
Obesity-Related Kidney Disease: A Growing Threat to Renal Health
 , , , ,
, , , ,  and
and {kind=link}
{kind=link}
Abstract
1. Introduction
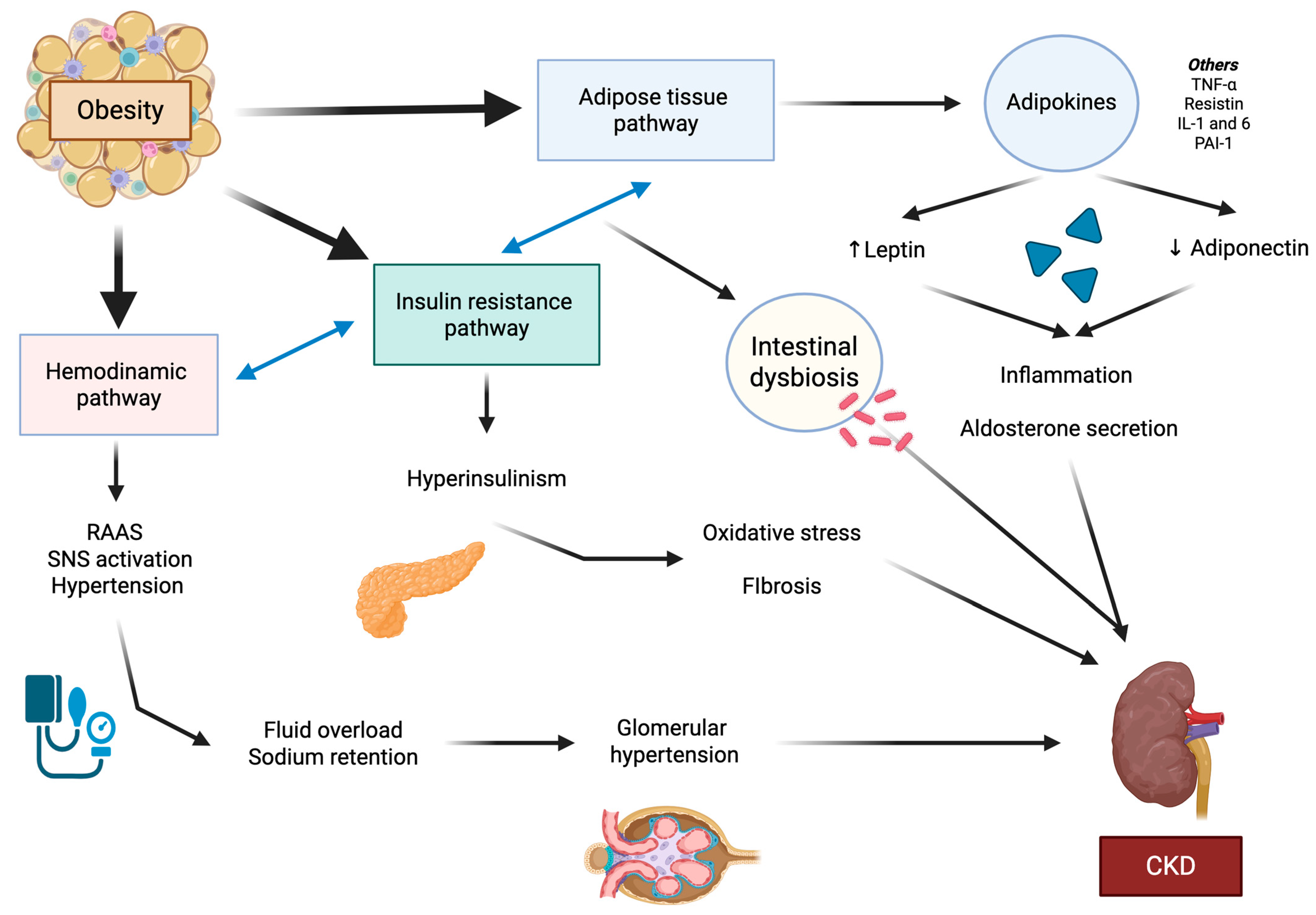
2. Mechanisms Underlying Chronic Kidney Disease Development in Obesity
2.1. The Hemodynamic Pathway
2.2. Adipose Tissue-Related Pathway
2.3. Insulin Resistance–Hyperinsulinism Pathway
3. Effect of Obesity on Kidney
4. Obesity and Cardiovascular–Kidney–Metabolic Syndrome
5. Obesity, Diabetes, and Their Link with Kidney Disease
6. Challenges of New Management Options for Obesity and Kidney Disease
6.1. Lifestyle Interventions and Traditional Drugs
6.2. The Emerging Treatments of Cardiovascular–Kidney–Metabolic Syndrome: Incretin-Based Therapies and Gliflozins
6.3. Bariatric Surgery and Alternative Weight Loss Procedures
6.4. Emerging Frontiers
6.5. Challenges
6.6. Future Directions
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lingvay, I.; Cohen, R.V.; le Roux, C.W.; Sumithran, P. Obesity in adults. Lancet 2024, 404, 972–987. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. News-Room Fact-Sheets Detail Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 7 June 2025).
