
Exploring the Relationship of rs2802292 with Diabetes and NAFLD in a Southern Italian Cohort—Nutrihep Study
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
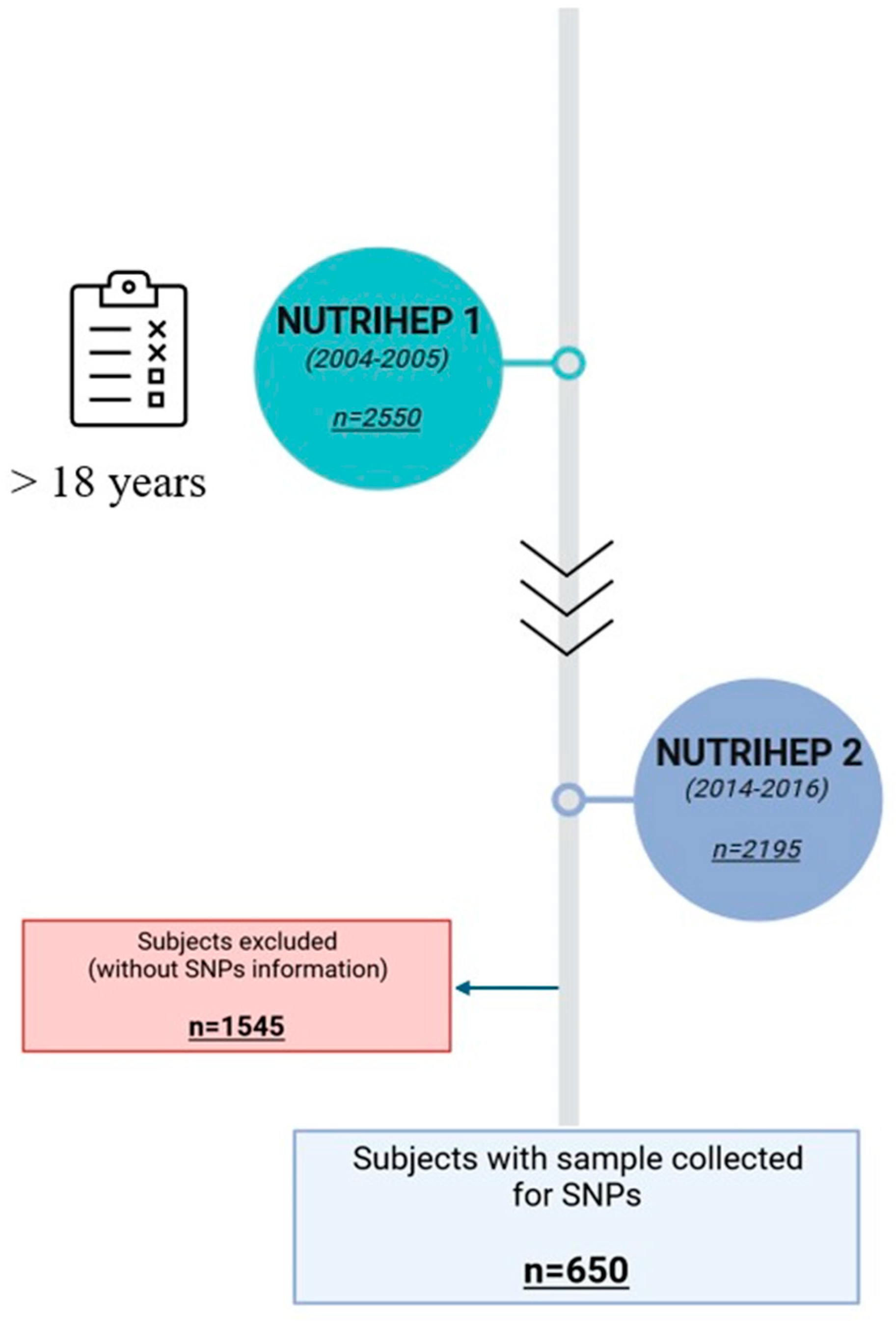
4.1. Study Population
4.2. Lifestyle, Clinical, and Dietary Assessment
4.3. DNA Extraction and TaqMan PCR Assay
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Genetics of Healthy Aging and Longevity—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/23925498/ (accessed on 19 June 2024).
- Genetic Factors Associated with Longevity: A Review of Recent Findings—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/25446805/ (accessed on 19 June 2024).
- The Metabolic Syndrome: Is This Diagnosis Necessary?—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/16762930/ (accessed on 19 June 2024).
