
A Cross-Sectional Study of Protein Changes Associated with Dementia in Non-Obese Weight Matched Women with and without Polycystic Ovary Syndrome



Abstract
:1. Introduction
2. Results
2.1. Levels of Alzheimer’s-Related Proteins in PCOS
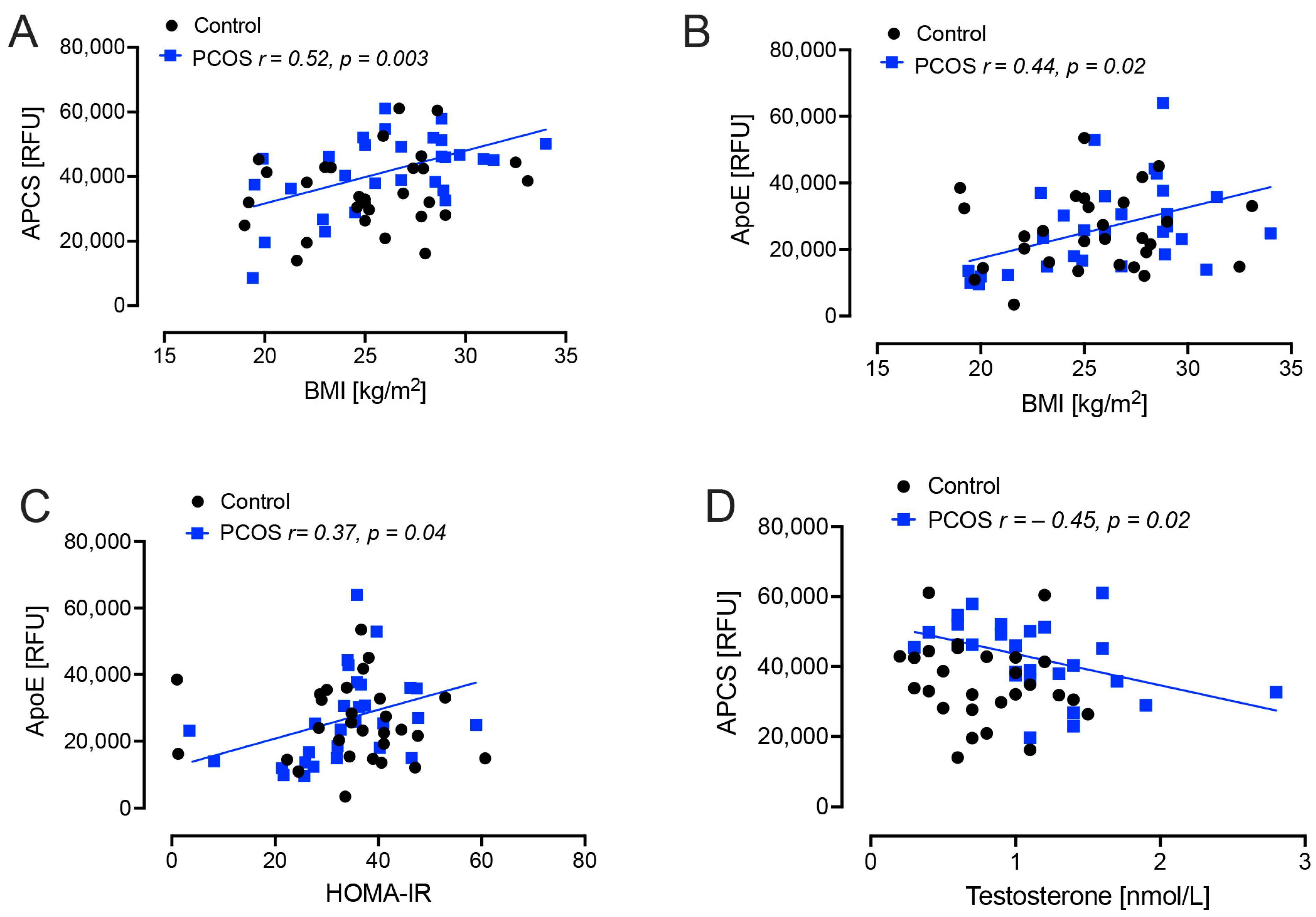
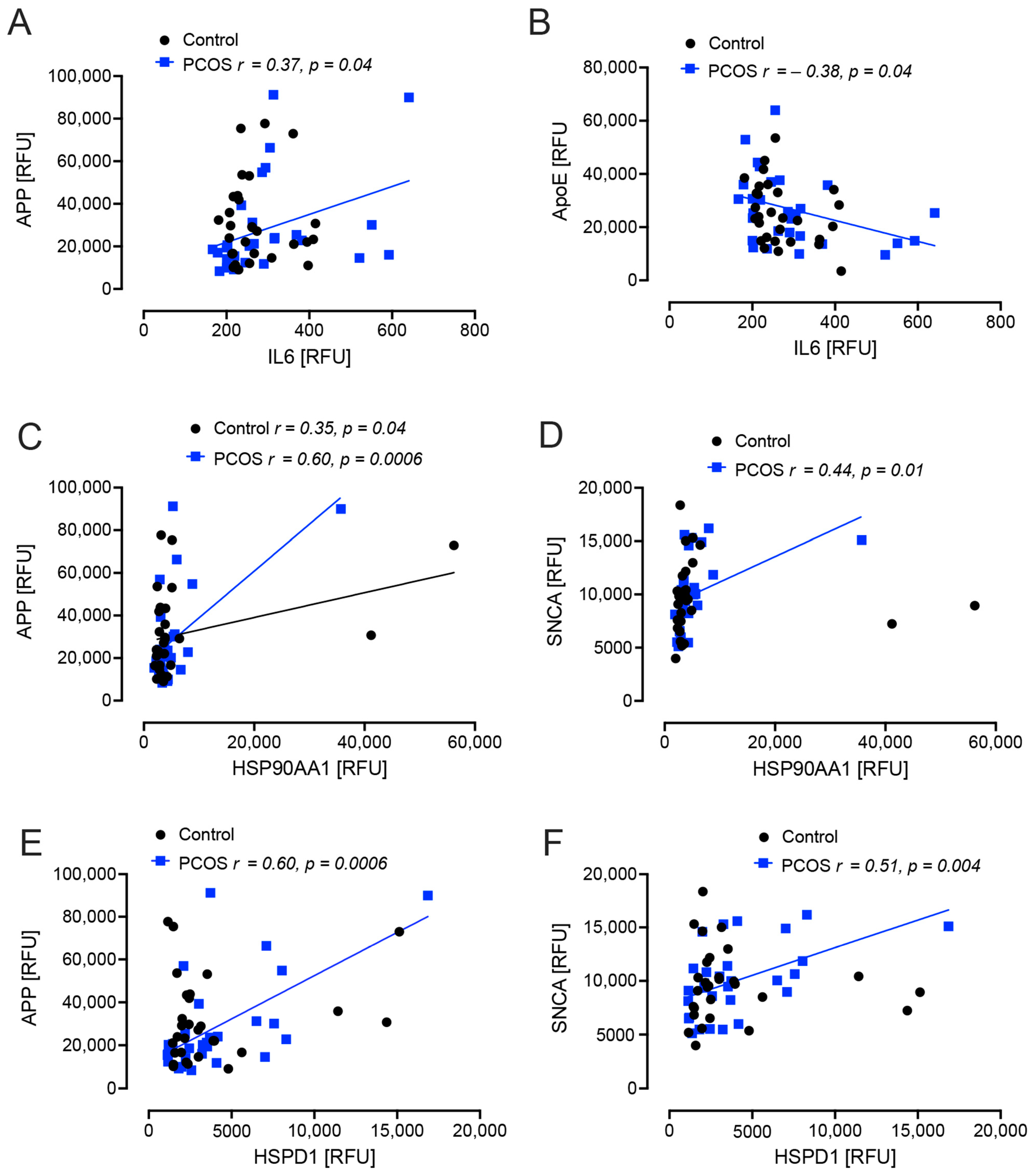
2.2. Correlation Analyses
3. Discussion
4. Materials and Methods
Study Design
5. Statistics
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sathyapalan, T.; Atkin, S.L. Recent advances in cardiovascular aspects of polycystic ovary syndrome. Eur. J. Endocrinol./Eur. Fed. Endocr. Soc. 2012, 166, 575–583. [Google Scholar] [CrossRef]
- Armanini, D.; Boscaro, M.; Bordin, L.; Sabbadin, C. Controversies in the Pathogenesis, Diagnosis and Treatment of PCOS: Focus on Insulin Resistance, Inflammation, and Hyperandrogenism. Int. J. Mol. Sci. 2022, 23, 4110. [Google Scholar] [CrossRef]
- Brutocao, C.; Zaiem, F.; Alsawas, M.; Morrow, A.S.; Murad, M.H.; Javed, A. Psychiatric disorders in women with polycystic ovary syndrome: A systematic review and meta-analysis. Endocrine 2018, 62, 318–325. [Google Scholar] [CrossRef]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The global prevalence of dementia: A systematic review and metaanalysis. Alzheimer’s Dement. 2013, 9, 63–75.e62. [Google Scholar] [CrossRef]
- Alzheimer’s Association. 2014 Alzheimer’s disease facts and figures. Alzheimer’s Dement. 2014, 10, e47–e92. [Google Scholar]
- Picone, P.; Di Carlo, M.; Nuzzo, D. Obesity and Alzheimer’s disease: Molecular bases. Eur. J. Neurosci. 2020, 52, 3944–3950. [Google Scholar] [CrossRef]
- Sedzikowska, A.; Szablewski, L. Insulin and Insulin Resistance in Alzheimer’s Disease. Int. J. Mol. Sci. 2021, 22, 9987. [Google Scholar] [CrossRef] [PubMed]
- Talbot, K.; Wang, H.-Y.; Kazi, H.; Han, L.-Y.; Bakshi, K.P.; Stucky, A.; Fuino, R.L.; Kawaguchi, K.R.; Samoyedny, A.J.; Wilson, R.S.; et al. Demonstrated brain insulin resistance in Alzheimer’s disease patients is associated with IGF-1 resistance, IRS-1 dysregulation, and cognitive decline. J. Clin. Investig. 2012, 122, 1316–1338. [Google Scholar] [CrossRef] [PubMed]
- Ly, M.; Yu, G.Z.; Mian, A.; Cramer, A.; Meysami, S.; Merrill, D.A.; Samara, A.; Eisenstein, S.A.; Hershey, T.; Babulal, G.M.; et al. Neuroinflammation: A Modifiable Pathway Linking Obesity, Alzheimer’s disease, and Depression. Am. J. Geriatr. Psychiatry 2023, 31, 853–866. [Google Scholar] [CrossRef] [PubMed]
