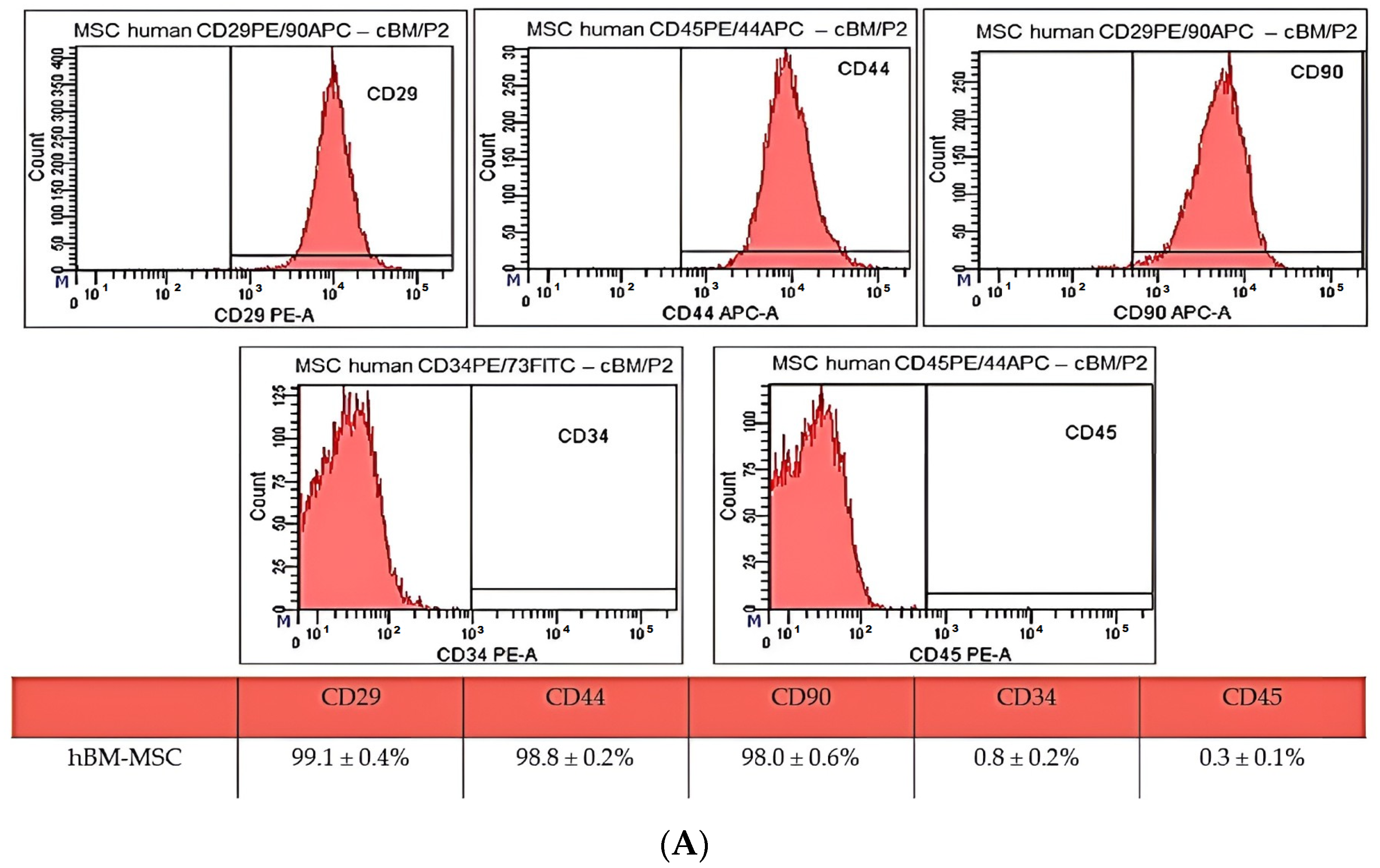
2.2. CD Characterization of Human Bone Marrow MSC
2.3. Multilineage Potential
2.4. Isolation and Characterization of Human Dermal Fibroblast Primary Culture
2.5. Preparation, Characterization and In Vitro Testing of Biopolymer Scaffolds
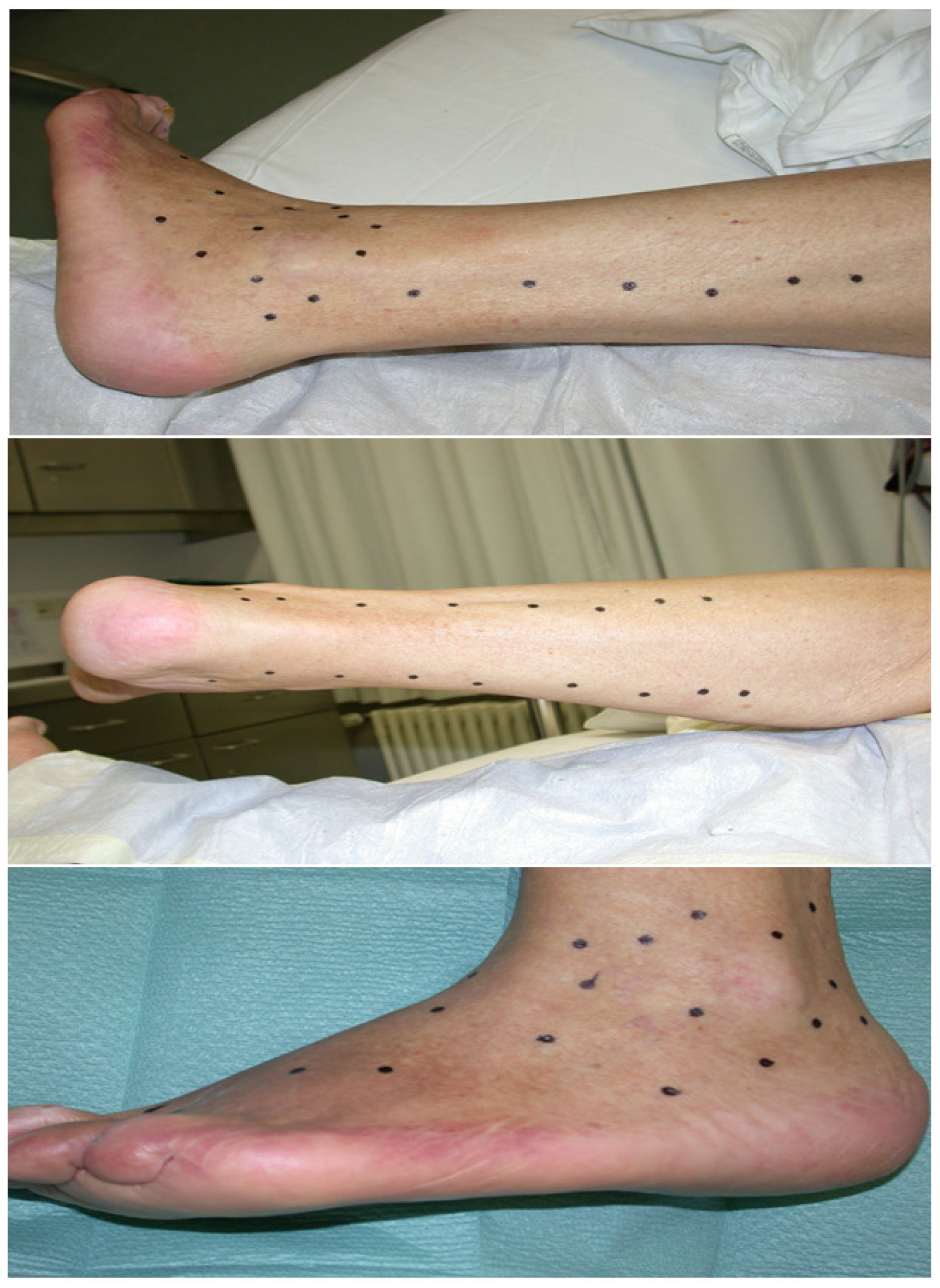
2.6. Application of Chitosan-Based Biomaterial Combined with Autologous Human Fibroblasts and Bone Marrow-Derived MSC for Treatment of Diabetic Foot Ulcer
3. Discussion
4. Materials and Methods
4.1. Isolation of MSC from Bone Marrow
4.2. Cell Passaging Procedures
4.3. CD Characterization of Bone Marrow MSC
4.4. Multilineage Potential
4.5. Isolation of Dermal Fibroblasts
4.6. Immunocytochemistry Characterization of Canine Skin Fibroblasts
4.7. Preparation of Biopolymer Scaffolds
4.7.1. Characterization of Porosity, Average Molecular Weight of Biopolymers in Scaffold, FTIR Analysis of Composites
4.7.2. In Vitro Cytotoxicity Testing
4.8. Application of Chitosan-Based Biomaterial Combined with Autologous Human Fibroblasts and Bone Marrow-Derived MSC for Treatment of Diabetic Foot Ulcer
5. Conclusions
- In the present study, we successfully isolated mesenchymal stem cells from the bone marrow. The yield of isolated cells was 17.9 × 106 cells/mL. hBM-MSC showed a high expression of CD29 (99.1 ± 0.4%), CD44 (99.8 ± 0.2%), CD90 (98.0 ± 0.6%) and low expression of CD34 (0.8 ± 0.2%) and CD45 (0.3 ± 0.1%).
- We were also able to isolate and cultivate a cell culture of dermal fibroblasts. The yield of isolated cells was 1.5 × 106 cells/mL. Cells from the cultivated population showed a spindle shape and 85–95 µm in size and, according to the results of immunocytochemistry staining, showed positivity for vimentin, collagen I and collagen III.
- We observed pain relief after the intramuscular application of autologous hBM-MSC, enhancement of healing process activation, formation of blood vessels and almost complete healing of the defect after skin graft transplantation and 8 months of therapy.
- The success of the treatment in this case can be explained by the synergistic positive healing effect of both the used material and the cell components, as fibroblasts and MSC show significant immunomodulating and paracrine potential, which plays an important role in the wound-healing process. In the same way, chitosan-based biomaterials are also used in the healing process of refractory wounds, which directly affects the hemostatic, proliferative and immunomodulating phase [52,54,57].