- Papatheodorou, I.; Petrovs, R.; Thornton, J.M. Comparison of the Mammalian Insulin Signalling Pathway to Invertebrates in the Context of FOXO-Mediated Ageing. Bioinformatics 2014, 30, 2999–3003. [Google Scholar] [CrossRef]
- Dijkers, P.F.; Medema, R.H.; Pals, C.; Banerji, L.; Thomas, N.S.; Lam, E.W.; Burgering, B.M.; Raaijmakers, J.A.; Lammers, J.W.; Koenderman, L.; et al. Forkhead Transcription Factor FKHR-L1 Modulates Cytokine-Dependent Transcriptional Regulation of P27(KIP1). Mol. Cell Biol. 2000, 20, 9138–9148. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.; Brunet, A.; Grenier, J.M.; Datta, S.R.; Fornace, A.J.; DiStefano, P.S.; Chiang, L.W.; Greenberg, M.E. DNA Repair Pathway Stimulated by the Forkhead Transcription Factor FOXO3a through the Gadd45 Protein. Science 2002, 296, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Ogg, S.; Paradis, S.; Gottlieb, S.; Patterson, G.I.; Lee, L.; Tissenbaum, H.A.; Ruvkun, G. The Fork Head Transcription Factor DAF-16 Transduces Insulin-like Metabolic and Longevity Signals in C. elegans. Nature 1997, 389, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Kops, G.J.P.L.; Dansen, T.B.; Polderman, P.E.; Saarloos, I.; Wirtz, K.W.A.; Coffer, P.J.; Huang, T.-T.; Bos, J.L.; Medema, R.H.; Burgering, B.M.T. Forkhead Transcription Factor FOXO3a Protects Quiescent Cells from Oxidative Stress. Nature 2002, 419, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Brunet, A.; Bonni, A.; Zigmond, M.J.; Lin, M.Z.; Juo, P.; Hu, L.S.; Anderson, M.J.; Arden, K.C.; Blenis, J.; Greenberg, M.E. Akt Promotes Cell Survival by Phosphorylating and Inhibiting a Forkhead Transcription Factor. Cell 1999, 96, 857–868. [Google Scholar] [CrossRef]
- Willcox, B.J.; Donlon, T.A.; He, Q.; Chen, R.; Grove, J.S.; Yano, K.; Masaki, K.H.; Willcox, D.C.; Rodriguez, B.; Curb, J.D. FOXO3A Genotype Is Strongly Associated with Human Longevity. Proc. Natl. Acad. Sci. USA 2008, 105, 13987–13992. [Google Scholar] [CrossRef]
- Eijkelenboom, A.; Burgering, B.M.T. FOXOs: Signalling Integrators for Homeostasis Maintenance. Nat. Rev. Mol. Cell Biol. 2013, 14, 83–97. [Google Scholar] [CrossRef]
- Bao, J.-M.; Song, X.-L.; Hong, Y.-Q.; Zhu, H.-L.; Li, C.; Zhang, T.; Chen, W.; Zhao, S.-C.; Chen, Q. Association between FOXO3A Gene Polymorphisms and Human Longevity: A Meta-Analysis. Asian J. Androl. 2014, 16, 446–452. [Google Scholar] [CrossRef]
- Willcox, B.J.; Tranah, G.J.; Chen, R.; Morris, B.J.; Masaki, K.H.; He, Q.; Willcox, D.C.; Allsopp, R.C.; Moisyadi, S.; Poon, L.W.; et al. The FoxO3 Gene and Cause-Specific Mortality. Aging Cell 2016, 15, 617–624. [Google Scholar] [CrossRef]
- Forte, G.; Grossi, V.; Celestini, V.; Lucisano, G.; Scardapane, M.; Varvara, D.; Patruno, M.; Bagnulo, R.; Loconte, D.; Giunti, L.; et al. Characterization of the Rs2802292 SNP Identifies FOXO3A as a Modifier Locus Predicting Cancer Risk in Patients with PJS and PHTS Hamartomatous Polyposis Syndromes. BMC Cancer 2014, 14, 661. [Google Scholar] [CrossRef]
- Grossi, V.; Forte, G.; Sanese, P.; Peserico, A.; Tezil, T.; Lepore Signorile, M.; Fasano, C.; Lovaglio, R.; Bagnulo, R.; Loconte, D.C.; et al. The Longevity SNP Rs2802292 Uncovered: HSF1 Activates Stress-Dependent Expression of FOXO3 through an Intronic Enhancer. Nucleic Acids Res. 2018, 46, 5587–5600. [Google Scholar] [CrossRef]
- Banasik, K.; Ribel-Madsen, R.; Gjesing, A.P.; Wegner, L.; Andersson, A.; Poulsen, P.; Borglykke, A.; Witte, D.R.; Pedersen, O.; Hansen, T.; et al. The FOXO3A Rs2802292 G-Allele Associates with Improved Peripheral and Hepatic Insulin Sensitivity and Increased Skeletal Muscle-FOXO3A mRNA Expression in Twins. J. Clin. Endocrinol. Metab. 2011, 96, E119–E124. [Google Scholar] [CrossRef]
- Dissecting Long-Term Glucose Metabolism Identifies New Susceptibility Period for Metabolic Dysfunction in Aged Mice—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26540285/ (accessed on 20 June 2024).
