
Placental Transfer Efficiency of Neutralizing Antibodies on SARS-CoV-2 Vaccination before and after Pregnancy in Mexican Women
 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Study Population
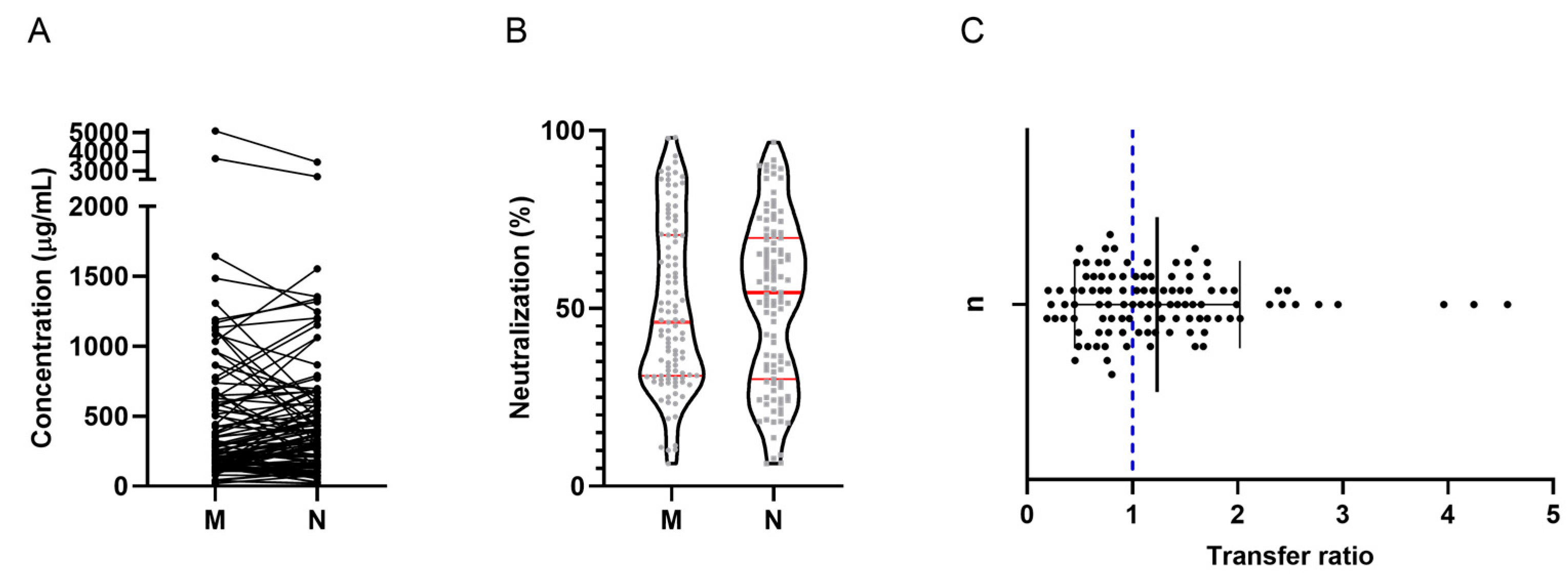
2.2. Binding IgG Antibody Response According to ELISA
2.3. Neutralizing Antibody Response by Flow Cytometry
2.4. Effect of the Number of Doses on Placental Transfer Efficiency
2.5. Effect of Gestational Age on Placental Transfer Efficiency
2.6. Association between Latency since Last Immunization and Placental Transfer Efficiency
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Samples Collection
4.3. Detection of Anti-SARS-CoV-2 IgG Antibodies (Spike Trimer) with ELISA
4.4. Detection of Anti-SARS-CoV-2 Neutralizing Antibodies by Flow Cytometry
4.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faust, J.S.; Rasmussen, S.A.; Jamieson, D.J. Pregnancy Should Be a Condition Eligible for Additional Doses of COVID-19 Messenger RNA Vaccines. Am. J. Obstet. Gynecol. MFM 2023, 138, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Joseph, N.T.; Dude, C.M.; Verkerke, H.P.; Irby, L.S.; Dunlop, A.L.; Patel, R.M.; Easley, K.A.; Smith, A.K.; Stowell, S.R.; Jamieson, D.J.; et al. Maternal Antibody Response, Neutralizing Potency, and Placental Antibody Transfer after Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Obstet. Gynecol. 2021, 138, 189. [Google Scholar] [CrossRef]
- Pham, A.; Aronoff, D.M.; Thompson, J.L. Maternal COVID-19, Vaccination Safety in Pregnancy, and Evidence of Protective Immunity. J. Allergy Clin. Immunol. 2021, 148, 728. [Google Scholar] [CrossRef]
- Lumbreras-Marquez, M.I.; Fields, K.G.; Campos-Zamora, M.; Rodriguez-Bosch, M.R.; Rodriguez-Sibaja, M.J.; Copado-Mendoza, D.Y.; Acevedo-Gallegos, S.; Farber, M.K. A Forecast of Maternal Deaths with and without Vaccination of Pregnant Women against COVID-19 in Mexico. Int. J. Gynaecol. Obstet. 2021, 154, 566–567. [Google Scholar] [CrossRef]
- Zhang, Z.; Mateus, J.; Coelho, C.H.; Dan, J.M.; Moderbacher, C.R.; Gálvez, R.I.; Cortes, F.H.; Grifoni, A.; Tarke, A.; Chang, J.; et al. Humoral and Cellular Immune Memory to Four COVID-19 Vaccines. Cell 2022, 185, 2434. [Google Scholar] [CrossRef] [PubMed]
- Kabarkouhi, Z.; Mehrarya, M.; Gharehchelou, B.; Jalilian, Z.; Jalili, R.; Wintrasiri, M.N.; Mozafari, M.R. Liposome, Nanoliposome and Allied Technologies in COVID-19 Vaccines: Key Roles and Functionalities. Curr. Drug Deliv. 2022, 20, 3–7. [Google Scholar] [CrossRef]
- Badell, M.L.; Dude, C.M.; Rasmussen, S.A.; Jamieson, D.J. State of the Art Review: COVID-19 Vaccination in Pregnancy. BMJ 2022, 378, e069741. [Google Scholar] [CrossRef]
- Munoz, F.M.; Posavad, C.M.; Richardson, B.A.; Badell, M.L.; Bunge, K.E.; Mulligan, M.J.; Parameswaran, L.; Kelly, C.W.; Olson-Chen, C.; Novak, R.M.; et al. COVID-19 Booster Vaccination during Pregnancy Enhances Maternal Binding and Neutralizing Antibody Responses and Transplacental Antibody Transfer to the Newborn. Vaccine 2023, 41, 5296–5303. [Google Scholar] [CrossRef]