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raja, J.M.; Maturana, M.A.; Kayali, S.; Khouzam, A.; Efeovbokhan, N. Diabetic Foot Ulcer: A Comprehensive Review of Pathophysiology and Management Modalities. World J. Clin. Cases 2023, 11, 1684. [Google Scholar] [CrossRef] [PubMed]
- Rinkel, W.D.; Luiten, J.; van Dongen, J.; Kuppens, B.; Van Neck, J.W.; Polinder, S.; Castro Cabezas, M.; Coert, J.H. In-Hospital Costs of Diabetic Foot Disease Treated by a Multidisciplinary Foot Team. Diabetes Res. Clin. Pract. 2017, 132, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Maida, C.; Pinto, A. Diabetic Foot Syndrome: Immune-Inflammatory Features as Possible Cardiovascular Markers in Diabetes. World J. Orthop. 2015, 6, 62–76. [Google Scholar] [CrossRef] [PubMed]
- Volmer-Thole, M.; Lobmann, R. Neuropathy and Diabetic Foot Syndrome. Int. J. Mol. Sci. 2016, 17, 917. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wei, J.; Lu, S. Association between Diabetic Retinopathy and Diabetic Foot Ulcer in Patients with Diabetes: A Meta-analysis. Int. Wound J. 2023, 20, 4077–4082. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wen, S.; Dong, M.; Yuan, Y.; Gong, M.; Wang, C.; Yuan, X.; Jin, J.; Zhou, M.; Zhou, L. The Metabolic Characteristics of Patients at the Risk for Diabetic Foot Ulcer: A Comparative Study of Diabetic Patients with and without Diabetic Foot. DMSO 2023, 16, 3197–3211. [Google Scholar] [CrossRef] [PubMed]
- Aldana, P.C.; Khachemoune, A. Diabetic Foot Ulcers: Appraising Standard of Care and Reviewing New Trends in Management. Am. J. Clin. Dermatol. 2020, 21, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Platonoff, A.; Florida Mejía-Mendoza, M.D.; Ibáñez-Doria, M.; Contreras-Ruiz, J. The gold standard in diabetic foot treatment: Total contact cast. Gac. Med. Mex. 2014, 150, 58–64. [Google Scholar] [PubMed]
- Borys, S.; Hohendorff, J.; Frankfurter, C.; Kiec-Wilk, B.; Malecki, M.T. Negative Pressure Wound Therapy Use in Diabetic Foot Syndrome-from Mechanisms of Action to Clinical Practice. Eur. J. Clin. Investig. 2019, 49, e13067. [Google Scholar] [CrossRef]
- Voza, F.A.; Huerta, C.T.; Le, N.; Shao, H.; Ribieras, A.; Ortiz, Y.; Atkinson, C.; Machuca, T.; Liu, Z.-J.; Velazquez, O.C. Fibroblasts in Diabetic Foot Ulcers. Int. J. Mol. Sci. 2024, 25, 2172. [Google Scholar] [CrossRef]
