



Osseointegration Potential Assessment of Bone Graft Materials Loaded with Mesenchymal Stem Cells in Peri-Implant Bone Defects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
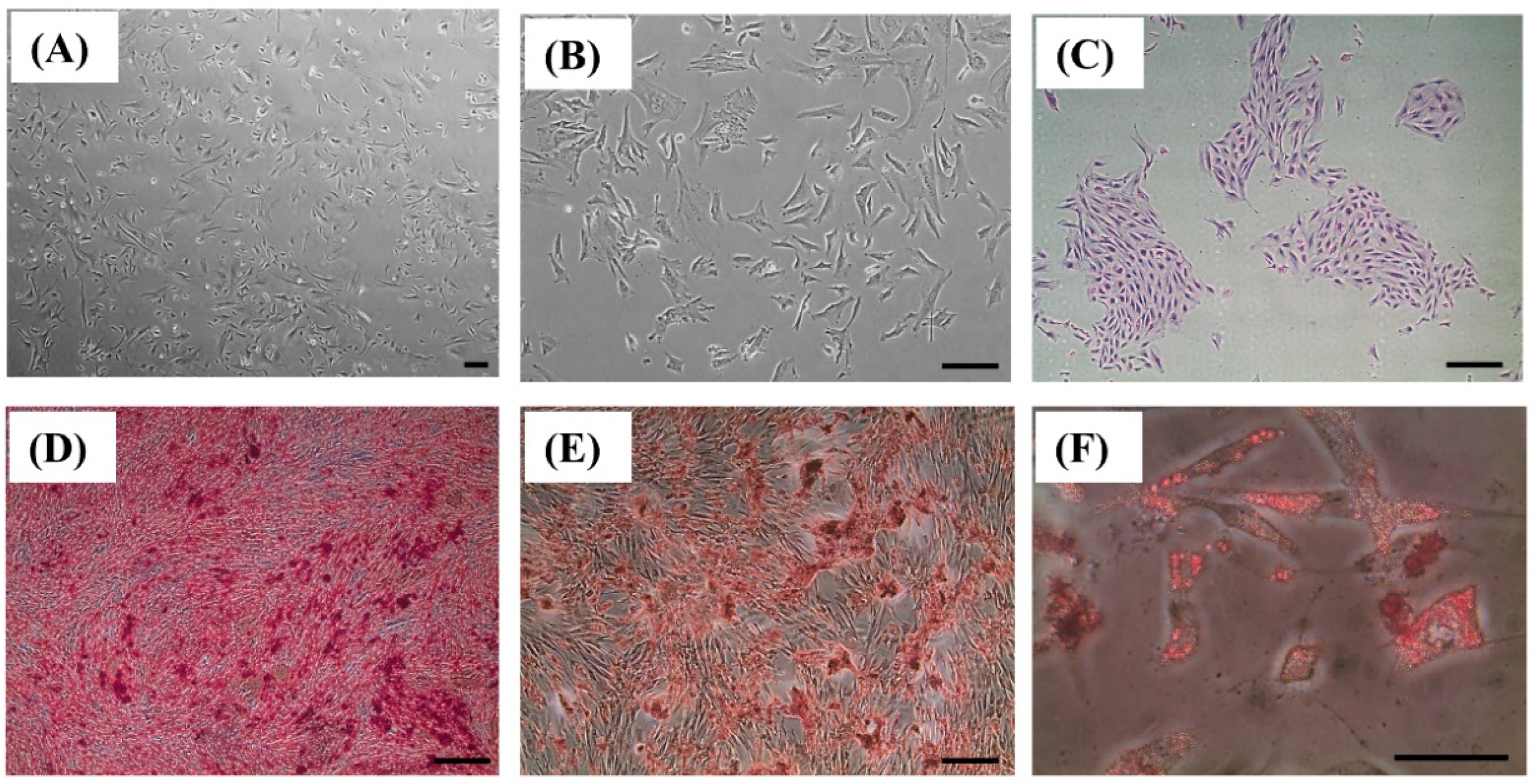
2.1. BMSC Isolation, Culture, and Osteogenic Differentiation
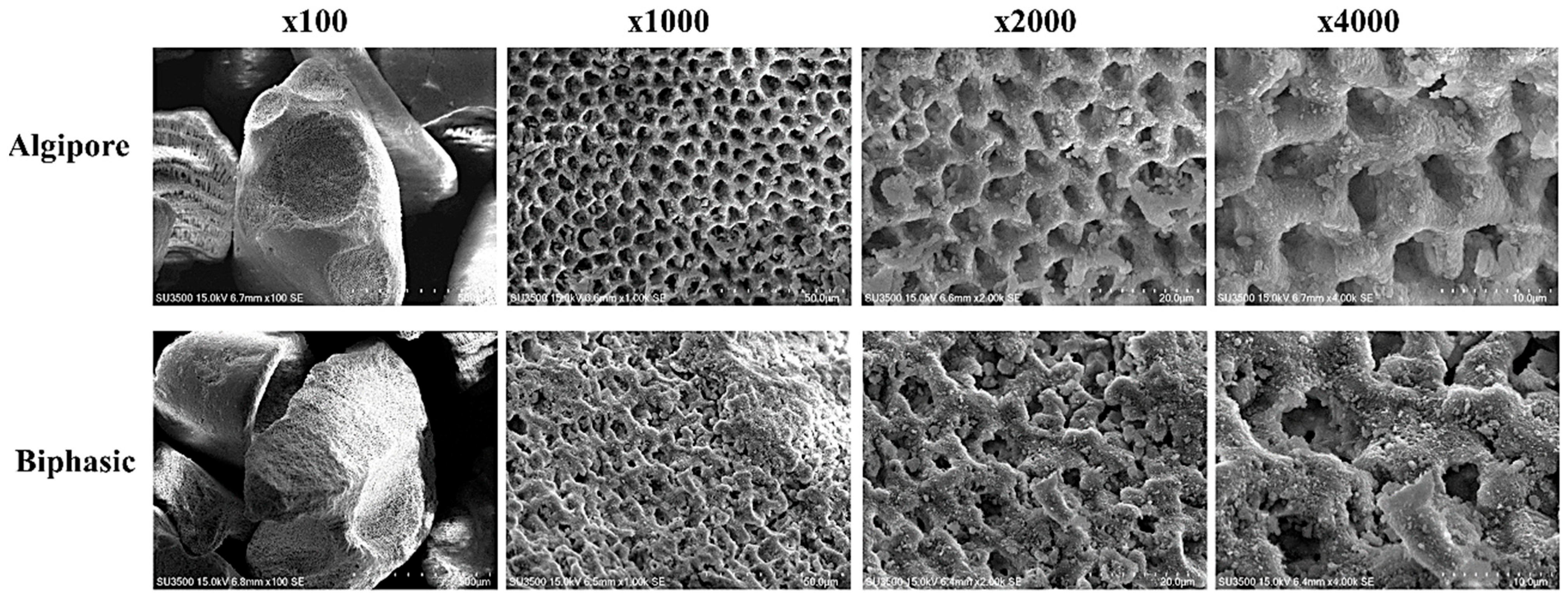
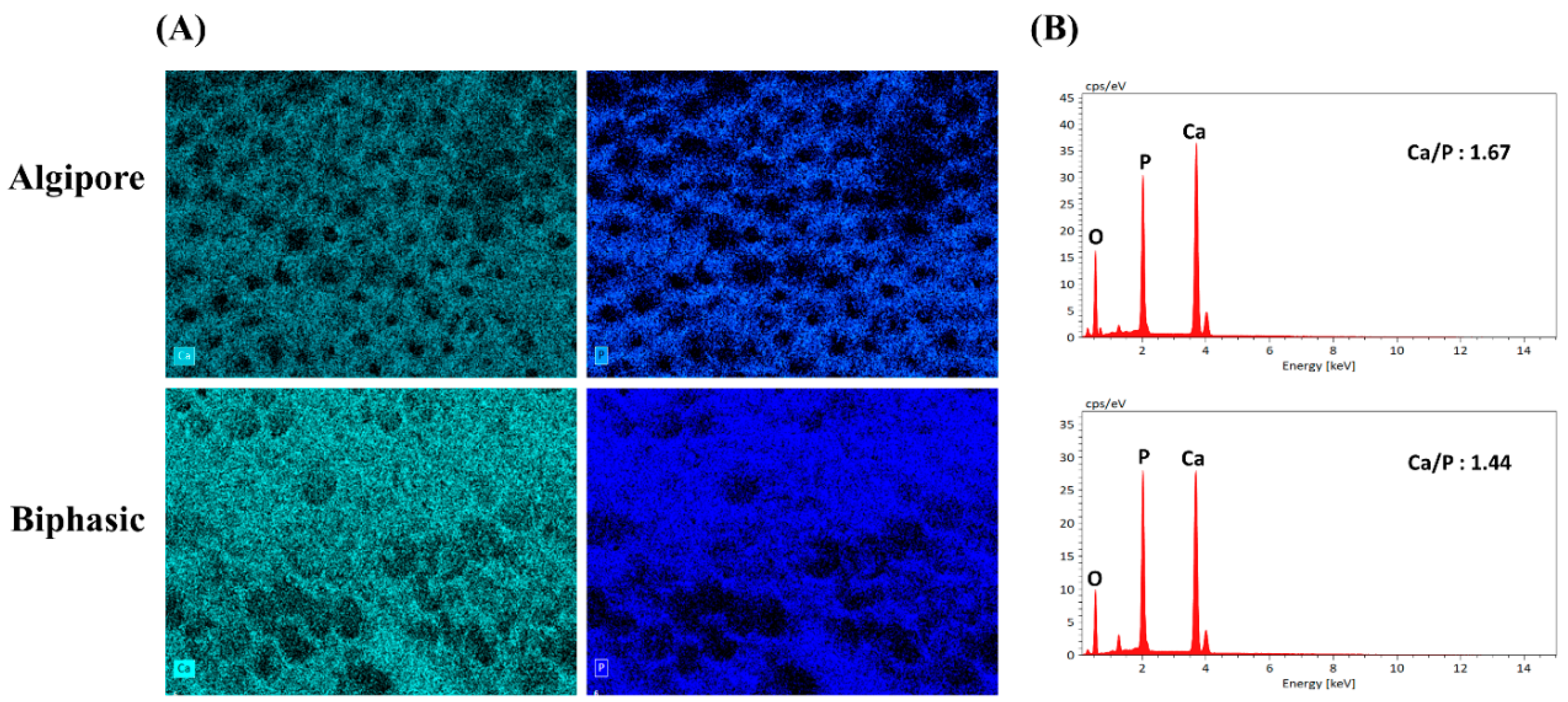
2.2. SEM and EDS
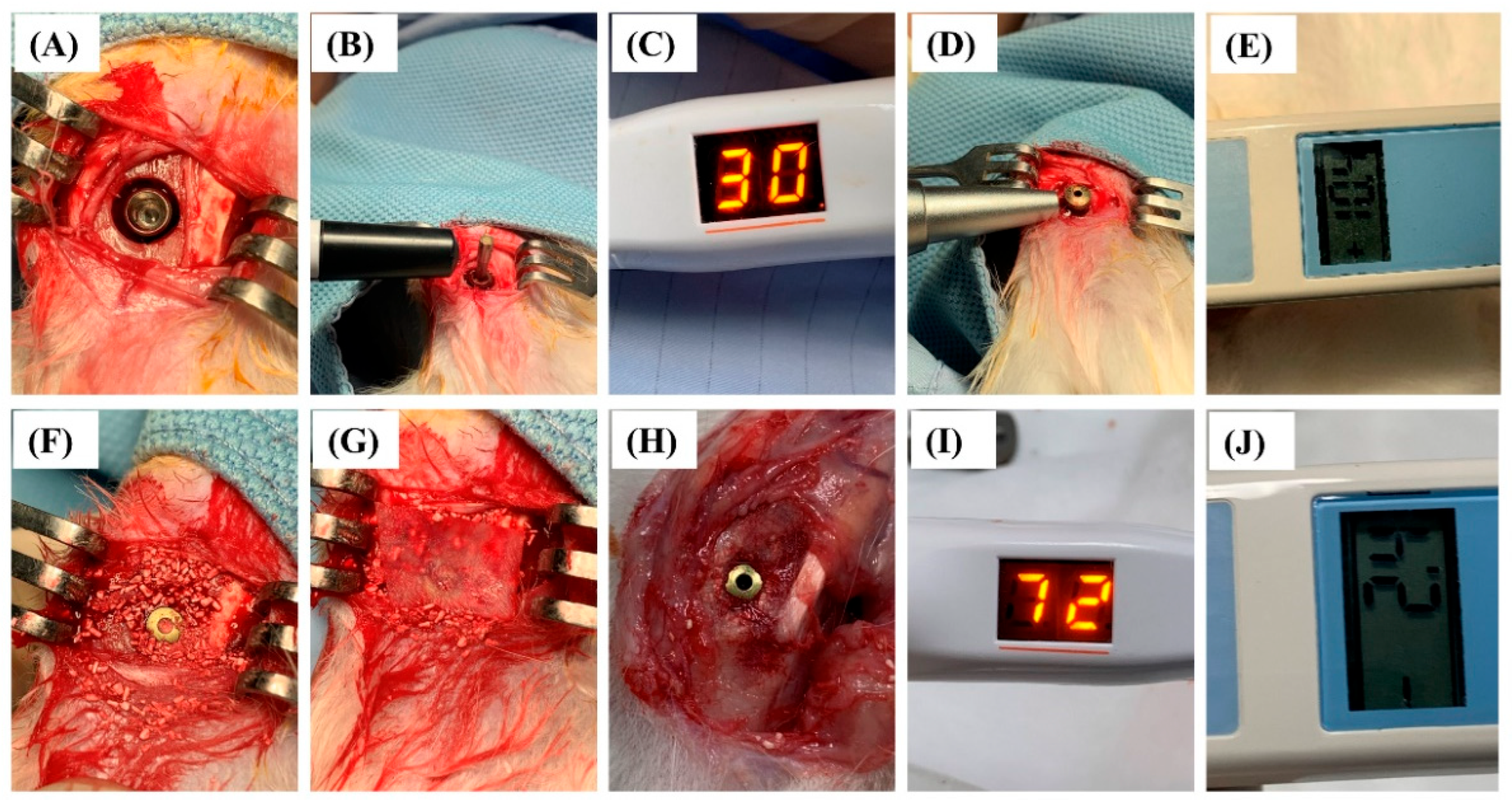
2.3. Animal Status and Implant Surgery Result
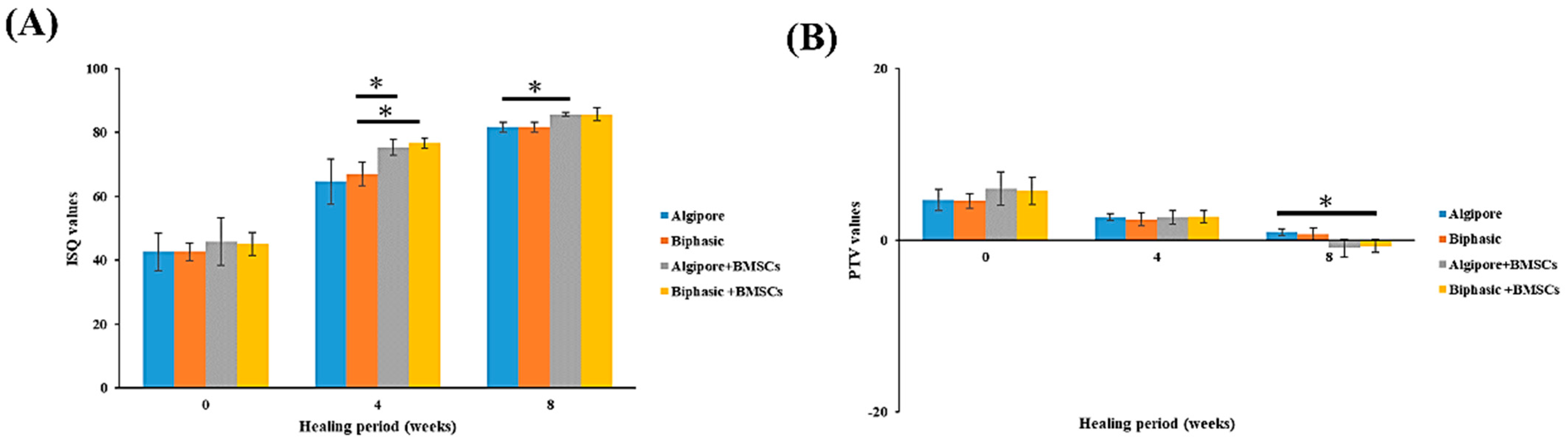
2.4. Implant Stability Detection
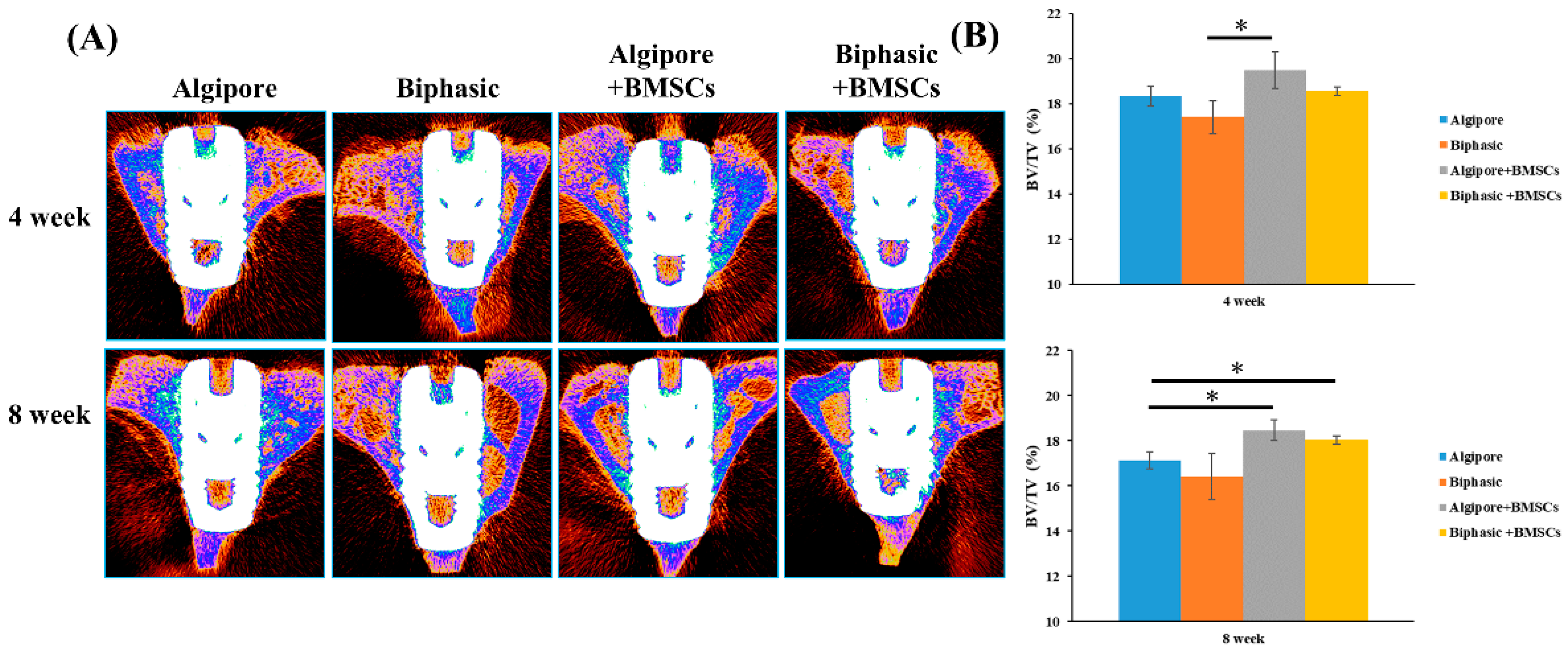
2.5. Micro-CT Measurements
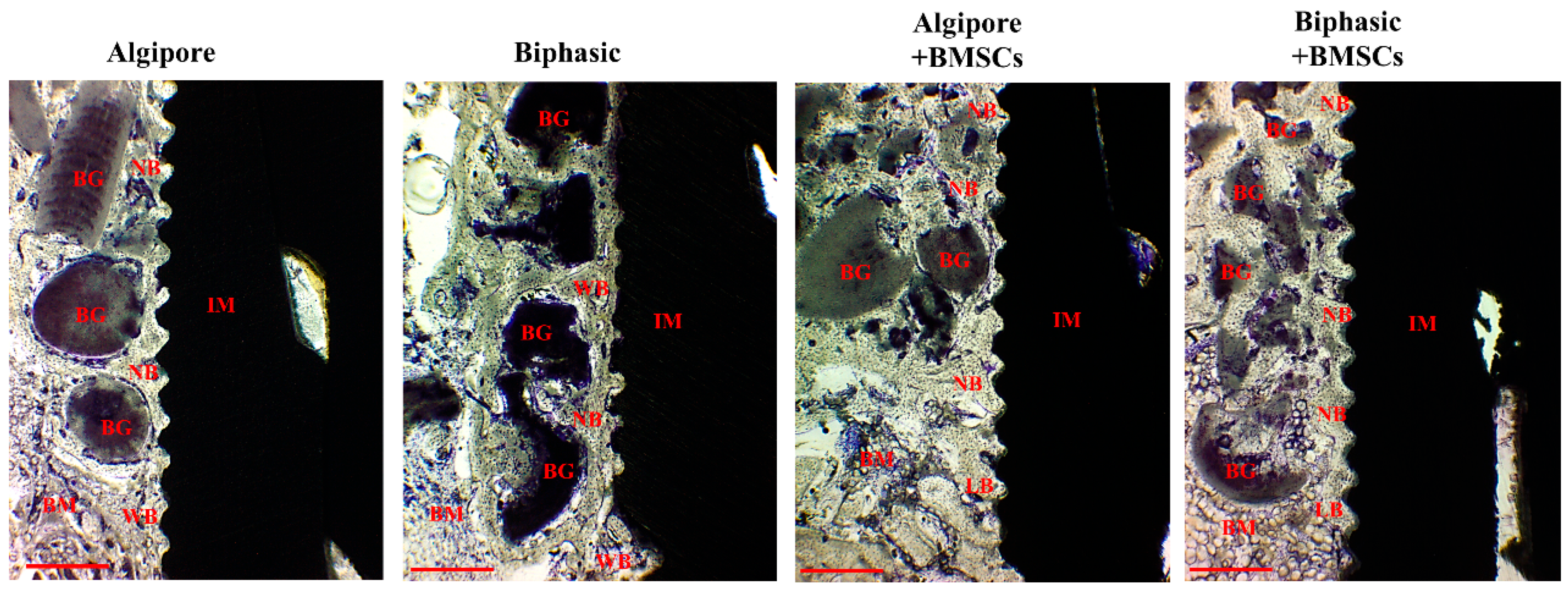
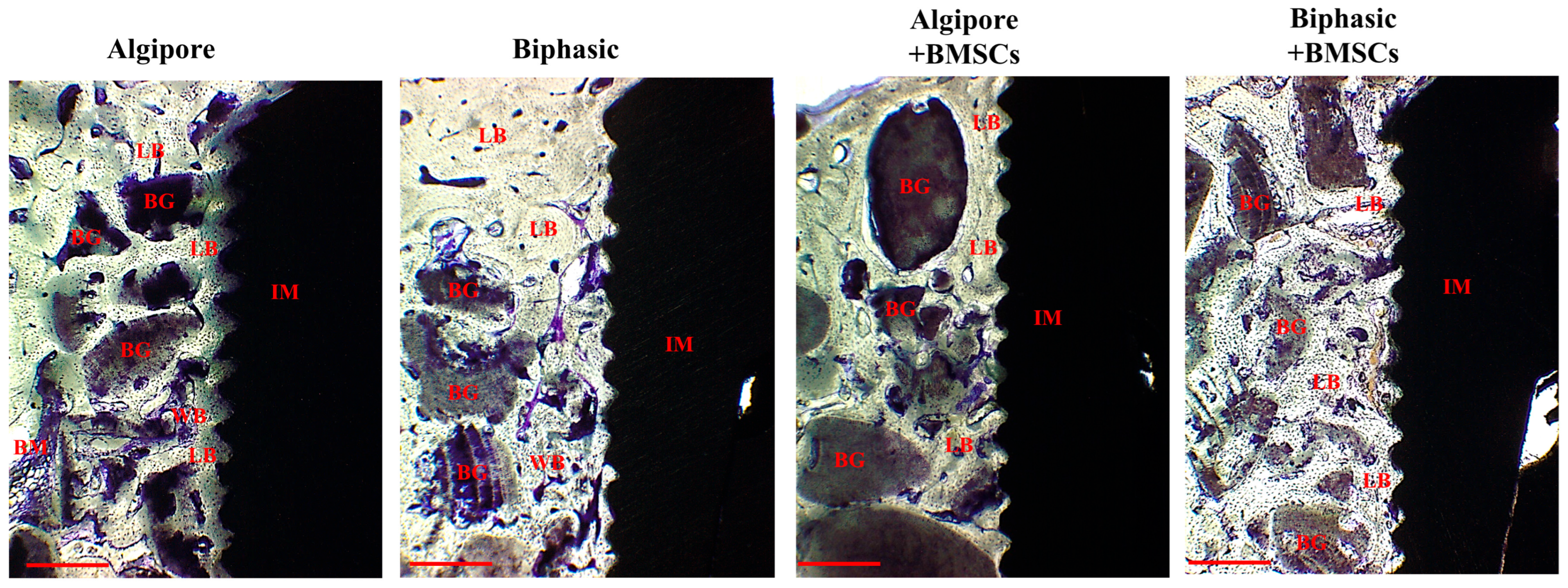
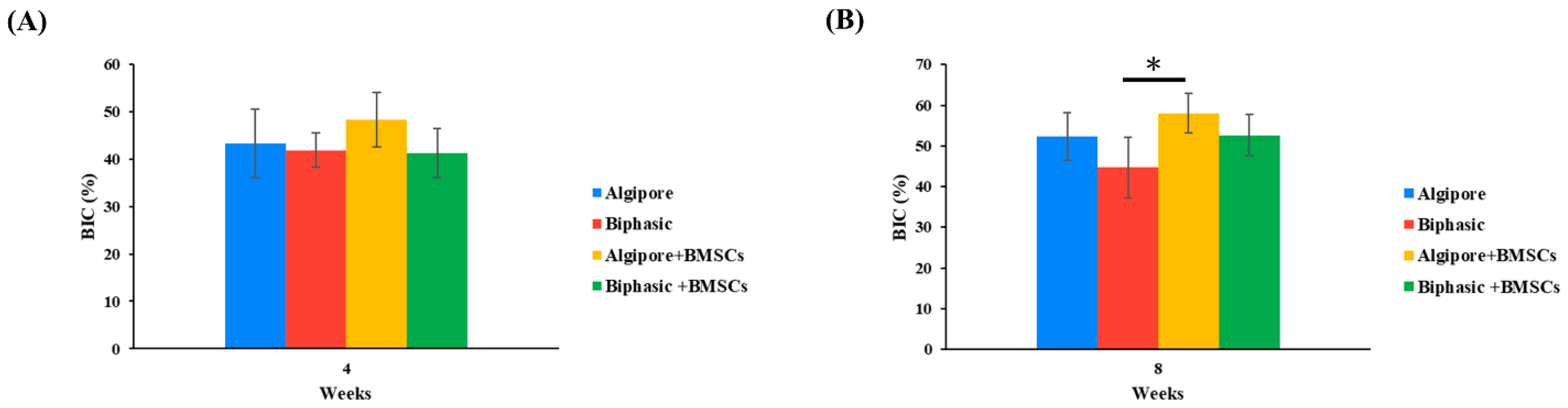
2.6. Histological and Histomorphometric Analyses
3. Discussion
4. Materials and Methods
4.1. BMSC Isolation, Culture, and Characterization
4.2. Scanning Electron Microscopy and Energy-Dispersive X-ray Spectroscopy
4.3. Implants, BGM, and Membranes
4.4. Surgical Procedures for Implants
4.5. Measurement of Implant Stability Parameters
4.6. Micro-Computed Tomography Measurement
4.7. Histology and Histomorphometric Analysis
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grassi, F.R.; Grassi, R.; Rapone, B.; Alemanno, G.; Balena, A.; Kalemaj, Z. Dimensional changes of buccal bone plate in immediate implants inserted through open flap, open flap and bone grafting and flapless techniques: A cone-beam computed tomography randomized controlled clinical trial. Clin. Oral Implants Res. 2019, 30, 1155–1164. [Google Scholar] [CrossRef]
- Huang, H.M.; Chee, T.J.; Lew, W.Z.; Feng, S.W. Modified surgical drilling protocols influence osseointegration performance and predict the value of implant stability parameters during implant healing process. Clin. Oral Investig. 2020, 24, 3445–3455. [Google Scholar] [CrossRef] [PubMed]