- Ott, A.; Stolk, R.P.; van Harskamp, F.; Pols, H.A.; Hofman, A.; Breteler, M.M. Diabetes mellitus and the risk of dementia: The Rotterdam Study. Neurology 1999, 53, 1937–1942. [Google Scholar] [CrossRef] [PubMed]
- Sims-Robinson, C.; Kim, B.; Rosko, A.; Feldman, E.L. How does diabetes accelerate Alzheimer disease pathology? Nat. Rev. Neurol. 2010, 6, 551–559. [Google Scholar] [CrossRef]
- Zilkens, R.R.; Davis, W.A.; Spilsbury, K.; Semmens, J.B.; Bruce, D.G. Earlier age of dementia onset and shorter survival times in dementia patients with diabetes. Am. J. Epidemiol. 2013, 177, 1246–1254. [Google Scholar] [CrossRef]
- Moin, A.S.M.; Al-Qaissi, A.; Sathyapalan, T.; Atkin, S.L.; Butler, A.E. Hypoglycaemia in type 2 diabetes exacerbates amyloid-related proteins associated with dementia. Diabetes Obes. Metab. 2021, 23, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Butler, A.E.; Moin AS, M.; Sathyapalan, T.; Atkin, S.L. A Cross-Sectional Study of Alzheimer-Related Proteins in Women with Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2024, 25, 1158. [Google Scholar] [CrossRef] [PubMed]
- Kakoly, N.S.; Khomami, M.B.; Joham, A.E.; Cooray, S.D.; Misso, M.L.; Norman, R.J.; Harrison, C.L.; Ranasinha, S.; Teede, H.J.; Moran, L.J. Ethnicity, obesity and the prevalence of impaired glucose tolerance and type 2 diabetes in PCOS: A systematic review and meta-regression. Hum. Reprod. Update 2018, 24, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Sarahian, N.; Sarvazad, H.; Sajadi, E.; Rahnejat, N.; Eskandari Roozbahani, N. Investigation of common risk factors between polycystic ovary syndrome and Alzheimer’s disease: A narrative review. Reprod. Health 2021, 18, 156. [Google Scholar] [CrossRef] [PubMed]
- Barber, T.M.; Kyrou, I.; Randeva, H.S.; Weickert, M.O. Mechanisms of Insulin Resistance at the Crossroad of Obesity with Associated Metabolic Abnormalities and Cognitive Dysfunction. Int. J. Mol. Sci. 2021, 22, 546. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Hu, J.; Zhang, S.; Fan, W.; Wen, L.; Wang, G.; Zhang, D. Changes in Resting-State Cerebral Activity in Women With Polycystic Ovary Syndrome: A Functional MR Imaging Study. Front. Endocrinol. 2020, 11, 603279. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.; Li, X.; Zhu, H.; Zhu, X.; Tan, H.; Feng, P.; Chen, L.; Luo, C. Plasma luteinizing hormone level affects the brain activity of patients with polycystic ovary syndrome. Psychoneuroendocrinology 2020, 112, 104535. [Google Scholar] [CrossRef]