- Ng, M.; Gakidou, E.; Lo, J.; Abate, Y.H.; Abbafati, C.; Abbas, N.; Abbasian, M.; Abd ElHafeez, S.; Abdel-Rahman, W.M.; Abd-Elsalam, S.; et al. Global, regional, and national prevalence of adult overweight and obesity, 1990–2021, with forecasts to 2050: A forecasting study for the Global Burden of Disease Study 2021. Lancet 2025, 405, 813–838. [Google Scholar] [CrossRef] [PubMed]
- Kaboré, S.; Millogo, T.; Soubeiga, J.K.; Lanou, H.; Bicaba, B.; Kouanda, S. Prevalence and risk factors for overweight and obesity: A cross-sectional countrywide study in Burkina Faso. BMJ Open 2020, 10, e032953. [Google Scholar] [CrossRef] [PubMed]
- Yau, K.; Kuah, R.; Cherney, D.Z.I.; Lam, T.K.T. Obesity and the kidney: Mechanistic links and therapeutic advances. Nat. Rev. Endocrinol. 2024, 20, 321–335. [Google Scholar] [CrossRef]
- Rubino, F.; Cummings, D.E.; Eckel, R.H.; Cohen, R.V.; Wilding, J.P.H.; Brown, W.A.; Stanford, F.C.; Batterham, R.L.; Farooqi, I.S.; Farpour-Lambert, N.J.; et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025, 13, 221–262. [Google Scholar] [CrossRef]
- Després, J.-P. Body Fat Distribution and Risk of Cardiovascular Disease: An update. Circulation 2012, 126, 1301–1313. [Google Scholar] [CrossRef]
- Busetto, L.; Dicker, D.; Frühbeck, G.; Halford, J.C.G.; Sbraccia, P.; Yumuk, V.; Goossens, G.H. A new framework for the diagnosis, staging and management of obesity in adults. Nat. Med. 2024, 30, 2395–2399. [Google Scholar] [CrossRef]
- Bremner, J.D.; Moazzami, K.; Wittbrodt, M.T.; Nye, J.A.; Lima, B.B.; Gillespie, C.F.; Rapaport, M.H.; Pearce, B.D.; Shah, A.J.; Vaccarino, V. Diet, Stress and Mental Health. Nutrients 2020, 12, 2428. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef]
- Zhang, X.; Ma, N.; Lin, Q.; Chen, K.; Zheng, F.; Wu, J.; Dong, X.; Niu, W. Body Roundness Index and All-Cause Mortality Among US Adults. JAMA Netw. Open 2024, 7, e2415051. [Google Scholar] [CrossRef] [PubMed]
- Frühbeck, G.; Busetto, L.; Dicker, D.; Yumuk, V.; Goossens, G.H.; Hebebrand, J.; Halford, J.G.; Farpour-Lambert, N.J.; Blaak, E.E.; Woodward, E.; et al. The ABCD of Obesity: An EASO Position Statement on a Diagnostic Term with Clinical and Scientific Implications. Obes. Facts 2019, 12, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Kovesdy, C.; Langham, R.; Rosenberg, M.; Jha, V.; Zoccali, C. A single number for advocacy and communication—Worldwide more than 850 million individuals have kidney diseases. Kidney Int. 2019, 96, 1048–1050. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P. Epidemiology of Chronic Kidney Disease: An Update in Kidney International Supplements; Elsevier B.V.: Amsterdam, The Netherlands, 2022; Volume 12, pp. 7–11. [Google Scholar]
- Chang, A.R.; Grams, M.E.; Ballew, S.H.; Bilo, H.; Correa, A.; Evans, M.; Gutierrez, O.M.; Hosseinpanah, F.; Iseki, K.; Kenealy, T.; et al. Adiposity and risk of decline in glomerular filtration rate: Meta-analysis of individual participant data in a global consortium. BMJ 2019, 364, k5301. [Google Scholar] [CrossRef]
- García-Carro, C.; Vergara, A.; Bermejo, S.; Azancot, M.A.; Sellarés, J.; Soler, M.J. A Nephrologist Perspective on Obesity: From Kidney Injury to Clinical Management. Front. Med. 2021, 8, 655871. [Google Scholar] [CrossRef]
