Abstract
The introduction of CFTR modulators in the clinics has improved body mass index in cystic fibrosis (CF) individuals. Leptin is a major regulator of appetite and energy expenditure but is also involved in bone metabolism. Whether circulating leptin levels are associated with low bone mineral density (BMD) and fracture risk in CF remains unknown. Therefore, the present study aims to analyze and integrate the current evidence linking leptin and bone loss in CF. As no scientific evidence was found, we focused on secondary dysregulations of bone loss in CF that may be linked to pathologies that are similar to the various dysregulations and multisystemic manifestations in CF. Studies published from 2001 to 2022 were identified through the PubMed, Scopus, and Web of Science databases, and screening was performed following the PRISMA guidelines. The included studies were assessed using a quality checklist. From the 774 records identified, 28 studies met the inclusion criteria. Although no evidence has been found directly related to bone loss in CF individuals, some studies revealed a positive association between leptin levels and BMD, while others found an inverse association. Current evidence suggests that for circulating leptin levels to be a predictive biomarker of bone health, further research will be needed to reveal the direct and indirect mechanisms behind leptin and bone loss and to understand whether changes in leptin levels correlate with changes in BMD. Of note, studies with CF people would be of high importance to understand the role of leptin in CF-related bone disease.
1. Introduction
Leptin is secreted by mature adipocytes in white adipose tissue and its levels are directly proportional to the amount of white adipose tissue [1,2]. Its main function is the regulation of appetite and energy intake. Nevertheless, this adipokine has other effects in the body, namely, in bone homeostasis [1]. Of note, circulating leptin levels require tight tuning, as both hyper- and hypoleptinemia have been associated with a pro-inflammatory state, increasing susceptibility to infections, autoimmune diseases and inflammatory responses [3]. Regarding bone homeostasis, leptin promotes osteoblast cell proliferation and differentiation while hampering osteoclast formation, suggesting an important role in the pathophysiology of bone diseases [4,5]. Therefore, leptin seems to improve bone anabolism while decreasing bone catabolism. Osteopenia or low bone mass are usually due to dysregulation of bone metabolism, such as increased bone degradation and decreased bone formation [6].
Cystic fibrosis (CF) patients have higher levels of leptin [7] and are at a higher risk of developing osteopenia and osteoporosis through a multifactorial and yet not clearly understood mechanism [6,8,9]. Bone tissue dysregulation may be influenced by genetic defects in cystic fibrosis transmembrane conductance regulator (CFTR), pro-inflammatory status, among other factors [6]. Cystic fibrosis bone disease (CFBD) has devastating consequences for the quality of life and longevity of CF individuals [6]. A key component of minimizing the negative effects of low bone mass is early detection of bone alterations in CFBD. According to American Cystic Fibrosis Foundation and European Cystic Fibrosis Society guidelines, bone density scans are a routine assessment of bone mineralization that is crucial to providing useful information about body composition [8,10,11,12]. Measurement of bone mineral density (BMD) by dual-energy X-ray absorptiometry (DEXA or DXA) is considered the gold standard non-invasive method. It is recommended that a baseline assessment of BMD be performed before puberty, followed by periodic reassessments based on those results [12,13]. However, DEXA has some limitations, such as the incapability to detect alterations in bone microarchitecture, the exposure to X-rays, and its high cost. Moreover, only 66% of adults with CF undergo DEXA in the US [14]. This evidence highlights the risk of underdiagnosis of CFBD, as well as the need for better biomarkers to stratify patients and predict the risk of developing bone disease [15]. For example, it would be more advantageous to find a biomarker present in the blood, allowing BMD monitoring through routine venipuncture during the clinical appointment. CF individuals have higher levels of leptin in circulation and those levels correlate inversely with lung function [7]. Moreover, leptin has been associated with BMD and fracture risk [1,2,16,17,18,19]. However, it is still unknown whether circulating leptin levels are associated with low bone mineral density and fracture risk in cystic fibrosis. Therefore, it would be important to analyze the effect of leptin on CFBD and observe whether there is a correlation with BMD. This systematic review aims to summarize the current evidence in this area. In this context, two important points will be analyzed and discussed: (a) the association between leptin and BMD, and (b) the importance of leptin levels as a biomarker of bone health. In addition, a quality assessment checklist will be used to assess the reporting quality of the included studies.
2. Materials and Methods
2.1. Protocol, Registration and Search Strategy
Published studies were screened following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Guidelines [20,21] (Tables S1 and S2). The protocol was developed according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines [22] and registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number CRD42025631901). PubMed (https://pubmed.ncbi.nlm.nih.gov/; accessed on 20 October 2024), Scopus (https://www.scopus.com; accessed on 20 October 2024), and Web of Science (https://www.webofscience.com; accessed on 20 October 2024) databases were searched from 2001 to 20 October 2024, with the following keywords or medical subject heading (MeSH) terms: (leptin) AND (low bone mineral density AND bone loss). No publication date or language restrictions were applied at this stage. The reference lists of selected studies were manually reviewed to ensure that all relevant articles were identified and included. The procedure followed to select studies is presented in the PRISMA flow diagram (Figure 1).
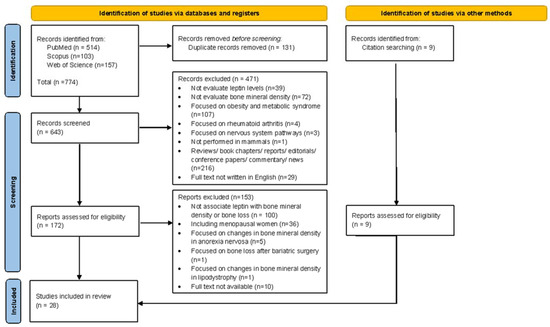
Figure 1.