- Trento, G.D.S.; Spin-Neto, R.; Bassi, A.P.F.; Okamoto, R.; Gabrielli, M.A.C.; Pereira-Filho, V.A. Bone tissue formation around two titanium implant surfaces placed in bone defects filled with bone substitute material or blood clot: A pilot study. Clin. Implant Dent. Relat. Res. 2019, 21, 1175–1180. [Google Scholar] [CrossRef] [PubMed]
- Shanbhag, S.; Pandis, N.; Mustafa, K.; Nyengaard, J.R.; Stavropoulos, A. Bone tissue engineering in oral peri-implant defects in preclinical in vivo research: A systematic review and meta-analysis. J. Tissue Eng. Regen. Med. 2018, 12, e336–e349. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, F.; Alshehri, M.; Sumague, T.; Niazy, A.; Jansen, J.; van den Beucken, J.; Alghamdi, H. Evaluation of Peri-Implant Bone Grafting Around Surface-Porous Dental Implants: An In Vivo Study in a Goat Model. Materials 2019, 12, 3606. [Google Scholar] [CrossRef]
- Dos Santos Trento, G.; Hassumi, J.S.; Buzo Frigério, P.; Farnezi Bassi, A.P.; Okamoto, R.; Gabrielli, M.A.C.; Pereira-Filho, V.A. Gene expression, immunohistochemical and microarchitectural evaluation of bone formation around two implant surfaces placed in bone defects filled or not with bone substitute material. Int. J. Implant Dent. 2020, 6, 80. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Sohn, J.Y.; Lim, H.C.; Jung, U.W.; Choi, S.H. Different bone regeneration patterns in periimplant circumferential gap defects grafted with two types of osteoconductive biomaterial. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 1202–1209. [Google Scholar] [CrossRef]
- Le Thieu, M.K.; Homayouni, A.; Hæren, L.R.; Tiainen, H.; Verket, A.; Ellingsen, J.E.; Rønold, H.J.; Wohlfahrt, J.C.; Cantalapiedra, A.G.; Muñoz, F.M.G.; et al. Impact of simultaneous placement of implant and block bone graft substitute: An in vivo peri-implant defect model. Biomater. Res. 2021, 25, 43. [Google Scholar] [CrossRef]