- Griffin, K.A.; Kramer, H.; Bidani, A.K. Adverse renal consequences of obesity. Am. J. Physiol.-Ren. Physiol. 2008, 294, F685–F696. [Google Scholar] [CrossRef]
- Xu, X.; Huang, X.; Zhang, L.; Huang, X.; Qin, Z.; Hua, F. Adiponectin protects obesity-related glomerulopathy by inhibiting ROS/NF-κB/NLRP3 inflammation pathway. BMC Nephrol. 2021, 22, 218. [Google Scholar] [CrossRef]
- Hall, J.E.; do Carmo, J.M.; da Silva, A.A.; Wang, Z.; Hall, M.E. Obesity-Induced Hypertension. Circ. Res. 2015, 116, 991–1006. [Google Scholar] [CrossRef]
- Perdomo, C.M.; Cohen, R.V.; Sumithran, P.; Clément, K.; Frühbeck, G. Contemporary medical, device, and surgical therapies for obesity in adults. Lancet 2023, 401, 1116–1130. [Google Scholar] [CrossRef]
- Soták, M.; Clark, M.; Suur, B.E.; Börgeson, E. Inflammation and resolution in obesity. Nat. Rev. Endocrinol. 2025, 21, 45–61. [Google Scholar] [CrossRef]
- Hall, J.E.; do Carmo, J.M.; da Silva, A.A.; Wang, Z.; Hall, M.E. Obesity, kidney dysfunction and hypertension: Mechanistic links. Nat. Rev. Nephrol. 2019, 15, 367–385. [Google Scholar] [CrossRef] [PubMed]
- Briffa, J.F.; McAinch, A.J.; Poronnik, P.; Hryciw, D.H. Adipokines as a link between obesity and chronic kidney disease. Am. J. Physiol. Physiol. 2013, 305, F1629–F1636. [Google Scholar] [CrossRef] [PubMed]
- Przybyciński, J.; Dziedziejko, V.; Puchałowicz, K.; Domański, L.; Pawlik, A. Adiponectin in Chronic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 9375. [Google Scholar] [CrossRef] [PubMed]
- Meyvis, K.; Verrijken, A.; Wouters, K.; Van Gaal, L. Plasma adiponectin level is inversely correlated with albuminuria in overweight and obese nondiabetic individuals. Metabolism 2013, 62, 1570–1576. [Google Scholar] [CrossRef]
- Fang, F.; Bae, E.H.; Hu, A.; Liu, G.C.; Zhou, X.; Williams, V.; Maksimowski, N.; Lu, C.; Konvalinka, A.; John, R.; et al. Deletion of the gene for adiponectin accelerates diabetic nephropathy in the Ins2 +/C96Y mouse. Diabetologia 2015, 58, 1668–1678. [Google Scholar] [CrossRef]
- Considine, R.V. Increased Serum Leptin Indicates Leptin Resistance in Obesity. Clin. Chem. 2011, 57, 1461–1462. [Google Scholar] [CrossRef]
- Zhao, J.; Rui, H.; Yang, M.; Sun, L.; Dong, H.; Cheng, H. CD36-Mediated Lipid Accumulation and Activation of NLRP3 Inflammasome Lead to Podocyte Injury in Obesity-Related Glomerulopathy. Mediat. Inflamm. 2019, 2019, 3172647. [Google Scholar]
- Rampanelli, E.; Orsó, E.; Ochodnicky, P.; Liebisch, G.; Bakker, P.J.; Claessen, N.; Butter, L.M.; Weerman, M.A.v.D.B.; Florquin, S.; Schmitz, G.; et al. Metabolic injury-induced NLRP3 inflammasome activation dampens phospholipid degradation. Sci. Rep. 2017, 7, 2861. [Google Scholar] [CrossRef]
- Ke, B.; Shen, W.; Fang, X.; Wu, Q. The NLPR3 inflammasome and obesity-related kidney disease. J. Cell. Mol. Med. 2017, 22, 16–24. [Google Scholar] [CrossRef]
- Yamamoto, T.; Takabatake, Y.; Takahashi, A.; Kimura, T.; Namba, T.; Matsuda, J.; Minami, S.; Kaimori, J.-Y.; Matsui, I.; Matsusaka, T.; et al. High-Fat Diet–Induced Lysosomal Dysfunction and Impaired Autophagic Flux Contribute to Lipotoxicity in the Kidney. J. Am. Soc. Nephrol. 2017, 28, 1534–1551. [Google Scholar] [CrossRef]
- Jiang, Z.; Wang, Y.; Zhao, X.; Cui, H.; Han, M.; Ren, X.; Gang, X.; Wang, G. Obesity and chronic kidney disease. Am. J. Physiol.-Endocrinol. Metab. 2023, 324, E24–E41. [Google Scholar] [CrossRef] [PubMed]