- Atyeo, C.; Pullen, K.M.; Bordt, E.A.; Fischinger, S.; Burke, J.; Michell, A.; Slein, M.D.; Loos, C.; Shook, L.L.; Boatin, A.A.; et al. Compromised SARS-CoV-2-Specific Placental Antibody Transfer. Cell 2021, 184, 628–642.e10. [Google Scholar] [CrossRef]
- Edlow, A.G.; Li, J.Z.; Collier, A.R.Y.; Atyeo, C.; James, K.E.; Boatin, A.A.; Gray, K.J.; Bordt, E.A.; Shook, L.L.; Yonker, L.M.; et al. Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2030455. [Google Scholar] [CrossRef]
- Flannery, D.D.; Gouma, S.; Dhudasia, M.B.; Mukhopadhyay, S.; Pfeifer, M.R.; Woodford, E.C.; Triebwasser, J.E.; Gerber, J.S.; Morris, J.S.; Weirick, M.E.; et al. Assessment of Maternal and Neonatal Cord Blood SARS-CoV-2 Antibodies and Placental Transfer Ratios. JAMA Pediatr. 2021, 175, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.C.; Leung, B.W.; Ma, T.; Yu, F.N.Y.; Kong, C.W.; Lo, T.K.; So, P.L.; Leung, W.C.; Shu, W.; Cheung, K.W.; et al. Relationship between Viral Load, Infection-to-Delivery Interval and Mother-to-Child Transfer of Anti-SARS-CoV-2 Antibodies. Ultrasound Obstet. Gynecol. 2021, 57, 974–978. [Google Scholar] [CrossRef]
- Beharier, O.; Mayo, R.P.; Raz, T.; Sacks, K.N.; Schreiber, L.; Suissa-Cohen, Y.; Chen, R.; Gomez-Tolub, R.; Hadar, E.; Gabbay-Benziv, R.; et al. Efficient Maternal to Neonatal Transfer of Antibodies against SARS-CoV-2 and BNT162b2 MRNA COVID-19 Vaccine. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Nir, O.; Schwartz, A.; Toussia-Cohen, S.; Leibovitch, L.; Strauss, T.; Asraf, K.; Doolman, R.; Sharabi, S.; Cohen, C.; Lustig, Y.; et al. Maternal-Neonatal Transfer of SARS-CoV-2 Immunoglobulin G Antibodies among Parturient Women Treated with BNT162b2 Messenger RNA Vaccine during Pregnancy. Am. J. Obstet. Gynecol. MFM 2021, 4, 100492. [Google Scholar] [CrossRef] [PubMed]
- Rottenstreich, A.; Zarbiv, G.; Oiknine-Djian, E.; Zigron, R.; Wolf, D.G.; Porat, S. Efficient Maternofetal Transplacental Transfer of Anti- SARS-CoV-2 Spike Antibodies after Antenatal SARS-CoV-2 BNT162b2 MRNA Vaccination. Clin. Infect. Dis. 2021, 73, 1909–1912. [Google Scholar] [CrossRef]
- Sawry, S.; Le Roux, J.; Wolter, N.; Mbatha, P.; Bhiman, J.; Balkus, J.; von Gottberg, A.; Cohen, C.; Chersich, M.; Kekana, M.; et al. High Prevalence of SARS-CoV-2 Antibodies in Pregnant Women after the Second Wave of Infections in the Inner-City of Johannesburg, Gauteng Province, South Africa. Int. J. Infect. Dis. 2022, 125, 241. [Google Scholar] [CrossRef] [PubMed]
- Atyeo, C.G.; Shook, L.L.; Brigida, S.; De Guzman, R.M.; Demidkin, S.; Muir, C.; Akinwunmi, B.; Baez, A.M.; Sheehan, M.L.; McSweeney, E.; et al. Maternal Immune Response and Placental Antibody Transfer after COVID-19 Vaccination across Trimester and Platforms. Nat. Commun. 2022, 13, 3571. [Google Scholar] [CrossRef]