Flow diagram of the studies’ selection and data collection process.
2.2. Eligibility Criteria
The inclusion criteria were (1) studies concerning the influence of leptin on bone mass; and (2) studies regarding circulating leptin levels associated with low bone mineral density. The exclusion criteria were as follows: (i) review articles, letters, case reports, editorials, book chapters, or conference papers; (ii) studies not performed in mammals; (iii) studies that did not evaluate the leptin levels; (iv) studies that did not evaluate the bone mineral density; (v) studies focused on obesity and metabolic syndrome; (vi) studies focused on rheumatoid arthritis; (vii) studies focused on nervous system pathways; (viii) studies including postmenopausal women; (ix) studies focused on changes in BMD in anorexia nervosa; (x) studies focused on bone loss after bariatric surgery; (xi) articles where full text was not available; and (xii) studies not written in the English language. For further explanation on the exclusion criteria please see the discussion section.
2.3. Study Selection and Data Collection Process
The reference list of the selected studies was screened independently by two reviewers (DC and ACG) according to the eligibility criteria. In a first phase, titles and abstracts were carefully analyzed, and studies that failed to meet the inclusion criteria were excluded immediately from further analysis. In a second phase, the full texts of the remaining studies were evaluated to determine their inclusion or exclusion. The reference lists of full articles that met inclusion criteria were then compared, and any discrepancies were resolved through discussion and consensus. There were no disagreements that required consultation with a third reviewer. The following information was collected from each selected study: authors’ names; publication year; population studied; study design; number of individuals/animals enrolled in the study; methodology related to leptin and BMD assessment; disease assessed in the study and main findings associated with leptin and BMD.
2.4. Quality Assessment
The quality assessment of the included studies was determined according to a quality checklist developed specifically for basic science studies by Cosme et al. [23] (Table 1 and Table 2). The authors (DC and ACG) applied the checklist with 14 criteria independently. No disagreements were found. Each criterion of the checklist was scored as follows: information not available in the paper (0 points); limited information provided (1 point); and complete information regarding that aspect (2 points). For each study, the scores of all criteria were added and divided by the maximum score (28 points) to obtain the overall quality score of the articles.

Table 1.
Characterization of the included studies performed in humans.
Table 2.
Characterization of the included studies performed in animal models.
3. Results
3.1. Literature Search and Study Selection
The initial electronic database search yielded 774 records (514 records in PubMed, 103 in Scopus, and 157 in ISI Web of Science), of which 131 were excluded for being duplicates (Figure 1). Based on titles and abstracts, 643 records were screened, and 471 studies were excluded. The remaining 172 studies were eligible for full text analysis (Figure 1). From these, 62 were excluded for not evaluating leptin levels associated with low BMD, 38 for not evaluating the influence of leptin on bone mass, 36 including postmenopausal women, 5 focused on changes in BMD in anorexia nervosa patients, 1 focused on bone loss after bariatric surgery, 1 focused on changes in BMD in lipodystrophy, and 10 for not having available full text (Figure 1). The manual search of relevant citations identified 9 additional studies. Overall, a total of 28 [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] studies were selected for inclusion in this systematic review.
3.2. Description of the Studies
The relevant data from each study are systematized in two tables, one including studies performed in humans (Table 1) and another comprising the findings from animal studies (Table 2). Regarding the studies included, leptin levels were quantified essentially by enzyme-linked immunoassay (ELISA) and radioimmunoassay (RIA). All included studies evaluate the BMD of individuals and the majority of the assessment was performed using dual energy X-ray absorptiometry (DEXA).
The included articles can be essentially divided into two main groups, observational and experimental study designs. Observational studies were mostly cross-sectional, case/control studies, also known as “retrospective studies”, which assessed associations between disease and exposure at one time point; and prospective cohort studies, a type of longitudinal study in which individuals are followed over a period of time [52,53]. The experimental study group randomly assigned the animal models in which the test group received the experimental intervention and the control group received a placebo or no treatment [52,53].
In this systematic review, the quality assessment performed for all included studies (Table 3, Table 4 and Table 5) revealed a mean quality score of 89% ± 0.29. The scores ranged from 75% [26,27] to 100% [39,48] (Table 3, Table 4 and Table 5 and Table S3).
Table 3.
Assessment of the reporting inclusiveness of the included studies; scored as 0 points (information not available in the paper); 1 point (limited information provided); 2 points (complete information regarding that aspect).
Table 4.
Assessment of the reporting inclusiveness of the included studies; scored as 0 points (information not available in the paper); 1 point (limited information provided); 2 points (complete information regarding that aspect). (Cont.).
Table 5.
Assessment of the reporting inclusiveness of the included studies; scored as 0 points (information not available in the paper); 1 point (limited information provided); 2 points (complete information regarding that aspect). (Cont.).
Considering the 14 defined criteria, the criteria with lower scores are definition of the endpoints of the study within the “Purpose and hypothesis” section; evaluation by independent observers; blinding; evidence of independent repetitions” allocated to “Data collection” section and disclose conflicts of interest and declaring funding sources within “Analyzing data and manuscript drafting” section.
Based on the characterization of the included studies (Table 1 and Table 2), we can highlight that none of the studies were related to CF or studied CF people. Nevertheless, some considered diseases related to the multisystemic manifestations of CF, such as lung disease [36,40], liver dysfunction [24,37], and diabetes [45]. These studies present evidence linking leptin and BMD between patients and healthy individuals in population samples. In line with the aim of this systematic review, scientific evidence was focused on the association of leptin with low BMD.