- El Hage, R.; Knippschild, U.; Arnold, T.; Hinterseher, I. Stem Cell-Based Therapy: A Promising Treatment for Diabetic Foot Ulcer. Biomedicines 2022, 10, 1507. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, K.; Sivaramakrishnan, G. Growth Factors for Diabetic Foot Ulcers: Mixed Treatment Comparison Analysis of Randomized Clinical Trials. Br. J. Clin. Pharmacol. 2018, 84, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Schmiedova, I.; Dembickaja, A.; Kiselakova, L.; Nowakova, B.; Slama, P. Using of Amniotic Membrane Derivatives for the Treatment of Chronic Wounds. Membranes 2021, 11, 941. [Google Scholar] [CrossRef] [PubMed]
- Bainbridge, P. Wound Healing and the Role of Fibroblasts. J. Wound Care 2013, 22, 407–408, 410–412. [Google Scholar] [CrossRef] [PubMed]
- Guillamat-Prats, R. The Role of MSC in Wound Healing, Scarring and Regeneration. Cells 2021, 10, 1729. [Google Scholar] [CrossRef]
- Hu, M.S.; Borrelli, M.R.; Lorenz, H.P.; Longaker, M.T.; Wan, D.C. Mesenchymal Stromal Cells and Cutaneous Wound Healing: A Comprehensive Review of the Background, Role, and Therapeutic Potential. Stem Cells Int. 2018, 2018, e6901983. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Cao, L.; Melino, S.; Candi, E.; Wang, Y.; Shao, C.; Melino, G.; Shi, Y.; Chen, X. Orchestration of Mesenchymal Stem/Stromal Cells and Inflammation During Wound Healing. Stem Cells Transl. Med. 2023, 12, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Heydari, M.B.; Ghanbari-Movahed, Z.; Heydari, M.; Farzaei, M.H. In Vitro Study of the Mesenchymal Stem Cells-Conditional Media Role in Skin Wound Healing Process: A Systematic Review. Int. Wound J. 2022, 19, 2210–2223. [Google Scholar] [CrossRef]
- Maxson, S.; Lopez, E.A.; Yoo, D.; Danilkovitch-Miagkova, A.; LeRoux, M.A. Concise Review: Role of Mesenchymal Stem Cells in Wound Repair. Stem Cells Transl. Med. 2012, 1, 142–149. [Google Scholar] [CrossRef]
- Landén, N.X.; Li, D.; Ståhle, M. Transition from Inflammation to Proliferation: A Critical Step during Wound Healing. Cell Mol. Life Sci. 2016, 73, 3861–3885. [Google Scholar] [CrossRef]