- Lovre, D.; Shah, S.; Sihota, A.; Fonseca, V.A. Managing Diabetes and Cardiovascular Risk in Chronic Kidney Disease Patients. Endocrinol. Metab. Clin. North Am. 2018, 47, 237–257. [Google Scholar] [CrossRef] [PubMed]
- Popkov, V.A.; Zharikova, A.A.; Demchenko, E.A.; Andrianova, N.V.; Zorov, D.B.; Plotnikov, E.Y. Gut Microbiota as a Source of Uremic Toxins. Int. J. Mol. Sci. 2022, 23, 483. [Google Scholar] [CrossRef] [PubMed]
- López-Contreras, B.E.; Morán-Ramos, S.; Villarruel-Vázquez, R.; Macías-Kauffer, L.; Villamil-Ramírez, H.; León-Mimila, P.; Vega-Badillo, J.; Sánchez-Muñoz, F.; Llanos-Moreno, L.E.; Canizalez-Román, A.; et al. Composition of gut microbiota in obese and normal-weight Mexican school-age children and its association with metabolic traits. Pediatr. Obes. 2018, 13, 381–388. [Google Scholar] [CrossRef]
- Arneth, B. Mechanisms of Insulin Resistance in Patients with Obesity. Endocrines 2024, 5, 153–165. [Google Scholar] [CrossRef]
- Piwkowska, A.; Rogacka, D.; Kasztan, M.; Angielski, S.; Jankowski, M. Insulin increases glomerular filtration barrier permeability through dimerization of protein kinase G type Iα subunits. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2013, 1832, 791–804. [Google Scholar] [CrossRef]
- Coward, R.; Fornoni, A. Insulin signaling. Curr. Opin. Nephrol. Hypertens. 2015, 24, 104–110. [Google Scholar] [CrossRef]
- Welsh, G.I.; Hale, L.J.; Eremina, V.; Jeansson, M.; Maezawa, Y.; Lennon, R.; Pons, D.A.; Owen, R.J.; Satchell, S.C.; Miles, M.J.; et al. Insulin Signaling to the Glomerular Podocyte Is Critical for Normal Kidney Function. Cell Metab. 2010, 12, 329–340. [Google Scholar] [CrossRef]
- Wasik, A.A.; Lehtonen, S. Glucose Transporters in Diabetic Kidney Disease—Friends or Foes? Front. Endocrinol. 2018, 9, 155. [Google Scholar] [CrossRef]
- Brauer, M.; A Roth, G.; Aravkin, A.Y.; Zheng, P.; Abate, K.H.; Abate, Y.H.; Abbafati, C.; Abbasgholizadeh, R.; Abbasi, M.A.; Abbasian, M.; et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2162–2203. [Google Scholar] [CrossRef]
- Segev, D.L.; Simpkins, C.E.; Thompson, R.E.; Locke, J.E.; Warren, D.S.; Montgomery, R.A. Obesity Impacts Access to Kidney Transplantation. J. Am. Soc. Nephrol. 2008, 19, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Jay, C.; Schold, J.D. Measuring Transplant Center Performance: The Goals Are Not Controversial but the Methods and Consequences Can Be. Curr. Transplant. Rep. 2017, 4, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Valizadeh, M.; Ahmadi, A.R.; Abbaspour, F.; Valizadeh, A.; Syed Hasani, A.H.; Moteshakereh, S.M.; Nikoohemmat, M.; Abiri, B. The risk of kidney dysfunction in metabolically healthy/unhealthy population with normal weight or overweight/obesity: A systematic review and meta-analysis. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2024, 29, 69. [Google Scholar] [CrossRef]
- de Vries, A.P.J.; Ruggenenti, P.; Ruan, X.Z.; Praga, M.; Cruzado, J.M.; Bajema, I.M.; D’AGati, V.D.; Lamb, H.J.; Barlovic, D.P.; Hojs, R.; et al. Fatty kidney: Emerging role of ectopic lipid in obesity-related renal disease. Lancet Diabetes Endocrinol. 2014, 2, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P.; Furth, S.L.; Zoccali, C.; World Kidney Day Steering Committee. Obesity and kidney disease: Hidden consequences of the epidemic. Kidney Int. 2017, 91, 260–262. [Google Scholar] [CrossRef]