- Janha, R.E.; Bah, A.; Jah, H.; Touray, F.; Idris, Y.; Keita, S.; Gaye, Y.; Jallow, S.; Faye-Joof, T.; Njie, B.; et al. SARS-CoV-2 Seroprevalence in Pregnant Women during the First Three COVID-19 Waves in The Gambia. Int. J. Infect. Dis. 2023, 135, 109–117. [Google Scholar] [CrossRef]
- Kugelman, N.; Nahshon, C.; Shaked-Mishan, P.; Kleifeld, S.; Cohen, N.; Sher, M.L.; Zahran, H.; Barsha, H.; Assaf, W.; Shalabna, E.; et al. Maternal and Neonatal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Immunoglobulin G Levels after the Pfizer-BioNTech Booster Dose for Coronavirus Disease 2019 (COVID-19) Vaccination during the Second Trimester of Pregnancy. Obstet. Gynecol. 2022, 140, 187–193. [Google Scholar] [CrossRef]
- Marshall, N.E.; Blanton, M.B.; Doratt, B.M.; Malherbe, D.C.; Rincon, M.; True, H.; Mcdonald, T.; Beauregard, C.; Adatorwovor, R.; Messaoudi, I. SARS-CoV-2 vaccine booster elicits robust prolonged maternal antibody 1 responses and passive transfer via the placenta and breastmilk. bioRxiv 2022. [Google Scholar] [CrossRef]
- Mithal, L.B.; Otero, S.; Shanes, E.D.; Goldstein, J.A.; Miller, E.S. Cord Blood Antibodies Following Maternal Coronavirus Disease 2019 Vaccination during Pregnancy. Am. J. Obstet. Gynecol. 2021, 225, 192–194. [Google Scholar] [CrossRef] [PubMed]
- Prahl, M.; Golan, Y.; Cassidy, A.G.; Matsui, Y.; Li, L.; Alvarenga, B.; Chen, H.; Jigmeddagva, U.; Lin, C.Y.; Gonzalez, V.J.; et al. Evaluation of Transplacental Transfer of MRNA Vaccine Products and Functional Antibodies during Pregnancy and Infancy. Nat. Commun. 2022, 13, 4422. [Google Scholar] [CrossRef] [PubMed]
- Rottenstreich, A.; Zarbiv, G.; Oiknine-Djian, E.; Vorontsov, O.; Zigron, R.; Kleinstern, G.; Wolf, D.G.; Porat, S. Timing of SARS-CoV-2 Vaccination during the Third Trimester of Pregnancy and Transplacental Antibody Transfer: A Prospective Cohort Study. Clin. Microbiol. Infect. 2022, 28, 419. [Google Scholar] [CrossRef]
- Zdanowski, W.; Waśniewskii, T. Evaluation of SARS-CoV-2 Spike Protein Antibody Titers in Cord Blood after COVID-19 Vaccination during Pregnancy in Polish Healthcare Workers: Preliminary Results. Vaccines 2021, 9, 675. [Google Scholar] [CrossRef] [PubMed]
- Marchand, G.; Masoud, A.T.; Grover, S.; King, A.; Brazil, G.; Ulibarri, H.; Parise, J.; Arroyo, A.; Coriell, C.; Goetz, S.; et al. Maternal and Neonatal Outcomes of COVID-19 Vaccination during Pregnancy, a Systematic Review and Meta-Analysis. NPJ Vaccines 2023, 8, 103. [Google Scholar] [CrossRef]
- Prabhu, M.; Murphy, E.A.; Sukhu, A.C.; Yee, J.; Singh, S.; Eng, D.; Zhao, Z.; Riley, L.E.; Yang, Y.J. Antibody Response to Coronavirus Disease 2019 (COVID-19) Messenger RNA Vaccination in Pregnant Women and Transplacental Passage Into Cord Blood. Obstet. Gynecol. 2021, 138, 278–280. [Google Scholar] [CrossRef] [PubMed]