- Schattmann, L.; Sherwin, B.B. Testosterone levels and cognitive functioning in women with polycystic ovary syndrome and in healthy young women. Horm. Behav. 2007, 51, 587–596. [Google Scholar] [CrossRef]
- Macut, D.; Bjekić-Macut, J.; Rahelić, D.; Doknić, M. Insulin and the polycystic ovary syndrome. Diabetes Res. Clin. Pract. 2017, 130, 163–170. [Google Scholar] [CrossRef]
- Teunissen, C.; Del Campo, M.; Peeters, C.; Meeter, L.; Seelaar, H.; Koel-Simmelink, M.; Ramakers, I.; Middelkoop, H.; De Deyn, P.; Claessen, J. Blood-based protein biomarkers in definite frontotemporal dementia: A case-control study. 2022; preprint. [Google Scholar]
- Nishiyama, E.; Iwamoto, N.; Kimura, M.; Arai, H. Serum amyloid P component level in Alzheimer’s disease. Dementia 1996, 7, 256–259. [Google Scholar] [CrossRef]
- Verwey, N.A.; Schuitemaker, A.; van der Flier, W.M.; Mulder, S.D.; Mulder, C.; Hack, C.E.; Scheltens, P.; Blankenstein, M.A.; Veerhuis, R. Serum amyloid p component as a biomarker in mild cognitive impairment and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2008, 26, 522–527. [Google Scholar] [CrossRef]
- Roberts, J.A.; Varma, V.R.; Candia, J.; Tanaka, T.; Ferrucci, L.; Bennett, D.A.; Thambisetty, M. Unbiased proteomics and multivariable regularized regression techniques identify SMOC1, NOG, APCS, and NTN1 in an Alzheimer’s disease brain proteomic signature. NPJ Aging 2023, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Baldacci, F.; Daniele, S.; Piccarducci, R.; Giampietri, L.; Pietrobono, D.; Giorgi, F.S.; Nicoletti, V.; Frosini, D.; Libertini, P.; Lo Gerfo, A.; et al. Potential Diagnostic Value of Red Blood Cells alpha-Synuclein Heteroaggregates in Alzheimer’s Disease. Mol. Neurobiol. 2019, 56, 6451–6459. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.M.; Cho, S.J.; Jo, C.; Park, M.H.; Han, C.; Koh, Y.H. Elevation of plasma soluble amyloid precursor protein beta in Alzheimer’s disease. Arch. Gerontol. Geriatr. 2020, 87, 103995. [Google Scholar] [CrossRef] [PubMed]