- Farabi, B.; Roster, K.; Hirani, R.; Tepper, K.; Atak, M.F.; Safai, B. The Efficacy of Stem Cells in Wound Healing: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 3006. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Ogino, R.; Yamakawa, S.; Suda, S.; Hayashida, K. Role and Function of Mesenchymal Stem Cells on Fibroblast in Cutaneous Wound Healing. Biomedicines 2022, 10, 1391. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Guarino, M.; Hernández-Bule, M.L.; Bacci, S. Cellular and Molecular Processes in Wound Healing. Biomedicines 2023, 11, 2526. [Google Scholar] [CrossRef] [PubMed]
- Sathyaraj, W.V.; Prabakaran, L.; Bhoopathy, J.; Dharmalingam, S.; Karthikeyan, R.; Atchudan, R. Therapeutic Efficacy of Polymeric Biomaterials in Treating Diabetic Wounds—An Upcoming Wound Healing Technology. Polymers 2023, 15, 1205. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Zharkinbekov, Z.; Raziyeva, K.; Tabyldiyeva, L.; Berikova, K.; Zhumagul, D.; Temirkhanova, K.; Saparov, A. Chitosan-Based Biomaterials for Tissue Regeneration. Pharmaceutics 2023, 15, 807. [Google Scholar] [CrossRef] [PubMed]
- Olmo, J.; Alonso, J.; Saez, V.; Benito Cid, S.; Moreno, I.; Larrauri, M.; González, R.; Vilas, J.; Perez, L. Self-Healing, Antibacterial and Anti-Inflammatory Chitosan-PEG Hydrogels for Ulcerated Skin Wound Healing and Drug Delivery. Biomater. Adv. 2022, 139, 212992. [Google Scholar] [CrossRef]
- Rajkumar, D.S.R.; Keerthika, K.; Vijayaragavan, V. Chitosan-Based Biomaterial in Wound Healing: A Review. Cureus 2024, 16, e55193. [Google Scholar] [CrossRef]
- Apte, A.; Liechty, K.W.; Zgheib, C. Immunomodulatory Biomaterials on Chemokine Signaling in Wound Healing. Front. Pharmacol. 2023, 14, 1084948. [Google Scholar] [CrossRef] [PubMed]
- Humenik, F.; Maloveská, M.; Hudáková, N.; Petroušková, P.; Šufliarska, Z.; Horňáková, Ľ.; Valenčáková, A.; Kožár, M.; Šišková, B.; Mudroňová, D.; et al. Impact of Canine Amniotic Mesenchymal Stem Cell Conditioned Media on the Wound Healing Process: In Vitro and In Vivo Study. Int. J. Mol. Sci. 2023, 24, 8214. [Google Scholar] [CrossRef]
- Humenik, F.; Danko, J.; Krešáková, L.; Vdoviaková, K.; Vrabec, V.; Vasilová, E.; Giretová, M.; Tóth, Š.; Fagová, Z.; Babík, J.; et al. A Chitosan-Based Biomaterial Combined with Mesenchymal Stem Cell-Conditioned Medium for Wound Healing and Skin Regeneration. Int. J. Mol. Sci. 2023, 24, 16080. [Google Scholar] [CrossRef]