3.3. Association Between Leptin Levels and Bone Mineral Density: Evidence from Human Studies
3.3.1. Studies with Negative Association Between Leptin Levels and Bone Mass
The first study included in this systematic review to address was a case/control study of 58 adult patients with chronic liver disease and 54 healthy controls [24]. It demonstrated that leptin levels were negatively correlated with BMD at the lumbar spine and femoral neck in patients with chronic liver disease [24]. These results were later confirmed in chronic liver disease patients without renal disease [37]. In patients with chronic obstructive pulmonary disease, BMD was also negatively related with leptin levels [40]. Anagnostis et al. found that leptin levels were negatively associated with BMD at the femoral neck and total hip in hemophiliac men in a cross-sectional study [41]. More recently, Normand et al. carried out a cross-sectional pilot study in adolescents with idiopathic scoliosis and observed that leptin levels were higher in the patient group, but no association with BMD was observed [46]. In contrast, in the healthy individuals, it was observed that leptin levels were inversely correlated with BMD [46]. A cross-sectional study with patients with Duchenne muscular dystrophy demonstrated that these patients had higher levels of leptin than the healthy individuals, but had reduced BMD and reduced bone turnover markers [34]. Additionally, some observational studies conducted in healthy individuals, both young [32] and adult [25,29] men, revealed an inverse association between leptin and BMD.
3.3.2. Studies with Positive Association Between Leptin Levels and Bone Mass
Despite the previous results with negative associations, an observational study of 363 healthy adult men found a positive correlation between BMD and leptin levels [27]. However, the leptin levels of men with normal and low BMD did not differ significantly. Along these lines, a population analysis that included 117 healthy infants quantified leptin through umbilical cord blood and observed a positive correlation between leptin and whole-body mineral content, bone area and estimated volumetric BMD [28]. Through a cross-sectional and longitudinal study, Crabbe and colleagues demonstrated that there was no significant association between leptin and baseline BMD in the hip and forearm of elderly men [31]. However, this study reports that, prospectively, forearm BMD loss was positively associated with leptin levels, suggesting that age may be an interplay between leptin levels and bone loss. Female adolescents with idiopathic scoliosis with low BMD showed reduced leptin levels compared to healthy female controls [33]. Moreover, this work reports that BMD in the lumbar spine and femoral neck is positively associated with leptin levels [33]. In a cross-sectional study, leptin levels in male patients with chronic obstructive pulmonary disease (COPD) directly correlated with BMD [36]. Furthermore, the COPD patients with osteoporosis had lower leptin levels compared to those without osteoporosis. Similar conclusions were obtained in a single-center prospective study with inflammatory bowel disease patients [38]. More recently, Ho-Pham and colleagues observed that higher leptin levels were positively associated with BMD at the lumbar spine and femoral in both women and men [44]. These authors also reported that in healthy males, leptin levels were also correlated with whole-body BMD. Additionally, Brown et al. showed through univariate analysis that higher leptin levels were associated with increased BMD in patients infected with human immunodeficiency virus [42]. In a placebo-controlled study, long-term leptin administration in lean lypoleptinemic women led to an increase in lumbar spine BMD and bone mineral content [39].
3.3.3. Studies with No Association Between Leptin Levels and Bone Mass
Another group of studies found no association between leptin levels and BMD [26,30,35,43,45]. A study encompassing 105 healthy female adolescents concluded that leptin levels were not associated with total body BMD and bone mineral content [26]. Additionally, a retrospective study that included 20 survivors of childhood leukemia and lymphoma and 20 healthy children revealed that leptin levels were not correlated with BMD and osteocalcin, a marker of bone formation [30]. On the other hand, a prospective study conducted in 57 preterm newborns measured the cord blood serum leptin levels and found that cord blood serum leptin were significantly lower when compared to full-term newborns, but no association was found with lumbar spine BMD during the first two years [43]. Similar findings were obtained in a study of mothers with gestational diabetes or type 2 diabetes and normoglycemia, in which cord blood leptin levels of their infants were not associated with infant BMD [45]. Peng et al. in an observational study including 232 healthy men, also found no association between leptin levels and BMD [35].
In the quality assessment of the included studies performed in humans, six articles obtained a score above 90% [28,36,38,40,45,46] and only one article achieved the best score of 100% [39] (Table 3, Table 4, Table 5 and Table S3). In this set of publications, some articles have scores below 90% [24,25,26,27,29,30,31,32,33,34,35,37,41,42,43,44], which can be justified by the lack of information about the purpose and hypothesis and study design.
3.4. Impact of Leptin Administration on Bone Mineral Density: Evidence from Animal Studies
Although most published studies are observational and focus on the association of leptin with BMD in humans, some research has been performed in experimental animal models. Martin and colleagues, in 2015, observed that daily administration of 0.35 mg leptin per kg during 14 days prevented a progressive decrease in BMD in tail-suspended female Wistar rats [48]. Two years later, the same research team observed that a lower dose (50 µg/kg·day) of leptin administration was able to prevent the suspension-induced bone loss [49]. Given these results, it can be concluded that the effect of leptin on bone metabolism was dose dependent. In turn, Stunes et al. demonstrate that treatment with 100 µg/day of leptin resulted in a significant reduction in BMD in female Fisher rats [51]. According to Motyl et al. in diabetic rodent models, leptin levels were reduced and leptin replacement was not effective in preventing bone loss [50]. A study performed on rodents treated with clenbuterol, a type 2 adrenergic agonist, showed a decrease in leptin levels and BMD, and an increase in C-terminal collagen crosslink, a bone-resorption marker [47].