- D’AGati, V.D.; Chagnac, A.; de Vries, A.P.; Levi, M.; Porrini, E.; Herman-Edelstein, M.; Praga, M. Obesity-related glomerulopathy: Clinical and pathologic characteristics and pathogenesis. Nat. Rev. Nephrol. 2016, 12, 453–471. [Google Scholar] [CrossRef]
- Tsuboi, N.; Okabayashi, Y.; Shimizu, A.; Yokoo, T. The Renal Pathology of Obesity. Kidney Int. Rep. 2017, 2, 251–260. [Google Scholar] [CrossRef]
- Nawaz, S.; Chinnadurai, R.; Al-Chalabi, S.; Evans, P.; Kalra, P.A.; Syed, A.A.; Sinha, S. Obesity and chronic kidney disease: A current review. Obes. Sci. Pract. 2023, 9, 61–74. [Google Scholar] [CrossRef]
- Kambham, N.; Markowitz, G.S.; Valeri, A.M.; Lin, J.; D’AGati, V.D. Obesity-related glomerulopathy: An emerging epidemic. Kidney Int. 2001, 59, 1498–1509. [Google Scholar] [CrossRef]
- Navarro-Díaz, M.; López-Martínez, M. The Role of miRNAs as Early Biomarkers in Obesity-Related Glomerulopathy: Implications for Early Detection and Treatment. Biomedicines 2025, 13, 1030. [Google Scholar] [CrossRef]
- Kriz, W.; Lemley, K.V. A Potential Role for Mechanical Forces in the Detachment of Podocytes and the Progression of CKD. J. Am. Soc. Nephrol. 2015, 26, 258–269. [Google Scholar] [CrossRef]
- López-Martínez, M.; Armengol, M.P.; Pey, I.; Farré, X.; Rodríguez-Martínez, P.; Ferrer, M.; Porrini, E.; Luis-Lima, S.; Díaz-Martín, L.; Rodríguez-Rodríguez, A.E.; et al. Integrated miRNA–mRNA Analysis Reveals Critical miRNAs and Targets in Diet-Induced Obesity-Related Glomerulopathy. Int. J. Mol. Sci. 2024, 25, 6437. [Google Scholar] [CrossRef] [PubMed]
- Koskinas, K.C.; Van Craenenbroeck, E.M.; Antoniades, C.; Blüher, M.; Gorter, T.M.; Hanssen, H.; Marx, N.; McDonagh, T.A.; Mingrone, G.; Rosengren, A.; et al. Obesity and cardiovascular disease: An ESC clinical consensus statement. Eur. Heart J. 2024, 45, 4063–4098. [Google Scholar] [CrossRef] [PubMed]
- Polkinghorne, M.D.; West, H.W.; Antoniades, C. Adipose Tissue in Cardiovascular Disease: From Basic Science to Clinical Translation. Annu. Rev. Physiol. 2024, 86, 175–198. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. The changing landscape of atherosclerosis. Nature 2021, 592, 524–533. [Google Scholar] [CrossRef]
- Lopez-Jimenez, F.; Almahmeed, W.; Bays, H.; Cuevas, A.; Di Angelantonio, E.; le Roux, C.W.; Sattar, N.; Sun, M.C.; Wittert, G.; Pinto, F.J.; et al. Obesity and cardiovascular disease: Mechanistic insights and management strategies. A joint position paper by the World Heart Federation and World Obesity Federation. Eur. J. Prev. Cardiol. 2022, 29, 2218–2237. [Google Scholar] [CrossRef]
- Ndumele, C.E.; Rangaswami, J.; Chow, S.L.; Neeland, I.J.; Tuttle, K.R.; Khan, S.S.; Coresh, J.; Mathew, R.O.; Baker-Smith, C.M.; Carnethon, M.R.; et al. Cardiovascular-Kidney-Metabolic Health: A Presidential Advisory From the American Heart Association. Circulation 2023, 148, 1606–1635. [Google Scholar] [CrossRef]
- Hossain, M.J.; Al-Mamun, M.; Islam, M.R. Diabetes mellitus, the fastest growing global public health concern: Early detection should be focused. Health Sci Rep. 2024, 7, e2004. [Google Scholar] [CrossRef]