- Trento, G.; de A Carvalho, P.H.; de C Reis, E.N.R.; Spin-Neto, R.; Bassi, A.P.F.; Pereira-Filho, V.A. Bone formation around two titanium implant surfaces placed in bone defects with and without a bone substitute material: A histological, histomorphometric, and micro-computed tomography evaluation. Clin. Implant Dent. Relat. Res. 2020, 22, 177–185. [Google Scholar] [CrossRef]
- Verket, A.; Lyngstadaas, S.P.; Tiainen, H.; Rønold, H.J.; Wohlfahrt, J.C. Impact of particulate deproteinized bovine bone mineral and porous titanium granules on early stability and osseointegration of dental implants in narrow marginal circumferential bone defects. Int. J. Oral Maxillofac. Surg. 2018, 47, 1086–1094. [Google Scholar] [CrossRef]
- Jun, J.H.; Oh, K.C.; Park, K.H.; Jung, N.; Li, J.; Moon, H.S. Improvement of Osseointegration by Ultraviolet and/or Simvastatin Treatment on Titanium Implants with or without Bone Graft Materials. Materials 2021, 14, 3707. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef] [PubMed]
- Damerau, J.M.; Bierbaum, S.; Wiedemeier, D.; Korn, P.; Smeets, R.; Jenny, G.; Nadalini, J.; Stadlinger, B. A systematic review on the effect of inorganic surface coatings in large animal models and meta-analysis on tricalcium phosphate and hydroxyapatite on periimplant bone formation. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 157–175. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.K.; Nandi, S.K.; Kundu, B.; Datta, S.; De, D.K.; Roy, S.K.; Basu, D. In vivo response of porous hydroxyapatite and beta-tricalcium phosphate prepared by aqueous solution combustion method and comparison with bioglass scaffolds. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 86, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Li, P.; Zhu, J.; Xia, Y.; Zhang, W. Polygonatum polysaccharide modified montmorillonite/chitosan/glycerophosphate composite hydrogel for bone tissue engineering. Int. J. Polym. Mater. 2022, 71, 1176–118716. [Google Scholar] [CrossRef]