4. Discussion
Leptin has been linked to direct or indirect involvement in bone metabolism [1]. However, despite the scientific evidence published in recent years, it is still unknown whether leptin levels associate with BMD. To help answer this question, we analyzed and integrated current evidence on the relationship between circulating leptin levels and BMD. Even though no study directly studied CF individuals or focused on CFBD, several studies focused on pathologies that are similar to the various dysregulations and multisystemic manifestations in CF. Furthermore, we also considered studies that included healthy individuals. Additionally, a qualitative assessment of the included studies was also performed.
To minimize the possibility of bias in this systematic review, we excluded studies related to various manifestations/diseases unrelated to CF manifestations, such as obesity and metabolic syndrome, rheumatoid arthritis, nervous system pathways, postmenopausal osteoporosis, anorexia nervosa, bariatric surgery, and lipodystrophy. The results of these studies may give misleading conclusions regarding the association between leptin and BMD and are difficult to translate to CFBD. According to previous systematic reviews and meta-analyses performed in healthy individuals, leptin levels were positively associated with BMD, but this association was dependent on the menopausal status of women [16,17]. In published articles, leptin appears to be positively correlated with BMD, especially in postmenopausal women [16,17,18]. Studies including postmenopausal women have shown that high levels of leptin are associated with higher BMD levels and a lower risk of bone fractures [17,18]. Therefore, with the intention of minimizing bias in this review, we did not include studies involving menopausal and postmenopausal women. Our decision was based on data from the 2023 Cystic Fibrosis Foundation Registry, as the average age of death for individuals with CF was 36.9 years [9], indicating that most female CF individuals are at a pre-menopausal status. Nevertheless, the average survival age for CF individuals is increasing with improved CFTR modulator therapy, and for those born between 2019 and 2023, the prediction is 61 years [9]. Given that the average survival age in CF individuals is increasing, we considered studies that included middle-aged and elderly men to observe the association between leptin and BMD. Additionally, the impact of estrogen deprivation in CF women after menopause on bone health and CFBD should be addressed in future studies.
4.1. Evidence from Observational Studies
In this systematic review, evidence from human studies was analyzed separately from that performed in animal models to facilitate comparison of the main results. The studies included here approach the association of leptin levels with BMD in several pathologies: chronic obstructive pulmonary disease [36,40], chronic liver disease [24,37], chronic renal disease [37], type 2 diabetes mellitus [45], inflammatory bowel disease (IBD) [38], idiopathic scoliosis [33,46], Duchenne muscular dystrophy [34], and hypoleptinemia [39]. Additionally, the association between leptin and BMD has also been evaluated in healthy individuals: men, both young [32], adults [25,27,29,44], and elderly [31]; women, both young [26] and adults [44]; and infants [28,30,43].
Observational studies have shown that the association between leptin and BMD is still controversial. Despite the inconsistency in the results, this review reveals that considering individuals with associated pathology, the available studies reported a positive association between leptin levels and BMD. Evidence shows that a deterioration in lung function is correlated with a reduction in BMD [36], which is similar to CFBD because lung function and its decay have been correlated with low BMD [54,55,56,57,58,59,60]. Leptin levels were lower in men with obstructive pulmonary disease and osteoporosis than in those without osteoporosis [36]. To our best knowledge, the levels of leptin have not been compared in CF patients regarding BMD status. We hypothesize that future studies focusing on this relationship should be carried out. Along these lines, patients with IBD and osteoporosis had lower leptin levels compared to normal BMD patients [38]. Therefore, reduced leptin levels may decrease bone formation and increase bone resorption. Other studies have associated reduced BMD with advanced age in men [31]. CFBD is mostly diagnosed in adults, but bone defects may appear early in life [61,62] and progress with age [63]. Of note, in healthy individuals (men, women, and infants), circulating leptin levels are also positively associated with BMD [27,28,44].
Some studies have reported higher leptin levels in patient groups compared to control groups [34,37,46]. Circulating leptin levels are also increased in CF patients compared to healthy individuals [15]. Yet, the impact of these higher levels on bone health remains unexplored. On the other hand, one of the studies included in this systematic review reported a negative correlation between leptin and BMD in patients with chronic liver disease [37]. Other studies did not find a consensual association between leptin levels and BMD in adolescents with idiopathic scoliosis [33,46] and Duchenne muscular dystrophy [34]. While patients with Duchenne muscular dystrophy had a reduction in BMD and markers of bone formation and bone resorption [34], adolescents with idiopathic scoliosis and low BMD presented two scenarios: BMD and leptin were positively correlated in one of the studies [33], with no correlation in the second [46]. The remaining literature found no significant association between leptin and BMD. These studies highlight the importance of addressing leptin levels in the context of each pathology and always having in mind the population studied. Moreover, it is possible that the association between leptin levels and BMD is not direct and depends on other factors. This concept is particularly relevant in CFBD due to its multifactorial etiology [6].
4.2. Evidence from Experimental Studies
Regarding experimental studies using animal models, the consistency of published data follows the same line. The effect of leptin on BMD is dose- and time-dependent [48,49,51]. These observations raise the question of whether leptin effects on the bone are similar to parathyroid hormone (PTH), as continuous exposure to high levels of PTH leads to bone resorption but intermittent exposure to PTH promotes bone anabolism [64]. Nevertheless, type 1 diabetic rodents had reduced circulating leptin levels, and leptin replacement did not prevent bone loss [50]. Yet, the lack of effect of leptin replacement may be obscured by the endocrine dysfunction. This is particularly important in CFBD, as CF-related diabetes may impact bone loss [65]. Along these lines, hypoleptinemic women receiving long-term leptin administration had an increase in BMD at the lumbar spine [39]. Overall, the lack of consistency in the results and the reduced number of studies prompt that more research is needed.