- Bush, A.I.; Beyreuther, K.; Masters, C.L. Beta A4 amyloid protein and its precursor in Alzheimer’s disease. Pharmacol. Ther. 1992, 56, 97–117. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, G.; Gainder, S.; Suri, V.; Sachdeva, N.; Chopra, S. Comparison of the Different PCOS Phenotypes Based on Clinical Metabolic, and Hormonal Profile, and their Response to Clomiphene. Indian J. Endocrinol. Metab. 2019, 23, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, F.; Wang, Q.; McKay, N.S.; Keefe, S.; Hantler, N.; Hornbeck, R.; Wang, Y.; Hassenstab, J.; Schindler, S.; Xiong, C.; et al. Sex-Specific Patterns of Body Mass Index Relationship with White Matter Connectivity. J. Alzheimers Dis. 2022, 86, 1831–1848. [Google Scholar] [CrossRef] [PubMed]
- Pennings, N.; Jaber, J.; Ahiawodzi, P. Ten-year weight gain is associated with elevated fasting insulin levels and precedes glucose elevation. Diabetes/Metab. Res. Rev. 2018, 34, e2986. [Google Scholar] [CrossRef]
- Akiyama, H.; Barger, S.; Barnum, S.; Bradt, B.; Bauer, J.; Cole, G.M.; Cooper, N.R.; Eikelenboom, P.; Emmerling, M.; Fiebich, B.L.; et al. Inflammation and Alzheimer’s disease. Neurobiol. Aging 2000, 21, 383–421. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Tong, M.; Hang, S.; Deochand, C.; de la Monte, S. CSF and Brain Indices of Insulin Resistance, Oxidative Stress and Neuro-Inflammation in Early versus Late Alzheimer’s Disease. J. Alzheimers Dis. Park. 2013, 3, 128. [Google Scholar] [CrossRef]
- Marriott, R.J.; Murray, K.; Flicker, L.; Hankey, G.J.; Matsumoto, A.M.; Dwivedi, G.; Antonio, L.; Almeida, O.P.; Bhasin, S.; Dobs, A.S.; et al. Lower serum testosterone concentrations are associated with a higher incidence of dementia in men: The UK Biobank prospective cohort study. Alzheimer’s Dement. 2022, 18, 1907–1918. [Google Scholar] [CrossRef] [PubMed]
- Norman, R.J.; Teede, H.J. A new evidence-based guideline for assessment and management of polycystic ovary syndrome. Med. J. Aust. 2018, 209, 299–300. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Lee, S.H. Effectiveness of Lifestyle Modification in Polycystic Ovary Syndrome Patients with Obesity: A Systematic Review and Meta-Analysis. Life 2022, 12, 308. [Google Scholar] [CrossRef]
- Ee, C.; Pirotta, S.; Mousa, A.; Moran, L.; Lim, S. Providing lifestyle advice to women with PCOS: An overview of practical issues affecting success. BMC Endocr. Disord. 2021, 21, 234. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Ma, L.; Xia, X.; Ying, T.; Zhou, M.; Zou, S.; Yu, H.; Yin, J. Efficacy of Bariatric Surgery in the Treatment of Women With Obesity and Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2022, 107, e3217–e3229. [Google Scholar] [CrossRef]