- Ruze, R.; Liu, T.; Zou, X.; Song, J.; Chen, Y.; Xu, R.; Yin, X.; Xu, Q. Obesity and Type 2 Diabetes Mellitus: Connections in Epidemiology, Pathogenesis, and Treatments. Front. Endocrinol. 2023, 14, 1161521. [Google Scholar] [CrossRef]
- Angulo, P.; Keach, J.C.; Batts, K.P.; Lindor, K.D. Independent Predictors of Liver Fibrosis in Patients with Nonalcoholic Steatohepatitis. Hepatology 1999, 30, 1356–1362. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Tran, T.; Everhart, J.E. Diabetes Increases the Risk of Chronic Liver Disease and Hepatocellular Carcinoma. Gastroenterology 2004, 126, 460–468. [Google Scholar] [CrossRef]
- Bril, F.; Cusi, K. Management of Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: A Call to Action. Diabetes Care 2017, 40, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Wild, S.H.; Morling, J.R.; McAllister, D.A.; Kerssens, J.; Fischbacher, C.; Parkes, J.; Roderick, P.J.; Sattar, N.; Byrne, C.D.; Scottish and Southampton Diabetes and Liver Disease Group; et al. Type 2 Diabetes and Risk of Hospital Admission or Death for Chronic Liver Diseases. J. Hepatol. 2016, 64, 1358–1364. [Google Scholar] [CrossRef] [PubMed]
- Baffy, G.; Brunt, E.M.; Caldwell, S.H. Hepatocellular Carcinoma in Non-Alcoholic Fatty Liver Disease: An Emerging Menace. J. Hepatol. 2012, 56, 1384–1391. [Google Scholar] [CrossRef] [PubMed]
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to Diabetes Mellitus, Cardiovascular Disease or Cirrhosis. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 330–344. [Google Scholar] [CrossRef]
- Ramaswamy, S.; Nakamura, N.; Sansal, I.; Bergeron, L.; Sellers, W.R. A Novel Mechanism of Gene Regulation and Tumor Suppression by the Transcription Factor FKHR. Cancer Cell 2002, 2, 81–91. [Google Scholar] [CrossRef]
- Fernández de Mattos, S.; Essafi, A.; Soeiro, I.; Pietersen, A.M.; Birkenkamp, K.U.; Edwards, C.S.; Martino, A.; Nelson, B.H.; Francis, J.M.; Jones, M.C.; et al. FoxO3a and BCR-ABL Regulate Cyclin D2 Transcription through a STAT5/BCL6-Dependent Mechanism. Mol. Cell. Biol. 2004, 24, 10058–10071. [Google Scholar] [CrossRef] [PubMed]
- Seoane, J.; Le, H.-V.; Shen, L.; Anderson, S.A.; Massagué, J. Integration of Smad and Forkhead Pathways in the Control of Neuroepithelial and Glioblastoma Cell Proliferation. Cell 2004, 117, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Medema, R.H.; Kops, G.J.; Bos, J.L.; Burgering, B.M. AFX-like Forkhead Transcription Factors Mediate Cell-Cycle Regulation by Ras and PKB through P27kip1. Nature 2000, 404, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Jensen, K.S.; Binderup, T.; Jensen, K.T.; Therkelsen, I.; Borup, R.; Nilsson, E.; Multhaupt, H.; Bouchard, C.; Quistorff, B.; Kjaer, A.; et al. FoxO3A Promotes Metabolic Adaptation to Hypoxia by Antagonizing Myc Function. EMBO J. 2011, 30, 4554–4570. [Google Scholar] [CrossRef]
- Bouchard, C.; Marquardt, J.; Brás, A.; Medema, R.H.; Eilers, M. Myc-Induced Proliferation and Transformation Require Akt-Mediated Phosphorylation of FoxO Proteins. EMBO J. 2004, 23, 2830–2840. [Google Scholar] [CrossRef]
- Furukawa-Hibi, Y.; Yoshida-Araki, K.; Ohta, T.; Ikeda, K.; Motoyama, N. FOXO Forkhead Transcription Factors Induce G(2)-M Checkpoint in Response to Oxidative Stress. J. Biol. Chem. 2002, 277, 26729–26732. [Google Scholar] [CrossRef]
- Flachsbart, F.; Caliebe, A.; Kleindorp, R.; Blanché, H.; von Eller-Eberstein, H.; Nikolaus, S.; Schreiber, S.; Nebel, A. Association of FOXO3A Variation with Human Longevity Confirmed in German Centenarians. Proc. Natl. Acad. Sci. USA 2009, 106, 2700–2705. [Google Scholar] [CrossRef]