- Ruze, R.; Liu, T.; Zou, X.; Song, J.; Chen, Y.; Xu, R.; Yin, X.; Xu, Q. Obesity and type 2 diabetes mellitus: Connections in epidemiology, pathogenesis, and treatments. Front. Endocrinol. 2023, 14, 1161521. [Google Scholar] [CrossRef]
- Okunogbe, A.; Nugent, R.; Spencer, G.; Powis, J.; Ralston, J.; Wilding, J. Economic impacts of overweight and obesity: Current and future estimates for 161 countries. BMJ Glob. Health 2022, 7, e009773. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Reyes-García, R.; Modrego-Pardo, I.; López-Martínez, M.; Soler, M.J. Are we ready for an adipocentric approach in people living with type 2 diabetes and chronic kidney disease? Clin. Kidney J. 2024, 17, sfae039. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Tronieri, J.S.; Butryn, M.L. Lifestyle modification approaches for the treatment of obesity in adults. Am. Psychol. 2020, 75, 235–251. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.M.; E Cooper, M.; de Zeeuw, D.; Grunfeld, J.-P.; Keane, W.F.; Kurokawa, K.; McGill, J.B.; E Mitch, W.; Parving, H.H.; Remuzzi, G.; et al. The losartan renal protection study—Rationale, study design and baseline characteristics of RENAAL (Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan). J. Renin-Angiotensin-Aldosterone Syst. 2000, 1, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Lewis, E.J. The role of angiotensin II receptor blockers in preventing the progression of renal disease in patients with type 2 diabetes. Am. J. Hypertens. 2002, 15, 123S–128S. [Google Scholar] [CrossRef]
- Wang, J.-Y.; Wang, Q.-W.; Yang, X.-Y.; Yang, W.; Li, D.-R.; Jin, J.-Y.; Zhang, H.-C.; Zhang, X.-F. GLP−1 receptor agonists for the treatment of obesity: Role as a promising approach. Front. Endocrinol. 2023, 14, 1085799. [Google Scholar] [CrossRef]
- Ussher, J.R.; Drucker, D.J. Glucagon-like peptide 1 receptor agonists: Cardiovascular benefits and mechanisms of action. Nat. Rev. Cardiol. 2023, 20, 463–474. [Google Scholar] [CrossRef]
- Méndez Fernández, A.B.; Vergara Arana, A.; Olivella San Emeterio, A.; Azancot Rivero, M.A.; Soriano Colome, T.; Soler Romeo, M.J. Cardiorenal syndrome and diabetes: An evil pairing. Front. Cardiovasc. Med. 2023, 10, 1185707. [Google Scholar] [CrossRef]
- Rico-Fontalvo, J.; Reina, M.; Soler, M.J.; Unigarro-Palacios, M.; Castañeda-González, J.P.; Quintero, J.J.; Raad-Sarabia, M.; de Moraes, T.P.; Daza-Arnedo, R. Kidney effects of Glucagon-Like Peptide 1 (GLP1): From molecular foundations to a pharmacophysiological perspective. Braz. J. Nephrol. 2024, 46, e20240101. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.E.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Green, J.B.; Hernandez, A.F.; D’Agostino, R.B.; Granger, C.B.; Janmohamed, S.; Jones, N.P.; Leiter, L.A.; Noronha, D.; Russell, R.; Sigmon, K.; et al. Harmony Outcomes: A randomized, double-blind, placebo-controlled trial of the effect of albiglutide on major cardiovascular events in patients with type 2 diabetes mellitus—Rationale, design, and baseline characteristics. Am. Heart J. 2018, 203, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Lincoff, A.M.; Brown-Frandsen, K.; Colhoun, H.M.; Deanfield, J.; Emerson, S.S.; Esbjerg, S.; Hardt-Lindberg, S.; Hovingh, G.K.; Kahn, S.E.; Kushner, R.F.; et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N. Engl. J. Med. 2023, 389, 2221–2232. [Google Scholar] [CrossRef] [PubMed]