- Barouch, D.H.; Stephenson, K.E.; Sadoff, J.; Yu, J.; Chang, A.; Gebre, M.; McMahan, K.; Liu, J.; Chandrashekar, A.; Patel, S.; et al. Durable Humoral and Cellular Immune Responses 8 Months after Ad26.COV2.S Vaccination. N. Engl. J. Med. 2021, 385, 951–953. [Google Scholar] [CrossRef]
- Pegu, A.; O’Connell, S.E.; Schmidt, S.D.; O’Dell, S.; Talana, C.A.; Lai, L.; Albert, J.; Anderson, E.; Bennett, H.; Corbett, K.S.; et al. Durability of MRNA-1273 Vaccine-Induced Antibodies against SARS-CoV-2 Variants. Science 2021, 373, 1372–1377. [Google Scholar] [CrossRef]
- Alcorta-Nuñez, F.; Pérez-Ibave, D.C.; Burciaga-Flores, C.H.; Garza, M.Á.; González-Escamilla, M.; Rodríguez-Niño, P.; González-Guerrero, J.F.; Alcorta-Garza, A.; Vidal-Gutiérrez, O.; Ramírez-Correa, G.A.; et al. SARS-CoV-2 Neutralizing Antibodies in Mexican Population: A Five Vaccine Comparison. Diagnostics 2023, 13, 1194. [Google Scholar] [CrossRef]
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E.; et al. Homologous and Heterologous COVID-19 Booster Vaccinations. N. Engl. J. Med. 2022, 386, 1046–1057. [Google Scholar] [CrossRef]
- Liu, X.; Shaw, R.H.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and Immunogenicity of Heterologous versus Homologous Prime-Boost Schedules with an Adenoviral Vectored and MRNA COVID-19 Vaccine (Com-COV): A Single-Blind, Randomised, Non-Inferiority Trial. Lancet 2021, 398, 856. [Google Scholar] [CrossRef] [PubMed]
- Barros-Martins, J.; Hammerschmidt, S.I.; Cossmann, A.; Odak, I.; Stankov, M.V.; Morillas Ramos, G.; Dopfer-Jablonka, A.; Heidemann, A.; Ritter, C.; Friedrichsen, M.; et al. Immune Responses against SARS-CoV-2 Variants after Heterologous and Homologous ChAdOx1 NCoV-19/BNT162b2 Vaccination. Nat. Med. 2021, 27, 1525. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%) | |
|---|---|
| Vaccination against COVID-19 | |
| Unvaccinated | 26 (22.8) |
| 1 dose | 18 (15.8) |
| 2 doses | 34 (29.8) |
| 3 doses | 33 (28.9) |
| 4 doses | 3 (2.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Quezada, R.; Miguel-Rodríguez, C.E.; Ramírez-Lozada, T.; Valencia-Ledezma, O.E.; Acosta-Altamirano, G. Placental Transfer Efficiency of Neutralizing Antibodies on SARS-CoV-2 Vaccination before and after Pregnancy in Mexican Women. Int. J. Mol. Sci. 2024, 25, 1516. https://doi.org/10.3390/ijms25031516
Martínez-Quezada R, Miguel-Rodríguez CE, Ramírez-Lozada T, Valencia-Ledezma OE, Acosta-Altamirano G. Placental Transfer Efficiency of Neutralizing Antibodies on SARS-CoV-2 Vaccination before and after Pregnancy in Mexican Women. International Journal of Molecular Sciences. 2024; 25(3):1516. https://doi.org/10.3390/ijms25031516
Chicago/Turabian StyleMartínez-Quezada, Rebeca, Carlos Emilio Miguel-Rodríguez, Tito Ramírez-Lozada, Omar Esteban Valencia-Ledezma, and Gustavo Acosta-Altamirano. 2024. "Placental Transfer Efficiency of Neutralizing Antibodies on SARS-CoV-2 Vaccination before and after Pregnancy in Mexican Women" International Journal of Molecular Sciences 25, no. 3: 1516. https://doi.org/10.3390/ijms25031516