- Anselmi, C.V.; Malovini, A.; Roncarati, R.; Novelli, V.; Villa, F.; Condorelli, G.; Bellazzi, R.; Puca, A.A. Association of the FOXO3A Locus with Extreme Longevity in a Southern Italian Centenarian Study. Rejuvenation Res. 2009, 12, 95–104. [Google Scholar] [CrossRef]
- Donlon, T.A.; Morris, B.J.; Chen, R.; Masaki, K.H.; Allsopp, R.C.; Willcox, D.C.; Elliott, A.; Willcox, B.J. FOXO3 Longevity Interactome on Chromosome 6. Aging Cell 2017, 16, 1016–1025. [Google Scholar] [CrossRef]
- Flachsbart, F.; Dose, J.; Gentschew, L.; Geismann, C.; Caliebe, A.; Knecht, C.; Nygaard, M.; Badarinarayan, N.; ElSharawy, A.; May, S.; et al. Identification and Characterization of Two Functional Variants in the Human Longevity Gene FOXO3. Nat. Commun. 2017, 8, 2063. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, C.; Chang, J.; Gensch, E.; Rudner, A.; Tabtiang, R. A C. elegans Mutant That Lives Twice as Long as Wild Type. Nature 1993, 366, 461–464. [Google Scholar] [CrossRef]
- Willcox, B.J.; Morris, B.J.; Tranah, G.J.; Chen, R.; Masaki, K.H.; He, Q.; Willcox, D.C.; Allsopp, R.C.; Moisyadi, S.; Gerschenson, M.; et al. Longevity-Associated FOXO3 Genotype and Its Impact on Coronary Artery Disease Mortality in Japanese, Whites, and Blacks: A Prospective Study of Three American Populations. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 724–728. [Google Scholar] [CrossRef]
- Klinpudtan, N.; Allsopp, R.C.; Kabayama, M.; Godai, K.; Gondo, Y.; Masui, Y.; Akagi, Y.; Srithumsuk, W.; Sugimoto, K.; Akasaka, H.; et al. The Association between Longevity-Associated FOXO3 Allele and Heart Disease in Septuagenarians and Octogenarians: The SONIC Study. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 1542–1548. [Google Scholar] [CrossRef] [PubMed]
- Morris, B.J.; Chen, R.; Donlon, T.A.; Evans, D.S.; Tranah, G.J.; Parimi, N.; Ehret, G.B.; Newton-Cheh, C.; Seto, T.; Willcox, D.C.; et al. Association Analysis of FOXO3 Longevity Variants with Blood Pressure and Essential Hypertension. Am. J. Hypertens. 2016, 29, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Morris, B.J.; Donlon, T.A.; Ross, G.W.; Kallianpur, K.J.; Allsopp, R.C.; Nakagawa, K.; Willcox, B.J.; Masaki, K.H. Incidence of Alzheimer’s Disease in Men with Late-Life Hypertension Is Ameliorated by FOXO3 Longevity Genotype. J. Alzheimers Dis. 2023, 95, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Chen, R.; Greenberg, S.M.; Ross, G.W.; Willcox, B.J.; Donlon, T.A.; Allsopp, R.C.; Willcox, D.C.; Morris, B.J.; Masaki, K.H. Forkhead Box O3 Longevity Genotype May Attenuate the Impact of Hypertension on Risk of Intracerebral Haemorrhage. J. Hypertens. 2022, 40, 2230–2235. [Google Scholar] [CrossRef]
- Sun, L.; Hu, C.; Qian, Y.; Zheng, C.; Liang, Q.; Lv, Z.; Huang, Z.; Qi, K.; Huang, J.; Zhou, Q.; et al. Age-Based Differences in the Genetic Determinants of Glycemic Control: A Case of FOXO3 Variations. PLoS ONE 2015, 10, e0126696. [Google Scholar] [CrossRef]
- Mao, Y.-Q.; Liu, J.-F.; Han, B.; Wang, L.-S. Longevity-Associated Forkhead Box O3 (FOXO3) Single Nucleotide Polymorphisms Are Associated with Type 2 Diabetes Mellitus in Chinese Elderly Women. Med. Sci. Monit. 2019, 25, 2966–2975. [Google Scholar] [CrossRef]
- Ma, W.-T.; Gao, F.; Gu, K.; Chen, D.-K. The Role of Monocytes and Macrophages in Autoimmune Diseases: A Comprehensive Review. Front. Immunol. 2019, 10, 1140. [Google Scholar] [CrossRef]
- Pant, T.; Lin, C.-W.; Bedrat, A.; Jia, S.; Roethle, M.F.; Truchan, N.A.; Ciecko, A.E.; Chen, Y.-G.; Hessner, M.J. Monocytes in Type 1 Diabetes Families Exhibit High Cytolytic Activity and Subset Abundances That Correlate with Clinical Progression. Sci. Adv. 2024, 10, eadn2136. [Google Scholar] [CrossRef]