- Rapone, B.; Inchingolo, A.D.; Trasarti, S.; Ferrara, E.; Qorri, E.; Mancini, A.; Montemurro, N.; Scarano, A.; Inchingolo, A.M.; Dipalma, G.; et al. Long-Term Outcomes of Implants Placed in Maxillary Sinus Floor Augmentation with Porous Fluorohydroxyapatite (Algipore® FRIOS®) in Comparison with Anorganic Bovine Bone (Bio-Oss®) and Platelet Rich Plasma (PRP): A Retrospective Study. J. Clin. Med. 2022, 11, 2491. [Google Scholar] [CrossRef]
- Noelken, R.; Pausch, T.; Wagner, W.; Al-Nawas, B. Peri-implant defect grafting with autogenous bone or bone graft material in immediate implant placement in molar extraction sites-1- to 3-year results of a prospective randomized study. Clin. Oral Implants Res. 2020, 31, 1138–1148. [Google Scholar] [CrossRef]
- Al-Maawi, S.; Rutkowski, J.L.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. The Biomaterial-Induced Cellular Reaction Allows a Novel Classification System Regardless of the Biomaterials Origin. J. Oral Implantol. 2020, 46, 190–207. [Google Scholar] [CrossRef]
- Galindo-Moreno, P.; Padial-Molina, M.; Lopez-Chaichio, L.; Gutiérrez-Garrido, L.; Martín-Morales, N.; O’Valle, F. Algae-derived hydroxyapatite behavior as bone biomaterial in comparison with anorganic bovine bone: A split-mouth clinical, radiological, and histologic randomized study in humans. Clin. Oral Implants Res. 2020, 31, 536–548. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Ahmad, M.; Bruun, N.H.; Becktor, J.P. Patient’s perception of recovery after maxillary sinus floor augmentation with autogenous bone graft compared with composite grafts: A single-blinded randomized controlled trial. Int. J. Implant Dent. 2021, 7, 99. [Google Scholar] [CrossRef]