4.3. Limitations
To date, as far as the authors know, no systematic review has been performed on the association between leptin and BMD with a focus on CFBD. This systematic review was performed according to the PRISMA guidelines [20], and the results of our analysis are reliable and useful for the next steps of sustained research in this field. Nevertheless, this systematic review has some limitations that should be considered. Firstly, despite the best efforts to optimize search strategies, 9 articles did not appear in electronic search. Possibly, this may be due to difficulties in keyword-based indexing services that are related to adequate keyword selection, which should be as closely as possible in line with medical subject headings and subheadings. Secondly, as a result of the heterogeneity found in the study design used in the included articles, it is difficult to generalize and compare the main findings in a suitable systematic review. Furthermore, several studies performed a cross-sectional analysis with short follow-up periods. In addition, there are few quantitative data available, which limits the potential for meta-analysis.
5. Conclusions
Overall, the available data do not clearly associate leptin levels with BMD due to the discrepancy of the results found. Some studies point to a positive association between leptin levels and BMD, while others reveal an inverse association. Several studies associate leptin and BMD, but none directly aimed to address the direct relationship between leptin levels and bone metabolism. While we found no evidence directly related to bone loss in CF patients, several studies included pathologies similar to CF-related disorders as well as multifactorial complications of CF. Yet, further studies using cohorts of CF patients need to be performed to dissect whether or not leptin levels correlate with alterations in bone mineral density and whether this association is modified by treatment with CFTR modulators.
The applicability of leptin as a biomarker for bone health has not been addressed. It will be important to determine whether changes in leptin levels correlate with changes in bone mineral density and architecture. This would be particularly important for CF-related bone disease due to the gap in surveillance of bone health and diagnosis of bone disease.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijms26052066/s1.
Author Contributions
D.C. was involved in data acquisition, interpretation, and manuscript drafting; A.C.G. was involved in the analysis of studies and manuscript drafting; A.C.G. and D.C. coordinated study conception, data interpretation, and manuscript drafting. All authors have read and agreed to the published version of the manuscript.
Funding
This work was performed under the financial support of a 2-year Pilot & Feasibility award, 003055G22, from the Cystic Fibrosis Foundation. D. Cosme acknowledges Cystic Fibrosis Foundation under Grant Ref. CFF—Research Grants 2021—BoneSAAver.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| BALP | Bone-specific alkaline phosphatase |
| BMD | Bone mineral density |
| CF | Cystic fibrosis |
| CFBD | Cystic fibrosis bone disease |
| CFTR | Cystic fibrosis transmembrane conductance regulator |
| COPD | Chronic obstructive pulmonary disease |
| DEXA | Dual-energy X-ray absorptiometry |
| ELISA | Enzyme-linked immunoassay |
| MeSH | Medical subject heading |
| PINP | Serum type I procollagen intact amino-terminal propeptide |
| PRISMA | Preferred reporting items for systematic reviews and meta-analysis |
| PRISMA-P | Preferred reporting items for systematic Review and Meta-Analysis Protocols |
| PROSPERO | Prospective register of systematic reviews |
| PTH | Parathyroid hormone |
| RIA | Radioimmunoassay |
| TRACP5b | Acid phosphatase isoform 5b |
References
- Upadhyay, J.; Farr, O.M.; Mantzoros, C.S. The role of leptin in regulating bone metabolism. Metabolism 2015, 64, 105–113. [Google Scholar] [CrossRef]
- Chen, X.X.; Yang, T. Roles of leptin in bone metabolism and bone diseases. J. Bone Miner. Metab. 2015, 33, 474–485. [Google Scholar] [CrossRef]
- Dornbush, S.; Aeddula, N. Physiology, Leptin. In StatPearls [Internet]; Updated 2023 April 10; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537038/ (accessed on 22 October 2024).
- Gordeladze, J.O.; Drevon, C.A.; Syversen, U.; Reseland, J.E. Leptin stimulates human osteoblastic cell proliferation, de novo collagen synthesis, and mineralization: Impact on differentiation markers, apoptosis, and osteoclastic signaling. J. Cell Biochem. 2002, 85, 825–836. [Google Scholar] [CrossRef]
- Cornish, J.; Callon, K.E.; Bava, U.; Lin, C.; Naot, D.; Hill, B.L.; Grey, A.; Broom, N.; Myers, D.; Nicholson, G.; et al. Leptin directly regulates bone cell function in vitro and reduces bone fragility in vivo. J. Endocrinol. 2002, 175, 405–415. [Google Scholar] [CrossRef]
- Fonseca, Ó.; Gomes, M.S.; Amorim, M.A.; Gomes, A.C. Cystic Fibrosis Bone Disease: The Interplay between CFTR Dysfunction and Chronic Inflammation. Biomolecules 2023, 13, 425. [Google Scholar] [CrossRef] [PubMed]
- Galiniak, S.; Podgórski, R.; Rachel, M.; Mazur, A. Serum leptin and neuropeptide Y in patients with cystic fibrosis-A single center study. Front. Med. 2022, 9, 959584. [Google Scholar] [CrossRef] [PubMed]
- Shteinberg, M.; Haq, I.J.; Polineni, D.; Davies, J.C. Cystic fibrosis. Lancet 2021, 397, 2195–2211. [Google Scholar] [CrossRef] [PubMed]