- Stallhofer, J.; Veith, L.; Diegelmann, J.; Probst, P.; Brand, S.; Schnitzler, F.; Olszak, T.; Török, H.; Mayerle, J.; Stallmach, A.; et al. Iron Deficiency in Inflammatory Bowel Disease Is Associated with Low Levels of Vitamin D Modulating Serum Hepcidin and Intestinal Ceruloplasmin Expression. Clin. Transl. Gastroenterol. 2022, 13, e00450. [Google Scholar] [CrossRef] [PubMed]
- Cozzolongo, R.; Osella, A.R.; Elba, S.; Petruzzi, J.; Buongiorno, G.; Giannuzzi, V.; Leone, G.; Bonfiglio, C.; Lanzilotta, E.; Manghisi, O.G.; et al. Epidemiology of HCV Infection in the General Population: A Survey in a Southern Italian Town. Am. J. Gastroenterol. 2009, 104, 2740–2746. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Albert, J.M.; Nelson, S. Generalized Causal Mediation Analysis. Biometrics 2011, 67, 1028–1038. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Parameters * | Total Cohort (n = 650) | Genotypes | p ^ | Multiple Comparisons Ψ | ||||
|---|---|---|---|---|---|---|---|---|
| Homozygous Minor (GG) (n = 163) (a) | Heterozygous (GT) (n = 334) (b) | Homozygous Major (TT) (n = 153) (c) | (b) vs. (a) | (c) vs. (a) | (c) vs. (b) | |||
| Gender (M) (%) | 274 (42.15) | 65 (39.88) | 142 (42.51) | 67 (43.79) | 0.77 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Age (yrs) | 61.25 ± 11.91 | 61.93 ± 12.50 | 60.70 ± 11.73 | 61.72 ± 11.68 | 0.30 | 0.46 | 0.99 | 0.23 |
| Age Classes (%) (yrs) | 0.37 † | 0.99 ¥ | 0.99 ¥ | 0.50 ¥ | ||||
| Adults (≤65) | 394 (60.62) | 98 (60.12) | 210 (62.87) | 86 (56.21) | ||||
| Elderly (>65) | 256 (39.38) | 65 (39.88) | 124 (37.13) | 67 (43.79) | ||||
| Education (%) | 0.08 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ | ||||
| None | 14 (2.26) | 4 (2.60) | 4 (1.25) | 6 (4.08) | ||||
| Elementary School | 193 (31.13) | 44 (28.57) | 99 (31.03) | 50 (34.01) | ||||
| Secondary School | 204 (32.90) | 51 (33.12) | 101 (31.66) | 52 (35.37) | ||||
| High School | 163 (26.29) | 43 (27.92) | 90 (28.21) | 30 (20.41) | ||||
| Degree | 22 (3.55) | 7 (4.55) | 15 (4.70) | 0 (0.00) | ||||
| Post-Degree | 24 (3.87) | 5 (3.25) | 10 (3.13) | 9 (6.12) | ||||
| Civil Status (%) | 0.68 † | 0.99 ¥ | 0.89 ¥ | 0.57 ¥ | ||||
| Single | 48 (7.74) | 14 (9.09) | 26 (8.15) | 8 (5.44) | ||||
| Married or Cohabiting | 508 (81.94) | 126 (81.82) | 257 (80.56) | 125 (85.03) | ||||
| Divorced or Separated | 17 (2.74) | 3 (1.95) | 12 (3.76) | 2 (1.36) | ||||
| Widow/er | 47 (7.58) | 11 (7.14) | 24 (7.52) | 12 (8.16) | ||||
| Smoker (Yes) (%) | 71 (11.40) | 18 (11.46) | 37 (11.56) | 16 (10.96) | 0.98 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Waist Circumference (cm) | 93.68 ± 12.64 | 92.90 ± 11.91 | 93.49 ± 12.54 | 94.94 ± 13.56 | 0.31 | 0.99 | 0.28 | 0.24 |
| Hip Circumference (cm) | 103.58 ± 9.32 | 103.56 ± 9.52 | 103.44 ± 9.17 | 103.92 ± 9.48 | 0.89 | 0.99 | 0.98 | 0.99 |
| BMI (Kg/m2) | 28.24 ± 4.70 | 28.27 ± 4.51 | 28.16 ± 4.51 | 28.39 ± 5.31 | 0.96 | 0.99 | 0.99 | 0.99 |
| Systolic Blood Pressure (mmHg) | 124.91 ± 15.15 | 124.81 ± 14.72 | 124.85 ± 15.07 | 125.16 ± 15.87 | 0.95 | 0.99 | 0.99 | 0.99 |
| Diastolic Blood Pressure (mmHg) | 78.65 ± 7.70 | 78.49 ± 7.33 | 78.94 ± 7.92 | 78.20 ± 7.60 | 0.55 | 0.68 | 0.99 | 0.48 |
| Diabetes (Yes) (%) | 58 (8.92) | 13 (7.98) | 23 (6.89) | 22 (14.38) | 0.02 † | 0.99 ¥ | 0.21 ¥ | 0.05 ¥ |
| Hypertension (Yes) (%) | 261 (42.16) | 63 (40.38) | 134 (42.14) | 64 (44.14) | 0.80 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Ulcer (Yes) (%) | 38 (6.14) | 9 (5.77) | 18 (5.66) | 11 (7.59) | 0.71 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Heart Attack (Yes) (%) | 15 (2.42) | 2 (1.28) | 7 (2.20) | 6 (4.14) | 0.29 † | 0.99 ¥ | 0.39 ¥ | 0.88 ¥ |