- Lee, J.; Yang, K.-H.; Joe, C.O.; Kang, S.-S. Formation of Distinct Inclusion Bodies by Inhibition of Ubiquitin-Proteasome and Autophagy-Lysosome Pathways. Biochem. Biophys. Res. Commun. 2011, 404, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Ravikanth, M.; Soujanya, P.; Manjunath, K.; Saraswathi, T.; Ramachandran, C. Heterogenecity of Fibroblasts. J. Oral. Maxillofac. Pathol. 2011, 15, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Vasiliadis, A.V.; Galanis, N. Human Bone Marrow-Derived Mesenchymal Stem Cells from Different Bone Sources: A Panorama. Stem Cell Investig. 2020, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Kannan, S.; Gokul Krishna, S.; Gupta, P.K.; Kolkundkar, U.K. Advantages of Pooling of Human Bone Marrow-Derived Mesenchymal Stromal Cells from Different Donors versus Single-Donor MSCs. Sci. Rep. 2024, 14, 12654. [Google Scholar] [CrossRef] [PubMed]
- Davies, O.G.; Cooper, P.R.; Shelton, R.M.; Smith, A.J.; Scheven, B.A. Isolation of Adipose and Bone Marrow Mesenchymal Stem Cells Using CD29 and CD90 Modifies Their Capacity for Osteogenic and Adipogenic Differentiation. J. Tissue Eng. 2015, 6, 2041731415592356. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, Y.-Q.; Wang, A.-T.; Yu, C.-Y.; Luo, Y.; Liu, R.-M.; Zhao, Y.-J.; Xiao, J.-H. Effect of CD44 on Differentiation of Human Amniotic Mesenchymal Stem Cells into Chondrocytes via Smad and ERK Signaling Pathways. Mol. Med. Rep. 2020, 21, 2357–2366. [Google Scholar] [CrossRef] [PubMed]
- Pérez, L.A.; León, J.; López, J.; Rojas, D.; Reyes, M.; Contreras, P.; Quest, A.F.G.; Escudero, C.; Leyton, L. The GPI-Anchored Protein Thy-1/CD90 Promotes Wound Healing upon Injury to the Skin by Enhancing Skin Perfusion. Int. J. Mol. Sci. 2022, 23, 12539. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhao, L.; Terry, P.D.; Chen, J. Reciprocal Effect of Environmental Stimuli to Regulate the Adipogenesis and Osteogenesis Fate Decision in Bone Marrow-Derived Mesenchymal Stem Cells (BM-MSCs). Cells 2023, 12, 1400. [Google Scholar] [CrossRef]
- Li, C.; Wu, X.; Tong, J.; Yang, X.; Zhao, J.; Zheng, Q.; Zhao, G.; Ma, Z. Comparative Analysis of Human Mesenchymal Stem Cells from Bone Marrow and Adipose Tissue under Xeno-Free Conditions for Cell Therapy. Stem Cell Res. Ther. 2015, 6, 55. [Google Scholar] [CrossRef]
- Chen, Q.; Shou, P.; Zheng, C.; Jiang, M.; Cao, G.; Yang, Q.; Cao, J.; Xie, N.; Velletri, T.; Zhang, X.; et al. Fate Decision of Mesenchymal Stem Cells: Adipocytes or Osteoblasts? Cell Death Differ. 2016, 23, 1128–1139. [Google Scholar] [CrossRef]