- Jacquot, J.; Delion, M.; Gangloff, S.; Braux, J.; Velard, F. Bone disease in cystic fibrosis: New pathogenic insights opening novel therapies. Osteoporos. Int. 2016, 27, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Cystic Fibrosis Foundation Patient Registry. 2023 Annual Data Report; Cystic Fibrosis Foundation: Bethesda, MD, USA, 2024. [Google Scholar]
- Sermet-Gaudelus, I.; Bianchi, M.L.; Garabédian, M.; Aris, R.M.; Morton, A.; Hardin, D.S.; Elkin, S.L.; Compston, J.E.; Conway, S.P.; Castanet, M.; et al. European cystic fibrosis bone mineralisation guidelines. J. Cyst. Fibros. 2011, 10 (Suppl. S2), S16–S23. [Google Scholar] [CrossRef]
- Southern, K.W.; Addy, C.; Bell, S.C.; Bevan, A.; Borawska, U.; Brown, C.; Burgel, P.-R.; Button, B.; Castellani, C.; Chansard, A.; et al. Standards for the care of people with cystic fibrosis; establishing and maintaining health. J. Cyst. Fibros. 2024, 23, 12–28. [Google Scholar] [CrossRef] [PubMed]
- Putman, M.S.; Baker, J.F.; Uluer, A.; Herlyn, K.; Lapey, A.; Sicilian, L.; Tillotson, A.P.; Gordon, C.M.; Merkel, P.A.; Finkelstein, J.S. Trends in bone mineral density in young adults with cystic fibrosis over a 15 year period. J. Cyst. Fibros. 2015, 14, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Ratti, G.A.; Fernandez, G.S.; Schechter, M.S.; Stalvey, M.S.; Ostrenga, J.; Fink, A.K.; Jain, R. Bone mineral density screening by DXA for people with cystic fibrosis: A registry analysis of patient and program factors influencing rates of screening. J. Cyst. Fibros. 2022, 21, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Silva Júnior, C.C.d.; Marques Queiroz, D.J.; de Paiva, M.P.; Lopes, M.T.; da Cunha Costa, M.; de Matos Bezerra, P.G.; de Carvalho Costa, M.J.; Silva, A.S.; Filho, J.M.; Cartaxo, C.G.B.; et al. Evaluation of anthropometry as an alternative to DXA as predictor of low bone mineral density in children and adolescents with cystic fibrosis. Clin. Nutr. ESPEN 2021, 45, 229–235. [Google Scholar] [CrossRef]
- Biver, E.; Salliot, C.; Combescure, C.; Gossec, L.; Hardouin, P.; Legroux-Gerot, I.; Cortet, B. Influence of adipokines and ghrelin on bone mineral density and fracture risk: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2011, 96, 2703–2713. [Google Scholar] [CrossRef]
- Liu, K.; Liu, P.; Liu, R.; Wu, X.; Cai, M. Relationship between serum leptin levels and bone mineral density: A systematic review and meta-analysis. Clin. Chim. Acta 2015, 444, 260–263. [Google Scholar] [CrossRef]
- Mohammadi, S.M.; Saniee, N.; Borzoo, T.; Radmanesh, E. Osteoporosis and Leptin: A Systematic Review. Iran. J. Public Health 2024, 53, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.R.; Baldock, P.A.; Cornish, J. Effects of Leptin on the Skeleton. Endocr. Rev. 2018, 39, 938–959. [Google Scholar] [CrossRef] [PubMed]
- Matthew, J.P.; David, M.; Patrick, M.B.; Isabelle, B.; Tammy, C.H.; Cynthia, D.M.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Cosme, D.; Estevinho, M.M.; Rieder, F.; Magro, F. Potassium channels in intestinal epithelial cells and their pharmacological modulation: A systematic review. Am. J. Physiol. Cell Physiol. 2021, 320, C520–C546. [Google Scholar] [CrossRef]
- Ormarsdóttir, S.; Ljunggren, O.; Mallmin, H.; Olofsson, H.; Blum, W.F.; Lööf, L. Inverse relationship between circulating levels of leptin and bone mineral density in chronic liver disease. J. Gastroenterol. Hepatol. 2001, 16, 1409–1414. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Takeda, N.; Sarui, H.; Takami, R.; Takami, K.; Hayashi, M.; Sasaki, A.; Kawachi, S.; Yoshino, K.; Yasuda, K. Association between serum leptin concentrations and bone mineral density, and biochemical markers of bone turnover in adult men. J. Clin. Endocrinol. Metab. 2001, 86, 5273–5276. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.C.; Cheng, W.C.; Yen, R.F.; Tsai, K.S.; Tai, T.Y.; Yang, W.S. Lack of independent relationship between plasma adiponectin, leptin levels and bone density in nondiabetic female adolescents. Clin. Endocrinol. 2004, 61, 204–208. [Google Scholar] [CrossRef]
- Papadopoulou, F.; Krassas, G.E.; Kalothetou, C.; Koliakos, G.; Constantinidis, T.C. Serum leptin values in relation to bone density and growth hormone-insulin like growth factors axis in healthy men. Arch. Androl. 2004, 50, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.K.; Godfrey, K.M.; Taylor, P.; Robinson, S.M.; Crozier, S.R.; Dennison, E.M.; Robinson, J.S.; Breier, B.R.; Arden, N.K.; Cooper, C. Umbilical cord leptin predicts neonatal bone mass. Calcif. Tissue Int. 2005, 76, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.W.; Lee, W.Y.; Rhee, E.J.; Baek, K.H.; Yoon, K.H.; Kang, M.I.; Yun, E.J.; Park, C.Y.; Ihm, S.H.; Choi, M.G.; et al. The relationship between serum resistin, leptin, adiponectin, ghrelin levels and bone mineral density in middle-aged men. Clin. Endocrinol. 2005, 63, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Yaris, N.; Sözen, E.; Erduran, E.; Okten, A.; Orem, A.; Cakirbay, H. Bone mineral metabolism and its relationship to leptin levels in survivors of childhood leukemia and lymphoma. Pediatr. Hematol. Oncol. 2005, 22, 489–498. [Google Scholar] [CrossRef]
- Crabbe, P.; Goemaere, S.; Zmierczak, H.; Van Pottelbergh, I.; De Bacquer, D.; Kaufman, J.M. Are serum leptin and the Gln223Arg polymorphism of the leptin receptor determinants of bone homeostasis in elderly men? Eur. J. Endocrinol. 2006, 154, 707–714. [Google Scholar] [CrossRef]
- Lorentzon, M.; Landin, K.; Mellström, D.; Ohlsson, C. Leptin is a negative independent predictor of areal BMD and cortical bone size in young adult Swedish men. J. Bone Miner. Res. 2006, 21, 1871–1878. [Google Scholar] [CrossRef]