| Stroke (Yes) (%) | 2 (0.32) | 1 (0.64) | 1 (0.31) | 0 (0.00) | 0.74 † | 0.99 ¥ | -- | -- |
| NAFLD (Yes) (%) | 393 (60.46) | 98 (60.12) | 199 (59.58) | 96 (62.75) | 0.80 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| HOMA | 1.98 ± 1.91 | 1.90 ± 1.08 | 2.00 ± 2.38 | 2.03 ± 1.38 | 0.20 | 0.29 | 0.99 | 0.18 |
| Out of Range (>2.5) (%) | 142 (22.12) | 35 (22.01) | 64 (19.34) | 43 (28.29) | 0.09 † | 0.99 ¥ | 0.61 ¥ | 0.11 ¥ |
| Glycemia (mg/dL) | 99.14 ± 17.61 | 98.84 ± 18.15 | 98.40 ± 17.44 | 101.07 ± 17.38 | 0.13 | 0.99 | 0.13 | 0.10 |
| Out of Range (60–110) (%) | 91 (14.02) | 20 (12.35) | 41 (12.28) | 30 (19.61) | 0.07 † | 0.99 ¥ | 0.24 ¥ | 0.14 ¥ |
| Insulin (mmol/L) | 7.77 ± 4.98 | 7.50 ± 3.30 | 7.77 ± 5.56 | 8.03 ± 5.13 | 0.21 | 0.16 | 0.99 | 0.35 |
| Out of Range (1.9–23) (%) | 13 (2.02) | 3 (1.89) | 6 (1.81) | 4 (2.63) | 0.82 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Cholesterol (mg/dL) | 194.96 ± 36.37 | 197.93 ± 38.22 | 196.86 ± 34.40 | 187.69 ± 37.79 | 0.03 | 0.96 | 0.02 | 0.03 |
| Out of Range (>220) (%) | 156 (24.04) | 45 (27.78) | 81 (24.25) | 30 (19.61) | 0.23 † | 0.99 ¥ | 0.26 ¥ | 0.73 ¥ |
| Triglycerides (mg/dL) | 105.71 ± 67.45 | 115.42 ± 72.65 | 103.04 ± 63.38 | 101.23 ± 69.76 | 0.11 | 0.11 | 0.09 | 0.99 |
| Out of Range (36–165) (%) | 111 (17.10) | 34 (20.99) | 53 (15.87) | 24 (15.69) | 0.32 † | 0.53 ¥ | 0.67 ¥ | 0.99 ¥ |
| HDL (mg %) | 50.86 ± 12.63 | 50.65 ± 13.02 | 50.82 ± 12.49 | 51.16 ± 12.60 | 0.81 | 0.99 | 0.77 | 0.98 |
| Out of Range (40–60) (%) | 253 (38.98) | 60 (37.04) | 131 (39.22) | 62 (40.52) | 0.81 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| RBC (106/µL) | 4.96 ± 0.52 | 4.92 ± 0.54 | 4.98 ± 0.52 | 4.96 ± 0.51 | 0.41 | 0.30 | 0.45 | 0.99 |
| Out of Range (3.83–5.08) (%) | 244 (37.60) | 57 (35.19) | 129 (38.62) | 58 (37.91) | 0.76 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Hemoblogin (g/dL) | 14.04 ± 1.45 | 13.96 ± 1.49 | 14.12 ± 1.40 | 13.95 ± 1.52 | 0.44 | 0.43 | 0.99 | 0.46 |
| Out of Range (11.7–15.5) (%) | 122 (18.80) | 33 (20.37) | 62 (18.56) | 27 (17.65) | 0.82 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Hematocrit (L/L) | 42.30 ± 3.72 | 42.11 ± 3.83 | 42.46 ± 3.55 | 42.16 ± 3.95 | 0.55 | 0.49 | 0.99 | 0.66 |
| Out of Range (34.5–46.3) (%) | 94 (14.48) | 25 (15.43) | 47 (14.07) | 22 (14.38) | 0.92 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| MCV (fL) | 85.77 ± 7.43 | 86.09 ± 7.24 | 85.77 ± 7.04 | 85.44 ± 8.43 | 0.62 | 0.52 | 0.99 | 0.89 |
| Out of Range (80.4–95.9) (%) | 80 (12.33) | 20 (12.35) | 36 (10.78) | 24 (15.69) | 0.31 † | 0.99 ¥ | 0.99 ¥ | 0.45 ¥ |
| MCH (pg) | 28.46 ± 2.77 | 28.54 ± 2.77 | 28.51 ± 2.62 | 28.25 ± 3.06 | 0.65 | 0.97 | 0.53 | 0.80 |
| Out of Range (27.2–33.5) (%) | 112 (17.26) | 32 (19.75) | 51 (15.27) | 29 (18.95) | 0.38 † | 0.68 ¥ | 0.99 ¥ | 0.97 ¥ |
| MCHC (g/dL) | 33.16 ± 1.08 | 33.12 ± 1.10 | 33.23 ± 1.08 | 33.04 ± 1.03 | 0.11 | 0.39 | 0.65 | 0.07 |
| Out of Range (32.5–35.2) (%) | 176 (27.12) | 45 (27.78) | 86 (25.75) | 45 (29.41) | 0.68 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| RDW-CV (%) | 13.87 ± 1.48 | 13.93 ± 1.66 | 13.80 ± 1.39 | 13.95 ± 1.51 | 0.25 | 0.43 | 0.99 | 0.18 |
| Out of Range (10–15) (%) | 76 (11.71) | 19 (11.73) | 37 (11.08) | 20 (13.07) | 0.82 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Platelets (103/µL) | 230.88 ± 56.01 | 236.08 ± 65.02 | 229.02 ± 52.32 | 229.41 ± 53.50 | 0.58 | 0.44 | 0.78 | 0.99 |