- Tencerova, M.; Kassem, M. The Bone Marrow-Derived Stromal Cells: Commitment and Regulation of Adipogenesis. Front. Endocrinol. 2016, 7, 127. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.A. Is Adipocyte Differentiation the Default Lineage for Mesenchymal Stem/Progenitor Cells after Loss of Mechanical Loading? A Perspective from Space Flight and Model Systems. J. Biomed. Sci. Eng. 2014, 7, 799–808. [Google Scholar] [CrossRef]
- Sanchez-Castro, E.; Pajuelo-Reyes, C.; Tejedo Cahuana, R.; Soria-Juan, B.; Tapia-Limonchi, R.; Andreu, E.; Hitos, A.; Martín, F.; Cahuana, G.; Guerra-Duarte, C.; et al. Mesenchymal Stromal Cell-Based Therapies as Promising Treatments for Muscle Regeneration After Snakebite Envenoming. Front. Immunol. 2021, 11, 609961. [Google Scholar] [CrossRef] [PubMed]
- Ezquerra, S.; Zuleta, A.; Arancibia, R.; Estay, J.; Aulestia, F.; Carrion, F. Functional Properties of Human-Derived Mesenchymal Stem Cell Spheroids: A Meta-Analysis and Systematic Review. Stem Cells Int. 2021, 2021, 8825332. [Google Scholar] [CrossRef] [PubMed]
- Romanov, Y.A.; Svintsitskaya, V.A.; Smirnov, V.N. Searching for Alternative Sources of Postnatal Human Mesenchymal Stem Cells: Candidate MSC-Like Cells from Umbilical Cord. Stem Cells 2003, 21, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.-Z.; Su, W.-R.; Shi, S.-H.; Wilder-Smith, P.; Xiang, A.P.; Wong, A.; Nguyen, A.L.; Kwon, C.W.; Le, A.D. Human Gingiva-Derived Mesenchymal Stem Cells Elicit Polarization of M2 Macrophages and Enhance Cutaneous Wound Healing. Stem Cells 2010, 28, 1856–1868. [Google Scholar] [CrossRef]
- Taufiq, H.; Shaik Fakiruddin, K.; Muzaffar, U.; Lim, M.N.; Rusli, S.; Kamaluddin, N.R.; Esa, E.; Abdullah, S. Systematic Review and Meta-Analysis of Mesenchymal Stromal/Stem Cells as Strategical Means for the Treatment of COVID-19. Ther. Adv. Respir. Dis. 2023, 17, 17534666231158276. [Google Scholar] [CrossRef]
- Manoharan, R.; Kore, R.A.; Mehta, J.L. Mesenchymal Stem Cell Treatment for Hyperactive Immune Response in Patients with COVID-19. Immunotherapy 2022, 14, 1055–1065. [Google Scholar] [CrossRef]
- Adas, G.; Cukurova, Z.; Yasar, K.K.; Yilmaz, R.; Isiksacan, N.; Kasapoglu, P.; Yesilbag, Z.; Koyuncu, I.; Karaoz, E. The Systematic Effect of Mesenchymal Stem Cell Therapy in Critical COVID-19 Patients: A Prospective Double Controlled Trial. Cell Transpl. 2021, 30, 09636897211024942. [Google Scholar] [CrossRef]