- Cunningham, T.K.; Allgar, V.; Dargham, S.R.; Kilpatrick, E.; Sathyapalan, T.; Maguiness, S.; Mokhtar Rudin, H.R.; Abdul Ghani, N.M.; Latiff, A.; Atkin, S.L. Association of Vitamin D Metabolites With Embryo Development and Fertilization in Women With and Without PCOS Undergoing Subfertility Treatment. Front. Endocrinol. 2019, 10, 13. [Google Scholar] [CrossRef]
- Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [CrossRef]
- Legro, R.S.; Arslanian, S.A.; Ehrmann, D.A.; Hoeger, K.M.; Murad, M.H.; Pasquali, R.; Welt, C.K. Diagnosis and Treatment of Polycystic Ovary Syndrome: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2013, 98, 4565–4592. [Google Scholar] [CrossRef]
- World Health Organization. Waist Circumference and Waist–Hip Ratio. Report of a WHO Expert Consultation, Geneva; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Kahal, H.; Halama, A.; Aburima, A.; Bhagwat, A.M.; Butler, A.E.; Graumann, J.; Suhre, K.; Sathyapalan, T.; Atkin, S.L. Effect of induced hypoglycemia on inflammation and oxidative stress in type 2 diabetes and control subjects. Sci. Rep. 2020, 10, 4750. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, S.; Vaught, J.D.; Bock, C.; Gold, L.; Katilius, E.; Keeney, T.R.; Kim, N.; Saccomano, N.A.; Wilcox, S.K.; Zichi, D.; et al. From SOMAmer-based biomarker discovery to diagnostic and clinical applications: A SOMAmer-based, streamlined multiplex proteomic assay. PLoS ONE 2011, 6, e26332. [Google Scholar] [CrossRef] [PubMed]
- Gold, L.; Ayers, D.; Bertino, J.; Bock, C.; Bock, A.; Brody, E.N.; Carter, J.; Dalby, A.B.; Eaton, B.E.; Fitzwater, T.; et al. Aptamer-based multiplexed proteomic technology for biomarker discovery. PLoS ONE 2010, 5, e15004. [Google Scholar] [CrossRef] [PubMed]
- Suhre, K.; Arnold, M.; Bhagwat, A.M.; Cotton, R.J.; Engelke, R.; Raffler, J.; Sarwath, H.; Thareja, G.; Wahl, A.; DeLisle, R.K.; et al. Connecting genetic risk to disease end points through the human blood plasma proteome. Nat. Commun. 2017, 8, 14357. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Control (n = 24) | PCOS (n = 24) | p-Value | |
|---|---|---|---|
| Age (years) | 32.5 ± 4.1 | 31 ± 6.4 | 0.14 |
| BMI (kg/m2) | 24.8 ± 1.1 | 25.9 ± 1.8 | 0.56 |
| Fasting glucose (nmol/L) | 4.9 ± 0.4 | 4.7 ± 0.8 | 0.06 |
| HbA1C (mmol/mol) | 30.9 ± 6.5 | 31.8 ± 3.0 | 0.9 |
| HOMA-IR | 1.8 ± 1.0 | 1.9 ± 1.6 | 0.97 |