- McGuire, D.K.; Marx, N.; Mulvagh, S.L.; Deanfield, J.E.; Inzucchi, S.E.; Pop-Busui, R.; Mann, J.F.; Emerson, S.S.; Poulter, N.R.; Engelmann, M.D.; et al. Oral Semaglutide and Cardiovascular Outcomes in High-Risk Type 2 Diabetes. N. Engl. J. Med. 2025, 392, 2001–2012. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Sattar, N.; Rosenstock, J.; Ramasundarahettige, C.; Pratley, R.; Lopes, R.D.; Lam, C.S.; Khurmi, N.S.; Heenan, L.; Del Prato, S.; et al. Cardiovascular and Renal Outcomes with Efpeglenatide in Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 896–907. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Lakshmanan, M.C.; Rayner, B.; Busch, R.S.; Zimmermann, A.G.; Woodward, D.B.; Botros, F.T. Dulaglutide versus insulin glargine in patients with type 2 diabetes and moderate-to-severe chronic kidney disease (AWARD-7): A multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 605–617. [Google Scholar] [CrossRef]
- Gragnano, F.; De Sio, V.; Calabrò, P. FLOW trial stopped early due to evidence of renal protection with semaglutide. Eur. Hear. J.-Cardiovasc. Pharmacother. 2024, 10, 7–9. [Google Scholar] [CrossRef]
- Apperloo, E.M.; Gorriz, J.L.; Soler, M.J.; Guldris, S.C.; Cruzado, J.M.; Puchades, M.J.; López-Martínez, M.; Waanders, F.; Laverman, G.D.; Beek, A.v.d.A.-V.d.; et al. Semaglutide in patients with overweight or obesity and chronic kidney disease without diabetes: A randomized double-blind placebo-controlled clinical trial. Nat. Med. 2025, 31, 278–285. [Google Scholar] [CrossRef]
- Vergara, A.; Jacobs-Cacha, C.; Llorens-Cebria, C.; Ortiz, A.; Martinez-Diaz, I.; Martos, N.; Dominguez-Báez, P.; Bosch, M.M.V.D.; Bermejo, S.; Pieper, M.P.; et al. Enhanced Cardiorenal Protective Effects of Combining SGLT2 Inhibition, Endothelin Receptor Antagonism and RAS Blockade in Type 2 Diabetic Mice. Int. J. Mol. Sci. 2022, 23, 12823. [Google Scholar] [CrossRef]
- Fonseca-Correa, J.I.; Correa-Rotter, R. Sodium-Glucose Cotransporter 2 Inhibitors Mechanisms of Action: A Review. Front. Med. 2021, 8, 777861. [Google Scholar] [CrossRef]
- Vergara, A.; Jacobs-Cachá, C.; Soler, M.J. Sodium-glucose cotransporter inhibitors: Beyond glycaemic control. Clin. Kidney J. 2019, 12, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Iordan, L.; Gaita, L.; Timar, R.; Avram, V.; Sturza, A.; Timar, B. The Renoprotective Mechanisms of Sodium-Glucose Cotransporter-2 Inhibitors (SGLT2i)—A Narrative Review. Int. J. Mol. Sci. 2024, 25, 7057. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- The EMPA-KIDNEY Collaborative Group; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2020, 383, 2219–2229. [Google Scholar] [CrossRef]
- Filippatos, G.; Anker, S.D.; Agarwal, R.; Ruilope, L.M.; Rossing, P.; Bakris, G.L.; Tasto, C.; Joseph, A.; Kolkhof, P.; Lage, A.; et al. Finerenone Reduces Risk of Incident Heart Failure in Patients With Chronic Kidney Disease and Type 2 Diabetes: Analyses From the FIGARO-DKD Trial. Circulation 2022, 145, 437–447. [Google Scholar] [CrossRef]
- Sjöström, L.; Narbro, K.; Sjöström, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef]
- Navarro-Díaz, M.; Serra, A.; Romero, R.; Bonet, J.; Bayés, B.; Homs, M.; Pérez, N.; Bonal, J. Effect of Drastic Weight Loss after Bariatric Surgery on Renal Parameters in Extremely Obese Patients. J. Am. Soc. Nephrol. 2006, 17, S213–S217. [Google Scholar] [CrossRef]