- Chan, Y.H.; Ho, K.N.; Lee, Y.C.; Chou, M.J.; Lew, W.Z.; Huang, H.M.; Lai, P.C.; Feng, S.W. Melatonin enhances osteogenic differentiation of dental pulp mesenchymal stem cells by regulating MAPK pathways and promotes the efficiency of bone regeneration in calvarial bone defects. Stem Cell Res. Ther. 2022, 13, 73. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, M.; Atsuta, I.; Ayukawa, Y.; Yamaza, T.; Kondo, R.; Matsuura, Y.; Koyano, K. The influence of systemically or locally administered mesenchymal stem cells on tissue repair in a rat oral implantation model. Int. J. Implant Dent. 2018, 4, 2. [Google Scholar] [CrossRef] [PubMed]
- Leocádio, A.C.S.; Silva, M., Jr.; de Oliveira, G.J.P.L.; Marcantonio, É., Jr. Osseointegration of different implant surfaces in areas grafted with deproteinized bovine bone associated or not with fresh bone marrow-Preclinical study in rabbits. Clin. Oral Implants Res. 2021, 32, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.H.; Han, S.H.; Choi, S.H.; Lee, M.H.; Lee, S.J.; Song, S.U.; Oh, N. Effects of bone marrow-derived mesenchymal stem cells and platelet-rich plasma on bone regeneration for osseointegration of dental implants: Preliminary study in canine three-wall intrabony defects. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 1021–1030. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, Ö.; Supachawaroj, N.; Soontornvipart, K.; Kheolamai, P. Treatment of Peri-Implant Defects in the Rabbit’s Tibia with Adipose or Bone Marrow-Derived Mesenchymal Stems Cells. Clin. Implant Dent. Relat. Res. 2016, 18, 1003–1014. [Google Scholar] [CrossRef]
- Abdullah Alqahtani, N.; Chandramoorthy, H.C.; Shaik, S.; Syed, J.; Chowdhary, R.; Antony, L. Bone Marrow Mesenchymal Stromal Cells (BMMSCs) Augment Osteointegration of Dental Implants in Type 1 Diabetic Rabbits: An X-Ray Micro-Computed Tomographic Evaluation. Medicina 2020, 56, 148. [Google Scholar] [CrossRef]