- Sliogeryte, K.; Gavara, N. Vimentin Plays a Crucial Role in Fibroblast Ageing by Regulating Biophysical Properties and Cell Migration. Cells 2019, 8, 1164. [Google Scholar] [CrossRef]
- Nissen, N.I.; Johansen, A.Z.; Chen, I.; Johansen, J.S.; Pedersen, R.S.; Hansen, C.P.; Karsdal, M.A.; Willumsen, N. Collagen Biomarkers Quantify Fibroblast Activity In Vitro and Predict Survival in Patients with Pancreatic Ductal Adenocarcinoma. Cancers 2022, 14, 819. [Google Scholar] [CrossRef] [PubMed]
- Correa-Gallegos, D.; Jiang, D.; Rinkevich, Y. Fibroblasts as Confederates of the Immune System. Immunol. Rev. 2021, 302, 147–162. [Google Scholar] [CrossRef] [PubMed]
- Bautista-Hernández, L.A.; Gómez-Olivares, J.L.; Buentello-Volante, B.; Bautista-de Lucio, V.M. Fibroblasts: The Unknown Sentinels Eliciting Immune Responses Against Microorganisms. Eur. J. Microbiol. Immunol. 2017, 7, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Sadik, A.O.E.; Ghamrawy, T.A.E.; El-Galil, T.I.A. The Effect of Mesenchymal Stem Cells and Chitosan Gel on Full Thickness Skin Wound Healing in Albino Rats: Histological, Immunohistochemical and Fluorescent Study. PLoS ONE 2015, 10, e0137544. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Chen, S.; Zhang, C.; Han, J.; Lin, C.; Zhao, X.; Guo, H.; Tan, Y. Enhanced Therapeutic Effects of Mesenchymal Stem Cell-Derived Extracellular Vesicles within Chitosan Hydrogel in the Treatment of Diabetic Foot Ulcers. J. Mater. Sci. Mater. Med. 2023, 34, 43. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.-X.; Zhao, W.-Y.; Fang, Q.-Q.; Wang, X.-F.; Chen, C.-Y.; Shi, B.-H.; Zheng, B.; Wang, S.-J.; Tan, W.-Q.; Wu, L.-H. Effects of Chitosan-Collagen Dressing on Wound Healing in Vitro and in Vivo Assays. J. Appl. Biomater. Funct. Mater. 2021, 19, 2280800021989698. [Google Scholar] [CrossRef] [PubMed]
- Pusateri, A.E.; McCarthy, S.J.; Gregory, K.W.; Harris, R.A.; Cardenas, L.; McManus, A.T.; Goodwin, C.W. Effect of a Chitosan-Based Hemostatic Dressing on Blood Loss and Survival in a Model of Severe Venous Hemorrhage and Hepatic Injury in Swine. J. Trauma. 2003, 54, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Matica, M.A.; Aachmann, F.L.; Tøndervik, A.; Sletta, H.; Ostafe, V. Chitosan as a Wound Dressing Starting Material: Antimicrobial Properties and Mode of Action. Int. J. Mol. Sci. 2019, 20, 5889. [Google Scholar] [CrossRef]