| SHBG (nmol/L) | 104.2 ± 80.3 | 71.7 ± 62.2 | 0.01 |
| Free androgen index (FAI) | 1.3 ± 0.5 | 4.2 ± 2.9 | 0.0001 |
| CRP (mg L−1) | 2.34 ± 2.34 | 2.77 ± 2.57 | 0.43 |
| AMH (ng/mL) | 24.3 ± 13.1 | 57.2 ± 14.2 | 0.0001 |
| Control Mean (SD) | PCOS Mean (SD) | p-Value | |
|---|---|---|---|
| APP | 31,246 (19,569) | 28,300 (22,332) | 0.60 |
| SNCA | 9673 (3322) | 10,012 (3343) | 0.70 |
| APCS | 35,663 (11,717) | 41,518 (11,879) | 0.03 |
| PAPPA | 10,201 (5799) | 10,065 (4505) | 0.92 |
| MAPT | 129 (48) | 130 (36) | 0.89 |
| apoE | 25,296 (11,517) | 26,588 (13,321) | 0.69 |
| apoE2 | 214,964 (67,686) | 221,851 (56,020) | 0.68 |
| apoE3 | 148,321 (59,451) | 157,453 (59,480) | 0.56 |
| apoE4 | 170,531 (57,851) | 173,799 (63,642) | 0.84 |
| SAA | 1211 (1150) | 1585 (2774) | 0.51 |
| NOG | 3081 (1063) | 3203 (2582) | 0.82 |
| apoA1 | 12,344 (2248) | 12,392 (2448) | 0.94 |
| vWF | 11,481 (14,223) | 10,746 (9306) | 0.82 |
| FN | 18,553 (16,585) | 19,991 (12,729) | 0.71 |
| FN1.3 | 4360 (7520) | 3368 (2021) | 0.50 |
| FN1.4 | 63,653 (33,196) | 69,376 (26,468) | 0.47 |
| ECM1 | 18,037 (6143) | 19,345 (5284) | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butler, A.E.; Moin, A.S.M.; Sathyapalan, T.; Atkin, S.L. A Cross-Sectional Study of Protein Changes Associated with Dementia in Non-Obese Weight Matched Women with and without Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2024, 25, 2409. https://doi.org/10.3390/ijms25042409
Butler AE, Moin ASM, Sathyapalan T, Atkin SL. A Cross-Sectional Study of Protein Changes Associated with Dementia in Non-Obese Weight Matched Women with and without Polycystic Ovary Syndrome. International Journal of Molecular Sciences. 2024; 25(4):2409. https://doi.org/10.3390/ijms25042409
Chicago/Turabian StyleButler, Alexandra E., Abu Saleh Md Moin, Thozhukat Sathyapalan, and Stephen L. Atkin. 2024. "A Cross-Sectional Study of Protein Changes Associated with Dementia in Non-Obese Weight Matched Women with and without Polycystic Ovary Syndrome" International Journal of Molecular Sciences 25, no. 4: 2409. https://doi.org/10.3390/ijms25042409
APA StyleButler, A. E., Moin, A. S. M., Sathyapalan, T., & Atkin, S. L. (2024). A Cross-Sectional Study of Protein Changes Associated with Dementia in Non-Obese Weight Matched Women with and without Polycystic Ovary Syndrome. International Journal of Molecular Sciences, 25(4), 2409. https://doi.org/10.3390/ijms25042409