- Dos Santos, P.L.; de Molon, R.S.; Queiroz, T.P.; Okamoto, R.; de Souza Faloni, A.P.; Gulinelli, J.L.; Luvizuto, E.R.; Garcia, I.R., Jr. Evaluation of bone substitutes for treatment of peri-implant bone defects: Biomechanical, histological, and immunohistochemical analyses in the rabbit tibia. J. Periodontal Implant Sci. 2016, 46, 176–196. [Google Scholar] [CrossRef]
- Fraser, D.; Mendonca, G.; Sartori, E.; Funkenbusch, P.; Ercoli, C.; Meirelles, L. Bone response to porous tantalum implants in a gap-healing model. Clin. Oral Implants Res. 2019, 30, 156–168. [Google Scholar] [CrossRef]
- Ding, L.; Tang, S.; Liang, P.; Wang, C.; Zhou, P.F.; Zheng, L. Bone Regeneration of Canine Peri-implant Defects Using Cell Sheets of Adipose-Derived Mesenchymal Stem Cells and Platelet-Rich Fibrin Membranes. J. Oral Maxillofac. Surg. 2019, 77, 499–514. [Google Scholar] [CrossRef]
- Misawa, M.Y.O.; Huynh-Ba, G.; Villar, G.M.; Villar, C.C. Efficacy of stem cells on the healing of peri-implant defects: Systematic review of preclinical studies. Clin. Exp. Dent Res. 2016, 2, 18–34. [Google Scholar] [CrossRef]
- Santos, P.L.; Gulinelli, J.L.; Telles Cda, S.; Betoni Júnior, W.; Okamoto, R.; Chiacchio Buchignani, V.; Queiroz, T.P. Bone substitutes for peri-implant defects of postextraction implants. Int. J. Biomater. 2013, 2013, 307136. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Perrotti, V.; Degidi, M.; Piattelli, A.; Iezzi, G. Bone regeneration with algae-derived hydroxyapatite: A pilot histologic and histomorphometric study in rabbit tibia defects. Int. J. Oral Maxillofac. Implants 2012, 27, 336–340. [Google Scholar] [PubMed]