- Gonzalez, A.C.d.O.; Costa, T.F.; Andrade, Z.d.A.; Medrado, A.R.A.P. Wound Healing—A Literature Review. An. Bras. Dermatol. 2016, 91, 614–620. [Google Scholar] [CrossRef]
- Liu, H.; Wang, C.; Li, C.; Qin, Y.; Wang, Z.; Yang, F.; Li, Z.; Wang, J. A Functional Chitosan-Based Hydrogel as a Wound Dressing and Drug Delivery System in the Treatment of Wound Healing. RSC Adv. 2018, 8, 7533–7549. [Google Scholar] [CrossRef]
- Escárcega-Galaz, A.A.; Cruz-Mercado, J.L.D.L.; López-Cervantes, J.; Sánchez-Machado, D.I.; Brito-Zurita, O.R.; Ornelas-Aguirre, J.M. Chitosan Treatment for Skin Ulcers Associated with Diabetes. Saudi J. Biol. Sci. 2018, 25, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Velazco, G.; Gonzalez, A.; Ortiz, R. Apósitos de quitosano para el tratamiento de pie diabético (Chitosan films for the diabetic foot treatment). Av. Biomed. 2012, 1, 38–41. [Google Scholar]
- Padda, J.; Khalid, K.; Zubair, U.; Al Hennawi, H.; Yadav, J.; Almanie, A.H.; Mehta, K.A.; Tasnim, F.; Cooper, A.C.; Jean-Charles, G. Stem Cell Therapy and Its Significance in Pain Management. Cureus 2021, 13, e17258. [Google Scholar] [CrossRef] [PubMed]
- Almahasneh, F.; Abu-El-Rub, E.; Khasawneh, R.R. Mechanisms of Analgesic Effect of Mesenchymal Stem Cells in Osteoarthritis Pain. World J. Stem Cells 2023, 15, 196–208. [Google Scholar] [CrossRef]












Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Humenik, F.; Vdoviaková, K.; Krešáková, L.; Danko, J.; Giretová, M.; Medvecký, Ľ.; Lengyel, P.; Babík, J. The Combination of Chitosan-Based Biomaterial and Cellular Therapy for Successful Treatment of Diabetic Foot—Pilot Study. Int. J. Mol. Sci. 2024, 25, 8388. https://doi.org/10.3390/ijms25158388
Humenik F, Vdoviaková K, Krešáková L, Danko J, Giretová M, Medvecký Ľ, Lengyel P, Babík J. The Combination of Chitosan-Based Biomaterial and Cellular Therapy for Successful Treatment of Diabetic Foot—Pilot Study. International Journal of Molecular Sciences. 2024; 25(15):8388. https://doi.org/10.3390/ijms25158388
Chicago/Turabian StyleHumenik, Filip, Katarína Vdoviaková, Lenka Krešáková, Ján Danko, Mária Giretová, Ľubomír Medvecký, Peter Lengyel, and Ján Babík. 2024. "The Combination of Chitosan-Based Biomaterial and Cellular Therapy for Successful Treatment of Diabetic Foot—Pilot Study" International Journal of Molecular Sciences 25, no. 15: 8388. https://doi.org/10.3390/ijms25158388