| Out of Range (159–388) (%) | 52 (8.01) | 12 (7.41) | 24 (7.19) | 16 (10.46) | 0.44 † | 0.99 ¥ | 0.99 ¥ | 0.75 ¥ |
| WBC (103/µL) | 5.89 ± 1.86 | 5.73 ± 1.56 | 5.97 ± 2.11 | 5.87 ± 1.56 | 0.60 | 0.69 | 0.49 | 0.99 |
| Out of Range (4.1–11.2) (%) | 75 (11.56) | 21 (12.96) | 42 (12.57) | 12 (7.84) | 0.26 † | 0.99 ¥ | 0.40 ¥ | 0.28 ¥ |
| Neutrophils (%) | 57.77 ± 7.74 | 58.28 ± 7.43 | 57.40 ± 7.93 | 58.03 ± 7.65 | 0.50 | 0.39 | 0.99 † | 0.75 † |
| Out of Range (39.9–73) (%) | 27 (4.16) | 7 (4.32) | 14 (4.19) | 6 (3.92) | 0.98 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Lymphocytes (%) | 31.47 ± 7.26 | 30.95 ± 7.25 | 31.86 ± 7.37 | 31.19 ± 7.02 | 0.55 | 0.49 | 0.99 | 0.64 |
| Out of Range (18.8–50.8) (%) | 35 (5.39) | 11 (6.79) | 15 (4.49) | 9 (5.88) | 0.54 † | 0.94 ¥ | 0.99 ¥ | 0.99 ¥ |
| Monocytes (%) | 7.36 ± 1.67 | 7.48 ± 1.73 | 7.33 ± 1.52 | 7.30 ± 1.91 | 0.30 | 0.60 | 0.18 | 0.50 |
| Out of Range (4.1–12.2) (%) | 13 (2.00) | 4 (2.47) | 2 (0.60) | 7 (4.58) | 0.009 † | 0.44 ¥ | 0.94 ¥ | 0.07 ¥ |
| Basophils (%) | 0.54 ± 0.33 | 0.53 ± 0.31 | 0.55 ± 0.35 | 0.51 ± 0.30 | 0.20 | 0.48 | 0.77 | 0.13 |
| Out of Range (0.3–1.8) (%) | 89 (13.71) | 24 (14.81) | 40 (11.98) | 25 (16.34) | 0.38 † | 0.99 ¥ | 0.99 ¥ | 0.63 ¥ |
| Neutrophils (109/L) | 3.45 ± 1.43 | 3.38 ± 1.16 | 3.49 ± 1.65 | 3.43 ± 1.17 | 0.73 | 0.99 | 0.72 | 0.73 |
| Out of Range (1.8–6.4) (%) | 40 (6.16) | 8 (4.94) | 25 (7.49) | 7 (4.58) | 0.35 † | 0.76 ¥ | 0.99 ¥ | 0.57 ¥ |
| Lymphocytes (103/µL) | 1.81 ± 0.58 | 1.73 ± 0.50 | 1.85 ± 0.60 | 1.81 ± 0.60 | 0.23 | 0.13 | 0.58 | 0.75 |
| Out of Range (1.2–3.6) (%) | 61 (9.40) | 19 (11.73) | 27 (8.08) | 15 (9.80) | 0.42 † | 0.64 ¥ | 0.99 ¥ | 0.99 ¥ |
| Monocytes (103/µL) | 0.43 ± 0.15 | 0.43 ± 0.17 | 0.43 ± 0.15 | 0.42 ± 0.13 | 0.86 | 0.98 | 0.99 | 0.99 |
| Out of Range (0.3–0.9) (%) | 117 (18.03) | 35 (21.60) | 56 (16.77) | 26 (16.99) | 0.39 † | 0.62 ¥ | 0.90 ¥ | 0.99 ¥ |
| Basophils (103/µL) | 0.03 ± 0.05 | 0.03 ± 0.02 | 0.03 ± 0.07 | 0.03 ± 0.02 | 0.42 | 0.37 | 0.99 | 0.51 |
| Out of Range (0–0.2) (%) | 1 (0.15) | 0 (0.00) | 1 (0.30) | 0 (0.00) | 0.99 † | -- | -- | -- |
| Eosinophils (103/µL) | 0.17 ± 0.15 | 0.16 ± 0.16 | 0.17 ± 0.13 | 0.17 ± 0.17 | 0.37 | 0.26 | 0.40 | 0.99 |
| Out of Range (0.1–0.5) (%) | 202 (31.12) | 57 (35.19) | 103 (30.84) | 42 (27.45) | 0.33 † | 0.99 ¥ | 0.41 ¥ | 0.99 ¥ |
| HbA1c (mmol/mol) | 38.08 ± 7.68 | 38.67 ± 8.67 | 37.57 ± 6.84 | 38.55 ± 8.24 | 0.45 | 0.61 | 0.99 | 0.36 |
| Out of Range (20–42) (%) | 113 (17.44) | 26 (16.05) | 52 (15.62) | 35 (22.88) | 0.13 † | 0.99 ¥ | 0.38 ¥ | 0.20 ¥ |
| Total Bilirubin (mg/dL) | 0.70 ± 0.36 | 0.67 ± 0.30 | 0.70 ± 0.36 | 0.75 ± 0.41 | 0.44 | 0.83 | 0.31 | 0.57 |
| Out of Range (0.1–1.2) (%) | 65 (10.02) | 11 (6.79) | 32 (9.58) | 22 (14.38) | 0.07 † | 0.82 ¥ | 0.09 ¥ | 0.42 ¥ |
| Direct Bilirubin (mg/dL) | 0.17 ± 0.05 | 0.17 ± 0.05 | 0.17 ± 0.05 | 0.18 ± 0.06 | 0.51 | 0.99 | 0.43 | 0.49 |
| Out of Range (0.1–0.5) (%) | 4 (0.62) | 1 (0.63) | 2 (0.60) | 1 (0.65) | 0.99 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| GOT (U/L) | 22.30 ± 8.67 | 23.51 ± 14.08 | 22.23 ± 6.19 | 21.17 ± 4.87 | 0.18 | 0.87 | 0.11 | 0.20 |
| Out of Range (0–30) (%) | 38 (5.86) | 10 (6.17) | 22 (6.59) | 6 (3.92) | 0.50 † | 0.99 ¥ | 0.99 ¥ | 0.60 ¥ |
| SGPT (U/L) | 22.22 ± 12.05 | 22.28 ± 15.04 | 22.88 ± 11.89 | 20.71 ± 8.14 | 0.17 † | 0.38 | 0.84 | 0.11 |
| Out of Range (0–30) (%) | 77 (11.86) | 18 (11.11) | 49 (14.67) | 10 (6.54) | 0.03 † | 0.77 ¥ | 0.45 ¥ | 0.01 ¥ |
| GGT (U/L) | 17.82 ± 13.84 | 18.72 ± 17.98 | 17.68 ± 12.77 | 17.17 ± 10.75 | 0.61 | 0.99 | 0.61 | 0.52 |