- Sokolowski, A.; Sokolowski, A.; Schwarze, U.; Theisen, K.; Payer, M.; Lorenzoni, M.; Wegscheider, W. Phycogenic bone substitutes for sinus floor augmentation: Histomorphometric comparison of hydroxyapatite and biphasic calcium phosphate in a randomised clinical pilot study. Int. J. Oral Implantol. 2020, 13, 387–399. [Google Scholar]
- Prati, C.; Zamparini, F.; Botticelli, D.; Ferri, M.; Yonezawa, D.; Piattelli, A.; Gandolfi, M.G. The Use of ESEM-EDX as an Innovative Tool to Analyze the Mineral Structure of Peri-Implant Human Bone. Materials 2020, 13, 1671. [Google Scholar] [CrossRef]
- El Chaar, E.; Zhang, L.; Zhou, Y.; Sandgren, R.; Fricain, J.C.; Dard, M.; Pippenger, B.; Catros, S. Osseointegration of Superhydrophilic Implants Placed in Defect Grafted Bones. Int. J. Oral Maxillofac. Implants 2019, 34, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Stramandinoli-Zanicotti, R.T.; Sassi, L.M.; Rebelatto, C.L.; Boldrine-Leite, L.M.; Brofman, P.R.; Carvalho, A.L. The effect of bone marrow-derived stem cells associated with platelet-rich plasma on the osseointegration of immediately placed implants. J. Clin. Exp. Dent. 2021, 13, e8–e13. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Sim, J.H.; Yeo, I.L. Characteristics of contact and distance osteogenesis around modified implant surfaces in rabbit tibiae. J. Periodontal. Implant Sci. 2017, 47, 182–192. [Google Scholar] [CrossRef]
- Davies, J.E. Mechanisms of endosseous integration. Int. J. Prosthodont. 1998, 11, 391–401. [Google Scholar]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. PLoS Biol. 2020, 18, e3000410. [Google Scholar]
- Feng, S.W.; Ho, K.N.; Chan, Y.H.; Chang, K.J.; Lai, W.Y.; Huang, H.M. Damping Factor as a Diagnostic Parameter for Assessment of Osseointegration during the Dental Implant Healing Process: An Experimental Study in Rabbits. Ann. Biomed. Eng. 2016, 44, 3668–3678. [Google Scholar] [CrossRef]