- Qiu, Y.; Sun, X.; Qiu, X.; Li, W.; Zhu, Z.; Zhu, F.; Wang, B.; Yu, Y.; Qian, B. Decreased circulating leptin level and its association with body and bone mass in girls with adolescent idiopathic scoliosis. Spine 2007, 32, 2703–2710. [Google Scholar] [CrossRef] [PubMed]
- Söderpalm, A.C.; Magnusson, P.; Ahlander, A.C.; Karlsson, J.; Kroksmark, A.K.; Tulinius, M.; Swolin-Eide, D. Low bone mineral density and decreased bone turnover in Duchenne muscular dystrophy. Neuromuscul. Disord. 2007, 17, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.D.; Xie, H.; Zhao, Q.; Wu, X.P.; Sun, Z.Q.; Liao, E.Y. Relationships between serum adiponectin, leptin, resistin, visfatin levels and bone mineral density, and bone biochemical markers in Chinese men. Clin. Chim. Acta 2008, 387, 31–35. [Google Scholar] [CrossRef]
- Vondracek, S.F.; Voelkel, N.F.; McDermott, M.T.; Valdez, C. The relationship between adipokines, body composition, and bone density in men with chronic obstructive pulmonary disease. Int. J. Chron. Obstruct Pulmon Dis. 2009, 4, 267–277. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ghonemy, T.A.; Salim, E.M.; Atia, M.; Fekry, A.; Shawky, K. Serum leptin and bone mineral density in hemodialysis patients with or without liver diseases. Arab. J. Nephrol. Transplant. 2011, 4, 131–136. [Google Scholar] [CrossRef]
- Koutroubakis, I.E.; Zavos, C.; Damilakis, J.; Papadakis, G.; Neratzoulakis, J.; Karkavitsas, N.; Kouroumalis, E.A. Role of ghrelin and insulin-like growth factor binding protein-3 in the development of osteoporosis in inflammatory bowel disease. J. Clin. Gastroenterol. 2011, 45, e60–e65. [Google Scholar] [CrossRef] [PubMed]
- Sienkiewicz, E.; Magkos, F.; Aronis, K.N.; Brinkoetter, M.; Chamberland, J.P.; Chou, S.; Arampatzi, K.M.; Gao, C.; Koniaris, A.; Mantzoros, C.S. Long-term metreleptin treatment increases bone mineral density and content at the lumbar spine of lean hypoleptinemic women. Metabolism 2011, 60, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Fountoulis, G.A.; Minas, M.; Georgoulias, P.; Fezoulidis, I.V.; Gourgoulianis, K.I.; Vlychou, M. Association of bone mineral density, parameters of bone turnover, and body composition in patients with chronic obstructive pulmonary disease. J. Clin. Densitom. 2012, 15, 217–223. [Google Scholar] [CrossRef]
- Anagnostis, P.; Vakalopoulou, S.; Charizopoulou, M.; Kazantzidou, E.; Chrysopoulou, T.; Moka, E.; Agapidou, A.; Zournatzi, V.; Garipidou, V. Is there any association between leptin levels and bone mineral density in haemophiliac men? Arch. Med. Sci. 2013, 9, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.T.; Chen, Y.; Currier, J.S.; Ribaudo, H.J.; Rothenberg, J.; Dubé, M.P.; Murphy, R.; Stein, J.H.; McComsey, G.A. Body composition, soluble markers of inflammation, and bone mineral density in antiretroviral therapy-naive HIV-1-infected individuals. J. Acquir. Immune Defic. Syndr. 2013, 63, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Veselá, P.K.; Kaniok, R.; Bayer, M. Markers of bone metabolism, serum leptin levels and bone mineral density in preterm babies. J. Pediatr. Endocrinol. Metab. 2016, 29, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ho-Pham, L.T.; Lai, T.Q.; Nguyen, U.D.; Bui, Q.V.; Nguyen, T.V. Delineating the Relationship Between Leptin, Fat Mass, and Bone Mineral Density: A Mediation Analysis. Calcif. Tissue Int. 2017, 100, 13–19. [Google Scholar] [CrossRef]
- Krishnan, S.; Aston, C.E.; Fields, D.A.; Teague, A.M.; Lyons, T.J.; Chernausek, S.D. Bone Mass Accrual in First Six Months of Life: Impact of Maternal Diabetes, Infant Adiposity, and Cord Blood Adipokines. Calcif. Tissue Int. 2022, 111, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Normand, E.; Franco, A.; Alos, N.; Parent, S.; Moreau, A.; Marcil, V. Circulatory Adipokines and Incretins in Adolescent Idiopathic Scoliosis: A Pilot Study. Children 2022, 9, 1619. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, N.; Benhamou, C.L.; Brunet-Imbault, B.; Arlettaz, A.; Horcajada, M.N.; Richard, O.; Vico, L.; Collomp, K.; Courteix, D. Severe bone alterations under β2 agonist treatments:: Bone mass, microarchitecture and strength analyses in female rats. Bone 2005, 37, 622–633. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; de Vittoris, R.; David, V.; Moraes, R.; Bégeot, M.; Lafage-Proust, M.H.; Alexandre, C.; Vico, L.; Thomas, T. Leptin modulates both resorption and formation while preventing disuse-induced bone loss in tail-suspended female rats. Endocrinology 2005, 146, 3652–3659. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; David, V.; Malaval, L.; Lafage-Proust, M.H.; Vico, L.; Thomas, T. Opposite effects of leptin on bone metabolism: A dose-dependent balance related to energy intake and insulin-like growth factor-I pathway. Endocrinology 2007, 148, 3419–3425. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Motyl, K.J.; McCabe, L.R. Leptin treatment prevents type I diabetic marrow adiposity but not bone loss in mice. J. Cell Physiol. 2009, 218, 376–384. [Google Scholar] [CrossRef]
- Stunes, A.K.; Westbroek, I.; Gordeladze, J.O.; Gustafsson, B.I.; Reseland, J.E.; Syversen, U. Systemic leptin administration in supraphysiological doses maintains bone mineral density and mechanical strength despite significant weight loss. Endocrinology 2012, 153, 2245–2253. [Google Scholar] [CrossRef]
- Library, H.H.S. Study Design 101. Available online: https://guides.himmelfarb.gwu.edu/studydesign101 (accessed on 18 September 2024).