| Out of Range (7–22) (%) | 111 (17.10) | 26 (16.05) | 60 (17.96) | 25 (16.34) | 0.93 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Alkaline Phosphatase (U/L) | 56.44 ± 16.42 | 57.31 ± 15.69 | 56.03 ± 16.58 | 56.42 ± 16.88 | 0.34 | 0.21 | 0.54 | 0.99 |
| Out of Range (38–126) (%) | 52 (8.04) | 13 (8.02) | 31 (9.28) | 8 (5.30) | 0.33 † | 0.99 ¥ | 0.99 ¥ | 0.30 ¥ |
| Albumin (g/dL) | 4.07 ± 0.27 | 4.08 ± 0.31 | 4.08 ± 0.26 | 4.05 ± 0.24 | 0.72 | 0.99 | 0.99 | 0.64 |
| Out of Range (3.5–5.5) (%) | 7 (1.13) | 4 (2.58) | 1 (0.31) | 2 (1.36) | 0.06 † | 0.25 ¥ | 0.99 ¥ | 0.89 ¥ |
| Iron (µg/dL) | 90.35 ± 31.20 | 90.69 ± 32.25 | 89.46 ± 30.29 | 91.95 ± 32.15 | 0.59 | 0.99 | 0.70 | 0.47 |
| Out of Range (49–151) (%) | 71 (10.97) | 21 (13.04) | 34 (10.18) | 16 (10.53) | 0.62 † | 0.99 ¥ | 0.99 ¥ | 0.99 ¥ |
| Ferritin (ng/mL) | 91.48 ± 83.35 | 88.09 ± 85.05 | 95.84 ± 88.09 | 85.55 ± 69.75 | 0.34 | 0.26 | 0.99 | 0.48 |
| Out of Range (11–200) (%) | 542 (83.51) | 134 (82.72) | 284 (85.03) | 124 (81.05) | 0.52 † | 0.99 ¥ | 0.99 ¥ | 0.85 ¥ |
| Ceruloplasmin (mg/dL) | 30.83 ± 6.49 | 31.83 ± 6.24 | 30.49 ± 6.43 | 30.49 ± 6.80 | 0.04 | 0.02 | 0.06 | 0.99 |
| Out of Range (25–63) (%) | 112 (17.26) | 16 (9.88) | 68 (20.36) | 28 (18.30) | 0.01 † | 0.004 ¥ | 0.09 ¥ | 0.99 ¥ |
| α1AT (mg/dL) | 172.25 ± 27.36 | 175.10 ± 28.26 | 171.00 ± 27.82 | 171.95 ± 25.26 | 0.08 | 0.04 | 0.17 | 0.99 |
| Out of Range (90–200) (%) | 86 (13.25) | 30 (18.52) | 40 (11.98) | 16 (10.46) | 0.07 † | 0.19 ¥ | 0.12 ¥ | 0.99 ¥ |
| Genotypes | OR | se (OR) | 95% C.I. | p |
|---|---|---|---|---|
| GG [Ref.] | -- | -- | -- | -- |
| GT | 0.95 | 0.35 | 0.46 to 1.98 | 0.90 |
| TT | 2.14 | 0.82 | 1.01 to 4.53 | 0.05 |
| G-Carriers | ||||
| TT [Ref.] | -- | -- | -- | -- |
| GG/GT | 0.45 | 0.13 | 0.25 to 0.81 | 0.008 |
| Effects | β | se (β) | 95% C.I. | p |
|---|---|---|---|---|
| Indirect | ||||
| rs2802292 (GT) → Diabetes → NAFLD | −0.001 | 0.006 | −0.01 to 0.01 | 0.84 |
| rs2802292 (TT) → Diabetes → NAFLD | 0.01 | 0.008 | −0.001 to 0.03 | 0.08 |
| Component | ||||
| rs2802292 (GT) → Diabetes | −0.01 | 0.03 | −0.06 to 0.05 | 0.83 |
| rs2802292 (TT) → Diabetes | 0.10 | 0.03 | 0.003 to 0.12 | 0.04 |
| Diabetes → NAFLD | 0.13 | 0.06 | 0.10 to 0.35 | <0.001 |
| Direct | ||||
| rs2802292 (GT) → NAFLD | 0.008 | 0.04 | −0.08 to 0.09 | 0.85 |
| rs2802292 (TT) → NAFLD | 0.009 | 0.05 | −0.09 to 0.11 | 0.84 |
| Total | ||||
| rs2802292 (GT) → NAFLD | 0.007 | 0.04 | −0.08 to 0.09 | 0.88 |
| rs2802292 (TT) → NAFLD | 0.02 | 0.05 | −0.08 to 0.13 | 0.63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forte, G.; Donghia, R.; Lepore Signorile, M.; Tatoli, R.; Bonfiglio, C.; Losito, F.; De Marco, K.; Manghisi, A.; Guglielmi, F.A.; Disciglio, V.; et al. Exploring the Relationship of rs2802292 with Diabetes and NAFLD in a Southern Italian Cohort—Nutrihep Study. Int. J. Mol. Sci. 2024, 25, 9512. https://doi.org/10.3390/ijms25179512
Forte G, Donghia R, Lepore Signorile M, Tatoli R, Bonfiglio C, Losito F, De Marco K, Manghisi A, Guglielmi FA, Disciglio V, et al. Exploring the Relationship of rs2802292 with Diabetes and NAFLD in a Southern Italian Cohort—Nutrihep Study. International Journal of Molecular Sciences. 2024; 25(17):9512. https://doi.org/10.3390/ijms25179512
Chicago/Turabian StyleForte, Giovanna, Rossella Donghia, Martina Lepore Signorile, Rossella Tatoli, Caterina Bonfiglio, Francesco Losito, Katia De Marco, Andrea Manghisi, Filomena Anna Guglielmi, Vittoria Disciglio, and et al. 2024. "Exploring the Relationship of rs2802292 with Diabetes and NAFLD in a Southern Italian Cohort—Nutrihep Study" International Journal of Molecular Sciences 25, no. 17: 9512. https://doi.org/10.3390/ijms25179512