- Huang, H.; Lu, J.; Dai, X.; Li, Z.; Zhu, L.; Zhu, S.; Wu, L. Improvement of Renal Function After Bariatric Surgery: A Systematic Review and Meta-analysis. Obes. Surg. 2021, 31, 4470–4484. [Google Scholar] [CrossRef]
- Li, K.; Zou, J.; Ye, Z.; Di, J.; Han, X.; Zhang, H.; Liu, W.; Ren, Q.; Zhang, P.; Joles, J.A. Effects of Bariatric Surgery on Renal Function in Obese Patients: A Systematic Review and Meta Analysis. PLoS ONE 2016, 11, e0163907. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.; Porrini, E.; Martin-Taboada, M.; Luis-Lima, S.; Vila-Bedmar, R.; de Pablos, I.G.; Gómez, P.; Rodríguez, E.; Torres, L.; Lanzón, B.; et al. Renoprotective role of bariatric surgery in patients with established chronic kidney disease. Clin. Kidney J. 2021, 14, 2037–2046. [Google Scholar] [CrossRef] [PubMed]
- Nofal, M.; Yousef, A.; Alkhawaldeh, I.; Al-Jafari, M.; Zuaiter, S.; Eddin, S.Z. Dumping Syndrome after Bariatric Surgery. Ann. Ital. Chir. 2024, 95, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Gambioli, R.; Lepore, E.; Biondo, F.G.; Bertolani, L.; Unfer, V. Risks and limits of bariatric surgery: Old solutions and a new potential option. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 5831–5840. [Google Scholar]
- Gulinac, M.; Miteva, D.G.; Peshevska-Sekulovska, M.; Novakov, I.P.; Antovic, S.; Peruhova, M.; Snegarova, V.; Kabakchieva, P.; Assyov, Y.; Vasilev, G.; et al. Long-term effectiveness, outcomes and complications of bariatric surgery. World J. Clin. Cases 2023, 11, 4504–4512. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Agarwal, R.; Bakris, G.L.; I Cherney, D.Z.; Lam, C.S.P.; Neuen, B.L.; A Sarafidis, P.; Tuttle, K.R.; Wanner, C.; Brinker, M.D.; et al. Design and baseline characteristics of the Finerenone, in addition to standard of care, on the progression of kidney disease in patients with Non-Diabetic Chronic Kidney Disease (FIND-CKD) randomized trial. Nephrol. Dial. Transplant. 2025, 40, 308–319. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
León-Román, J.; López-Martínez, M.; Esteves, A.; Ciudin, A.; Núñez-Delgado, S.; Álvarez, T.; Lecube, A.; Rico-Fontalvo, J.; Soler, M.J. Obesity-Related Kidney Disease: A Growing Threat to Renal Health. Int. J. Mol. Sci. 2025, 26, 6641. https://doi.org/10.3390/ijms26146641
León-Román J, López-Martínez M, Esteves A, Ciudin A, Núñez-Delgado S, Álvarez T, Lecube A, Rico-Fontalvo J, Soler MJ. Obesity-Related Kidney Disease: A Growing Threat to Renal Health. International Journal of Molecular Sciences. 2025; 26(14):6641. https://doi.org/10.3390/ijms26146641
Chicago/Turabian StyleLeón-Román, Juan, Marina López-Martínez, Alexandra Esteves, Andreea Ciudin, Sara Núñez-Delgado, Tiffany Álvarez, Albert Lecube, Jorge Rico-Fontalvo, and María José Soler. 2025. "Obesity-Related Kidney Disease: A Growing Threat to Renal Health" International Journal of Molecular Sciences 26, no. 14: 6641. https://doi.org/10.3390/ijms26146641
APA StyleLeón-Román, J., López-Martínez, M., Esteves, A., Ciudin, A., Núñez-Delgado, S., Álvarez, T., Lecube, A., Rico-Fontalvo, J., & Soler, M. J. (2025). Obesity-Related Kidney Disease: A Growing Threat to Renal Health. International Journal of Molecular Sciences, 26(14), 6641. https://doi.org/10.3390/ijms26146641