- Ranganathan, P. Understanding Research Study Designs. Indian. J. Crit. Care Med. 2019, 23 (Suppl. S4), S305–S307. [Google Scholar] [CrossRef]
- Conway, S.P.; Morton, A.M.; Oldroyd, B.; Truscott, J.G.; White, H.; Smith, A.H.; Haigh, I. Osteoporosis and osteopenia in adults and adolescents with cystic fibrosis: Prevalence and associated factors. Thorax 2000, 55, 798. [Google Scholar] [CrossRef] [PubMed]
- Elkin, S.L.; Fairney, A.; Burnett, S.; Kemp, M.; Kyd, P.; Burgess, J.; Compston, J.E.; Hodson, M.E. Vertebral Deformities and Low Bone Mineral Density in Adults with Cystic Fibrosis: A Cross-sectional Study. Osteoporos. Int. 2001, 12, 366–372. [Google Scholar] [CrossRef]
- Flohr, F.; Lutz, A.; App, E.; Matthys, H.; Reincke, M. Bone mineral density and quantitative ultrasound in adults with cystic fibrosis. Eur. J. Endocrinol. 2002, 146, 531–536. [Google Scholar] [CrossRef][Green Version]
- Rossini, M.; Del Marco, A.; Dal Santo, F.; Gatti, D.; Braggion, C.; James, G.; Adami, S. Prevalence and correlates of vertebral fractures in adults with cystic fibrosis. Bone 2004, 35, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Legroux-Gérot, I.; Leroy, S.; Prudhomme, C.; Perez, T.; Flipo, R.M.; Wallaert, B.; Cortet, B. Bone loss in adults with cystic fibrosis: Prevalence, associated factors, and usefulness of biological markers. Jt. Bone Spine 2012, 79, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Bravo, M.P.; Balboa, P.; Torrejón, C.; Bozzo, R.; Boza, M.L.; Contreras, I.; Jorquera, P.; Astorga, L. Bone mineral density, lung function, vitamin D and body composition in children and adolescents with cystic fibrosis: A multicenter study. Nutr. Hosp. 2018, 35, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, I.H.; Pressler, T.; Oturai, P.; Katzenstein, T.L.; Skov, M.; Frikke-Schmidt, R.; Hitz, M.F. Osteoporosis Is Associated with Deteriorating Clinical Status in Adults with Cystic Fibrosis. Int. J. Endocrinol. 2018, 2018, 4803974. [Google Scholar] [CrossRef] [PubMed]
- Ambroszkiewicz, J.; Sands, D.; Gajewska, J.; Chelchowska, M.; Laskowska-Klita, T. Bone turnover markers, osteoprotegerin and RANKL cytokines in children with cystic fibrosis. Adv. Med. Sci. 2013, 58, 338–343. [Google Scholar] [CrossRef]
- Sharma, S.; Jaksic, M.; Fenwick, S.; Byrnes, C.; Cundy, T. Accrual of Bone Mass in Children and Adolescents With Cystic Fibrosis. J. Clin. Endocrinol. Metab. 2017, 102, 1734–1739. [Google Scholar] [CrossRef]
- Bass, R.M.; Zemel, B.S.; Stallings, V.A.; Leonard, M.B.; Tsao, J.; Kelly, A. Bone accrual and structural changes over one year in youth with cystic fibrosis. J. Clin. Transl. Endocrinol. 2022, 28, 100297. [Google Scholar] [CrossRef]
- Silva, B.C.; Bilezikian, J.P. Parathyroid hormone: Anabolic and catabolic actions on the skeleton. Curr. Opin. Pharmacol. 2015, 22, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, I.H.; Hitz, M.F.; Katzenstein, T.L.; Oturai, P.; Skov, M.; Jørgensen, N.R.; Jensen, P.Ø.; Mikkelsen, C.R.; Krogh-Madsen, R.; Pressler, T.; et al. Markers of bone turnover are reduced in patients with CF related diabetes; the role of glucose. J. Cyst. Fibros. 2019, 18, 436–441. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).