- Chan, Y.H.; Lew, W.Z.; Lu, E.; Loretz, T.; Lu, L.; Lin, C.T.; Feng, S.W. An evaluation of the biocompatibility and osseointegration of novel glass fiber reinforced composite implants: In vitro and in vivo studies. Dent. Mater. 2018, 34, 470–485. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Meng, Y.; Hao, D.; Liu, H. Parathyroid hormone enhances gap healing and osseointegration in orthopedic porous coated titanium implants: A correlative micro-computed tomographic, histomorphometric and biomechanical analysis. BMC Musculoskelet. Disord. 2022, 23, 17. [Google Scholar] [CrossRef] [PubMed]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, K.-F.; Shiu, S.-T.; Hung, C.-Y.; Chan, Y.-H.; Chee, T.-J.; Huang, P.-C.; Lai, P.-C.; Feng, S.-W. Osseointegration Potential Assessment of Bone Graft Materials Loaded with Mesenchymal Stem Cells in Peri-Implant Bone Defects. Int. J. Mol. Sci. 2024, 25, 862. https://doi.org/10.3390/ijms25020862
Tseng K-F, Shiu S-T, Hung C-Y, Chan Y-H, Chee T-J, Huang P-C, Lai P-C, Feng S-W. Osseointegration Potential Assessment of Bone Graft Materials Loaded with Mesenchymal Stem Cells in Peri-Implant Bone Defects. International Journal of Molecular Sciences. 2024; 25(2):862. https://doi.org/10.3390/ijms25020862
Chicago/Turabian StyleTseng, Kuo-Fang, Shiau-Ting Shiu, Chia-Yi Hung, Ya-Hui Chan, Tze-Jian Chee, Pai-Chun Huang, Pin-Chuang Lai, and Sheng-Wei Feng. 2024. "Osseointegration Potential Assessment of Bone Graft Materials Loaded with Mesenchymal Stem Cells in Peri-Implant Bone Defects" International Journal of Molecular Sciences 25, no. 2: 862. https://doi.org/10.3390/ijms25020862
APA StyleTseng, K.-F., Shiu, S.-T., Hung, C.-Y., Chan, Y.-H., Chee, T.-J., Huang, P.-C., Lai, P.-C., & Feng, S.-W. (2024). Osseointegration Potential Assessment of Bone Graft Materials Loaded with Mesenchymal Stem Cells in Peri-Implant Bone Defects. International Journal of Molecular Sciences, 25(2), 862. https://doi.org/10.3390/ijms25020862